You’re Missing This: Why mTOR Activation Is the Real Goal of Strength Training
Discover why mTOR activation—not just lifting weights—is the real driver of muscle growth, fat loss, and metabolic health. Learn how resistance training reprograms your body at the cellular level to improve insulin sensitivity, build lean muscle, and slow aging.
EXERCISEMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/10/202627 min read
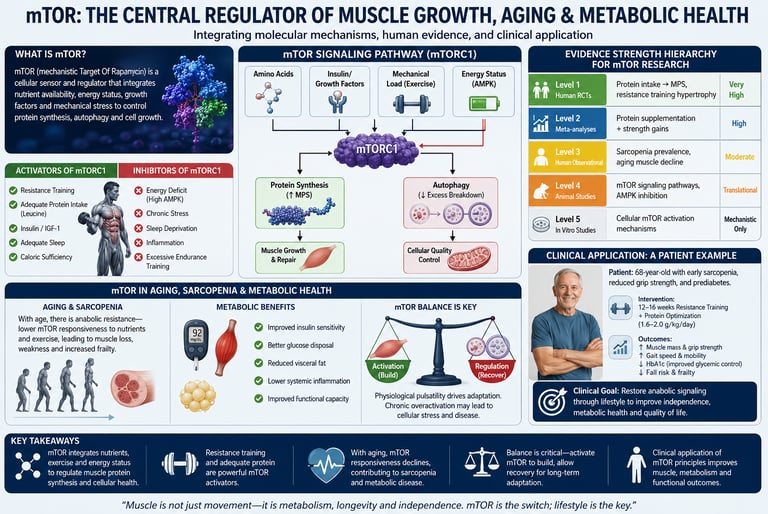
mTOR is your body's build-and-repair switch. Resistance training and leucine-rich protein turn it on in a healthy, pulsatile way. That signal tells muscle to grow, improves blood sugar control, and supports brain health through BDNF. Chronic elevation from inactivity and overeating is harmful. Pulsatile activation from exercise is therapeutic.
Key points
1. mTOR is your muscle’s master growth switch, and resistance training flips it on
When you lift weights or push a muscle under tension, proteins in the cell membrane sense that load. This triggers the mTORC1 pathway, which tells your muscle to build new proteins. The activation is pulsatile: it rises sharply after training, drives adaptation, then returns to baseline. That on/off cycle is healthy. Chronic, unrelenting mTOR elevation from overeating and inactivity is not.
2. Protein + resistance training creates a synergy you cannot get from either alone
Mechanical load activates mTOR through the PI3K/Akt pathway. The amino acid leucine activates mTOR through the Ragulator complex. Together, they produce a stronger signal than either stimulus by itself. This is the molecular reason behind the post-workout protein recommendation. Aim for 25–40g of high-quality protein per meal, with at least 2.5–3g of leucine, to reliably cross the threshold.
3. Muscle is a metabolic organ, not just a cosmetic one
Skeletal muscle handles about 80% of blood sugar disposal after meals. When you contract muscle, GLUT4 transporters move to the cell surface and pull glucose in without needing insulin. More muscle mass means a bigger “metabolic sink” for glucose. This is why resistance training improves blood sugar control in type 2 diabetes, often within a single session.
4. Aging blunts mTOR, but it does not stop it
After age 50, muscle becomes less sensitive to protein and training — a condition called anabolic resistance. The fix is not to give up. It is to adjust the dose. Older adults need more protein per meal, roughly 30–40 g with 3 g leucine, and sufficient training intensity, typically 60–85% of 1RM. Multiple trials show meaningful muscle and strength gains are possible into your 80s and 90s.
5. Resistance training builds mitochondria too
The old divide was simple: weights for muscle, cardio for mitochondria. New research shows hypertrophy-focused resistance training also improves mitochondrial capacity. mTOR does not just coordinate muscle fiber growth. It also supports mitochondrial biogenesis depending on the training stimulus. You are not forced to choose between strength and metabolic health.
6. Timing matters, but consistency matters more
mTOR signaling shows circadian variation. Mid to late afternoon may offer a small biological advantage for anabolic response. But the best time to train is the time you will do consistently. A suboptimal time you use beats a perfect time you skip. If you train in the morning, allow a longer warm-up.
7. The mTOR–AMPK balance is the real story behind strength vs endurance
AMPK is the cellular energy sensor that rises during prolonged aerobic work and suppresses mTOR. mTOR rises when energy is abundant and load is applied. They oppose each other moment to moment, but both are necessary for health. Moderate cardio does not “kill gains.” It improves capillary density and recovery. Separate sessions by 6+ hours when possible, and prioritize resistance training first on the same day.
8. Sleep, recovery, and progressive overload are part of the mTOR protocol
Most mTOR-driven protein synthesis occurs during sleep when growth hormone peaks. Chronic sleep restriction undercuts your results regardless of diet or training quality. Equally critical: you must increase load, reps, or volume over time. Without progressive overload, the mTOR signal adapts and plateaus. Train 3–4 times per week, sleep 7–9 hours, and add one rep before you add weight.
Bottom line for patients: Think of resistance training as controlled, pulsatile mTOR therapy. You are not just lifting weights. You are activating a pathway that builds muscle, clears blood sugar, supports your brain through BDNF, and helps offset age-related decline. The dose is load + protein + sleep + progression.
What Is mTOR — And Why Should You Care?
Every time you lift a weight, pick up a heavy bag, or push your muscles close to their limit, a molecular switch deep inside your muscle cells flips on. That switch is called mTOR — the mechanistic target of rapamycin — and it may be the single most important biological pathway governing how your body builds muscle, manages blood sugar, ages, and adapts to physical stress.
Most people think of resistance training as a way to get stronger or look better. That is true — but it fundamentally undersells what is actually happening at the cellular level. When you understand mTOR, you stop thinking of the gym as a cosmetic tool and start treating it as what the science increasingly says it is: medicine.
This guide breaks down exactly how mTOR works, why its activation pattern matters more than most people realize, what the latest research says about training, nutrition, and aging, and how you can use this knowledge to build a smarter, more effective approach to your long-term health.
What you will learn in this article:
The molecular mechanism by which resistance training activates mTOR
How mTOR activation links to insulin sensitivity, fat loss, and disease prevention
Why timing your training and meals affects mTOR signaling
How aging blunts the mTOR response — and how to overcome that
A practical, evidence-based protocol for maximizing mTOR-driven adaptation
How Resistance Training Activates mTOR
The Mechanotransduction Cascade
When a muscle fiber is placed under mechanical load — during a squat, a deadlift, a push-up, or any resistance movement — specialized proteins embedded in the cell membrane sense that tension. This triggers a process called mechanotransduction: the conversion of a physical force into a biochemical signal.
The cascade works roughly like this:
Mechanical tension deforms the cell membrane and activates integrins (structural proteins that anchor the cell to its surroundings)
Integrins activate focal adhesion kinase (FAK), an enzyme that acts as an early signal relay
FAK signals upstream through the PI3K/Akt pathway, a central anabolic hub
Akt activates mTORC1 — the specific mTOR complex responsible for muscle protein synthesis
mTORC1 phosphorylates p70S6 kinase, accelerating ribosome production and protein translation
New muscle proteins are assembled; the fiber grows
This entire process begins within minutes of a training session and peaks in the hours that follow. Critically, the activation is pulsatile — it rises, drives adaptation, and then subsides. This on/off cycling is what makes exercise-induced mTOR signaling healthy and beneficial, in contrast to the chronic, low-grade mTOR overactivation seen in metabolic disease.
The Non-Negotiable Four for mTOR-Driven Health
1. Mechanical Load (The Workout)
The Target: Aim for 3 to 4 resistance training sessions per week. Use a weight that is 60–85% of your maximum (a weight you can lift for 8 to 12 repetitions), performing 2 to 4 sets per exercise. Make sure to progress slightly every week.
Why It Matters: Physical tension is the primary trigger that flips your muscle-building switch (mTORC1) to "on." If you don't challenge the muscle with a sufficient load, the body simply won't send the signal to grow or repair.
2. Protein + Leucine (The Fuel)
The Target: Eat a total of 1.6 to 2.2 grams of protein per kilogram of body weight daily. Divide this across 3 to 4 meals, aiming for 25 to 40 grams of protein per meal, ensuring each meal contains 2.5 to 3 grams of leucine.
Why It Matters: Leucine is the specific amino acid that acts as a direct chemical sensor, telling your cells that building blocks are available. Spreading this out ensures your body gets consistent "grow and repair" signals throughout the day.
3. Sleep (The Construction Phase)
The Target: Get 7 to 9 hours of quality sleep nightly, keeping your sleep schedule consistent.
Why It Matters: Working out only sets the stage; sleep is when the actual building happens. Growth hormone peaks during deep sleep, and the vast majority of muscle repair and protein synthesis occurs overnight while your body rests.
4. Recovery Cycling (The Balance)
The Target: Take at least 1 to 2 dedicated rest days per week, and avoid training the exact same muscle group on back-to-back days.
Why It Matters: Your muscle-building switch shouldn't be left on 24/7. It needs to turn off periodically to allow your body to clear out cellular waste (a process called autophagy) and fully repair. Healthier muscles thrive on a natural rhythm of hard work followed by deliberate rest.
The Science of Muscle Hypertrophy: Three Pathways
Muscle hypertrophy — the actual growth of muscle fiber size — does not happen in the gym. It happens afterward, during recovery, as your body responds to the signals generated during training. Three partially overlapping mechanisms drive this process.
1. Mechanical Tension (Primary Driver)
The dominant stimulus for hypertrophy is mechanical tension applied to the muscle. This tension activates satellite cells — the muscle stem cells responsible for repair and growth — and initiates the mTOR signaling cascade described above. Progressive overload, the systematic increase of training stress over time, is essential for maintaining this stimulus. Without progression, adaptation plateaus.
2. Metabolic Stress (Secondary Anabolic Signal)
High-rep training at moderate loads generates metabolic stress: lactate accumulation, cellular swelling, and controlled production of reactive oxygen species (ROS). These metabolic byproducts serve as secondary anabolic signals, contributing to hypertrophy even when loads are relatively light — provided sets are taken close to muscular failure.
3. Muscle Damage and Repair
Eccentric contractions — the lowering phase of a lift — produce microscopic trauma to muscle fibers. The subsequent inflammatory response recruits immune cells and satellite cells to the damaged area, and the repair process contributes to long-term structural adaptation. Note that muscle damage is not required for hypertrophy; it is one contributing mechanism among several.
A New Finding: Resistance Training Also Builds Mitochondria
For decades, aerobic exercise was considered the primary driver of mitochondrial adaptation. That view is being revised. A 2025 study by Jerez-Martínez & Romero-Arenas, using near-infrared spectroscopy to measure mitochondrial function directly, found that hypertrophy-focused resistance training produced significant improvements in mitochondrial capacity — challenging the assumption that you must choose between building muscle and improving metabolic endurance at the cellular level.
This finding aligns with a 2025 review by Zhao, which documented mTOR's dual role in skeletal muscle: not only does it coordinate hypertrophic adaptation, it also promotes mitochondrial biogenesis depending on training stimulus and metabolic context. mTOR, in other words, is not just an anabolic switch — it is a context-sensitive metabolic regulator.
If You Are Over 50: Adjust the Dose
Anabolic resistance is real, but reversible. Your muscle needs a stronger signal to respond.
Protein per meal: Push to 30–40 g with 3 g+ leucine. Think 5 eggs, 150g chicken, 1.5 scoops whey, or 280g cottage cheese.
Training load: Do not stay with light bands forever. Work toward loads you can only lift 8–12 times with good form.
Prioritize grip strength: It is a validated proxy for total-body muscle health and longevity. Farmer carries, deadlifts, and pull-ups all help.
mTOR and Metabolic Health: Beyond Building Muscle
Skeletal Muscle as a Metabolic Organ
Skeletal muscle accounts for roughly 80% of postprandial glucose disposal — meaning it is the primary tissue responsible for clearing blood sugar after a meal. When muscle mass declines, or when muscle cells become insulin-resistant, this clearing capacity is severely impaired. Blood glucose remains elevated, the pancreas compensates with more insulin, and a cycle of metabolic dysfunction begins.
Resistance training addresses this directly through two mechanisms:
GLUT4 translocation: Muscle contractions activate signaling cascades that move glucose transporter proteins (GLUT4) to the cell surface, allowing glucose to enter the muscle cell independently of insulin. This is sometimes called the "insulin-independent glucose uptake" pathway — and it is one reason why a single resistance training session can meaningfully improve blood sugar control in people with type 2 diabetes.
Increased muscle mass: More total muscle tissue means a larger "metabolic sink" for glucose disposal. This effect is durable and cumulative with consistent training.
The Myokine Effect: Your Muscles as a Pharmacy
Contracting muscle does not just consume energy and build protein. It also acts as an endocrine organ, secreting signaling molecules called myokines into the bloodstream. These include:
IL-6 (interleukin-6): In the context of exercise, IL-6 functions as an anti-inflammatory signal — contrasting with its pro-inflammatory role in sedentary, obese individuals
Irisin: Stimulates fat browning (conversion of metabolically inert white fat to more active brown fat) and crosses the blood-brain barrier to stimulate BDNF production
BDNF (brain-derived neurotrophic factor): Supports neuronal growth, synaptic plasticity, and cognitive resilience
A 2025 study by Bulgay et al. found that BDNF co-expresses with mTOR in muscle tissue and is positively associated with muscle fiber size, lean mass, and power-related performance traits — suggesting that the brain-body benefits of resistance training are more tightly linked to mTOR signaling than previously appreciated.
The Chronic vs Pulsatile mTOR Distinction
Here is a nuance that most fitness content misses entirely: mTOR is not always beneficial. Chronic, unrelenting mTOR activation — driven by persistent hyperinsulinemia, excess caloric intake, and physical inactivity — has been linked to accelerated aging, impaired autophagy (the cellular self-cleaning process), and increased risk of insulin resistance and cardiometabolic disease.
Exercise-induced mTOR activation is categorically different. It is pulsatile: a sharp, well-defined rise in response to a defined stimulus, followed by a return to baseline that allows autophagy to resume. This cycling — anabolism followed by recovery — is what makes resistance training therapeutic rather than harmful. The goal is not to keep mTOR perpetually activated; it is to activate it strategically, through training and protein intake, and then allow the system to reset.
Sarcopenia: The Silent Muscle Loss Epidemic
What Is Sarcopenia?
Sarcopenia — from the Greek for "poverty of flesh" — is the progressive, age-related loss of skeletal muscle mass and strength. It is not simply feeling weaker as you get older. It is a diagnosable condition with measurable criteria:
Low muscle mass (assessed by DEXA scan or bioelectrical impedance analysis)
Reduced grip strength (below established age- and sex-specific thresholds)
Impaired physical performance (slow gait speed, difficulty rising from a chair)
Sarcopenia affects an estimated 10–27% of community-dwelling older adults globally, rising to over 50% in institutionalized or hospitalized populations. Beyond its impact on quality of life, it is an independent predictor of hospitalization, disability, and all-cause mortality.
The Molecular Drivers of Muscle Loss
At the cellular level, sarcopenia involves:
Increased protein breakdown via the ubiquitin-proteasome pathway
Overexpression of myostatin, a growth-inhibiting protein that suppresses muscle development
Chronic low-grade inflammation ("inflammaging") that disrupts anabolic signaling
Declining satellite cell function, impairing the muscle's regenerative capacity
Hormonal decline: testosterone, growth hormone, and IGF-1 all fall with age, reducing mTOR activation in response to both exercise and protein
A related condition gaining recognition is sarcopenic obesity — the simultaneous presence of excess fat mass and reduced lean mass. This combination is particularly dangerous, as the metabolic dysfunction of excess adipose tissue compounds the insulin resistance driven by muscle loss.
Resistance Training Reverses Sarcopenia — The Evidence
The good news: sarcopenia is substantially reversible. A 2025 scoping review by Sharma et al. systematically examined the effects of different resistance exercise variants — from traditional weight training to elastic band exercise and water-based resistance — and concluded that progressive overload is the key principle regardless of modality. Equipment matters less than consistency and progression.
A second comprehensive 2025 scoping review by Govindasamy et al. examined the physiological mechanisms through which resistance training reduces sarcopenia risk in healthy older adults. The review documented improvements across multiple systems:
Muscle fiber type composition shifts toward fast-twitch preservation
Enhanced neuromuscular recruitment patterns
Improved hormonal responsiveness (including mTOR signaling sensitivity)
Reduced systemic markers of inflammation
Anabolic Resistance After 50: Why Older Muscles Struggle
The Blunted mTOR Response
One of the most clinically significant phenomena in exercise physiology is anabolic resistance: the blunted muscle protein synthesis response to both protein intake and mechanical load that characterizes aging muscle.
An older adult consuming 20g of protein post-workout may experience significantly less mTOR activation than a younger person consuming the same amount. Similarly, the same training load that produces robust hypertrophy in a 25-year-old may be insufficient to overcome the anabolic threshold in a 65-year-old.
The mechanisms behind this include:
Impaired upstream mTOR signaling (reduced sensitivity to leucine and IGF-1)
Elevated myostatin expression
Reduced satellite cell density and responsiveness
Higher baseline levels of systemic inflammation
How to Overcome Anabolic Resistance
Anabolic resistance does not mean muscle growth is impossible in older adults. Multiple randomized controlled trials have demonstrated meaningful gains in muscle mass and strength in people well into their 80s and 90s. The approach, however, must be calibrated:
1. Increase protein intake per meal. Current evidence suggests older adults require a higher leucine threshold per meal to trigger robust mTOR activation — typically requiring 30–40g of high-quality protein (rather than the 20–25g sufficient for younger adults), providing at least 3g of leucine per sitting.
2. Prioritize leucine-rich protein sources. Whey protein, eggs, beef, chicken, fish, and dairy are all leucine-dense. For plant-based eaters, combining sources or using leucine-enriched blends is advisable.
3. Train with sufficient intensity. Light resistance training can produce some benefit, but loads at or above 60% of one-repetition maximum (1RM) produce more reliable mTOR activation across most older populations.
4. Address systemic inflammation. Adequate sleep, omega-3 fatty acid intake, and minimizing ultra-processed food consumption all help reduce the chronic inflammatory background that blunts anabolic signaling.
Circadian Timing and mTOR: Does When You Train Matter?
The Time-of-Day Effect
Emerging research suggests that the timing of your training session may influence mTOR activation beyond what load and volume alone can explain.
A 2025 study by Mishima, Takenaka, and colleagues examined the time-of-day effect of high-intensity muscle contraction on mTOR signaling and protein synthesis in mice. The findings indicated that mTOR signaling and muscle protein synthesis showed significant variation depending on the time of exercise, consistent with circadian regulation of anabolic pathways.
While direct translation to human training recommendations requires more research, the mechanistic basis is plausible: mTOR activity is regulated by circadian clock proteins, and the anabolic sensitivity of muscle tissue fluctuates across the 24-hour cycle.
Practical Takeaway
Mid-to-late afternoon (roughly 3–6 PM) appears to be a biologically advantageous window for resistance training in most people, coinciding with peaks in core body temperature, muscle strength, and hormonal readiness
Consistency matters more than timing. Training at a suboptimal time regularly will outperform occasional "optimal-time" sessions
Morning training is not counterproductive — it simply may require a slightly longer warm-up and may produce marginally different hormonal responses
BDNF, Satellite Cells, and the Overlooked mTOR Signals
Satellite Cells: The Repair Crew
Satellite cells are muscle stem cells that reside in a dormant state between the muscle fiber and its surrounding membrane. When a muscle fiber is stressed — by mechanical load, damage, or metabolic challenge — satellite cells are activated, proliferate, and fuse into existing fibers, contributing new nuclei and accelerating protein synthesis.
mTOR is a critical regulator of satellite cell activation and differentiation. A 2021 paper by Fukada and Ito clarified that mTOR-independent pathways also contribute to hypertrophy, particularly through satellite cell-mediated mechanisms, suggesting that the full picture of muscle adaptation is broader than mTOR alone. This does not diminish mTOR's centrality — it enriches it.
The mTOR–BDNF Connection
The 2025 study by Bulgay et al. adds a compelling new dimension: BDNF co-expression with mTOR in muscle tissue is associated with muscle fiber size, lean mass, and power output. This suggests that resistance training's cognitive and neurological benefits — improved mood, memory, and mental resilience — are not separate from its muscular effects. They may be mechanistically coupled through shared mTOR-associated signaling.
In practical terms: when you lift weights consistently and progressively, you are not just building a stronger body. You are potentially building a more resilient brain as well.
The mTOR–AMPK Balance: Strength vs. Endurance
Two Opposing Sensors
mTOR does not operate in isolation. It exists in a dynamic, reciprocal relationship with AMPK (AMP-activated protein kinase) — the body's primary cellular energy sensor. When energy stores are low (as during prolonged aerobic exercise), AMPK rises and actively suppresses mTOR. When energy and nutrients are abundant and mechanical load is applied (as during resistance training), mTOR predominates.
Signal State AMPK mTOR Outcome Prolonged aerobic exercise ↑ High ↓ Suppressed Mitochondrial biogenesis, fat oxidation Resistance training + protein ↓ Lower ↑ Activated Muscle protein synthesis, hypertrophy Caloric excess + inactivity Dysregulated ↑ Chronically elevated Insulin resistance, impaired autophagy Aging Dysregulated Blunted response Sarcopenia, metabolic dysfunction
A 2025 study by Mingzheng and You specifically examined the AMPK/mTOR balance in aging muscle, concluding that age-related dysregulation of this balance contributes meaningfully to both sarcopenia and insulin resistance — and that resistance training can partially restore appropriate AMPK/mTOR cycling.
The Concurrent Training Question
A common fear among gym-goers: "Will cardio kill my gains?" The interference effect — the idea that aerobic exercise undermines mTOR-driven hypertrophy — is real but substantially overstated in clinical populations.
Low-to-moderate intensity aerobic work (sometimes called "Zone 2" training, roughly 60–70% of maximum heart rate) actually enhances recovery by increasing capillary density — improving nutrient and oxygen delivery to mTOR-activated satellite cells. The interference effect is most pronounced when endurance sessions are long, frequent, and performed immediately before resistance training.
Practical guidance: Keep cardio sessions to 20–40 minutes of moderate intensity. Prioritize resistance training first if both are done on the same day. Allow at least 6 hours between the two where possible.
A Note on Metformin
Metformin — one of the most widely prescribed medications for type 2 diabetes — activates AMPK. This is part of its mechanism for lowering blood glucose. However, because AMPK suppresses mTOR, some research suggests that metformin may partially blunt the hypertrophic adaptation to resistance training. This does not negate the value of either intervention; resistance training remains highly beneficial for people on metformin. But clinicians and patients should be aware of this potential interaction and monitor muscle mass accordingly.
Red Flags You Are Missing mTOR Activation
You train but never increase weight or reps for months.
You eat “high protein” but only once per day, usually at dinner.
You are losing strength despite dieting.
You sleep under 6 hours and feel constantly sore.
Fix one variable at a time. Start with progressive overload, then protein distribution.
Practical Training Protocol for mTOR Activation
Core Variables: The FITT-VP Framework
Effective resistance training for mTOR activation, hypertrophy, and sarcopenia prevention requires attention to these variables:
Frequency (3–4 sessions per week): Aim to train each muscle group at least 2 times per week to keep the growth signals active.
Intensity (60–85% of your maximum weight): Choose a weight where you can manage 8 to 12 repetitions. This provides a heavy enough load to reliably flip your muscle-building switch on.
Volume (2–4 sets per exercise): Stick within this evidence-supported range to get the best muscle-growth results without overtraining.
Type (Compound movements + accessories): Focus on big, multi-joint exercises (like squats or presses) alongside smaller helper exercises to recruit and challenge as many muscle fibers as possible.
Progressive Overload (Weekly increases): Make sure to slightly increase your weight, reps, or total sets every week. This constant, gradual challenge is required to keep stimulating your muscle cells to grow.
Rest Between Sets (90–180 seconds): Rest for 1.5 to 3 minutes between your sets. This gives your muscles enough time to partially recover their energy stores so you can give your next set maximum effort
A Sample Weekly Structure
Day 1 — Lower Body (Squat-Dominant)
Barbell Back Squat: 4 × 8
Romanian Deadlift: 3 × 10
Bulgarian Split Squat: 3 × 10 each leg
Leg Press: 3 × 12
Calf Raise: 3 × 15
Day 2 — Upper Body (Push)
Bench Press: 4 × 8
Overhead Press: 3 × 10
Incline Dumbbell Press: 3 × 12
Tricep Dips: 3 × 12
Lateral Raise: 3 × 15
Day 3 — Rest or Zone 2 Cardio (20–30 min walking, cycling)
Day 4 — Lower Body (Hinge-Dominant)
Deadlift: 4 × 5
Hip Thrust: 3 × 10
Leg Curl: 3 × 12
Step-Up: 3 × 10 each leg
Day 5 — Upper Body (Pull)
Pull-Up or Lat Pulldown: 4 × 8
Barbell Row: 3 × 10
Seated Cable Row: 3 × 12
Face Pull: 3 × 15
Bicep Curl: 3 × 12
Days 6–7 — Rest
Special Considerations for Older Adults
Begin with bodyweight exercises or resistance bands to establish technique
Prioritize single-leg and single-arm movements to detect and correct asymmetries
Rest periods may be extended (up to 3 minutes) to allow full recovery between sets
Prioritize grip strength work — it is a proxy for overall muscle health and longevity
Supervised training with a physiotherapist or certified trainer is strongly advisable initially
Consult your doctor before starting a new resistance training program, particularly if you have cardiovascular disease, orthopedic injuries, osteoporosis, or uncontrolled diabetes.
Nutrition for mTOR Activation: Protein, Leucine, and Meal Timing
Daily Protein Targets
Protein provides the amino acid building blocks that mTOR directs into new muscle tissue. Without adequate protein, even a well-designed training program will fail to produce maximum adaptation.
Population Protein Target Sedentary adults 0.8 g/kg/day (minimum) Recreationally active adults 1.2–1.6 g/kg/day Actively building muscle 1.6–2.2 g/kg/day Older adults (>60 years) 1.6–2.0 g/kg/day minimum Older adults during muscle-building phase Up to 2.2–2.5 g/kg/day
A large scientometric analysis by Chen (2025), covering over three decades of nutritional intervention research in the context of resistance training (1992–2025), confirmed that leucine-rich protein sources consistently outperform alternatives for mTOR activation and hypertrophic outcome.
The Leucine Threshold
Leucine, a branched-chain amino acid (BCAA), is the primary nutritional activator of mTORC1. It works through the Ragulator-Rag GTPase complex, directly signaling mTOR that amino acids are available for protein synthesis.
A threshold of approximately 2.5–3g of leucine per meal appears necessary for robust mTOR activation. This is typically achieved through:
To maximize muscle growth, aiming for about 3 grams of leucine per meal is the sweet spot to fully turn on your body's muscle-building switch.
Here is how much of each food you need to eat to hit that 3-gram leucine goal:
Whey Protein Concentrate: 1 large scoop (delivering about 35g of protein)
Chicken Breast: ~150g (about 5.3 oz) cooked
Salmon: ~180g (about 6.3 oz) cooked
Eggs: 5 large eggs
Cottage Cheese: ~280g (about 1.2 cups)
Greek Yogurt: ~350g (about 1.5 cups)
Pea Protein Isolate: ~45g of protein powder (look for leucine-enriched formulas)Meal Distribution Strategy
Distributing protein intake across 3–4 meals per day — rather than consuming most protein at a single evening meal — maximizes the number of leucine threshold-crossing events throughout the day. Each crossing triggers a discrete mTOR activation window.
Sample high-protein day for a 75kg adult targeting 1.8 g/kg (135g total):
Breakfast: 3 whole eggs + 150g Greek yogurt + fruit → ~35g protein
Lunch: 150g grilled chicken breast + legumes + salad → ~40g protein
Post-workout snack: 35g whey protein shake → ~28g protein
Dinner: 180g salmon + vegetables + rice → ~40g protein
Post-Workout Timing
Consuming protein within 2 hours post-exercise supports muscle recovery and extends the period of elevated mTOR signaling initiated by training. While total daily protein intake is the most important variable, post-workout protein consumption remains a clinically useful strategy, particularly for older adults where the anabolic window may be narrower.
Evidence Summary: Key Studies at a Glance
1. It Builds Muscle and Boosts Energy (Metabolism)
For a long time, people thought weight lifting was just for building muscle size, while cardio was for metabolic health. The latest science completely flips that script.
The Science: Research demonstrates that lifting weights activates central cellular pathways—specifically the mammalian target of rapamycin (mTOR)—which simultaneously coordinate both muscle growth (hypertrophy) and the creation of new mitochondria, the energy factories inside your cells (Zhao, 2025).
The Patient Takeaway: Resistance training acts as a dual-threat. It increases your physical strength while drastically improving your body's overall metabolic capacity and cellular energy production.
2. Timing Might Give You an Extra Edge
The Science: Emerging research indicates that our 24-hour internal body clock (circadian rhythm) directly affects how our muscles respond to workouts. Muscle-building signals and protein synthesis appear to show variations over the course of the day, with afternoon windows offering potential advantages (Mishima et al., 2025).
The Patient Takeaway: If your schedule allows for flexibility, exercising in the afternoon might optimize your body’s natural muscle-building response compared to early morning sessions.
3. The Strong Body, Strong Brain Connection
The Science: Scientists have discovered a fascinating "muscle-brain axis." A critical brain chemical called BDNF (brain-derived neurotrophic factor, which helps your brain grow and adapt) co-expresses directly with the mTOR gene inside human skeletal muscle, linking greater expression to larger fast-twitch muscle fibers and enhanced power output (Bulgay et al., 2025).
The Patient Takeaway: Lifting weights doesn't just build bigger, more powerful muscles—it is deeply linked to your nervous system health and overall physical power potential.
4. The Ultimate Defense Against Aging (Sarcopenia)
As we get older, we naturally lose muscle mass and strength—a clinical condition known as sarcopenia. This deterioration is often driven by a cellular imbalance between AMPK (an energy-sensing engine) and mTOR (the growth engine), underlying muscle loss and insulin resistance (Mingzheng & You, 2025).
The Science: Multiple studies confirm that consistent resistance training directly restores this signaling balance in aging muscle tissue. It counters sarcopenia by optimizing hormonal, neuromuscular, and anti-inflammatory pathways (Govindasamy et al., 2025; Mingzheng & You, 2025). Furthermore, this progressive stimulus improves mitochondrial capacity, challenging the old view that only aerobic "cardio" can boost cellular health (Jerez-Martínez & Romero-Arenas,2026).
The Patient Takeaway: Progressive weight training is non-negotiable for healthy aging. The exact type of equipment or training modality you use matters far less than simply challenging your muscles with a heavier load or more reps over time (Sharma et al., 2025).
5. Quality of Protein Matters More Than Quantity
The Science: Dietary research emphasizes that amino-acid composition dictates muscle repair. Specifically, leucine-rich protein sources consistently outperform other options for muscle growth because they successfully cross the required threshold to trigger cellular pathways, independent of total generic protein intake alone (Chen, 2025).
The Patient Takeaway: To trigger muscle repair effectively, focus on hitting that "leucine threshold" (about 3 grams per meal) using high-quality sources like chicken, eggs, or whey, rather than just tracking your overall daily protein numbers.
Common Myths and Mistakes
Myth 1: "Older adults cannot build muscle."
False. While anabolic resistance blunts the response relative to younger adults, multiple randomized controlled trials have demonstrated meaningful gains in muscle mass and strength in adults in their 70s, 80s, and even 90s. The stimulus must be appropriate, protein intake must be sufficient, and progression must be consistent.
Myth 2: "Light weights are enough for muscle growth."
Partially true — with important caveats. Light loads can stimulate hypertrophy when sets are taken close to muscular failure. However, loads of 60% 1RM or higher produce more reliable, consistent results across most populations, and carry the additional benefit of bone loading stimulus — particularly important for older adults at risk of osteoporosis.
Myth 3: "Protein alone can reverse sarcopenia."
False. Protein intake without the mechanical stimulus of resistance training is insufficient to reverse established sarcopenia. Protein requires a training-induced anabolic environment — an elevated mTOR context — to be effectively channeled into new muscle tissue. Neither intervention is fully effective without the other.
Myth 4: "Cardio kills muscle gains."
Overstated. The interference effect is real but context-dependent. Low-to-moderate intensity aerobic training actually enhances recovery and may improve the delivery of nutrients to mTOR-activated satellite cells. The interference effect is most relevant when cardio volume is very high or sessions immediately precede resistance training.
Myth 5: "mTOR should always be as high as possible."
Dangerously incomplete. Chronic mTOR overactivation — not the pulsatile kind produced by exercise — is associated with impaired autophagy, accelerated aging, and increased cancer and metabolic disease risk. The goal is strategic, cyclical mTOR activation followed by recovery. This is precisely what resistance training with proper rest days produces.
Mistake: Neglecting sleep.
Research consistently shows that the majority of mTOR-driven protein synthesis occurs during sleep, when growth hormone release peaks. Getting 7–9 hours of quality sleep is not optional — it is part of the recovery protocol. Chronic sleep restriction undermines mTOR signaling and impairs training adaptation regardless of how well you eat or train.
Frequently Asked Questions
Q1. What exactly is mTOR, and how does resistance training activate it?
mTOR (mechanistic target of rapamycin) is a protein complex that functions as the master regulator of muscle protein synthesis and cellular growth. Resistance training activates it through mechanotransduction: when mechanical load is applied to muscle fibers, integrin proteins signal through FAK and the PI3K/Akt pathway to activate mTORC1, which then accelerates the machinery responsible for building new proteins inside muscle cells. The activation is pulsatile — it rises with training and nutrition, drives adaptation, and returns to baseline during recovery.
Q2. How quickly will I see results from resistance training?
Initial strength improvements typically appear within 2–4 weeks, primarily due to neurological adaptations as your nervous system learns to recruit muscle fibers more efficiently. Measurable changes in muscle size generally require 6–12 weeks of consistent, progressive training. In older adults, functional improvements — better balance, easier daily activities, reduced fatigue — often precede visible changes in body composition.
Q3. Is resistance training safe for people over 65?
Yes, and it is among the most evidence-supported interventions available at this life stage. Multiple clinical trials have demonstrated safety and efficacy in adults in their 70s, 80s, and 90s. Begin with bodyweight exercises or low-resistance bands, prioritize technique over load, and consult your doctor before starting, particularly if you have cardiovascular disease, osteoporosis, or other relevant conditions.
Q4. Do I need protein supplements, or can I get enough from food?
Whole food protein sources — meat, fish, eggs, dairy, and legumes — are entirely sufficient for most people. Protein supplements are not superior to food sources with equivalent leucine content; they are simply convenient. If meeting your protein targets through diet alone is difficult, a whey or plant-based protein supplement can be a practical addition.
Q5. What is the difference between mTOR activation from exercise and from overeating?
The difference is context, pattern, and consequence. Exercise-induced mTOR activation is acute, pulsatile, and coupled with mechanical adaptation signals — it produces muscle growth and then subsides, allowing autophagy (cellular cleanup) to resume. Overnutrition and inactivity produce chronic, low-grade mTOR elevation that impairs autophagy, disrupts insulin signaling, and is associated with metabolic disease and accelerated aging.
Q6. Can resistance training help manage type 2 diabetes?
Yes — meaningfully so. Resistance training increases GLUT4 translocation in muscle cells (enabling insulin-independent glucose uptake) and increases total muscle mass, expanding the body's capacity to dispose of blood glucose. In some clinical studies, the glycemic benefits of structured resistance training are comparable to those of first-line medications. Discuss exercise planning with your diabetes care team, as blood glucose monitoring and medication adjustments may be warranted.
Q7. How much protein do I need per meal to activate mTOR?
Research points to a leucine threshold of approximately 2.5–3g per meal as necessary for robust mTOR activation. This typically requires 25–40g of high-quality protein per meal, depending on the source. Older adults may require the higher end of this range (30–40g) due to anabolic resistance. Distributing protein evenly across 3–4 meals maximizes the number of daily mTOR activation events.
Q8. Does the time of day I train affect mTOR activation?
Emerging evidence, including a 2025 study by Mishima et al. in mice, suggests that mTOR signaling and muscle protein synthesis vary with circadian timing, with some evidence favoring mid-to-late afternoon training. However, consistency and progressive overload remain far more important than timing. Train when you can train regularly — the optimal time you won't use is inferior to the suboptimal time you will.
Q9. What role does sleep play in mTOR signaling?
Sleep is when growth hormone peaks and a significant portion of mTOR-driven protein synthesis occurs. Chronic sleep restriction (below 7 hours per night) blunts mTOR signaling and impairs training adaptation. Prioritize 7–9 hours of quality sleep as a non-negotiable component of your training program.
Q10. What is sarcopenic obesity, and how is resistance training relevant?
Sarcopenic obesity is the simultaneous presence of excess fat mass and reduced muscle mass — a combination that carries particularly high cardiometabolic risk. Standard dietary caloric restriction often accelerates muscle loss alongside fat loss, worsening metabolic rate. Resistance training is the only non-pharmacological intervention proven to preserve lean mass during a fat-loss phase, making it essential in any weight management strategy for older or metabolically compromised individuals.
Q11. Is combining strength and cardio training (concurrent training) advisable?
Yes — for most people, concurrent training is advisable, not problematic. The so-called "interference effect" of cardio on strength gains is largely overstated. Zone 2 aerobic work (moderate intensity, conversational pace, 20–40 minutes) enhances recovery, improves capillary density, and supports cardiovascular health without meaningfully impeding mTOR-driven hypertrophy when properly programmed.
Q12. I take metformin for diabetes. Does it affect my resistance training results?
Metformin activates AMPK, which competes with mTOR. Some research suggests it may partially reduce hypertrophic adaptation to resistance training. However, the benefits of both interventions substantially outweigh this interaction for most patients. Do not stop metformin without consulting your doctor. Ensure adequate protein intake, and consider discussing this interaction with your care team so muscle mass can be monitored.
Conclusion and Action Steps
The evidence assembled here points to a clear conclusion: resistance training is not merely physical exercise. It is a targeted molecular intervention that modulates the same signaling pathways your body uses to regulate aging, metabolism, and disease.
mTOR sits at the center of this paradigm — integrating mechanical load, nutritional status, and hormonal context to determine whether muscle grows, shrinks, or adapts metabolically. When activated in the pulsatile, exercise-driven manner that resistance training uniquely provides, it drives outcomes that no pharmaceutical intervention can fully replicate: increased lean muscle mass, improved insulin sensitivity, reduced systemic inflammation, stronger bones, and a more metabolically resilient body.
Your Action Steps
This week:
[ ] Calculate your daily protein target (1.6–2.2 g/kg body weight)
[ ] Plan 3 resistance training sessions of 45–60 minutes each
[ ] Identify your primary compound lifts (squat, hinge, push, pull)
[ ] Ensure each main meal contains 25–40g of leucine-rich protein
[ ] Protect 7–9 hours of sleep
This month:
[ ] Establish a training log to track progressive overload
[ ] Schedule a blood test with your doctor to measure fasting glucose and HbA1c (baseline for metabolic health tracking)
[ ] If over 60: consider a grip strength assessment and speak to your doctor about DEXA scanning to establish a muscle mass baseline
Long-term:
[ ] Progress your training loads consistently — at minimum, increase by one rep per set per week before adding weight
[ ] Reassess every 12 weeks: strength, body composition, energy levels, blood markers
[ ] Treat your training and protein intake as non-negotiable health behaviours — not optional extras
Speak to your doctor or a qualified exercise professional before beginning a new training program, especially if you have existing health conditions. The recommendations in this article are evidence-informed frameworks, not individualized medical prescriptions.
Author’s Note (Clinician’s Perspective)
From a clinical standpoint, mTOR sits at the intersection of metabolism, aging biology, and functional capacity. What is often presented in simplified fitness narratives is, in reality, a tightly regulated survival pathway that integrates mechanical load, nutrient availability, and endocrine signals to determine whether skeletal muscle is maintained or progressively lost. In my clinical practice, muscle health is not a cosmetic endpoint—it is a predictor of frailty, insulin sensitivity, and long-term independence.
Resistance training emerges as one of the most reliable non-pharmacological interventions to restore anabolic signaling in both young and older adults. By intermittently activating mTORC1 through structured mechanical stress and adequate protein intake, we observe improvements not only in muscle mass but also in glucose handling, mobility, and systemic inflammatory markers. Importantly, the goal is not chronic activation of mTOR, but physiological pulsatility that allows recovery and cellular renewal.
A typical patient example is a 68-year-old individual presenting with early sarcopenia, reduced grip strength, and prediabetes. After 12–16 weeks of supervised resistance training combined with protein optimization (1.6–2.0 g/kg/day), there is often a measurable improvement in gait speed, HbA1c reduction, and increased lean body mass. Clinically, this translates into improved resilience, reduced fall risk, and better metabolic control—outcomes far more meaningful than weight alone.
This article is intended for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before beginning a new exercise or nutrition program, especially if you have an existing medical condition.
Related Articles
mTOR, Protein, and Autophagy: How to Build Muscle Without Compromising Longevity
The mTOR Switch: Why Your Cells Stopped Listening to Insulin | DR T S DIDWAL
Can Resistance Training Reverse Diabetes? The Muscle–mTOR Link | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
No Time to Train? Science-Backed Workouts That Deliver | DR T S DIDWAL
References
Zhao, Y.-C. (2025). Dual roles of mTOR in skeletal muscle adaptation: Coordinating hypertrophic and mitochondrial biogenesis pathways for exercise-induced chronic disease management. Frontiers in Medicine, 12, 1635219. https://doi.org/10.3389/fmed.2025.1635219
Mishima, T., Takenaka, Y., Hashimoto-Hachiya, A., et al. (2025). Time-of-day effect of high-intensity muscle contraction on mTOR signaling and protein synthesis in mice. Scientific Reports, 15, 23702. https://doi.org/10.1038/s41598-025-06709-z
Fukada, S., & Ito, N. (2021). Regulation of muscle hypertrophy: Involvement of the Akt-independent pathway and satellite cells in muscle hypertrophy. Experimental Cell Research, 409(2), 112907. https://doi.org/10.1016/j.yexcr.2021.112907
Bulgay, C., Zorba, E., Kazan, H. H., et al. (2025). BDNF coexpresses with MTOR and is associated with muscle fiber size, lean mass and power-related traits. European Journal of Applied Physiology, 125, 2781–2792. https://doi.org/10.1007/s00421-025-05804-3
Mingzheng, X., & You, W. (2025). AMPK/mTOR balance during exercise: Implications for insulin resistance in aging muscle. Molecular and Cellular Biochemistry, 480, 5941–5953. https://doi.org/10.1007/s11010-025-05362-4
Jerez-Martínez, A., & Romero-Arenas, S. (2026). Impact of hypertrophy-focused resistance training on mitochondrial capacity: A new perspective through near-infrared spectroscopy. Research Quarterly for Exercise and Sport, 97(1), 60–67. https://doi.org/10.1080/02701367.2025.2542816
Sharma, S., Sharma, M., Tripathi, D., et al. (2025). Impact of resistance exercise variants on sarcopenia: A scoping review. Discover Public Health, 22, 474. https://doi.org/10.1186/s12982-025-00866-2
Govindasamy, K., Rao, C. R., Chandrasekaran, B., Parpa, K., & Granacher, U. (2025). Effects of resistance training on sarcopenia risk among healthy older adults: A scoping review of physiological mechanisms. Life, 15(5), 688. https://doi.org/10.3390/life15050688
Behringer, M., Heinrich, C., & Franz, A. (2025). Anabolic signals and muscle hypertrophy: Significance for strength training in sports medicine. Sports Orthopaedics and Traumatology, 41(1), 9–18. https://doi.org/10.1016/j.orthtr.2025.01.002
Chen, W. (2025). Nutritional interventions in muscle hypertrophy research: A scientometric analysis within the context of resistance training (1992–2025). Journal of Health, Population and Nutrition, 44, 272. https://doi.org/10.1186/s41043-025-01031-w
Zhao, Y. C., & Gao, H. (2024). mTOR and mitochondrial biogenesis in skeletal muscle: Dual roles in metabolic regulation. Acta Physiologica Sinica, 77(3), 573–586. https://doi.org/10.13294/j.aps.2025.0048
Deldicque, L., Theisen, D., & Francaux, M. (2005). Regulation of mTOR by amino acids and resistance exercise in skeletal muscle. European Journal of Applied Physiology, 94(1–2), 1–10. https://doi.org/10.1007/s00421-004-1255-6
Bodine, S. C., Stitt, T. N., Gonzalez, M., et al. (2001). Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nature Cell Biology, 3(11), 1014–1019. https://doi.org/10.1038/ncb1101-1014
Morton, R. W., Murphy, K. T., McKellar, S. R., et al. (2018). A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine, 52(6), 376–384. https://doi.org/10.1136/bjsports-2017-097608
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., et al. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Pedersen, B. K., & Febbraio, M. A. (2012). Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nature Reviews Endocrinology, 8(8), 457–465. https://doi.org/10.1038/nrendo.2012.49
Phillips, S. M. (2017). Current concepts and unresolved questions in dietary protein requirements and supplements in adults. Frontiers in Nutrition, 4, 13. https://doi.org/10.3389/fnut.2017.00013
Wilkinson, D. J., Hossain, T., Hill, D. S., et al. (2013). Effects of leucine and its metabolite β-hydroxy-β-methylbutyrate on human skeletal muscle protein metabolism. Journal of Physiology, 591(11), 2911–2923. https://doi.org/10.1113/jphysiol.2013.253203