Anabolic Resistance After 50: How to Preserve Muscle Strength, Metabolism, and Longevity
Anabolic resistance explained: how aging blunts muscle protein synthesis and how to restore it with optimal protein intake and resistance training.
SARCOPENIAAGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/11/202627 min read
Anabolic resistance is the age-related blunting of your muscles' ability to respond to protein and exercise. It begins around age 50, accelerates after 70, and is driven by impaired mTORC1 signaling, inflammation, and amino acid "leakage" to the gut and liver. It is countered with 1.2–1.6 g of protein per kg of body weight per day, leucine-rich meals, and progressive resistance training 2–3×/week.
Ways to reverse anabolic resistance after 50:
Eat 1.2–1.6g protein per kg of body weight daily, spread across 3–4 meals
Hit 30–40g protein + 2.5–3.5g leucine per meal to trigger muscle building
Do resistance training 2–3x per week with progressive overload
Take creatine 3–5g/day and omega-3s 2–4g/day to improve muscle sensitivity
Reduce inflammation with 7–9 hours of sleep and a Mediterranean-style diet
Key Takeaways: Anabolic Resistance After 50
1. Anabolic resistance is biology, not personal failure
After about age 50, muscle cells become less responsive to protein and exercise. This is called anabolic resistance. It’s driven by changes in mTORC1 signaling, inflammation, and how your gut handles amino acids — not a lack of effort. And importantly, it’s modifiable at any age.
2. The 0.8 g/kg/day protein rule is outdated for you
That recommendation prevents deficiency in young adults. For muscle preservation after 50, we aim for 1.2–1.6 g protein per kg of body weight daily. For a 165 lb person, that’s 90–120 g per day. You need more protein to deliver the same amino acid dose to muscle.
3. You have a higher “leucine threshold” now
Leucine is the amino acid that flips the muscle-building switch. A younger adult needs ~2 g of leucine per meal. After 60, you need 2.5–3.5 g per meal to trigger the same response. Practically, that means 30–40 g of high-quality protein at breakfast, lunch, and dinner — not just at dinner.
4. Resistance training is medicine for your muscles
Lifting weights or doing bodyweight exercises does something protein alone can’t: it directly reactivates mTORC1 and makes your muscles sensitive to amino acids for 24–48 hours. 2–3 sessions per week using progressive overload is the most powerful intervention we have. It’s never too late — we see gains in patients in their 70s and 80s.
5. Inflammation is an anabolic brake
Chronic low-grade inflammation, or “inflammageing,” suppresses the signals that build muscle. Poor sleep, excess stress, and ultra-processed diets all feed this. A Mediterranean-style diet, 7–9 hours of sleep, and stress management aren’t “extras” — they directly improve your muscle’s ability to respond.
6. Your gut takes a bigger “protein tax” with age
We call it splanchnic sequestration. Your gut and liver extract more amino acids before they reach muscle. That’s one reason why older adults need higher total protein and better distribution across meals. Spreading protein evenly beats loading it all at dinner.
7. A few supplements have real evidence behind them
If you’re doing the fundamentals, these can help:
Creatine monohydrate 3–5 g/day: Augments strength and mass gains from training. Safe, well-studied.
Omega-3s 2–4 g EPA+DHA/day: Improve muscle sensitivity to protein.
Vitamin D: Correct if deficient — common after 50 and needed for muscle function.
Whey or EAA: Useful if hitting 30–40 g per meal with food is difficult.
8. This is reversible, and small changes compound
Muscle loss is not inevitable. With consistent resistance training, leucine-rich meals 3x/day, and attention to sleep and inflammation, we can restore a significant portion of your anabolic sensitivity. Strength gains often appear in 4–6 weeks; muscle mass changes follow in 2–4 months. The trajectory is modifiable.
What Is Anabolic Resistance?
You're eating plenty of protein. You're staying active. Yet somewhere after your 50th birthday, something changes — recovery slows, strength plateaus, and the mirror tells a story you didn't write.
This is not a failure of effort. It has a name, a mechanism, and — crucially — a solution.
Anabolic resistance is the reduced ability of aging skeletal muscle to mount a protein synthesis response to the two most powerful anabolic stimuli available to us: dietary protein and physical exercise. It is the primary biological engine driving sarcopenia (age-related muscle loss), and it sits at the intersection of metabolic health, functional independence, and longevity.
The numbers are stark:
Adults lose 5–8% of skeletal muscle mass per decade after midlife (Pérez-Castillo et al., 2025)
Decline accelerates sharply after age 70
Muscle loss is directly linked to insulin resistance, type 2 diabetes, falls, frailty, and premature death
What makes anabolic resistance particularly frustrating — and scientifically fascinating — is this: older adults eating the same protein and doing similar exercise as younger adults generate a significantly weaker muscle protein synthesis (MPS) response (Deane et al., 2024). Same input. Weaker output.
The problem is not your protein. The problem is your muscles' ability to hear its signal.
The good news: Anabolic resistance is modifiable. With the right nutrition, training, and lifestyle strategies, you can significantly restore your muscles' anabolic sensitivity — at any age.
Why Muscles Stop Responding After 50
To understand anabolic resistance, you need a working model of how muscles normally grow and maintain themselves.
Every day, your muscles cycle through protein turnover: old or damaged muscle proteins are broken down (catabolism) and new ones are assembled (anabolism). When building exceeds breakdown, muscle grows. When they balance, muscle is maintained. When breakdown wins, muscle shrinks.
The three primary triggers for the anabolic side of this equation are:
Dietary protein — particularly essential amino acids (EAAs), especially leucine
Resistance exercise — mechanical loading that directly activates muscle growth machinery
Anabolic hormones — testosterone, insulin, IGF-1
In a young, healthy person, these signals work together efficiently. A meal containing 20–25 g of high-quality protein reliably activates the mTORC1 pathway — the master regulator of muscle protein synthesis — producing a robust, sustained anabolic response.
In aging muscle, this same meal may only produce a muted flicker of response. The sensing machinery is less sensitive. The signal pathway is partially blocked. The anabolic window is shorter.
Think of it this way: In a young muscle, a protein-rich meal is like turning on a light at full brightness. In an aging muscle, the same meal dims the room to a soft glow — and the glow fades faster.
This is anabolic resistance. And understanding exactly why it happens unlocks the most effective strategies to reverse it.
The Biology: 5 Mechanisms Driving the Problem
Recent research has identified several specific, overlapping mechanisms behind anabolic resistance. You don't need to memorize the molecular details — but understanding the "what" helps explain why the interventions that work actually work.
1. Impaired mTORC1 Signaling
The mTORC1 (mechanistic Target of Rapamycin Complex 1) pathway is the master switch of muscle protein synthesis. When amino acids — especially leucine — arrive in muscle cells after a meal, they are detected by molecular sensors including Sestrin2, CASTOR1, and the GATOR2 complex, which then activate mTORC1 to initiate protein building.
In aging muscles, this sensing machinery loses sensitivity. A landmark 2025 study published in the Journal of Cachexia, Sarcopenia and Muscle found that older men who maintained a robust anabolic response to protein showed significantly higher expression of amino acid sensors (including GATOR2 members and Sestrin2) and mTORC1 activators compared to peers who showed resistance (Horwath et al., 2025).
This finding is critically important: it means that preserving — or upregulating — this sensing machinery is a primary target of intervention.
Key insight: The problem isn't usually that older adults don't eat enough protein. The problem is that their muscles can't hear it as loudly.
2. Splanchnic Sequestration: The "Protein Tax"
When you eat protein, it's digested into amino acids that pass through your gut and liver before reaching your muscles. In younger adults, this "first-pass extraction" is relatively modest. In older adults, the gut and liver appear to extract a disproportionately large share of ingested amino acids for local metabolic demands — leaving less available in the bloodstream to stimulate peripheral muscle protein synthesis (Deane et al., 2024).
The practical consequence: older adults may need meaningfully more dietary protein than younger adults just to deliver the same amino acid dose to their muscles.
Plain-language version: There's a "protein tax" that increases with age. Your gut and liver take a bigger cut before the nutrients reach your biceps. You need to eat more to ensure your muscles get their share.
3. Reduced Anabolic Hormone Sensitivity
Aging is associated with declining testosterone, growth hormone, and IGF-1 — but equally important is that muscle cells become less sensitive to these hormones even when levels are adequate (Pérez-Castillo et al., 2025). Hormonal blunting compounds the reduced nutritional signaling, creating a double disadvantage.
4. Inflammageing: The Silent Anabolic Brake
Chronic, low-grade systemic inflammation — termed inflammageing — is a hallmark of biological aging. Inflammatory cytokines, particularly TNF-α and IL-6, directly interfere with the insulin/IGF-1 signaling axis and actively suppress mTORC1 function. The result is a pro-catabolic internal environment that promotes muscle breakdown even in the face of adequate protein intake (Pérez-Castillo et al., 2025).
This is why lifestyle factors like sleep quality, stress management, and dietary patterns are not peripheral concerns — they are directly upstream of muscle biology.
5. Gut Microbiome Shifts
Emerging evidence implicates the gut microbiome in anabolic resistance. Age-related changes in microbial composition can alter protein digestion efficiency, amino acid bioavailability, and even systemic inflammation — adding another layer to what is clearly a multifactorial problem (Pérez-Castillo et al., 2025; McColl et al., 2025).
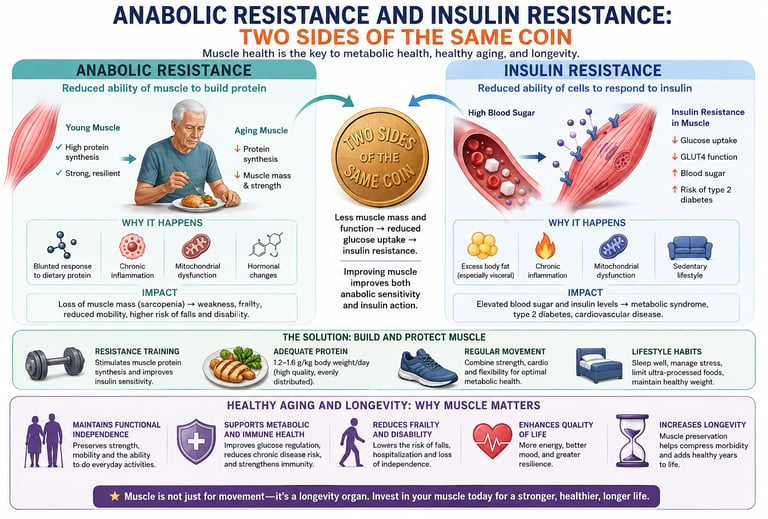
Anabolic Resistance and Insulin Resistance: Two Sides of the Same Coin
Skeletal muscle is the body's largest site of glucose disposal, accounting for nearly 80% of insulin-stimulated glucose uptake. As anabolic resistance develops with aging, muscles become less responsive not only to protein but also to insulin. Reduced muscle mass and impaired GLUT4-mediated glucose transport decrease glucose clearance from the bloodstream, promoting insulin resistance and increasing the risk of metabolic syndrome and Type 2 diabetes. Conversely, resistance training improves both anabolic sensitivity and insulin action by increasing muscle mass, enhancing GLUT4 translocation, and restoring metabolic flexibility. This makes muscle preservation one of the most effective strategies for maintaining healthy glucose metabolism during aging.
Healthy Aging and Longevity: Why Muscle Matters
Muscle is increasingly recognized as a critical longevity organ. Beyond strength and mobility, healthy muscle supports metabolic health, immune function, glucose regulation, and resilience during illness. Age-related muscle loss is strongly associated with frailty, falls, disability, hospitalization, and reduced quality of life. Preserving muscle through adequate protein intake, resistance training, and healthy lifestyle habits helps maintain functional independence and compress morbidity—reducing the years spent living with chronic disease and disability. In many ways, maintaining muscle mass is one of the most powerful investments in healthy aging and long-term vitality.
Protein Strategy: How Much, How Often, What Type
Nutrition is your most accessible lever for overcoming anabolic resistance. Here is what the current evidence actually recommends — and why it differs significantly from standard guidelines.
How Much Protein Do You Actually Need After 50?
The standard guideline of 0.8 g/kg/day was established primarily from studies in younger populations and reflects the minimum needed to prevent deficiency — not the amount needed to preserve or build muscle in aging adults.
For older adults with anabolic resistance, most leading researchers now recommend:
Goal Protein Target Minimum for muscle maintenance 1.0–1.2 g/kg/day Optimal for muscle preservation 1.2–1.6 g/kg/day Active aging / recovery from illness 1.6–2.0 g/kg/day
Real-world example: A 75 kg (165 lb) person aiming for muscle preservation needs approximately 90–120 g of protein per day — roughly double the standard RDA.
A comprehensive 2024 systematic review and meta-analysis by Hettiarachchi et al., published in Ageing Research Reviews, confirmed that higher protein supplementation doses produce meaningfully greater effects on muscle mass in older adults, with the benefit-to-dose relationship extending well above standard guidelines.
How Often Should You Eat Protein?
Distribution matters as much as total intake. Research consistently shows that spreading protein evenly across three to four meals per day is superior to loading protein into one or two sittings.
Many older adults eat relatively little protein at breakfast (toast, fruit, cereal), a moderate amount at lunch, and concentrate most protein at dinner. This pattern is suboptimal — it leaves your muscles without an anabolic stimulus for the majority of the day.
Target: 30–40 g of high-quality protein at each main meal.
A 2026 systematic review and meta-analysis by Kristiansen, Vissing, and Nielsen (Frontiers in Physiology) specifically examining age-related anabolic resistance and post-absorptive muscle protein synthesis reinforced that the post-absorptive state — the periods between meals — is where aging muscle is most vulnerable to net protein loss.
Animal vs. Plant Protein: Does It Matter?
Both can work, but with important nuances:
Animal proteins (meat, fish, eggs, dairy):
Higher in leucine per gram of protein
More bioavailable (less splanchnic sequestration)
Reliably overcome the leucine threshold with standard servings
Generally superior for MPS in older adults
Plant proteins (legumes, soy, grains, nuts):
Lower leucine density in most sources
Reduced bioavailability vs. animal sources
Can be effective when consumed in higher quantities
Strategic combinations (e.g., soy + wheat) improve amino acid profiles
Whole soy (tofu, edamame, tempeh) is among the best plant options
If you follow a plant-based diet: Increase total protein intake by approximately 20–30% above animal protein targets, prioritize complete plant proteins, and consider leucine supplementation (discussed below).
The Leucine Threshold Explained
Of all the amino acids, leucine plays a uniquely critical role in initiating muscle protein synthesis. It acts as the primary trigger for mTORC1 activation — the molecular "ignition key" that starts the muscle-building process.
Because ageing blunts the sensitivity of the leucine-sensing machinery (particularly Sestrins 2 and the GATOR2 complex), older adults require a higher leucine dose per meal to achieve the same anabolic response as younger adults.
The Leucine Threshold: What the Numbers Mean
Population Leucine Needed Per Meal to Trigger MPS Young adults (20–35) ~1.8–2.0 g Middle-aged adults (40–55) ~2.0–2.5 g Older adults (60+) ~2.5–3.5 g
Based on Deane et al. (2024) and Horwath et al. (2025)
Leucine Content of Common Foods (per 30g protein serving)
Whey Protein Concentrate (~3.0–3.5 g) | ✅ Optimal
The undisputed gold standard for rapid, high-concentration leucine delivery.
Cottage Cheese (~2.8–3.0 g) | ✅ Optimal
Exceptionally high for a whole food, making it an incredible slow-digesting casein option.
Chicken Breast (~2.5–2.8 g) | ✅ High
A reliable, lean staple that easily hits the optimal muscle-building threshold.
Greek Yogurt (~2.5–2.8 g) | ✅ High
Ties with chicken as a top-tier dairy source for leucine efficiency.
Salmon (~2.4–2.6 g) | ✅ High
Comfortably hits the sweet spot while pulling double duty with healthy omega-3 fats.
Eggs (Whole) (~2.3–2.5 g) | ✅ Good
Sits right on the threshold of the ideal "leucine trigger" zone.
Pea Protein Isolate (~2.0–2.2 g) | ✅ Moderate
Punches well above its weight for a vegan option, though slightly lower than animal sources.
Tofu (Firm) (~1.8–2.0 g) | ⚠️ Lower
Requires a larger total serving size to trigger optimal muscle protein synthesis.
Lentils (~1.5–1.7 g) | ⚠️ Lower
Typical for legumes; you will need to consume more total protein to get the same leucine spark.
Key Takeaways
The ~2.5g Trigger: Whey, cottage cheese, chicken, Greek yogurt, and salmon effortlessly clear the target leucine threshold within a standard 30g protein serving.
The Plant Fix: For lower-scoring plant sources like tofu and lentils, simply bump your meal target up to 35–40g of total protein to make up the leucine deficit.
At each main meal, aim for a protein source that delivers at least 2.5–3.5 g of leucine. Most servings of meat, fish, eggs, or dairy will achieve this if you're consuming 35–40 g of protein per meal. Plant-based eaters need larger portions or leucine supplementation.
Resistance Training: The Most Powerful Fix
If nutrition is one half of the equation, resistance training is the other — and arguably the more powerful half when it comes to reversing anabolic resistance.
Why Resistance Training Is Therapeutic, Not Optional
Mechanical loading of muscle does something no amount of dietary protein can do alone: it directly activates mTORC1 independently of amino acid availability. This means resistance training can partially restore anabolic signaling even before you've eaten a gram of protein.
Beyond mTORC1 activation, resistance training:
Sensitizes muscle to amino acids for 24–48 hours post-exercise — massively expanding the "anabolic window" beyond the 30-minute myth
Stimulates satellite cell activity — the stem cells of muscle tissue, essential for repair and growth
Reduces inflammageing by lowering circulating TNF-α, IL-6, and CRP
Restores GLUT4 translocation and insulin sensitivity — turning muscle back into a functioning metabolic sink for blood glucose
A 2023 study by Trommelen et al. published in Cell Reports Medicine demonstrated that the anabolic response to protein ingestion during recovery from exercise has no upper limit in magnitude or duration in healthy humans — a striking finding that underscores just how powerful the exercise–protein synergy is.
Resistance Training Prescription for Older Adults
Frequency: 2–3 sessions per week
Focus: Hit all major muscle groups across these sessions, allowing 48 hours of recovery between working the same muscles.
Intensity: 60–80% of 1-Rep Max (or RPE 6–8/10)
Focus: Work at a moderate-to-high effort where you finish each set feeling like you have 2–4 repetitions left in the tank.
Volume: 2–4 sets per exercise
Focus: This provides enough stimulus to trigger muscle growth and strength gains without causing excessive fatigue.
Rest Periods: 60–120 seconds between sets
Focus: Take closer to 60 seconds for smaller isolation moves (like curls) and closer to 120 seconds for heavy compound lifts (like squats).
Target Muscle Groups: All major groups
Focus: Ensure balanced development by targeting the legs, back, chest, shoulders, and arms.
Progression: Increase load or reps every 1–2 weeks
Focus: Apply progressive overload. Once you can easily hit the top end of your rep range, slightly increase the weight or add a repetition.
Progressive overload is non-negotiable. Your muscles adapt to the stimulus you give them. Doing the same weight with the same reps indefinitely is maintenance, not growth. Even small weekly progressions accumulate into significant strength and muscle gains over months.
Is It Too Late to Start?
Absolutely not. Pérez-Castillo et al. (2025) reviewed evidence showing that previously sedentary older adults — including those in their 70s and 80s — achieve significant gains in muscle mass, strength, and functional ability with progressive resistance training. Life-long exercisers do show advantages in preserved anabolic machinery, but the benefits of starting resistance training at any age are substantial and well-documented.
Combining Resistance and Cardio
Aerobic exercise (walking, cycling, swimming) provides complementary benefits through improved cardiovascular health, mitochondrial function, and insulin sensitivity. The emerging model of concurrent training — combining resistance and cardiovascular exercise — is well-supported, though the sequence matters: resistance training before cardio in the same session generally better preserves the muscle anabolic signal (Pérez-Castillo et al., 2025).
Supplements That Actually Help
The supplement market is flooded with products that overpromise and underdeliver. For anabolic resistance specifically, a short list of supplements has genuinely solid evidence behind it.
1. Creatine Monohydrate ⭐⭐⭐⭐⭐
Creatine is among the most rigorously studied supplements in sports and exercise science. For older adults specifically:
Augments the effects of resistance training on muscle mass and strength
Improves high-intensity exercise capacity, enabling more productive training
May have independent effects on muscle protein synthesis
Outstanding safety profile across decades of research
Dose: 3–5 g/day of creatine monohydrate (no loading phase necessary). Take with a meal containing carbohydrate and protein.
2. Omega-3 Fatty Acids (EPA/DHA) ⭐⭐⭐⭐
Evidence suggests that omega-3 supplementation can reduce anabolic resistance by enhancing muscle cell membrane fluidity and improving sensitivity to both amino acids and insulin. This is not a direct muscle builder but rather an anabolic sensitiser — making your muscles more receptive to the protein you're already eating.
Dose: 2–4 g/day of combined EPA + DHA from fish oil. Take with meals.
3. Leucine / Essential Amino Acids (EAAs) ⭐⭐⭐
When whole-food protein intake is inadequate — or for plant-based eaters who struggle to reach the leucine threshold — leucine supplementation or a full EAA supplement can bridge the gap.
Dose: 2.5–3 g of leucine supplemented around meals if needed; or a full EAA supplement containing ~3 g of leucine alongside meals.
4. Vitamin D ⭐⭐⭐
Deficiency is widespread in adults over 50 and is directly associated with impaired muscle function, reduced MPS, and increased sarcopenia risk. Vitamin D receptors are present in muscle tissue; adequate levels are necessary for optimal muscle response to exercise.
Dose: 1,000–2,000 IU/day (or as directed based on blood 25(OH)D levels). Supplement if you are deficient — discuss target levels with your doctor.
5. Protein Supplements (Whey, Casein, Pea) ⭐⭐⭐⭐
Not a replacement for whole food, but a valuable tool when meeting per-meal protein targets is difficult. Whey is fast-absorbing and high in leucine — ideal post-exercise. Casein is slow-absorbing — useful before bed to support overnight MPS. For plant-based individuals, pea protein isolate is the highest-quality option.
Anti-Inflammatory Lifestyle Strategies
Inflammageing is a direct upstream driver of anabolic resistance. Reducing chronic low-grade inflammation is not a soft lifestyle suggestion — it is a core therapeutic strategy.
Dietary Pattern
A Mediterranean-style diet — rich in vegetables, fruits, legumes, whole grains, fish, olive oil, and nuts — has the strongest anti-inflammatory evidence base of any dietary pattern. It is also associated with better muscle mass preservation in aging populations.
Key anti-inflammatory foods to prioritize:
Oily fish (salmon, sardines, mackerel) — omega-3s
Berries and cherries — anthocyanins, antioxidants
Leafy greens (spinach, kale) — magnesium, antioxidants
Extra virgin olive oil — oleocanthal (COX inhibitor)
Turmeric/curcumin — NF-κB inhibition
Green tea — EGCG, antioxidants
Foods to limit:
Ultra-processed foods
Refined seed oils (high omega-6)
Added sugars
Excessive alcohol
Sleep Quality
Poor sleep — even a single night — significantly elevates inflammatory markers and suppresses anabolic hormones including testosterone and IGF-1. Consistently sleeping 7–9 hours per night is a genuine metabolic intervention, not a luxury.
Stress Management
Chronic psychological stress elevates cortisol, which promotes muscle protein breakdown and blunts anabolic signaling. Mindfulness, social connection, time outdoors, and stress reduction practices directly support the anabolic environment in muscle tissue.
The Gut–Muscle Axis: A Frontier Worth Watching
The relationship between gut microbiome health and skeletal muscle function — the gut–muscle axis — is one of the most rapidly evolving areas of sarcopenia research.
Age-related changes in gut microbial composition (reduced Lactobacillus and Bifidobacterium species, increased pathobionts) may contribute to anabolic resistance through several pathways:
Reduced protein digestion efficiency
Altered amino acid bioavailability
Increased intestinal permeability (leading to systemic inflammation)
Impaired short-chain fatty acid production (affecting muscle metabolism)
A 2025 systems modeling study by McColl et al. (bioRxiv) identified gut microbiome composition as one of several interconnected factors in the multifactorial pathophysiology of anabolic resistance.
Practical implications: Supporting gut health through dietary fiber, fermented foods (yogurt, kefir, kimchi), and minimizing antibiotic use where possible may contribute — at the margin — to better amino acid bioavailability and reduced systemic inflammation.
This is a rapidly evolving space; targeted microbiome interventions for muscle health are likely to emerge in the coming years.
Evidence Summary: Study Comparison Table
Hettiarachchi et al. (2024) | Systematic Review & Meta-Analysis
Finding: Older adults require higher per-meal doses (35–40g of protein) to reliably trigger muscle protein synthesis (MPS). An even distribution of this protein across meals is vastly superior to backloading it at dinner.
Relevance: Establishes standard guidelines for optimal meal-by-meal protein dosing and distribution.
Deane et al. (2024) | Critical Review
Finding: Pinpoints the ideal leucine threshold at 2.5–3.5g per meal. Highlights that aging increases splanchnic sequestration—meaning the gut and liver trap more amino acids, preventing them from reaching peripheral muscles.
Relevance: Maps the exact leucine requirements and identifies the physical gut barriers that cause anabolic resistance.
Horwath et al. (2025) | Cross-Sectional Trial (Lean Older Men)
Finding: Older men who successfully preserved their muscle sensitivity showed significantly higher expression of Sestrin2 and GATOR2 (the cellular mechanisms responsible for sensing amino acids).
Relevance: Identifies a precise cellular and genetic target for physical and medical interventions against muscle wasting.
Pérez-Castillo et al. (2025) | Narrative Review
Finding: Lifelong exercisers exhibit a highly attenuated (reduced) level of anabolic resistance. The absolute most effective strategy to preserve muscle is a combined protocol of resistance training + optimal protein intake.
Relevance: Highlights the critical role of exercise history and mechanical tension in maintaining protein sensitivity.
Trommelen et al. (2023) | In Vivo Human Trial
Finding: Discovers that the anabolic response to protein ingested during exercise recovery has no upper limit in magnitude or duration.
Relevance: Upends old sports nutrition dogmas; proves that post-exercise protein synergy allows the body to efficiently utilize massive single doses of protein.
Kristiansen et al. (2026) | Systematic Review & Meta-Analysis
Finding: Confirms that age-related MPS blunting is a day-long issue. Specifically identifies post-absorptive periods (the fasting windows between meals) as high-risk vulnerability zones for accelerated muscle loss.
Relevance: Emphasizes the importance of meal frequency to protect against inter-meal muscle catabolism (breakdown).
McColl et al. (2025) | Systems Modeling Preprint
Finding: Demonstrates that anabolic resistance is a complex, multifactorial web where the gut microbiome, low-grade systemic inflammation, hormone sensitivity, and mTORC1 signaling all interact.
Relevance: Shifts the paradigm toward a holistic systems approach to muscle health rather than just counting daily protein grams.
Note: The McColl et al. (2025) paper is a preprint and has not yet completed formal peer review at the time of writing.
Common Myths & Mistakes
Myth 1: "I just need to eat more protein."
Reality: Protein quantity matters, but type, leucine content, distribution, and combination with exercise determine whether that protein actually reaches muscle. Eating 120 g of protein all at dinner is far less effective than 40 g at three meals.
Myth 2: "The anabolic window is 30 minutes post-workout."
Reality: Research has consistently shown that resistance training sensitizes muscle to amino acids for 24–48 hours post-exercise (Pérez-Castillo et al., 2025). While consuming protein near training is sensible, the obsession with a narrow post-workout window is not supported by current evidence for older adults. Overall daily protein intake and distribution matter more.
Myth 3: "Muscle loss after 50 is inevitable."
Reality: While anabolic resistance is a real biological shift, it is modifiable. Studies in adults in their 70s and 80s consistently show significant muscle and strength gains with resistance training and optimized protein intake. The trajectory is not fixed.
Myth 4: "Plant protein is just as good as animal protein."
Reality: Plant proteins can absolutely support muscle health — but not gram-for-gram equally in older adults. Lower leucine density and reduced bioavailability mean plant-based eaters generally need to consume more total protein and may benefit from leucine supplementation to overcome the higher anabolic threshold.
Myth 5: "Creatine is for young bodybuilders."
Reality: Creatine monohydrate has some of its strongest evidence in older adults. It augments resistance training adaptations, supports muscle mass retention, and has an excellent long-term safety record. It is arguably more relevant for a 65-year-old trying to preserve independence than for a 25-year-old optimizing aesthetics.
Myth 6: "I need to go to a gym to do resistance training."
Reality: Bodyweight exercises (squats, lunges, push-ups, rows with a resistance band) performed progressively can produce meaningful muscle and strength adaptations — particularly for previously inactive older adults. A gym provides more tools, but it is not a requirement for getting started.
Mistake: Skimping on Breakfast Protein
Many older adults eat the least protein at breakfast — the meal after the longest overnight fast, when muscles are in their most catabolic state. A high-protein breakfast (30–40 g) is one of the highest-leverage nutrition habits for muscle preservation.
Your 7-Day Muscle Preservation Protocol
This is a practical framework, not a rigid prescription. Adapt it to your food preferences, activity level, and any health conditions. Always consult your physician before making significant dietary or exercise changes.
Daily Nutrition Framework
Breakfast | Target: 30–40 g
Example: 3 whole eggs + 200g Greek yogurt + a handful of nuts.
Lunch | Target: 30–40 g
Example: 150g chicken breast + a mixed legume salad + drizzle of olive oil.
Pre/Post Training Snack | Target: 20–30 g
Example: 1 scoop of whey protein shake OR a serving of cottage cheese.
Dinner | Target: 30–40 g
Example: 180g salmon fillet + mixed vegetables + a side of quinoa.
Pre-Bed (Optional) | Target: 20–30 g
Example: 150g cottage cheese (ideal for providing slow-release casein protein overnight).
Why This Setup Works
Hits the Leucine Trigger: By keeping your main meals in the 30–40g range, you successfully clear the threshold required to signal muscle repair and growth.
Day-Long Protection: Spacing these meals out prevents long fasting windows, protecting your muscles from breakdown between breakfast and dinner.Daily Total: ~130–180 g protein (adjust for your body weight, targeting 1.2–1.6 g/kg)
Weekly Training Framework
Monday: Resistance Training (Lower Body Focus)
Goal: Build strength, power, and muscle mass in the legs, glutes, and core.
Tuesday: Light Cardio & Conditioning
Goal: 30–45 minutes of walking or steady-state light cardio to promote blood flow and active recovery.
Wednesday: Resistance Training (Upper Body Focus)
Goal: Build strength and structure in the chest, back, shoulders, and arms.
Thursday: Active Recovery & Mobility
Goal: Low-intensity movement like stretching, yoga, or a light walk to relieve muscle stiffness and improve flexibility.
Friday: Resistance Training (Full Body / Functional Focus)
Goal: Integrate the whole body with compound or functional movements to improve overall athletic performance and strength.
Saturday: Aerobic Conditioning (Activity of Choice)
Goal: Improve cardiovascular health through an enjoyable activity like cycling, swimming, running, or hiking.
Sunday: Rest & Recharge
Goal: Full physical rest or a casual, light walk to mentally and physically reset for the upcoming week.
Daily Supplement Checklist
☐ Creatine monohydrate: 5 g with breakfast
☐ Fish oil (omega-3): 2–4 g with a meal
☐ Vitamin D: 1,000–2,000 IU (if deficient; confirm with blood test)
☐ Leucine/EAA supplement if plant-based or struggling to reach protein targets
Lifestyle Checklist
☐ 7–9 hours of sleep per night
☐ At least 8,000 steps per day (non-exercise physical activity)
☐ Daily fruit and vegetables (anti-inflammatory micronutrients)
☐ Limit ultra-processed foods to < 20% of total intake
☐ Alcohol within recommended limits (or less)
FAQs
Q1: What is anabolic resistance and how does it differ from normal aging?
Anabolic resistance is a specific, measurable decline in the muscle's ability to respond to protein and exercise signals — it's not the same as simply getting weaker with age. Normal aging involves some degree of muscle loss, but anabolic resistance describes a cellular signaling failure: the mTORC1 pathway doesn't activate as strongly, amino acid sensors are less sensitive, and inflammatory signals interfere with repair. The significance is that it's a targetable mechanism — not just an inevitable aging process.
Q2: How much protein per day should a 60-year-old eat to preserve muscle?
Current evidence supports 1.2–1.6 g of protein per kilogram of body weight per day for adults over 50 who want to maintain or build muscle. For a 70 kg (154 lb) person, this means approximately 85–112 g of protein per day. This should be distributed evenly across three to four meals — approximately 30–40 g per meal — rather than concentrated in one sitting (Hettiarachchi et al., 2024).
Q3: Is whey protein or whole food better for overcoming anabolic resistance?
Both are effective, and ideally you prioritize whole food sources. However, whey protein has a particularly high leucine content and rapid absorption rate, making it a useful tool post-exercise when a whole-food meal isn't immediately practical. For older adults who struggle to consume sufficient protein through food alone, whey (or another high-quality protein supplement) can be a valuable addition.
Q4: Can I overcome anabolic resistance without lifting weights?
Resistance training is the most effective single intervention against anabolic resistance and sarcopenia. Optimizing protein intake alone will slow muscle loss, but it cannot replicate the direct mTORC1 activation, insulin-sensitizing effects, and satellite cell stimulation that resistance exercise provides. Walking and aerobic activity are valuable, but they are not substitutes for mechanical loading. Even bodyweight exercise (squats, push-ups, resistance bands) counts as resistance training.
Q5: When should I eat protein relative to my workout?
Within 1–2 hours of your resistance training session is sensible. However, current evidence indicates that for older adults, the total daily protein intake and its even distribution across meals matters more than hitting a precise post-workout window. The post-exercise period of enhanced amino acid sensitivity lasts 24–48 hours — so every meal on training days (and the days following) represents an anabolic opportunity (Pérez-Castillo et al., 2025; Trommelen et al., 2023).
Q6: Are plant-based proteins sufficient for older adults with anabolic resistance?
Yes, but with modifications. Plant proteins are typically lower in leucine and bioavailability than animal proteins. To overcome anabolic resistance on a plant-based diet, you should: (a) increase total protein intake by 20–30% above standard recommendations; (b) prioritize leucine-rich plant proteins like soy, edamame, and tempeh; (c) strategically combine protein sources (e.g., soy + wheat) to improve amino acid profiles; and (d) consider leucine or EAA supplementation around meals (Deane et al., 2024).
Q7: What role does sleep play in muscle preservation after 50?
A significant one. Sleep is when the majority of growth hormone secretion occurs, and it's when muscle repair and protein synthesis are prioritized by the body. Poor or insufficient sleep elevates cortisol (catabolic), suppresses testosterone and IGF-1 (anabolic hormones), and increases systemic inflammation — all of which worsen anabolic resistance. Seven to nine hours of quality sleep per night is a genuine component of any muscle preservation strategy.
Q8: Is it worth testing for hormonal deficiencies if I suspect anabolic resistance?
Yes, it's worth discussing with your physician. While hormone replacement therapy has specific clinical indications and is not appropriate for everyone, identifying and treating clinically significant testosterone deficiency, hypothyroidism, or vitamin D deficiency can meaningfully improve the anabolic environment in muscle tissue. A basic blood panel including testosterone (in men), 25(OH)D (vitamin D), thyroid function, and fasting insulin/glucose is a reasonable starting point.
Q9: Can I reverse anabolic resistance if I've been sedentary for years?
Absolutely. The evidence is clear that previously sedentary older adults — including those in their 70s and 80s — achieve significant and meaningful gains in muscle mass, strength, and functional independence with progressive resistance training combined with adequate protein intake. Starting later means you have more to gain, not less. The biology of muscle adaptation does not have an expiration date (Pérez-Castillo et al., 2025).
Q10: How long does it take to see results when fighting anabolic resistance?
Measurable strength improvements typically begin within 4–6 weeks of consistent resistance training — driven initially more by neural adaptations (your nervous system becoming more efficient) than actual muscle growth. Significant changes in muscle mass typically become measurable at 8–16 weeks with consistent training and protein optimization. The process is slower than in younger adults, but it is real and cumulative. Consistency across months and years is what produces transformative results.
Q11: Does HMB (beta-hydroxy beta-methylbutyrate) help with anabolic resistance?
HMB — a metabolite of leucine — has shown some benefit specifically in frail older adults or those with very low protein intake, where it may partially substitute for the leucine threshold trigger. However, evidence is less consistent than for creatine or omega-3s, and it is generally considered a second-line option. It may be most appropriate for older adults who are struggling with appetite or significant illness-related muscle loss.
Q12: Is anabolic resistance the same as sarcopenic obesity?
Not exactly, but they're closely related. Sarcopenic obesity describes the combination of low muscle mass and high fat mass — increasingly common with aging. Anabolic resistance is a key driver of the muscle loss component of sarcopenic obesity. People with sarcopenic obesity often have higher degrees of systemic inflammation and insulin resistance, which worsen anabolic resistance — creating a vicious cycle where muscle loss and metabolic dysfunction reinforce each other (Pérez-Castillo et al., 2025).
Conclusion & Action Steps
The evidence is unambiguous: muscle loss after 50 is not simply something that happens to you. It is driven by a specific, well-characterized biological process — anabolic resistance — and that process is modifiable.
The key shifts you need to make are not dramatic. They are consistent:
1. Increase and redistribute your protein. Aim for 1.2–1.6 g/kg/day, 30–40 g per meal, prioritizing leucine-rich sources at every sitting — including breakfast.
2. Resistance train, progressively, at least twice a week. This is not optional. It is the most powerful intervention available for restoring muscle's anabolic sensitivity and maintaining metabolic health.
3. Address the inflammatory environment. Poor sleep, chronic stress, and a highly processed diet are not peripheral lifestyle factors — they are active drivers of muscle breakdown. Addressing them is part of the intervention.
4. Consider targeted supplementation. Creatine monohydrate and omega-3 fatty acids have the strongest evidence base for older adults and are appropriate to discuss with your healthcare provider.
5. Start now. The research shows that the benefits of resistance training and protein optimization are available at every age. There is no threshold beyond which these interventions stop working. The biology of adaptation is remarkably persistent.
Anabolic resistance is modifiable. Your muscles are more capable of responding — and rebuilding — than you may have been led to believe.
Author’s Note
As a clinician, I have seen a recurring pattern in practice: patients doing “everything right”—eating reasonably well, staying moderately active—yet experiencing a steady decline in muscle strength, energy, and metabolic health after midlife. For years, this was often dismissed as an unavoidable consequence of aging.
The science now tells a very different story.
The concept of anabolic resistance has fundamentally reshaped our understanding of age-related muscle loss. What appears clinically as weakness or frailty is, at a deeper level, a failure of biological signaling—a reduced responsiveness of skeletal muscle to nutrition and exercise. This distinction matters, because it transforms sarcopenia from an inevitable process into a modifiable, treatable condition.
This article was written with two parallel audiences in mind:
Clinicians and health professionals, who need a mechanistic and evidence-based framework to guide intervention
Patients and informed readers, who deserve clear, actionable strategies grounded in real science—not oversimplified advice
Every recommendation presented here reflects current peer-reviewed evidence, particularly in areas such as mTORC1 signaling, leucine thresholds, protein distribution, and resistance training as anabolic therapy. However, it is equally important to recognize that responses to these interventions vary based on genetics, baseline fitness, metabolic health, and lifestyle history.
The most important message I want readers to take away is this:
muscle loss with aging is not inevitable—and it is not irreversible.
With the right combination of targeted nutrition, progressive resistance training, and metabolic optimization, it is possible not only to slow decline but to meaningfully restore strength, function, and independence—even in later decades of life.
This article is for informational and educational purposes only and does not constitute medical advice. Consult your physician, registered dietitian, or physiotherapist before making significant changes to your diet or exercise programme, particularly if you have existing health conditions or take medications.
Consult a specialist: If you are over 60 and experiencing unexplained muscle weakness, difficulty performing daily activities, or rapid unintentional weight loss, discuss sarcopenia screening with your physician. Early, targeted intervention produces the best outcomes.
Related Articles
SARMs vs Anabolic Steroids: Are They Really Safer? Benefits, Risks, and Clinical Evidence
Why Protein After 55 Isn’t Optional — The Science Behind Why the RDA Is Too Low | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
No Time to Train? Science-Backed Workouts That Deliver | DR T S DIDWAL
References
Deane, C. S., Cox, J., & Atherton, P. J. (2024). Critical variables regulating age-related anabolic responses to protein nutrition in skeletal muscle. Frontiers in Nutrition, 11, Article 1419229. https://doi.org/10.3389/fnut.2024.1419229
Hettiarachchi, J., Reijnierse, E. M., Kew, N., Fetterplace, K., Tan, S.-Y., & Maier, A. D. (2024). The effect of dose, frequency, and timing of protein supplementation on muscle mass in older adults: A systematic review and meta-analysis. Ageing Research Reviews, 99, Article 102325. https://doi.org/10.1016/j.arr.2024.102325
Horwath, O., Moberg, M., Hodson, N., Edman, S., Johansson, M., Andersson, E., van Hall, G., Rooyackers, O., Philp, A., & Apró, W. (2025). Anabolic sensitivity in healthy, lean, older men is associated with higher expression of amino acid sensors and mTORC1 activators compared to young. Journal of Cachexia, Sarcopenia and Muscle, 16, Article e13613. https://doi.org/10.1002/jcsm.13613
Kristiansen, J. B., Vissing, K., & Nielsen, J. L. (2026). Age-related anabolic resistance and post-absorptive muscle protein synthesis: integrative evidence from a systematic review and meta-analysis. Frontiers in Physiology, 17, 1740284. https://doi.org/10.3389/fphys.2026.1740284
McColl, T. J., Moore, D. R., Emberly, E., Church, D. D., & Clarke, D. C. (2025). Exploring the multifactorial causes and therapeutic strategies for anabolic resistance in sarcopenia: A systems modeling study [Preprint]. bioRxiv. https://doi.org/10.1101/2025.09.12.675977
Pérez-Castillo, Í. M., Rueda, R., Pereira, S. L., Bouzamondo, H., López-Chicharro, J., Segura-Ortiz, F., & Atherton, P. J. (2025). Age-related anabolic resistance: Nutritional and exercise strategies, and potential relevance to life-long exercisers. Nutrients, 17(22), Article 3503. https://doi.org/10.3390/nu17223503
Trommelen, J., van Lieshout, G. A. A., Nyakayiru, J., Holwerda, A. M., Smeets, J. S. J., Hendriks, F. K., & van Loon, L. J. C. (2023). The anabolic response to protein ingestion during recovery from exercise has no upper limit in magnitude and duration in vivo in humans. Cell Reports Medicine, 4(12), Article 101324. https://doi.org/10.1016/j.xcrm.2023.101324
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., ... & Zamboni, M. (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Moore, D. R., Robinson, M. J., Fry, J. L., Tang, J. E., Glover, E. I., Wilkinson, S. B., ... & Phillips, S. M. (2009). Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. American Journal of Clinical Nutrition, 89(1), 161–168. https://doi.org/10.3945/ajcn.2008.26401
Burd, N. A., Gorissen, S. H., van Vliet, S., Snijders, T., & van Loon, L. J. C. (2015). Differences in postprandial protein handling after beef compared with milk ingestion during postexercise recovery: A randomized controlled trial. American Journal of Clinical Nutrition, 102(4), 828–836. https://doi.org/10.3945/ajcn.114.103184
Smith, G. I., Atherton, P., Reeds, D. N., Mohammed, B. S., Rankin, D., Rennie, M. J., & Mittendorfer, B. (2011). Omega-3 polyunsaturated fatty acids augment the muscle protein anabolic response to hyperaminoacidemia–hyperinsulinemia in healthy young and middle aged men and women. Clinical Science, 121(6), 267–278. https://doi.org/10.1042/CS20100597
Landi, F., Calvani, R., Tosato, M., Martone, A. M., Ortolani, E., Savera, G., ... & Marzetti, E. (2016). Protein intake and muscle health in old age: From biological plausibility to clinical evidence. Nutrients, 8(5), 295. https://doi.org/10.3390/nu8050295
Churchward-Venne, T. A., Burd, N. A., Mitchell, C. J., West, D. W. D., Philp, A., Marcotte, G. R., ... & Phillips, S. M. (2012). Supplementation of a suboptimal protein dose with leucine or essential amino acids: Effects on myofibrillar protein synthesis at rest and following resistance exercise in men. Journal of Physiology, 590(11), 2751–2765. https://doi.org/10.1113/jphysiol.2012.228833
Bhasin, S., Apovian, C. M., Travison, T. G., Pencina, K., Moore, L. L., Huang, G., ... & Storer, T. W. (2018). Effect of protein intake on lean body mass in functionally limited older men: A randomized clinical trial. JAMA Internal Medicine, 178(4), 530–541. https://doi.org/10.1001/jamainternmed.2018.0008
Stout, J. R., Fukuda, D. H., Kendall, K. L., Smith-Ryan, A. E., Moon, J. R., & Hoffman, J. R. (2015). Effect of creatine supplementation on measures of sarcopenia in older adults: A narrative review. Journal of Cachexia, Sarcopenia and Muscle, 6(3), 200–207. https://doi.org/10.1002/jcsm.12050