Why Protein After 55 Isn’t Optional — The Science Behind Why the RDA Is Too Low
Discover why adults over 55 need more protein than the RDA. Learn how higher intake supports muscle mass, metabolism, and healthy aging.
NUTRITIONSARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/8/202620 min read
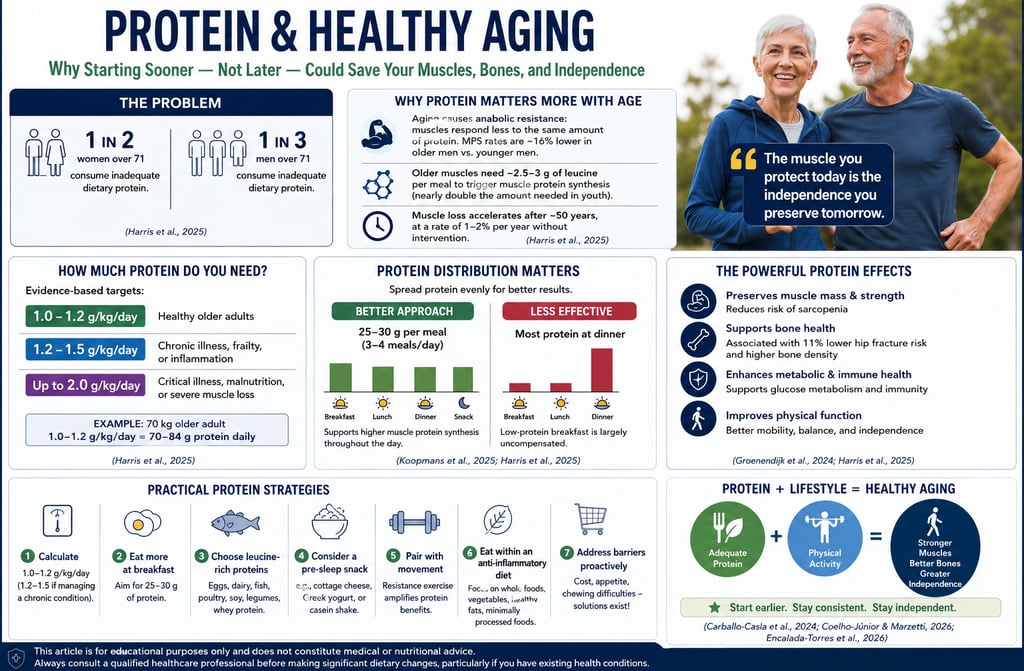
Most adults over 55 are not consuming enough protein to maintain muscle mass, bone strength, metabolic health, and physical independence as they age (Harris et al., 2025; Koopmans et al., 2025). Emerging evidence shows that aging muscles become progressively less responsive to dietary protein due to a biological process known as anabolic resistance, meaning older adults require both higher-quality protein and higher total protein intake to stimulate muscle protein synthesis effectively (Harris et al., 2025).
Current research suggests that the long-standing Recommended Dietary Allowance (RDA) of 0.8 g/kg/day is likely inadequate for healthy aging (Groenendijk et al., 2024; Harris et al., 2025). Evidence-based recommendations now support:
1.0–1.2 g/kg/day for healthy older adults
1.2–1.5 g/kg/day for individuals with chronic disease, inflammation, or frailty (Harris et al., 2025)
Higher protein intake in older adults has been associated with:
Reduced sarcopenia risk
Improved muscle strength and mobility
Better bone mineral density
Lower fracture risk
Enhanced metabolic and immune function (Groenendijk et al., 2024; Harris et al., 2025)
Research also demonstrates that protein timing and distribution matter significantly. Older adults achieve better muscle protein synthesis when protein intake is evenly distributed across meals rather than concentrated at dinner (Koopmans et al., 2025). Most experts recommend consuming approximately 25–30 grams of protein per meal, ideally from leucine-rich sources such as eggs, dairy, fish, poultry, soy, legumes, and whey protein (Harris et al., 2025).
Resistance exercise further amplifies the anabolic effects of dietary protein. Even modest strength training or walking can improve skeletal muscle sensitivity to amino acids for up to 24–48 hours after exercise (Harris et al., 2025; Encalada-Torres et al., 2026). Studies consistently show that the combination of adequate protein intake and physical activity produces superior functional outcomes compared with either strategy alone (Encalada-Torres et al., 2026).
Importantly, newer evidence suggests that protein optimization should begin before old age develops. Carballo-Casla et al. (2024) argue that the protective effects of higher protein intake accumulate over decades, making midlife an important window for preserving long-term muscle and metabolic resilience.
Emerging research also highlights that protein quality is strongly influenced by overall dietary patterns. Protein consumed within a Mediterranean-style, anti-inflammatory dietary pattern rich in vegetables, whole grains, olive oil, and minimally processed foods appears to produce better aging-related outcomes than equivalent protein intake within ultra-processed dietary patterns (Coelho-Júnior & Marzetti, 2026).
Key Takeaways
Aging muscles require more dietary protein because of anabolic resistance (Harris et al., 2025)
The current protein RDA may be insufficient for healthy aging (Groenendijk et al., 2024)
Older adults benefit from spreading protein evenly across meals (Koopmans et al., 2025)
Leucine-rich proteins are especially effective for stimulating muscle protein synthesis (Harris et al., 2025)
Resistance exercise substantially enhances the muscle-preserving effects of protein (Encalada-Torres et al., 2026)
Starting higher protein intake earlier in adulthood may help preserve long-term independence and physical function (Carballo-Casla et al., 2024)
How much protein should adults over 60 consume daily?
Most healthy older adults benefit from approximately 1.0–1.2 g/kg/day, while those with chronic disease or frailty may require 1.2–1.5 g/kg/day (Harris et al., 2025).
What are the best protein sources for older adults?
High-quality protein sources include eggs, Greek yoghurt, cottage cheese, fish, poultry, soy foods, lentils, and whey protein because they provide essential amino acids and leucine needed for muscle maintenance (Harris et al., 2025).
Can protein help prevent age-related muscle loss?
Yes. Higher protein intake combined with resistance exercise has been shown to preserve muscle mass, strength, mobility, and functional independence in older adults (Harris et al., 2025; Encalada-Torres et al., 2026).
Is a higher-protein diet safe for older adults?
For adults with normal kidney function, protein intakes within recommended ranges appear safe and beneficial. Individuals with chronic kidney disease should seek individualized medical advice before increasing protein intake (Harris et al., 2025).
Why is protein distribution across meals important?
Older muscles respond more effectively when protein is distributed evenly across three to four meals rather than heavily concentrated in one evening meal (Koopmans et al., 2025).
Why Protein Is the Single Most Important Nutrient After 55 — And How Most Older Adults Are Still Getting It Wrong
Here is a number that should give everyone pause: 30% of men and 50% of women over the age of 71 in the United States consume inadequate dietary protein (Harris et al., 2025). This is not a marginal shortfall — this is half of older women eating insufficiently to support the basic biological functions that keep their bodies functioning well.
The problem is compounded by the fact that aging itself fundamentally changes how your body processes protein. As you grow older, a phenomenon called anabolic resistance means that your muscles respond less efficiently to the protein you eat (Harris et al., 2025). In practical terms, this means that even if you are eating the same amount of protein you ate at 40, you may be getting significantly less benefit from it at 70. Research has quantified this blunted response: postprandial muscle protein synthesis (MPS) rates in older men are approximately 16% lower than in younger men after the same meal (Harris et al., 2025).
This is not just a matter of physical appearance or athletic performance. Muscle loss — clinically known as sarcopenia — is directly linked to increased fall risk, fractures, functional decline, loss of independence, and, critically, all-cause mortality. Research consistently shows that muscular strength is inversely associated with death from cancer and other causes, making muscle maintenance in older adults a matter of life and death (Harris et al., 2025).
Why the Standard RDA Is Not Enough for You
The current Recommended Dietary Allowance (RDA) for protein in the United States is 0.8 grams per kilogram of body weight per day — a figure that applies to healthy adults across the board. But the evidence strongly suggests this threshold is simply too low for adults over 65.
According to Harris et al. (2025), the scientific literature supports the following updated targets for older adults:
1.0–1.2 g/kg/day for healthy older adults to maintain muscle mass and support immune function
1.2–1.5 g/kg/day for older adults living with chronic illness, acute health events, frailty risk, or inflammatory conditions
Up to 2.0 g/kg/day in severe cases of malnutrition, critical illness, or significant muscle loss
These recommendations align closely with guidance from the European Society for Clinical Nutrition and Metabolism (ESPEN), which specifies 1.0–1.2 g/kg/day for healthy older adults and 1.2–1.5 g/kg/day for those with acute or chronic disease (Harris et al., 2025). It is worth noting that the European Food Safety Authority still aligns with the 0.83 g/kg/day population reference intake for all adults, which underscores the ongoing debate in the field — and why updated, individualised guidance is essential.
To put these numbers into everyday terms: a 70-kilogram (154-pound) healthy older adult should aim for roughly 70–84 grams of protein per day, rising to 84–105 grams per day if managing a chronic condition. For context, a single chicken breast provides about 30–35 grams of protein, and a large egg provides around 6 grams.
Protein, Muscles, and Bones: The Inextricable Link
One of the most compelling insights from recent research is that muscle health and bone health are not separate concerns — they are deeply intertwined, and protein is the common thread.
Groenendijk and colleagues (2024) at Wageningen University and the University of Copenhagen conducted a thorough mini-review examining the evidence for protein recommendations specifically for supporting both muscle and bone health in older adults. Their analysis drew on a prior systematic review and meta-analysis showing that a higher protein intake was associated with a significant 11% reduction in hip fractures among older adults. More striking still, one observational study included in their analysis found that older adults with higher protein intake (approximately 1.1 g/kg/day) had 1.8% higher mean hip BMD and 6.0% higher lumbar spine BMD at baseline compared to those eating closer to the RDA (Groenendijk et al., 2024).
Furthermore, research reviewed by Groenendijk et al. (2024) reported that a higher protein intake group had a 64% reduced risk of vertebral fractures during a five-year follow-up — a finding with enormous implications for quality of life in older adults.
The biological mechanism here is straightforward: muscles exert mechanical force on bones through everyday movement, and that loading signal is what stimulates bones to remain dense and strong. When muscles weaken from sarcopenia, bones lose that stimulus. Dietary protein supports both tissues simultaneously — providing the amino acid building blocks for muscle protein synthesis while also supporting bone mineralization through pathways involving insulin-like growth factor 1 (IGF-1) and calcium absorption (Harris et al., 2025; Groenendijk et al., 2024).
Groenendijk et al. (2024) conclude that a protein intake above the current population reference intake is scientifically justified for older adults — a statement that should prompt every healthcare provider working with older patients to revisit their nutrition counselling.
What Real Older Adults Are Actually Eating
Theory is important, but what does protein intake actually look like in the real world of community-dwelling older adults? Koopmans et al. (2025) shed direct light on this question with one of the most robust real-world datasets available to date.
Their 2025 study in Clinical Nutrition pooled baseline data from eight separate intervention studies, harmonising information on protein intake across a large population of adults over 55. Participants were stratified into four groups based on their habitual protein intake: below 0.8 g/kg/day, 0.8–0.99 g/kg/day, 1.0–1.2 g/kg/day, and above 1.2 g/kg/day. The study found that many community-dwelling older adults are clustered in the lower intake groups — consuming protein at or below levels that scientific evidence suggests are insufficient to preserve muscle mass and prevent sarcopenia (Koopmans et al., 2025).
Crucially, Koopmans and colleagues also examined protein sources and distribution patterns, recognising that it is not just the total amount of protein that matters, but how it is distributed across the day and where it comes from. Their findings support a growing consensus that improving daily protein intake in older adults requires targeted strategies addressing both the quantity and the timing of protein consumption — not simply telling people to "eat more protein."
The Secret Weapon: When and How You Eat Your Protein
One of the most actionable insights from current research is that how you distribute your protein throughout the day matters enormously. Most older adults tend to front-load carbohydrates at breakfast and back-load protein at dinner — and this pattern may be actively working against their muscle health.
Harris et al. (2025) summarise findings from multiple studies showing that MPS rates were increased by up to 25% when protein intake was balanced across three meals compared to the same amount skewed toward later in the day. An even protein distribution also reduces whole-body protein breakdown — meaning that the protein you eat is used more efficiently when spread evenly, rather than arriving in one large evening bolus.
The practical target, according to the reviewed literature, is 25–30 grams of protein per meal (approximately 0.4 g/kg body weight per meal), consumed across three to four eating occasions per day. Only about 1% of older adults in one study ate more than 20 grams of protein per meal at every meal — highlighting a significant opportunity for improvement (Harris et al., 2025).
There is also emerging evidence for a surprising strategy: pre-sleep protein feeding. Research reviewed by Harris et al. (2025) found that consuming 40 grams of protein (particularly casein) before bed — in combination with resistance exercise — enhanced muscle protein synthesis during overnight rest compared to controls. This window, typically wasted metabolically, can be transformed into a period of muscle repair and growth with something as simple as a high-protein evening snack.
Animal vs. Plant Protein: The Nuanced Truth
Few nutrition topics generate more confusion among older adults than the animal-versus-plant protein debate. The honest answer, according to the most current evidence, is nuanced — and depends significantly on your age, health status, and overall dietary pattern.
Animal proteins have a clear advantage for muscle protein synthesis in older adults. Harris et al. (2025) cite research showing that older adults who consumed a beef-containing omnivorous meal had approximately 47% higher rates of postprandial MPS compared to those eating a vegan meal, along with a 25% higher rise in plasma leucine, the amino acid most critical for triggering the muscle-building response. Animal proteins are complete proteins, containing all essential amino acids in proportions that more closely match human muscle requirements. They also have higher bioavailability and naturally higher leucine content, which is especially important given older adults' reduced sensitivity to anabolic signals.
Plant proteins, however, offer unique advantages that cannot be ignored. Higher plant protein intake has been associated with improved physical performance in older women, lower saturated fat content, anti-inflammatory properties, and — critically — a significantly lower risk of chronic kidney disease (CKD). Research summarised by Harris et al. (2025) found that replacing one serving of red meat with plant-based protein sources was associated with a 50.4% drop in kidney failure risk — a staggering finding for older adults who are at elevated CKD risk.
For plant proteins specifically, not all sources are equally effective. Legumes (beans, lentils, chickpeas), nuts, and seeds demonstrated the strongest associations with higher grip strength and lower sarcopenia risk in older adults, while cereal-based and starchy plant proteins did not show the same benefits (Harris et al., 2025).
This complexity around plant-based protein choices among older adults was directly explored by van Oppenraaij and colleagues (2025) in a qualitative study published in Scientific Reports. Their focus group research with 30 Dutch adults aged 55–74 identified the real-world facilitators and barriers to adopting a protein-rich, predominantly plant-based diet. Participants mapped their experiences to themes including perceptions of protein needs, attitudes toward plant-based foods, social influences, taste, cost, and habits. The COM-B model was used to analyse the data, revealing that while many older adults were open to increasing plant protein intake, knowledge gaps about which foods are high in protein, concerns about taste, social eating dynamics, and habitual food preferences formed significant barriers (van Oppenraaij et al., 2025).
This research is timely because global health and climate policies increasingly recommend that adults obtain at least 60% of their dietary proteins from plant sources. For older adults specifically, achieving this target while still meeting the elevated protein requirements needed to prevent sarcopenia presents a real nutritional challenge that requires active guidance from healthcare professionals (van Oppenraaij et al., 2025).
The most evidence-based recommendation for most omnivorous older adults: pursue a mixed-protein diet that emphasises high-quality animal proteins such as fish, eggs, poultry, and dairy alongside generous servings of legumes, nuts, and seeds — while limiting red and processed meats due to their association with inflammation and CKD risk (Harris et al., 2025).
Overcoming the Real Barriers: Cost, Appetite, and Dentition
Understanding the science is one thing; the reality of older adults' lives is another. Harris et al. (2025) devote significant attention to the practical barriers that prevent adequate protein intake — and they are worth taking seriously.
Financial concerns are a real obstacle. Protein-rich foods make up an estimated 24–52% of food costs for American adults (depending on whether dairy and mixed dishes are included). However, research suggests cost-effective strategies: eggs have been identified as one of the most economical protein sources, and whole-grain products combined with eggs, legumes, and affordable cuts of meat can help older adults maximise their protein intake within a tight budget (Harris et al., 2025).
Appetite loss affects 15–30% of community-dwelling older adults, driven by changes in gut motility, taste, smell, dentition, social isolation, and medication side effects. Because high-protein foods tend to be satiating, older adults with poor appetite may avoid them in favour of easier-to-eat carbohydrate-heavy options. This is precisely why spreading protein across multiple smaller meals — rather than concentrating it in one large meal — is such a valuable strategy: it allows older adults to meet their protein targets without overwhelming their appetite at any single sitting.
Dental health poses a unique challenge. Approximately 17% of Americans aged 65 and older have lost all of their teeth, and tooth loss — even when dentures are worn — is associated with significant changes in dietary intake, including reduced protein consumption (Harris et al., 2025). For older adults with dentition concerns, softer protein sources such as eggs, yoghurt, cottage cheese, minced meat, fish, hummus, and legume-based soups can help bridge the gap.
Practical Applications: Your Action Plan
Based on the totality of the research reviewed here, the following practical strategies are supported by current evidence for older adults aiming to optimise their protein intake:
1. Know your target. For a healthy 70-year-old weighing 70 kg, the goal is approximately 70–84 grams of protein per day. If you are managing a chronic condition, aim for 84–105 grams. Consult a registered dietitian for personalised targets.
2. Spread protein evenly. Aim for 25–30 grams of protein at each of three to four meals or eating occasions. Begin by auditing your breakfast — most older adults eat almost no protein in the morning. Add eggs, Greek yoghurt, cottage cheese, or smoked salmon to your morning routine.
3. Try a pre-sleep protein snack. A high-protein evening snack of approximately 40 grams — such as casein-based protein powder, cottage cheese, or a combination of yoghurt and nuts — can support overnight muscle repair, particularly when paired with any physical activity earlier in the day.
4. Diversify your protein sources. Prioritise fish, eggs, dairy, and poultry from animal sources, and integrate lentils, chickpeas, edamame, tofu, almonds, and pumpkin seeds from plant sources. Minimise red and processed meats.
5. Make it affordable. Eggs, tinned fish (tuna, sardines, salmon), legumes (dried or canned), and low-fat dairy are among the most cost-effective protein sources available. A can of chickpeas costs less than most snack foods and delivers a meaningful protein boost.
6. Pair protein with resistance exercise. Even light resistance training — chair squats, resistance bands, or wall push-ups — dramatically amplifies the muscle-building response to dietary protein. The combination is synergistic and recommended by all major expert bodies.
7. Address oral health. If chewing is a barrier, prioritise soft-textured, high-protein foods. Speak with your dentist about optimising dental function — it directly impacts your nutritional status.
8. If you have kidney disease, get specialist guidance. Protein recommendations for those with CKD differ significantly from those for healthy older adults. Do not self-prescribe high protein intakes without medical supervision.
To put these points into practice, consider these three "golden rules" of geriatric nutrition:
The Per-Meal Minimum: Aim for at least 25–30g of protein at every major meal to effectively "trigger" muscle building.
The Breakfast Shift: Most people eat the least protein at breakfast. Swapping toast for eggs or Greek yogurt is often the easiest way to hit these higher daily targets.
The Bioavailability Factor: Prioritize "complete" proteins (eggs, dairy, fish, poultry) which contain the high leucine content necessary to stimulate muscle repair in older tissue.
Frequently Asked Questions About Protein and Aging
1. Is 0.8 g/kg/day of protein really not enough for older adults? For most adults over 65, no. The 0.8 g/kg/day RDA was established for the general adult population, and growing evidence supports higher intakes of 1.0–1.2 g/kg/day for healthy older adults to maintain muscle mass, support immune function, and preserve bone density. For those with illness or frailty, the target is even higher (Harris et al., 2025; Groenendijk et al., 2024).
2. Can I get enough protein from a plant-based diet as I get older? Yes, but it requires planning. Plant proteins tend to have lower bioavailability and less leucine than animal proteins, which matters more as you age due to anabolic resistance. Focus on legumes, soy products (tofu, edamame), nuts, and seeds; use protein complementation to ensure all essential amino acids are covered; and consider higher total quantities than an omnivore would need to achieve the same muscle-building stimulus (Harris et al., 2025; van Oppenraaij et al., 2025).
3. What is anabolic resistance, and why does it matter for my diet? Anabolic resistance is the reduced ability of aging muscle to respond to the protein you eat. It means that older adults need more protein per meal — roughly double the amount per kilogram of body weight compared to younger adults — to stimulate the same level of muscle protein synthesis. This is one of the key reasons why the RDA is considered insufficient for older populations (Harris et al., 2025).
4. Does the timing of protein intake actually matter? Yes. Research shows that distributing protein evenly across three to four meals can increase MPS rates compared to eating the same total amount skewed toward one meal. Starting with a protein-rich breakfast — rather than a carbohydrate-heavy one — is one of the simplest and most impactful changes older adults can make (Harris et al., 2025; Koopmans et al., 2025).
5. Is a high-protein diet bad for my kidneys? This depends on your kidney health. For older adults with normal kidney function, intakes of 1.0–1.5 g/kg/day appear to be safe and beneficial. For those with established chronic kidney disease (especially stages 3–5), lower protein targets may be recommended to slow disease progression. Always follow personalised guidance from your physician or dietitian (Harris et al., 2025).
6. What are the best high-protein foods for older adults who struggle with chewing? Eggs (scrambled, poached, or in omelettes), Greek yoghurt, cottage cheese, ricotta, soft fish (salmon, tuna, tilapia), smooth nut butters, hummus, lentil soup, tofu, and protein-enriched smoothies are all excellent choices that require minimal chewing while delivering meaningful amounts of protein.
7. How does protein help my immune system as I age? The aging immune system undergoes a progressive decline known as immunosenescence, which increases susceptibility to infections and reduces vaccine effectiveness. Protein provides the amino acid building blocks for immune cells: glutamine and leucine support T-cell proliferation; arginine enables pathogen destruction through nitric oxide production; and cysteine supports glutathione synthesis, a powerful antioxidant that protects immune cells. A low protein status can worsen immune responses — while adequate intake helps maintain the body's defences (Harris et al., 2025).
A Note on Kidney Disease and Other Conditions
If you are living with chronic kidney disease, heart failure, cancer, liver disease, or any other serious medical condition, it is essential to work with a qualified healthcare team before making significant changes to your protein intake. The evidence clearly shows that blanket high-protein recommendations do not apply universally — and that what is beneficial for a healthy older adult may require modification for someone managing complex medical conditions. Always seek personalised guidance.
Key Points
Aging is not the primary problem—under-fueling is.
What appears as “natural aging” is often a manifestation of chronic inadequate protein intake, compounded by anabolic resistance. Muscle loss is not inevitable; it is, in many cases, nutritionally mediated and therefore modifiable.Anabolic resistance changes the rules after midlife.
Aging muscle becomes less responsive to dietary protein due to impaired mTORC1 signaling, requiring a higher threshold of amino acids—especially leucine (~2.5–3 g per meal)—to stimulate muscle protein synthesis (Harris et al., 2025).The RDA is a survival minimum—not an optimal target.
The long-standing recommendation of 0.8 g/kg/day is insufficient for preserving muscle mass, bone density, and metabolic health in older adults. Evidence consistently supports 1.0–1.2 g/kg/day or higher, particularly in the presence of illness or frailty (Groenendijk et al., 2024).Inflammaging accelerates muscle breakdown.
Chronic low-grade inflammation—driven by cytokines such as IL-6 and TNF-α—blunts anabolic signaling and promotes catabolism, creating a physiological environment where muscle loss outpaces repair.Muscle is a metabolic organ, not just structural tissue.
Loss of skeletal muscle worsens insulin resistance, reduces glucose disposal, and accelerates cardiometabolic disease, making sarcopenia a central player in ageing-related morbidity.Distribution matters as much as total intake.
Skewed eating patterns—low-protein breakfasts and protein-heavy dinners—fail to optimally stimulate MPS. A balanced intake of 25–30 g protein per meal is critical for maximizing anabolic response.Real-world data reveal a systemic gap.
Large cohort analyses show that many older adults consume protein at or below inadequate levels, highlighting a widespread disconnect between evidence-based recommendations and actual intake patterns (Koopmans et al., 2025).The clinical takeaway is clear:
Optimizing protein intake is one of the most powerful, underutilized interventions in preventive medicine, capable of preserving strength, independence, and metabolic health well into advanced age.
.Clinical pearls
1. Overcoming "Anabolic Resistance"
The Science: Aging is characterized by a blunted muscle protein synthesis (MPS) response to dietary amino acids. Research shows older adults require roughly double the protein per kilogram of body weight compared to younger individuals to trigger the same "growth signal."
For the Patient: Think of your muscles as a fading radio signal. To hear the music (build muscle), you have to turn the volume up. Eating more protein "turns up the volume" so your body can actually hear the signal to stay strong.
2. The "30-Gram Threshold" per Meal
The Science: To maximize MPS, older adults should aim for 25–30g of high-quality protein per eating occasion. Most seniors "back-load" protein at dinner, leaving them in a catabolic (muscle-wasting) state for the rest of the day.
For the Patient: Don't save all your protein for dinner. Your body can’t "store" protein for later like it does with fat. Aim for a "protein-first" breakfast—like eggs or Greek yoghurt—to jumpstart your muscle repair first thing in the morning.
3. The Leucine "Trigger"
The Science: Leucine is the primary branched-chain amino acid (BCAA) that activates the mTORC1 pathway, the master switch for muscle building. Studies suggest older adults need 2.5–3g of leucine per meal to overcome the anabolic threshold.
For the Patient: Not all proteins are created equal. High-leucine foods like whey, soy, fish, and lean meats act like a "key" that unlocks your muscle-building machinery. Ensure at least one high-leucine source is present in every major meal.
4. Bone Health is Muscle Health
The Science: Bone and muscle are a functional unit. High protein intake increases IGF-1 (Insulin-like Growth Factor 1) and improves intestinal calcium absorption. Recent 2024 reviews link higher protein intake to an 11% reduction in hip fractures.
For the Patient: Protein isn't just for "bulking up"; it is the hidden scaffold for your bones. Eating enough protein is just as important as taking calcium and Vitamin D to keep your frame sturdy and break-proof.
5. Pre-Sleep Feeding for Overnight Repair
The Science: Consuming 40g of slow-digesting protein (like casein) before sleep can maintain elevated MPS rates throughout the night, preventing the nocturnal muscle breakdown common in aging.
For the Patient: Your body does its best "construction work" while you sleep. A high-protein snack before bed—such as cottage cheese or a protein shake—provides the "bricks and mortar" your body needs to repair itself overnight.
6. The Synergy of "Protein + Resistance"
The Science: Diet alone is only half the battle. Resistance exercise sensitizes the muscle to amino acids for up to 24–48 hours post-workout, dramatically amplifying the effect of every gram of protein you eat.
For the Patient: Think of protein as the fuel and exercise as the engine. One doesn't work well without the other. Even simple movements like chair squats or using resistance bands make the protein you eat "stick" to your muscles much more effectively.
Author’s Note
As a clinician working at the intersection of metabolism, aging, and exercise physiology, I have repeatedly observed a striking and under-recognized pattern: many of the functional declines we attribute to “normal aging” are, in reality, modifiable consequences of inadequate nutrition—particularly insufficient protein intake.
This article was developed after a detailed review of recent peer-reviewed literature (2024–2025), with the goal of translating complex scientific insights on anabolic resistance, muscle protein synthesis, and sarcopenia into practical, actionable guidance. The intent is not only to inform clinicians and health professionals but also to empower older adults and caregivers with evidence-based strategies that can be implemented immediately.
It is important to emphasize that protein requirements are not static across the lifespan. Aging introduces physiological changes—including reduced anabolic sensitivity, chronic low-grade inflammation, and impaired muscle regeneration—that fundamentally alter how the body responds to dietary protein. As such, long-standing dietary recommendations may no longer be sufficient for maintaining muscle mass, metabolic health, and functional independence in later life.
At the same time, nutrition should never be considered in isolation. The most robust evidence consistently supports a synergistic approach, combining adequate protein intake with resistance exercise, physical activity, and individualized medical care.
Finally, while this article provides general, research-backed recommendations, clinical judgment remains paramount. Patients with conditions such as chronic kidney disease, advanced liver disease, or malignancy require tailored nutritional strategies under professional supervision.
The goal is simple but powerful: to shift the narrative from passive aging to proactive, evidence-based intervention—where preserving muscle is recognized as central to preserving life quality, resilience, and longevity.
Call to Action
Found this article useful? Here is how to get the most from what you have learned:
🔹 Calculate your protein target today. Take your body weight in kilograms, multiply by 1.0–1.2 (if you are healthy) or 1.2–1.5 (if you manage a chronic condition), and you have your daily protein goal in grams.
🔹 Share this article with an older adult in your life — a parent, a patient, or a friend — who may not realise how much their protein intake is shaping their health and independence.
🔹 Book a consultation with a registered dietitian or nutritionist who specialises in older adult health to get a personalised, condition-specific protein plan.
🔹 Start with breakfast. Today, swap out a low-protein breakfast for eggs, Greek yoghurt, or cottage cheese. It is the single fastest change you can make to move closer to your daily target.
🔹 Join the conversation below: What is your biggest challenge with getting enough protein? Leave a comment — we respond to everyone.
Save this article to your bookmarks for easy reference on protein targets and food sources.
Related Articles
Sarcopenia and the Mobility Crisis: Why Muscle Loss Threatens Independence | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
No Time to Train? Science-Backed Workouts That Deliver | DR T S DIDWAL
This article is for educational purposes only and does not constitute medical or nutritional advice. Always consult a qualified healthcare professional before making changes to your diet, particularly if you have existing health conditions.
References
Carballo-Casla, A., Dekhtyar, S., Vetrano, D. L., Calderón-Larrañaga, A., & Fratiglioni, L. (2024). Protein intake and healthy aging: Sooner rather than later? The American Journal of Clinical Nutrition, 119(2), 253–254. https://doi.org/10.1016/j.ajcnut.2023.12.006
Coelho-Júnior, H. J., & Marzetti, E. (2026). Protein intake and its interaction with dietary patterns on clinical outcomes among older adults. npj Aging. https://doi.org/10.1038/s41514-026-00368-8
Encalada-Torres, L., Buri-Encalada, I., Abril-Ulloa, V., Rodas-Guamán, C., & Quito-Parra, M. (2026). Nutritional status associated with physical activity in active older adults in southern Ecuador. Frontiers in Aging, 7, 1723742. https://doi.org/10.3389/fragi.2026.1723742
Groenendijk, I., de Groot, L. C. P. G. M., Tetens, I., & Grootswagers, P. (2024). Discussion on protein recommendations for supporting muscle and bone health in older adults: A mini review. Frontiers in Nutrition, 11, 1394916. https://doi.org/10.3389/fnut.2024.1394916
Harris, S., DePalma, J., & Barkoukis, H. (2025). Protein and aging: Practicalities and practice. Nutrients, 17(15), 2461. https://doi.org/10.3390/nu17152461
Koopmans, L., van Oppenraaij, S., Heijmans, M. W. F., Verlaan, S., Schoufour, J. D., Ten Haaf, D. S. M., van der Avoort, C. M. T., van den Helder, J., Memelink, R., Verreijen, A., Weijs, P. J. M., Eijsvogels, T. M. H., & Hopman, M. T. E. (2025). Dietary protein intake, protein sources & distribution patterns in community-dwelling older adults: A harmonized analysis of eight studies. Clinical Nutrition, 47, 177–184. https://doi.org/10.1016/j.clnu.2025.02.022
van Oppenraaij, S. L., Putker, M., van Schaik, A., Weijs, P. J. M., & Verlaan, S. (2025). Perspectives of adults aged 55+ on plant-based diets rich in protein. Scientific Reports, 15, 31537. https://doi.org/10.1038/s41598-025-17087-x