How to Build Stronger Bones: Why Lean Muscle Mass Matters More Than Weight Loss for Bone Density
How lean muscle mass, fat mass, and body composition affect bone mineral density and bone strength—backed by clinical research
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/21/202626 min read
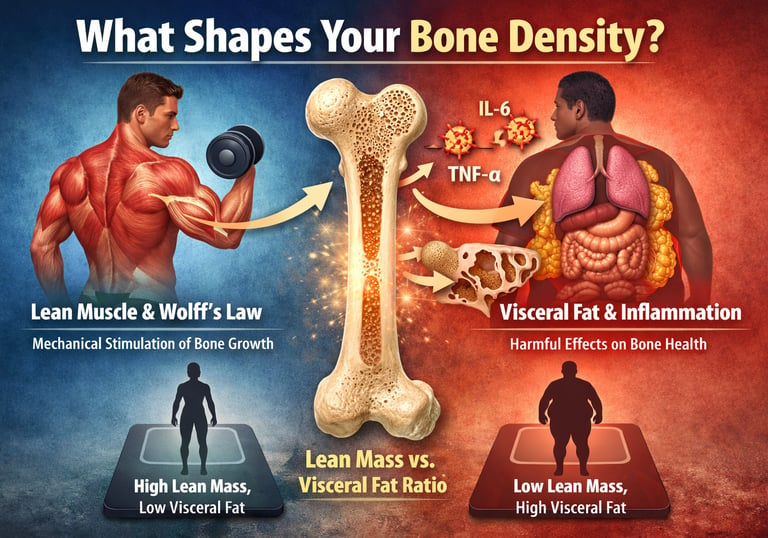
Lean muscle mass is the single most powerful modifiable factor for bone mineral density. Through mechanical loading (Wolff's Law), hormonal signaling, and anti-inflammatory effects, muscle actively builds and preserves bone—far more effectively than weight loss or calcium supplementation alone.
Key Takeaways
Lean muscle mass is the strongest modifiable predictor of bone mineral density (BMD). Resistance training stimulates bone formation through mechanical loading, myokine signaling, and anabolic hormones.
Visceral fat damages bone quality even when bone density appears normal. Chronic inflammation from abdominal fat accelerates bone breakdown and increases fracture risk.
Body composition matters more than body weight alone. Two people with the same weight can have dramatically different bone strength depending on their muscle-to-fat ratio.
The skeletal muscle-to-visceral fat ratio (SVR) may be one of the best modern predictors of bone health. Higher muscle and lower visceral fat are consistently associated with stronger bones and lower osteoporosis risk.
Resistance training, adequate protein intake, and visceral fat reduction are the most powerful lifestyle strategies for preserving lifelong skeletal health. Building muscle is one of the most effective ways to protect bones at any age.
1. Why This Matters More Than You Think
Every 3 seconds, somewhere in the world, a person over 50 suffers an osteoporotic fracture. In the United States alone, more than 10 million people have osteoporosis, and another 44 million have low bone density that puts them at serious risk.
The conventional advice? Drink more milk. Take calcium. Get your vitamin D. And while those factors are not irrelevant, decades of nutrition research have made one thing unmistakably clear: they are not the primary drivers of bone mineral density (BMD).
The primary driver is your body composition—specifically, how much lean muscle mass you carry relative to how much visceral fat you store.
This distinction has enormous practical consequences. It means:
Two people with identical weights can have dramatically different fracture risks.
Losing weight without preserving muscle can actively harm your bones.
Building strength may protect your skeleton better than any supplement on the market.
Certain patterns of obesity can produce bones that are simultaneously dense and dangerously fragile.
This guide synthesizes the latest research—including a landmark 2025 study from Scientific Reports and multiple large population analyses—to give you the most complete, evidence-based picture of what truly builds resilient bones. By the end, you'll have a clear, actionable framework for optimizing your body composition to support skeletal health for life.
2. What Is Bone Mineral Density—And What Actually Controls It?
Bone mineral density (BMD) refers to the concentration of minerals—primarily calcium and phosphate—within bone tissue. It is the most widely used clinical measure of bone health and fracture risk, typically assessed using dual-energy X-ray absorptiometry (DEXA or DXA) scanning.
Your T-score, obtained from a DEXA (DXA) scan, compares your bone mineral density (BMD) to that of a healthy young adult at peak bone mass.
T-score above −1.0
Classification: Normal bone density
Fracture Risk: Low
T-score between −1.0 and −2.5
Classification: Osteopenia (low bone mass)
Fracture Risk: Moderate
T-score below −2.5
Classification: Osteoporosis
Fracture Risk: High
Key Insight
A lower T-score indicates weaker bones and a greater risk of fractures, particularly at the hip, spine, and wrist. However, bone density is only part of the picture—bone quality, muscle mass, balance, and visceral fat also strongly influence real-world fracture risk
What DEXA Can and Cannot Tell You
DEXA measures areal BMD (grams per square centimetre)—a two-dimensional projection. It cannot fully account for:
Bone geometry and depth (trabecular vs. cortical architecture)
Bone microstructure (the quality of internal scaffolding)
Bone turnover rate (how fast bone is being built vs. broken down)
This is why someone can have "normal" or even high BMD on a DEXA scan and still be at elevated fracture risk. Bone quality and bone density are not the same thing—and body composition is the key variable that determines the gap between them.
The Four Key Controllers of BMD
Research consistently identifies four modifiable factors as the primary determinants of bone mineral density:
Lean muscle mass — The dominant positive driver through mechanical loading and hormonal signaling
Fat mass distribution — Complex effects that differ by fat type and location
Hormonal environment — Especially estrogen, IGF-1, and inflammatory cytokines
Physical activity type — Weight-bearing and resistance activities create bone-building stimuli
Of these, lean body mass is the most powerful and consistently beneficial. And unlike your hormonal profile or your genetic predisposition, it's something you can meaningfully change at any age.
3. The Muscle–Bone Connection: How Lean Mass Builds Skeletal Strength
Wolff's Law: Your Bones Are Listening to Your Muscles
In 1892, German surgeon Julius Wolff proposed what is now one of the foundational principles of bone biology: bone adapts its structure in response to the mechanical forces placed upon it. This principle—Wolff's Law—explains why astronauts lose bone mass in zero gravity, why bedridden patients develop osteoporosis, and why weight lifters have measurably denser bones than sedentary individuals.
The mechanism works like this:
Muscle contracts during movement or resistance exercise.
Force is transmitted through tendons to the attached bone.
Osteocytes (bone-sensing cells embedded in bone tissue) detect this mechanical deformation.
Osteoblasts (bone-building cells) are activated in response.
New bone matrix is laid down and mineralized, increasing BMD.
This is why lean muscle mass is not merely associated with stronger bones—it is the mechanical cause of bone formation. The more muscle you carry and the more frequently you challenge it, the stronger the signal your skeleton receives to maintain and build density.
The Endocrine Connection: Muscle as a Hormonal Organ
Beyond mechanical loading, lean mass influences bone health through powerful hormonal pathways that are often overlooked:
Insulin-Like Growth Factor 1 (IGF-1) Skeletal muscle is a major site of IGF-1 production and responsiveness. Higher lean body mass correlates with elevated circulating IGF-1, which directly stimulates osteoblast proliferation and bone matrix synthesis. IGF-1 is essentially a systemic "build" signal for both muscle and bone simultaneously.
Myokines: The Bone-Muscle Crosstalk Molecules Muscle tissue functions as an endocrine organ, releasing specialized signaling proteins called myokines during contraction. Several myokines—including irisin, osteocalcin-related signals, and IL-15—have been shown to directly promote osteoblast activity and suppress osteoclast (bone-breakdown) function. This means every time you exercise, your muscles are sending chemical messages to your bones to grow stronger.
Testosterone and Growth Hormone Resistance training elevates both testosterone and growth hormone in the short term, both of which independently support bone mineral density. Higher lean mass correlates with more favorable anabolic hormonal profiles over the long term.
What the Evidence Shows
A comprehensive Norwegian population study—the Hordaland Health Study—tracked the relationship between lean mass, fat mass, and BMD across diverse age groups and sexes. The findings were unambiguous: lean mass demonstrated strong, consistent positive associations with BMD at every skeletal site and in every age group studied (Gjesdal et al., 2008).
Similarly, research in young overweight and obese women found that lean mass was the dominant predictor of bone density even when total body weight was held constant—meaning that the composition of that weight mattered far more than the number on the scale (Garvey et al., 2022).
Bottom line: If you want stronger bones, you must prioritize building and preserving lean muscle mass. No supplement, no amount of dairy consumption, and no other lifestyle intervention comes close to the impact of consistent resistance training on skeletal health.
4. The Fat Mass Paradox: Dense Bones That Still Break
Here is one of the most clinically important—and counterintuitive—findings in modern bone research: obesity is associated with both higher BMD and higher fracture rates. This is known as the obesity paradox, and understanding it is essential for anyone managing their bone health.
Why Obesity Raises BMD (Mechanically)
Carrying excess body weight places continuous mechanical load on the skeleton, particularly on weight-bearing sites like the hips and spine. Just as resistance training stimulates bone formation, the added gravitational load of obesity activates osteoblasts and tends to increase BMD over time.
Additionally, adipose (fat) tissue produces estrogen through a process called peripheral aromatization—and estrogen is a potent inhibitor of osteoclast (bone-resorbing) activity. In postmenopausal women especially, where ovarian estrogen production has ceased, this adipose-derived estrogen provides some residual bone protection.
So yes—some degree of fat mass can support bone density.
Why Obese Individuals Still Break More Bones
The paradox arises because bone density and bone quality are not synonymous.
Excess fat mass—especially visceral adiposity—generates chronic, low-grade systemic inflammation. This inflammatory environment produces elevated levels of:
Tumor Necrosis Factor-alpha (TNF-α)
Interleukin-6 (IL-6)
Interleukin-1β (IL-1β)
These pro-inflammatory cytokines powerfully activate osteoclasts—the cells that break down bone. The result is accelerated bone turnover: bone is being both built (elevated osteoblast activity from mechanical loading) and destroyed (elevated osteoclast activity from inflammation) simultaneously.
When bone turnover accelerates this way, the internal microarchitecture of bone—the delicate lattice of trabecular (spongy) bone—becomes disrupted. DEXA scans may show adequate or even high mineral density, but the structural integrity of the bone has been compromised. These bones fracture under forces that normal bone would easily withstand.
The Critical Takeaway
Body weight alone is a poor predictor of bone health. What matters is the composition of that weight:
High lean mass + low fat mass = High BMD + High bone quality = Lowest fracture risk ✅
High lean mass + moderate fat mass = High BMD + Good bone quality ✅
Low lean mass + high fat mass = Variable BMD + Poor bone quality = High fracture risk ⚠️
Low lean mass + low fat mass = Low BMD = High fracture risk ⚠️
This is why researchers have increasingly focused on body composition ratios rather than absolute measures—and why the metric discussed in the next section is rapidly emerging as the gold standard for bone health assessment.
5. Visceral Fat: The Hidden Enemy of Bone Quality
Not all fat is created equal. Your body stores fat in two fundamentally different locations with profoundly different health consequences:
Types of Body Fat and Their Effects on Bone Health
Subcutaneous Fat
Location: Stored directly under the skin
Metabolic Activity: Moderate
Effect on Bone Health: Mildly protective due to estrogen production and some mechanical loading benefits
Visceral Fat
Location: Stored around internal organs within the abdominal cavity
Metabolic Activity: Very high
Effect on Bone Health: Detrimental; promotes chronic inflammation, insulin resistance, and increased bone breakdown, negatively affecting bone quality and fracture risk
Key Clinical Insight
Not all body fat affects the skeleton the same way. Subcutaneous fat may provide limited hormonal protection, whereas excess visceral fat is strongly associated with poorer bone quality, higher inflammation, and increased osteoporosis risk.
How Visceral Fat Harms Bone: The Mechanisms
Chronic Inflammation Visceral fat generates persistent low-grade inflammation via elevated IL-6, TNF-α, and C-reactive protein (CRP). This inflammatory state activates osteoclasts and suppresses osteoblast differentiation—a dual assault on bone formation.
Insulin Resistance Visceral adiposity is the strongest driver of insulin resistance. Insulin normally has modest anabolic effects on bone; insulin resistance disrupts these effects and further promotes inflammatory bone resorption.
Altered Adiponectin Signaling Visceral fat suppresses adiponectin—a hormone with protective effects on bone metabolism. Research suggests both very high and very low adiponectin levels can compromise BMD, with optimal bone density occurring within a specific mid-range that visceral obesity disrupts.
Bone Marrow Fat Infiltration Emerging research reveals that visceral fat correlates with increased fat accumulation within bone marrow itself. This marrow adiposity competes with hematopoietic (blood-forming) and osteoblastic cells for space and resources, directly impairing the local bone formation environment.
The Lean-to-Visceral-Fat Ratio: A More Powerful Predictor
A landmark cross-sectional analysis of U.S. population data (Li et al., 2023) demonstrated that the ratio of lean body mass to visceral fat mass is a stronger independent predictor of bone mineral density than either measurement alone, and stronger than total body weight or BMI.
This finding has been replicated across diverse populations and age groups. The clinical implication is clear: the goal of any bone-health intervention should not simply be to lower the number on the scale, but to shift the body composition ratio in favor of lean mass over visceral fat.
6. The Skeletal Muscle-to-Visceral Fat Ratio (SVR): The Metric That Changes Everything
Introducing SVR
A groundbreaking 2025 study published in Scientific Reports (Jin et al., 2025) introduced and validated a novel composite metric for bone health assessment: the Skeletal Muscle Mass-to-Visceral Adipose Tissue Area Ratio (SVR).
Calculated as skeletal muscle mass (kg) divided by visceral adipose tissue area (cm²), the SVR captures what previous individual measurements missed: the dynamic balance between the body's primary bone-building tissue (muscle) and its primary bone-eroding tissue (visceral fat).
In a study of 4,349 middle-aged adults (ages 40–59), the SVR proved to be a significantly more accurate predictor of lumbar spine BMD than:
Skeletal muscle mass alone
Visceral fat area alone
BMI
Total body weight
How SVR Works in Practice
The relationship between SVR and bone density is not identical for men and women—a finding with major clinical implications.
In Men: Linear and Straightforward
For men, the SVR–BMD relationship is direct and linear. As the muscle-to-visceral-fat ratio increases, lumbar bone density consistently improves. The practical prescription is uncomplicated: maximize muscle mass while minimizing visceral fat, and bone health follows.
In Premenopausal Women: The Goldilocks Zone
In premenopausal women, the relationship takes a different shape—a non-linear, inverted-U curve. BMD is optimized at an SVR threshold of approximately 0.31 kg/cm². Below this threshold, insufficient muscle and/or excess visceral fat undermine bone density. Beyond this threshold, excessively high ratios (as seen in very lean women with extremely low fat mass) may reduce BMD.
Why? Because adequate fat mass in premenopausal women is necessary to maintain estrogen production. When body fat drops too low, estrogen levels fall—and estrogen is a critical inhibitor of osteoclast activity. This is why female athletes with very low body fat percentages (e.g., elite distance runners) are disproportionately affected by stress fractures and the Female Athlete Triad (low energy availability + menstrual dysfunction + low BMD).
What SVR Means for You
Men (All Ages)
Maximize lean muscle mass
Minimize visceral fat accumulation
Higher skeletal muscle-to-visceral fat ratio (SVR) is consistently associated with better bone density and skeletal strength
Premenopausal Women
Optimize the SVR rather than pushing for extreme leanness
Avoid both:
Excess visceral fat
Excessively low body fat
Maintaining some protective fat mass is important for healthy estrogen production and bone preservation
Postmenopausal Women
Prioritize preserving and rebuilding muscle mass through resistance training
Aggressively address visceral fat accumulation, which tends to increase after estrogen decline
Muscle becomes increasingly important for skeletal protection after menopause
Middle-Aged Adults (40–59 Years)
SVR appears to be especially predictive of bone health during this stage of life
Early intervention is critical before age-related muscle loss and visceral fat gain accelerate
Focus on resistance training, metabolic health, and body composition improvement
Key Clinical Insight
The ideal bone-health strategy is not simply weight loss—it is improving the balance between lean muscle and visceral fat. A higher SVR generally reflects a stronger metabolic and skeletal profile.
7. Sex Differences in Body Composition and Bone Health
Research published in PLoS ONE (Lin & Teng, 2024) confirms what clinical observation has long suggested: the body composition–bone health relationship differs meaningfully between males and females, and a one-size-fits-all recommendation fails both groups.
Males: Lean Mass Dominates
In men, the relationship between lean body mass and bone strength is relatively direct and robust. Greater skeletal muscle mass predicts higher BMD across the lifespan with minimal confounding. Men benefit from:
Higher baseline testosterone (anabolic for both muscle and bone)
Less hormonal volatility over the lifespan
A more linear SVR–BMD relationship
Primary recommendation for men: Focus relentlessly on building and maintaining lean muscle mass through resistance training. The bone health benefit scales with muscle gain.
Females: Estrogen, Fat, and Complexity
Women face a more nuanced landscape, shaped by estrogen's dual role as both a bone protector and a mediator of fat mass effects.
Premenopausal women need sufficient body fat to maintain adequate estrogen production for bone protection—but excess visceral fat generates the inflammation that undermines bone quality. This creates an optimal range rather than a simple "less fat is always better" prescription.
Postmenopausal women experience the most rapid bone loss of any demographic group—up to 3–5% of BMD per year in the first 5 years after menopause. With ovarian estrogen production ceasing, the bone-protective effects of muscle become more critical than ever, and visceral fat accumulation (which accelerates post-menopause) becomes more damaging.
Research indicates that visceral fat is particularly detrimental to bone quality in women, interacting with estrogen-dependent mechanisms to accelerate bone resorption in ways not seen to the same degree in men.
Primary recommendation for women:
Pre-menopause: Optimize the SVR—build muscle, reduce visceral fat, avoid extreme leanness
Post-menopause: Prioritize resistance training to compensate for lost estrogenic bone protection; aggressively target visceral fat through diet, exercise, and sleep quality
8. Age and the Lifespan of Your Bones
Bone health is not a snapshot—it's a lifelong process with distinct phases, each requiring a tailored approach.
Childhood and Adolescence: The Peak Bone Mass Window
Approximately 90% of peak bone mass is acquired by age 18 in girls and age 20 in boys. The amount of bone mass built during these years establishes the skeletal "bank account" you'll draw from for the rest of your life.
Research in Chinese adolescents (Ma et al., 2024) found that teenagers with high fat mass and low lean mass had significantly reduced bone mineral content—even when their total body weight appeared normal for their age. This "high-fat, low-muscle" phenotype during adolescence can establish a bone health deficit that persists and compounds over decades.
Intervention priority in youth: Physical activity that builds muscle—particularly resistance training and high-impact sports—is the most powerful investment in lifelong skeletal resilience.
Young Adulthood (20–35): Building and Consolidating
Peak bone mass is typically reached in the late 20s to early 30s, after which BMD plateaus before its gradual age-related decline. This is the phase to:
Maximize lean mass through strength training
Establish exercise habits that will sustain BMD through middle age
Avoid prolonged caloric restriction without attention to lean mass preservation
Middle Age (35–60): The Critical Maintenance Phase
After peak bone mass, the priority shifts from accumulation to preservation. Lean mass naturally begins to decline (a process called sarcopenia that accelerates after age 40), and visceral fat tends to increase—an unfavorable compositional shift that attacks bone from both directions.
The SVR metric (Jin et al., 2025) was validated specifically in this 40–59 age range, highlighting it as the pivotal window for body composition intervention.
Older Adults (60+): Damage Control and Fracture Prevention
After 60—and especially post-menopause in women—BMD decline accelerates, and the consequences of falls become severe. The clinical priority becomes fracture prevention. Research confirms that:
Lean mass maintenance is the strongest modifiable predictor of BMD in older adults (Gjesdal et al., 2008)
Resistance training in older adults measurably increases BMD, even when begun late in life
Frailty (very low lean mass) dramatically multiplies fracture risk beyond what BMD scores alone predict
The key message: It is never too late to begin resistance training for bone health. Even frail older adults show measurable improvements in lean mass and BMD with appropriate progressive resistance programs.
9. What the Research Says: Key Studies Summarized
Study 1 — Lean Mass vs. Fat Mass in Young Women (Garvey et al., 2022)
Population: Young, overweight and obese women
Key Finding: Lean mass was the dominant independent predictor of BMD at all skeletal sites, even after controlling for total body weight.
Study 2 — Lean-to-Visceral-Fat Ratio and BMD in U.S. Adults (Li et al., 2023)
Population: Cross-sectional U.S. population data, diverse age groups and ethnicities
Key Finding: The lean body mass–to–visceral fat mass ratio independently predicted BMD better than total fat mass, lean mass, or BMI alone. The relationship held after adjusting for total body weight. Clinical Implication: Assess body composition ratios, not just absolute measurements. Target ratio improvement, not simply weight reductionStudy
3 — The Hordaland Health Study (Gjesdal et al., 2008)
Population: Large Norwegian community cohort, multiple age groups, both sexes.
Key Finding: Lean mass consistently predicted BMD across all age groups and skeletal sites. Fat mass showed age-dependent effects—modestly protective in younger adults, increasingly detrimental to bone quality with aging. Women showed greater lean mass dependency post-menopause. Clinical Implication: The importance of maintaining lean mass for bone health only increases with age.
Study 4 — High Fat/Low Lean Phenotype in Chinese Adolescents (Ma et al., 2024)
Population: Chinese adolescents, cross-sectional design
Key Finding: Adolescents with high fat and low lean mass had significantly reduced bone mineral content despite normal total body weight.
Clinical Implication: Youth body composition programs should prioritise lean mass development to optimise accrual of peak bone mass.
Study 5 — SVR and Sex-Specific BMD Predictions (Jin et al., 2025)
Population: 4,349 middle-aged U.S. adults (40–59 years), NHANES data
Key Finding: SVR (skeletal muscle mass ÷ visceral adipose tissue area) was the strongest predictor of lumbar BMD. Men showed a linear SVR–BMD relationship; premenopausal women showed a non-linear "Goldilocks zone" effect, with optimal BMD at SVR ≈ 0.31 kg/cm².
Clinical Implication: Bone health interventions in middle age should be sex-specific, targeting ratio optimization rather than weight loss alone.
Study 6 — Sex Differences in Fat/Lean Contributions to Bone Strength (Lin & Teng, 2024)
Population: Adult males and females, comparative analysis
Key Finding: Males showed stronger lean mass–bone strength correlations; females showed complex interactions between estrogen, visceral fat, and bone quality. Visceral fat was particularly harmful to bone in females.
Clinical Implication: Bone health strategies must be individually tailored by sex, with women giving extra emphasis to visceral fat reduction.
10. Evidence Table: Body Composition and Bone Health Studies at a Glance
Population: Young overweight women
Key Metric: Lean mass vs. fat mass
Main Finding: Lean mass was the strongest predictor of bone mineral density (BMD), outperforming fat mass in predicting skeletal strength.
Population: Diverse U.S. adult population
Key Metric: Lean-to-visceral-fat ratio
Main Finding: The lean-to-visceral-fat ratio predicted BMD more accurately than total body fat or body weight alone.
Population: Norwegian community cohort
Key Metric: Lean and fat mass
Main Finding: Lean mass showed a consistently positive relationship with bone health across all age groups.
Ma et al. (2024)
Population: Chinese adolescents
Key Metric: Fat/lean phenotype
Main Finding: Adolescents with high fat mass and low lean mass had significantly lower bone mineral content.
Jin et al. (2025)
Population: U.S. adults aged 40–59 years
Key Metric: Skeletal muscle-to-visceral-fat ratio (SVR)
Main Finding: SVR emerged as the strongest predictor of lumbar spine BMD.
Population: Adult men and women
Key Metric: Fat and lean mass indices
Main Finding: The influence of body composition on bone differed between sexes, demonstrating important sex-specific skeletal effects.
11. How to Optimize Your Body Composition for Maximum Bone Density
The research converges on a clear, evidence-based framework for building and preserving bone through body composition optimization. Here is your complete action plan.
Step 1: Know Your Starting Point
Before optimizing, measure. Request the following from your healthcare provider:
DEXA scan: For BMD assessment (T-score and Z-score) and body composition (lean mass, fat mass, visceral fat estimate)
Blood tests: Vitamin D (25-OH vitamin D), calcium, PTH, IGF-1, and in women, estradiol if peri- or postmenopausal
Inflammatory markers: CRP and fasting insulin can signal metabolic risk to bones
Step 2: Prioritize Resistance Training (Non-Negotiable)
This is the single most powerful intervention for lean mass and bone density. The evidence is overwhelming and consistent across every age group and sex.
Minimum effective dose: 2–3 sessions per week targeting all major muscle groups
Progressive overload principle: Gradually increase weight, reps, or volume over time—bones adapt to increasing mechanical stress, so consistent challenge is essential.
Optimal exercise types for bone health:
Compound barbell lifts (squats, deadlifts, bench press)
Dumbbell and machine resistance exercises
Bodyweight exercises with progressive difficulty
Resistance band training (effective for beginners and older adults)
Step 3: Add Weight-Bearing Cardiovascular Activity
Weight-bearing aerobic exercise creates additional mechanical loading for bone at the hip and spine—two of the most clinically significant fracture sites.
High-impact options (strongest bone signal):
Running and jogging
Jump rope
Hiking on varied terrain
Tennis and racket sports
Lower-impact options (for those with joint concerns):
Brisk walking
Stair climbing
Low-impact aerobics
Note: Swimming and cycling, while excellent for cardiovascular health, are non-weight-bearing and provide minimal bone-building stimulus. They should complement—not replace—weight-bearing activity.
Step 4: Optimize Protein Intake to Preserve Lean Mass
Muscle is the engine of bone health, and protein is the fuel for muscle. Current evidence supports:
General adults: 0.8–1.0 g of protein per kilogram of body weight per day (minimum)
Active adults building muscle: 1.2–1.6 g/kg/day
Older adults (65+): 1.2–2.0 g/kg/day (higher needs due to anabolic resistance)
During weight loss: Maintain protein at the upper end of your range to preserve lean mass while in a caloric deficit
High-quality protein sources:
Lean meats (chicken breast, turkey, lean beef)
Fish and seafood
Eggs and dairy (also provide calcium)
Greek yogurt
Legumes and pulses (for plant-based diets)
Protein supplements, when dietary targets are difficult to meet
Step 5: Reduce Visceral Fat Through Metabolic Health Strategies
Visceral fat responds best to a combination of targeted lifestyle interventions:
Dietary strategies:
Reduce refined carbohydrates and added sugars (primary drivers of visceral adiposity)
Prioritize dietary fiber from vegetables, legumes, and whole grains
Limit ultra-processed foods
Moderate alcohol consumption (alcohol significantly promotes visceral fat accumulation)
Sleep optimization:
Aim for 7–9 hours of quality sleep per night
Poor sleep elevates cortisol, which promotes visceral fat storage and accelerates bone loss
Address sleep apnea if present—untreated sleep apnea is independently associated with reduced BMD
Stress management:
Chronic psychological stress elevates cortisol chronically, suppressing osteoblast activity and promoting osteoclast activation
Mindfulness, structured relaxation, and social connection all reduce cortisol burden
12. Bone-Building Workout Protocol (Evidence-Based)
3-Day-Per-Week Resistance Training Program for Bone Density
Day 1 — Lower Body Focus
Barbell or goblet squat: 3 sets × 8–10 reps
Romanian deadlift: 3 sets × 8–10 reps
Walking lunges: 3 sets × 12 reps each leg
Calf raises (weighted): 3 sets × 15 reps
Hip thrust: 3 sets × 10 reps
Day 2 — Upper Body and Core
Bench press or push-ups (weighted): 3 × 8–10
Bent-over dumbbell row: 3 × 10
Overhead press: 3 × 8–10
Lat pulldown or assisted pull-up: 3 × 10
Plank: 3 × 30–45 seconds
Day 3 — Full Body and Hip-Spine Emphasis
Deadlift (conventional or trap bar): 3 × 6–8
Step-ups with dumbbells: 3 × 10 each leg
Single-leg Romanian deadlift: 3 × 8 each
Farmer's carry: 3 × 30 meters
Band pull-aparts: 3 × 15
Progressive overload rule: When you can complete all prescribed reps with good form, increase the load by 2.5–5% at the next session.
Supplemental weight-bearing cardio: 20–30 minutes of brisk walking or jogging on at least 3 additional days per week.
Safety Note: If you have been diagnosed with osteoporosis, osteopenia, or have other musculoskeletal conditions, consult a physical therapist or exercise physiologist before beginning this or any resistance training program. Modifications to loading, range of motion, and exercise selection may be necessary for your safety and benefit.
13. Nutrition for Bone Density: Beyond Calcium and Vitamin D
Most bone health nutrition advice begins and ends with calcium and vitamin D. Both are important, but the nutritional picture for bone health is considerably broader.
The Essential Bone Nutrition Checklist
Calcium — 1,000–1,200 mg/day for adults; prioritize dietary sources over supplements where possible
Best sources: dairy products, fortified plant milks, canned fish with bones, leafy greens (kale, bok choy)
Vitamin D — 1,500–2,000 IU/day is commonly recommended for adults at risk; blood testing (target 40–60 ng/mL) guides supplementation
Best sources: sunlight exposure, fatty fish, fortified foods, supplementation if deficient
Vitamin K2 (MK-7) — Directs calcium into bone (rather than arteries); evidence for fracture reduction is emerging
Best sources: fermented foods (natto, aged cheese), supplementation
Magnesium — Required for vitamin D activation and bone matrix formation; 30–40% of adults are deficient
Best sources: nuts, seeds, dark chocolate, leafy greens, whole grains
Phosphorus — Works in concert with calcium for bone mineralization; deficiency is rare in Western diets
Protein — As discussed above; provides the collagen matrix into which minerals are deposited
Omega-3 fatty acids — Anti-inflammatory; may blunt the bone-resorbing effects of inflammatory cytokines from visceral fat
Best sources: fatty fish (salmon, sardines, mackerel), walnuts, flaxseed, fish oil supplementation
What to Limit for Bone Health
Excess sodium: Promotes urinary calcium excretion
High alcohol intake: Suppresses osteoblast activity and impairs calcium absorption
Excess caffeine (> 4 cups/day): Modestly increases urinary calcium loss
Very-low-calorie diets without protein focus: Accelerate lean mass loss and compromise bone
14. Common Myths and Costly Mistakes
Myth 1: "Calcium Supplements Alone Will Protect My Bones"
The reality: Calcium is necessary but insufficient. Without adequate muscle mass (the mechanical stimulus for bone formation), vitamin K2 (to direct calcium into bone), and magnesium (to activate vitamin D), supplemental calcium has limited impact on fracture risk—and high-dose supplemental calcium may even increase cardiovascular risk in some populations. Whole-diet approaches are preferable to isolated supplementation.
Myth 2: "Losing Weight Will Improve My Bone Health"
The reality: Weight loss without lean mass preservation can significantly harm bone density. Caloric restriction reduces mechanical load on the skeleton, and if protein intake is insufficient, lean mass is catabolized—removing the primary stimulus for bone formation. Bone-healthy weight loss must include resistance training and adequate protein to ensure you're losing fat, not muscle.
Myth 3: "Swimming and Cycling Are Great for My Bones"
The reality: Both are excellent cardiovascular activities with many health benefits, but they are non-weight-bearing and provide minimal bone-building stimulus. Competitive swimmers and cyclists actually show lower BMD than runners and other weight-bearing athletes. These activities should be supplemented with weight-bearing and resistance exercise, not used as replacements.
Myth 4: "Osteoporosis Is an Old Person's Problem—I'll Worry About It Later"
The reality: Up to 90% of peak bone mass is set by age 20. Habits established in childhood and young adulthood determine your "bone bank account" for life. Adults in their 30s and 40s who neglect lean mass maintenance are rapidly drawing down a reserve that becomes increasingly difficult to rebuild. The best time to act was in your youth; the second-best time is now.
Myth 5: "If I'm Heavy, My Bones Must Be Strong"
The reality: The obesity paradox demonstrates the opposite can be true. High body weight does provide mechanical loading stimulus, but excess visceral fat generates bone-damaging inflammation. Obese individuals, particularly those with metabolically active visceral adiposity, can present with high DEXA BMD scores yet have compromised bone microarchitecture and elevated fracture rates.
Myth 6: "Women Who Are Very Lean Have the Healthiest Bones"
The reality: The Goldilocks Zone effect in premenopausal women means extreme leanness can be as harmful to bone as obesity. Very low body fat depresses estrogen production—a critical inhibitor of bone resorption. Female athletes with very low body fat percentages face disproportionate rates of stress fractures and the Female Athlete Triad. Bone-healthy leanness means optimizing the SVR, not minimizing fat at all costs.
15. FAQs: What People Are Actually Asking
Q: What is the most important factor for bone mineral density?
The single most consistently supported modifiable factor is lean muscle mass. Research across multiple large populations confirms that skeletal muscle mass is the dominant positive predictor of BMD at all major skeletal sites and in all age groups. Building and maintaining muscle through resistance training is the most powerful bone health intervention available.
Q: Does building muscle really help your bones?
Yes—directly and powerfully. Muscle contraction transmits mechanical force to bone, activating osteoblasts (bone-building cells) through a process described by Wolff's Law. Additionally, muscle tissue releases hormones (IGF-1) and myokines (irisin, IL-15) that chemically signal bone formation. Resistance training measurably increases bone mineral density in clinical trials across all age groups, including older adults.
Q: Can losing weight cause bone loss?
Yes, it can—if lean mass is not preserved during weight loss. Caloric restriction reduces mechanical loading and, without sufficient dietary protein and resistance training, causes muscle catabolism that removes the primary stimulus for bone formation. Weight loss that incorporates resistance training and adequate protein intake (1.2–1.6 g/kg/day) can maintain or even improve BMD while reducing body fat.
Q: Is it possible to have high bone density but still be at high fracture risk?
Yes. This is called the obesity paradox. Excess visceral fat generates chronic inflammation that compromises bone microarchitecture—the internal structural quality of bone—even when mineral density appears adequate on a DEXA scan. Bone quality (structural integrity) and bone density (mineral content) are distinct properties. High-density, low-quality bone can fracture under ordinary loads.
Q: What body composition ratio is best for bone health?
Research points to the Skeletal Muscle-to-Visceral Fat Ratio (SVR) as the most accurate predictor. For men, a higher SVR consistently predicts better bone density. For premenopausal women, there is an optimal SVR threshold of approximately 0.31 kg/cm²—both very low and very high ratios are associated with suboptimal bone density. For all adults, prioritizing lean mass while reducing visceral fat improves the ratio most favorably.
Q: Do men and women need different bone health strategies?
Yes, significantly so. Men show a more direct, linear relationship between lean mass and bone strength. Women face more complex interactions involving estrogen, fat mass distribution, and hormonal changes across the lifespan. Premenopausal women need to optimize—not minimize—their fat mass to maintain estrogen production. Postmenopausal women face the most rapid bone loss and need especially consistent resistance training combined with visceral fat reduction.
Q: What exercise is best for bone density?
For bone density specifically, progressive resistance training is the gold standard—squats, deadlifts, rows, presses, and other compound exercises that load the skeleton through muscular contraction. High-impact weight-bearing exercise (running, jumping, tennis) provides complementary bone stimulus at the hip and spine. The combination of both types produces superior BMD outcomes compared to either alone.
Q: How much protein do I need for bone health?
Protein is essential for maintaining lean mass—the primary mechanical driver of bone density—and also provides collagen, the structural matrix of bone tissue. Evidence supports 1.0–1.6 g of protein per kilogram of body weight per day for active adults focused on muscle and bone health, with higher needs (up to 2.0 g/kg/day) for older adults dealing with anabolic resistance. Spreading protein intake evenly across meals (rather than loading at dinner) optimizes muscle protein synthesis.
Q: At what age should I start worrying about bone health?
Immediately—at any age. During youth (up to ~age 20), the focus is on maximizing peak bone mass through physical activity and lean mass development. During young adulthood (20–35), consolidation of peak bone mass is the priority. From middle age onward, preventing the lean mass loss and visceral fat gain that accelerate BMD decline becomes critical. After menopause in women and after 65 in men, fracture prevention is the primary goal. Every decade of consistent resistance training reduces lifetime fracture risk.
Q: Is visceral fat the worst thing for bone health?
Among the factors within your control, visceral fat accumulation is among the most damaging—not because it doesn't contribute to mechanical loading (it does), but because it generates systemic inflammation that undermines bone quality through osteoclast activation and compromised bone microarchitecture. The particularly insidious aspect is that its effects are largely invisible on a standard DEXA scan, which measures mineral density but not internal structural quality.
Q: Can older adults actually build bone density, or is it too late?
It is never too late to improve your skeletal health relative to your baseline. Randomized controlled trials consistently demonstrate that resistance training in older adults—including those with existing osteoporosis—produces measurable increases in lean mass and BMD. While the magnitude of improvement is smaller than in younger adults (due to anabolic resistance and lower hormonal milieu), the fracture-preventing benefit of improved muscle strength and balance is clinically significant at any age.
Q: What foods are best for bone density?
Beyond adequate calcium and vitamin D, evidence supports the following dietary priorities for bone health: sufficient protein (for lean mass and bone matrix), magnesium (from nuts, seeds, greens), vitamin K2 (from fermented foods), omega-3 fatty acids (from fatty fish and walnuts—anti-inflammatory), and whole, minimally processed foods that support metabolic health and reduce visceral adiposity. Reducing added sugars, refined grains, excess sodium, and alcohol also meaningfully protects bone quality.
16. Conclusion and Action Plan
The science is clear: bone health is fundamentally a body composition problem—and the solution is a body composition solution.
Calcium and vitamin D matter. But they are not the primary levers. The primary lever is the balance between lean muscle mass and visceral fat tissue—a ratio that directly determines both the mechanical signals and the hormonal environment that govern how dense, strong, and resilient your bones become.
Your 5-Step Bone Health Action Plan
Step 1 — Measure. Get a DEXA scan to know your current BMD, lean mass, and fat distribution. Ask your doctor about your vitamin D level and basic bone metabolic markers.
Step 2 — Train with resistance. Commit to 2–3 progressive resistance training sessions per week targeting all major muscle groups. This is non-negotiable for bone health at any age.
Step 3 — Eat for lean mass. Prioritize protein at 1.2–1.6 g/kg/day. Ensure adequate intake of calcium, vitamin D, vitamin K2, magnesium, and omega-3s. Reduce ultra-processed foods and added sugars.
Step 4 — Target visceral fat. Reduce refined carbohydrates, optimize sleep (7–9 hours), manage chronic stress, and limit alcohol. These strategies reduce inflammatory adiposity more effectively than scale weight management alone.
Step 5 — Personalize by sex and age. Men: maximize the SVR without ceiling. Premenopausal women: target the optimal SVR range—build muscle but preserve adequate fat mass for estrogen. Postmenopausal women: resistance training and visceral fat reduction are your primary tools now that estrogen protection has been lost.
The skeleton you have at 70 is built from decisions you make today. Strong bones are not the product of supplements—they are the product of movement, muscle, metabolic health, and consistent, evidence-based lifestyle choices across the lifespan.
Call to Action: "If you found this guide helpful, share it with someone who needs it
Medical Disclaimer: This article is intended for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before beginning any new exercise program or making significant changes to your diet, especially if you have existing health conditions such as osteoporosis, osteopenia, cardiovascular disease, or metabolic disorders.
Related Articles
Best Exercises for Osteoporosis: Build Stronger Bones Safely
How to Build a Disease-Proof Body: Master Calories, Exercise & Longevity | DR T S DIDWAL
How to Maximize Muscle Growth: Evidence-Based Strength Training Strategies | DR T S DIDWAL
Lower Blood Pressure Naturally: Evidence-Based Exercise Guide for Metabolic Syndrome | DR T S DIDWAL
Exercise vs. Diet Alone: Which is Best for Body Composition? | DR T S DIDWAL
Movement Snacks: How VILPA Delivers Max Health Benefits in Minutes | DR T S DIDWAL
Breakthrough Research: Leptin Reduction is Required for Sustained Weight Loss | DR T S DIDWAL
HIIT Benefits: Evidence for Weight Loss, Heart Health, & Mental Well-Being | DR T S DIDWAL
References
Jin, F., Gao, S., Yao, X., et al. (2025). Sex-specific associations between muscle-fat ratio and bone density in middle-aged adults. Scientific Reports, 15, 29105. https://doi.org/10.1038/s41598-025-15069-7
Garvey, M. E., Shi, L., Lichtenstein, A. H., Must, A., Hayman, L. L., Crouter, S. E., & Camhi, S. M. (2022). Association of bone mineral density with lean mass, fat mass, and physical activity in young overweight and obese women. International Journal of Exercise Science, 15(7), 585–598. https://doi.org/10.70252/POYU6849
Gjesdal, C. G., Halse, J. I., Eide, G. E., Brun, J. G., & Tell, G. S. (2008). Impact of lean mass and fat mass on bone mineral density: The Hordaland Health Study. Maturitas, 59(2), 191–200. https://doi.org/10.1016/j.maturitas.2007.11.002
Li, L., Zhong, H., Shao, Y., Zhou, X., Hua, Y., & Chen, M. (2023). Association between lean body mass to visceral fat mass ratio and bone mineral density in United States population: A cross-sectional study. Archives of Public Health, 81(1), 180. https://doi.org/10.1186/s13690-023-01190-4
Lin, Y. H., & Teng, M. M. H. (2024). Different contributions of fat and lean indices to bone strength by sex. PLoS ONE, 19(11), e0313740. https://doi.org/10.1371/journal.pone.0313740
Ma, X., Tian, M., Liu, J., Tong, L., & Ding, W. (2024). Impact of high fat and low lean mass phenotype on bone mineral content: A cross-sectional study of Chinese adolescent population. Bone, 186, 117170. https://doi.org/10.1016/j.bone.2024.117170
Compston, J. E., McClung, M. R., & Leslie, W. D. (2019). Osteoporosis. The Lancet, 393(10169), 364–376. https://doi.org/10.1016/S0140-6736(18)32112-3
Wolff, J. (1892). Das Gesetz der Transformation der Knochen [The Law of Bone Remodeling]. Hirschwald.
Bhasin, S., Apovian, C. M., Travison, T. G., et al. (2018). Effect of protein intake on lean body mass in functionally limited older men: A randomized clinical trial. JAMA Internal Medicine, 178(4), 530–541. https://doi.org/10.1001/jamainternmed.2018.0008
Weaver, C. M., Gordon, C. M., Janz, K. F., et al. (2016). The National Osteoporosis Foundation's position statement on peak bone mass development and lifestyle factors. Osteoporosis International, 27(4), 1281–1386. https://doi.org/10.1007/s00198-015-3440-3
Holick, M. F. (2007). Vitamin D deficiency. New England Journal of Medicine, 357(3), 266–281. https://doi.org/10.1056/NEJMra070553
Frost, H. M. (2003). Bone's mechanostat: A 2003 update. The Anatomical Record, 275A(2), 1081–1101. https://doi.org/10.1002/ar.a.10119
Cauley, J. A. (2015). Estrogen and bone health in men and women. Steroids, 99(Pt A), 11–15. https://doi.org/10.1016/j.steroids.2014.12.010
Elbossaty, W. F. (2017). Mineralization of bones in osteoporosis and obesity. Annals of Clinical and Laboratory Science, 47(6), 647–651.
Farr, J. N., & Khosla, S. (2015). Skeletal changes through the lifespan—from growth to senescence. Nature Reviews Endocrinology, 11(9), 513–521. https://doi.org/10.1038/nrendo.2015.89
Boström, P., Wu, J., Jedrychowski, M. P., et al. (2012). A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature, 481(7382), 463–468. https://doi.org/10.1038/nature10777
Rubin, C. T., & Lanyon, L. E. (1985). Regulation of bone mass by mechanical strain magnitude. Calcified Tissue International, 37(4), 411–417.
Hannan, M. T., Felson, D. T., Dawson-Hughes, B., et al. (2000). Risk factors for longitudinal bone loss in elderly men and women: The Framingham Osteoporosis Study. Journal of Bone and Mineral Research, 15(4), 710–720.
Lewiecki, E. M. (2011). New targets for intervention in the treatment of postmenopausal osteoporosis. Nature Reviews Rheumatology, 7(11), 631–638.
Beck, B. R., & Snow, C. M. (2003). Bone health across the lifespan—exercising our options. Exercise and Sport Sciences Reviews, 31(3), 117–122.