Breakthrough Research: Leptin Reduction is Required for Sustained Weight Loss
Discover how leptin—the body’s fat-regulating hormone—shapes hunger, metabolism, and long-term weight loss. Learn the science behind leptin resistance, GLP-1 medications, obesity, and sustainable metabolic health.
OBESITY
Dr. T.S. Didwal, M.D.
5/16/202617 min read
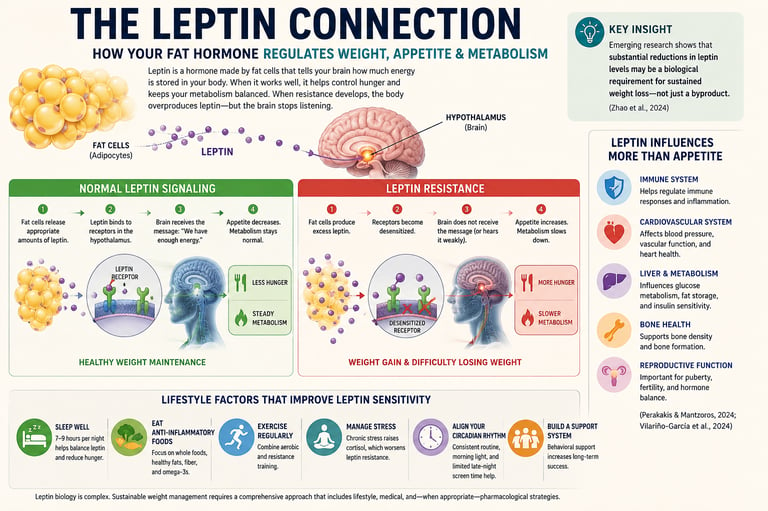
For decades, people struggling with weight were told the solution was simple: eat less, move more, and try harder. But modern obesity science is revealing a far more complex reality. Hidden deep within the body's metabolic circuitry is a powerful hormone called leptin—a chemical messenger produced by fat cells that helps regulate hunger, energy expenditure, and long-term body weight. Increasingly, researchers believe leptin reduction may represent a critical biologic component of durable weight loss. (Obradovic et al., 2021).
In a healthy metabolic state, leptin acts like the body's fuel gauge. When energy stores are sufficient, leptin signals the brain that the body has enough fuel, helping suppress appetite and maintain normal metabolism. But in obesity, this system often begins to malfunction. Fat cells produce progressively larger amounts of leptin, yet the brain becomes resistant to its signals—a phenomenon known as leptin resistance (Hu et al., 2025). The result is a biological paradox: despite excess energy stores, the brain behaves as though the body is starving. Hunger intensifies, cravings increase, and metabolism gradually slows.
This emerging understanding is transforming the field of obesity medicine. Scientists now recognize that successful long-term weight loss may depend not only on reducing calories, but on restoring the brain's sensitivity to leptin itself. Landmark research published in Diabetes in 2024 even suggested that substantial reductions in circulating leptin may be a critical biological component of durable weight loss across lifestyle intervention, bariatric surgery, and modern GLP-1 medications such as semaglutide and tirzepatide (Zhao et al., 2024).
Key Takeaways
Leptin is a hormone produced by fat cells that helps regulate hunger, metabolism, and long-term body weight by signaling the brain about energy stores.
Most people with obesity have high leptin levels, but their brains become resistant to its signals—a condition known as leptin resistance.
Emerging research suggests that meaningful reductions in leptin levels may be an important biological component of sustained weight loss and metabolic reset.
Modern obesity treatments—including GLP-1 medications, bariatric surgery, and intensive lifestyle intervention—may work partly by improving leptin sensitivity.
Sleep, exercise, anti-inflammatory nutrition, stress reduction, and long-term lifestyle consistency can help improve leptin function and support healthier weight regulation.
What Is Leptin Resistance—and Why Does It Matter?
Think of leptin as a key and your brain's hypothalamus as a lock. In a healthy metabolic state, the key fits perfectly: leptin signals arrive at the brain, appetite is modulated, and energy expenditure is appropriate.
In obesity, this system breaks down. Fat cells—being the primary producers of leptin—churn out increasing amounts of the hormone as fat mass grows. But the brain's leptin receptors, overwhelmed by constant signaling, begin to desensitize. The brain effectively stops "hearing" the message, even as leptin levels soar (Hu et al., 2025).
The result? Your brain perceives a state of starvation—despite abundant energy reserves. Hunger intensifies. Metabolism slows. The body fights back against every effort to lose weight.
This is not a willpower problem. This is biology.
Vilariño-García and colleagues (2024) demonstrated that leptin resistance doesn't just affect weight regulation—it connects to a web of metabolic consequences, including cardiovascular risk, type 2 diabetes susceptibility, chronic inflammation, and hormonal dysregulation. Leptin receptors are found not just in the hypothalamus but throughout the body: in the immune system, the cardiovascular system, the liver, and the reproductive organs. When leptin signaling breaks down, the ripple effects are widespread.
The Landmark Discovery: Leptin Reduction Is a Requirement, Not a Side Effect
For decades, researchers assumed that weight loss caused a leptin drop—simply because less fat tissue would naturally produce less of the hormone. A passive consequence of shedding pounds.
A landmark 2024 study published in Diabetes turned that assumption on its head.
Zhao and colleagues examined multiple weight-loss interventions—caloric restriction, bariatric surgery, and pharmacotherapy—across both animal models and human subjects. Their findings were striking: leptin reduction was not merely a result of weight loss. It appeared to be a prerequisite for sustained weight loss.
In other words, interventions that failed to substantially reduce circulating leptin also failed to produce durable weight loss—even when caloric deficits were achieved short-term. The metabolic system simply did not "reset" without a meaningful decrease in leptin levels.
The researchers proposed a compelling mechanism: when chronically elevated leptin drops significantly, the brain's leptin receptors get a chance to recalibrate. Sensitivity is restored. The hypothalamus can finally "hear" leptin's signals again—and respond appropriately by regulating appetite and metabolism (Zhao et al., 2024).
Think of it like turning down a blaring speaker. When the volume has been deafeningly loud for years, even normal sound seems quiet by comparison. Only by turning the volume down—substantially and consistently—can your ears adjust to normal hearing again.
The Genetics of Leptin: Why Some People Struggle More
Not everyone is equally vulnerable to leptin resistance—and increasingly, researchers are discovering that genetics plays a meaningful role.
A 2025 study by Durak and colleagues investigated variations in the LEP (leptin) gene and the LEPR (leptin receptor) gene in individuals with obesity. Their findings confirmed that specific genetic variants are associated with altered leptin production and reduced receptor sensitivity—explaining why some people develop severe obesity early in life while others with similar diets and activity levels remain metabolically healthier.
This doesn't mean destiny is fixed. But it does mean that a person carrying certain LEP or LEPR variants may need more aggressive intervention to achieve the same degree of leptin reduction and metabolic reset that another person achieves with moderate lifestyle changes (Durak et al., 2025).
This emerging field of leptin genetics is reshaping how clinicians think about personalized obesity medicine. In the near future, genetic screening may help identify who is most likely to benefit from pharmacotherapy versus intensive lifestyle intervention—and at what dose or intensity.
How Modern Weight-Loss Medications Work Through Leptin
The explosion of GLP-1 receptor agonists—medications like semaglutide (Ozempic, Wegovy) and dual GIP/GLP-1 agonists like tirzepatide (Mounjaro, Zepbound)—has transformed the treatment of obesity in recent years. And the leptin connection helps explain precisely why these drugs work as well as they do.
GLP-1 agonists reduce appetite by mimicking gut hormones that signal satiety to the brain, slow gastric emptying, and improve insulin secretion. Clinical trials have shown weight loss of 10–15% of body weight with semaglutide, and up to 20% or more with tirzepatide (Brandfon et al., 2023).
But here's the key insight: as fat mass decreases through medication-induced caloric reduction, leptin production falls proportionally. This drop in circulating leptin—large enough and sustained enough—is what allows the hypothalamus to regain sensitivity. The medication creates what researchers now call a "leptin-permissive state": biological conditions under which the brain can reset its leptin receptors and restore meaningful appetite regulation.
Beyond lowering leptin indirectly through fat mass reduction, GLP-1 medications also act upstream on hypothalamic pro-opiomelanocortin (POMC) neurons—the same appetite-regulating neural pathways targeted by leptin itself. This overlapping neurobiology may help explain the powerful synergy between GLP-1 signaling, appetite suppression, and long-term metabolic regulation.
This explains a frustrating clinical observation that puzzled doctors for years: why do some patients regain significant weight after stopping GLP-1 medications, even after substantial initial loss?
The answer lies in leptin regulation. Once the medication is discontinued, caloric intake often returns toward previous levels, fat mass begins to rebuild, and leptin climbs back toward its original, elevated—and resistance-inducing—baseline. The brain's receptors, not having had time to permanently recalibrate, slip back into their desensitised state. Compensatory hunger mechanisms reactivate (Brandfon et al., 2023).
This is why obesity medicine specialists increasingly frame obesity as a chronic disease requiring long-term management, not a condition to be "fixed" and then left unattended.
Intensive Lifestyle Intervention: A Legitimate Path to Leptin Reset
Medications rightly receive significant attention, but here's something the research makes abundantly clear: intensive lifestyle intervention can produce leptin reduction comparable to pharmacotherapy or bariatric surgery.
The operative word is intensive.
Zhao and colleagues (2024) found that comprehensive lifestyle programs—combining significant caloric restriction, structured exercise (both aerobic and resistance training), behavioral counseling, sleep optimization, and stress management—produced meaningful reductions in circulating leptin levels when participants lost 10–15% of body weight. In some individuals, leptin concentrations dropped by 40–50%.
This is not the effect of a casual "eat a little less and walk a bit more" approach. It is the result of a structured, multi-component program pursued consistently over months. When all the elements work in synergy, the biological outcomes can be genuinely transformative.
The mechanisms are multiple and interconnected:
Reduced fat mass directly lowers leptin production, since adipocytes are the primary source. This is the most direct pathway.
Reduced inflammation plays a critical supporting role. Chronic low-grade inflammation—common in obesity—contributes to leptin resistance by impairing receptor signaling pathways. Anti-inflammatory dietary patterns rich in omega-3 fatty acids, polyphenols, and fiber; combined with regular exercise; create a less inflamed cellular environment in which leptin receptors can function more normally (Obradovic et al., 2021).
Improved insulin sensitivity works synergistically with leptin signaling through shared intracellular pathways. Exercise and caloric restriction improve insulin sensitivity, which appears to have downstream benefits for leptin receptor responsiveness.
Sleep optimization addresses a frequently overlooked driver of leptin resistance. Sleep deprivation disrupts the hormonal axis that governs leptin and its counterpart, ghrelin (the hunger-stimulating hormone). Getting consistent, adequate sleep—7 to 9 hours nightly—helps normalize this balance and reduces leptin resistance (Zhao et al., 2024).
Stress reduction lowers cortisol, a hormone that, when chronically elevated, promotes visceral fat accumulation and worsens leptin signaling.
The challenge is not whether these lifestyle components can reset the leptin system—the evidence shows they can. The challenge is sustaining the intensity required over the long term, especially as the body fights back with increased hunger and reduced metabolic rate as leptin falls. This biological resistance to weight loss is not a personal failure; it is an evolutionarily programmed survival mechanism. For many patients, combining lifestyle intervention with pharmacological support represents the most realistic path to durable success.
Leptin's Broader Role: Beyond Appetite
Leptin's influence extends well beyond hunger regulation—a fact that has opened promising new clinical frontiers.
Research compiled by Perakakis and Mantzoros (2024) documented leptin's established and emerging clinical applications in several specialized contexts:
Hypothalamic amenorrhea: In women with very low body fat due to extreme exercise or restrictive eating, leptin levels fall below the threshold needed to sustain reproductive function. Leptin therapy has successfully restored menstrual cycles in carefully selected patients with this condition.
Lipodystrophy syndromes: In rare conditions where fat tissue is abnormally absent or redistributed, patients develop severe metabolic complications including extreme insulin resistance and triglyceride accumulation. Metreleptin—a synthetic leptin analogue—has received FDA approval for some of these patients with remarkable metabolic benefit.
Immune regulation: Leptin modulates both innate and adaptive immunity. Low leptin states suppress immune responses, while leptin resistance may contribute to chronic inflammatory conditions (Vilariño-García et al., 2024).
Bone metabolism: Leptin signaling influences bone density and turnover, suggesting future applications in osteoporosis research.
Crucially, while leptin therapy is highly effective in the rare condition of congenital leptin deficiency—where individuals truly cannot produce the hormone—it does not work for typical obesity, where the problem is receptor resistance, not hormonal absence. Adding more leptin to an already leptin-saturated system does not restore sensitivity (Perakakis & Mantzoros, 2024).
Leptin, Cardiovascular Disease, and Type 2 Diabetes: The Metabolic Triangle
The consequences of sustained leptin resistance reach far beyond weight gain.
Vilariño-García and colleagues (2024) provided a comprehensive analysis of how disrupted leptin signaling contributes to two of the world's most prevalent chronic diseases: cardiovascular disease and type 2 diabetes.
Leptin resistance promotes visceral fat accumulation—the most metabolically dangerous fat depot, surrounding abdominal organs and actively contributing to systemic inflammation. This visceral fat releases pro-inflammatory cytokines that damage blood vessel walls, impair insulin receptor function, and elevate cardiovascular risk.
Simultaneously, leptin resistance and insulin resistance frequently coexist and reinforce each other. As both systems fail, blood sugar regulation deteriorates, lipid profiles worsen, and blood pressure rises. The result is the well-recognized cardiometabolic syndrome that significantly elevates risk for heart attack, stroke, and kidney disease.
Understanding leptin resistance as a central driver of this metabolic cluster—rather than treating each condition in isolation—represents a more effective and physiologically coherent approach to preventive medicine.
The Hidden Metabolic Slowdown: Why the Body Fights Weight Loss
One of the most important—but often overlooked—aspects of weight loss is adaptive thermogenesis, sometimes called the body's “metabolic defense system.” As leptin levels fall during weight loss, the brain responds by conserving energy in multiple ways. Resting energy expenditure declines, meaning the body burns fewer calories at rest than expected for its new body size. Simultaneously, thyroid hormone activity may decrease and sympathetic nervous system signaling can slow, further reducing daily energy expenditure. This biologic adaptation evolved to protect humans from starvation, but in modern obesity treatment it can make long-term weight maintenance extraordinarily difficult. In essence, the body does not simply resist hunger—it also becomes metabolically more efficient, requiring fewer calories to function after weight loss. This helps explain why sustained obesity treatment often requires ongoing lifestyle support, pharmacotherapy, or both.
Obesity Is More Than Hormones Alone
While leptin plays a central role in weight regulation, modern obesity science recognizes that body weight is shaped by far more than hormones alone. Today's food environment—dominated by ultra-processed, calorie-dense foods engineered for hyper-palatability—interacts with chronic sleep disruption, sedentary lifestyles, circadian rhythm disturbance, psychological stress, socioeconomic pressures, neurobiology, and genetic susceptibility. These factors continuously influence appetite, reward pathways, inflammation, and energy expenditure. In reality, obesity emerges from the complex interaction between biology and environment, which is why effective treatment often requires both medical and societal approaches rather than relying on individual willpower alone.
Practical Applications: What You Can Do Starting Today
Understanding leptin biology is not just an academic exercise. Translated into daily habits, this science offers a clear framework for action.
1. Prioritize Sleep as a Medical Priority
Sleep deprivation is one of the most potent drivers of leptin resistance that most people underestimate. Consistent, high-quality sleep of 7–9 hours nightly supports healthy leptin-ghrelin balance and reduces appetite dysregulation. If you struggle with insomnia or sleep apnea, addressing these conditions is as important as any dietary change.
2. Pursue an Anti-Inflammatory Diet
A dietary pattern rich in vegetables, legumes, whole grains, fatty fish, olive oil, nuts, and berries reduces systemic inflammation—directly improving the cellular environment in which leptin receptors operate. Minimizing ultra-processed foods, refined carbohydrates, and excess added sugars reduces leptin-disrupting inflammatory load (Hu et al., 2025).
3. Combine Aerobic and Resistance Exercise
Both forms of exercise contribute to leptin normalization through complementary mechanisms. Aerobic exercise reduces fat mass and improves insulin sensitivity. Resistance training builds metabolically active muscle tissue that improves overall energy utilization. Aim for at least 150 minutes of moderate aerobic activity per week plus two resistance sessions.
4. Manage Chronic Stress Deliberately
Chronically elevated cortisol promotes visceral fat accumulation and worsens leptin signaling. Practices including mindfulness meditation, yoga, time in nature, and adequate boundaries around work and digital consumption have measurable effects on cortisol and downstream metabolic health.
5. Avoid Extreme Yo-Yo Dieting
Rapid cycles of severe restriction followed by overeating may worsen leptin resistance over time. A more gradual, sustained approach to caloric reduction—one that can be maintained—produces more durable leptin normalization than repeated crash dieting (Zhao et al., 2024).
6. Discuss Pharmacotherapy Openly with Your Doctor
If lifestyle interventions alone have not produced adequate or sustained weight loss, anti-obesity medications deserve serious consideration as first-line treatment—not a last resort. Modern GLP-1 and dual-receptor agonists work through mechanisms that directly support leptin normalization. This is a medical decision, not a personal failure.
7. Support Your Microbiome
Emerging research suggests gut microbiome composition influences systemic inflammation and leptin sensitivity. A fiber-rich, diverse diet supports a healthier microbiome—adding another pathway through which dietary choices influence leptin regulation.
Frequently Asked Questions
Q1: What exactly is leptin, and why does it matter for weight management?
Leptin is a hormone produced by fat cells that communicates your body's energy status to the brain. It functions as a satiety signal—when leptin levels are adequate and the brain is responding to them, appetite is modulated and metabolism runs normally. Groundbreaking research now shows that achieving a meaningful, sustained reduction in leptin is not just a side effect of weight loss, but appears to be a biological requirement for it (Zhao et al., 2024). Without this hormonal shift, the body's metabolic set-point does not reset, and weight regain becomes likely.
Q2: I have obesity—does that mean my leptin is too low?
Counterintuitively, no. Most people with obesity have elevated leptin levels because more fat tissue produces more leptin. The problem is leptin resistance—the brain's receptors become desensitized to the hormone's signals, even at high concentrations. The brain therefore behaves as though the body is starving, driving hunger and reducing metabolism despite adequate—or excessive—energy stores (Obradovic et al., 2021).
Q3: Can I take leptin as a supplement or medication to help me lose weight?
For the vast majority of people with obesity, leptin supplementation does not work. Since the problem is receptor resistance rather than leptin deficiency, adding more leptin to an already-saturated system does not restore sensitivity. Leptin therapy is effective only in the rare condition of congenital leptin deficiency—a genetic disorder affecting less than 1% of obesity cases—and in certain lipodystrophy syndromes. For everyone else, the goal is to reduce leptin levels by losing fat mass and improve receptor sensitivity through lifestyle and medical interventions (Perakakis & Mantzoros, 2024).
Q4: Why do so many people regain weight after stopping GLP-1 medications like semaglutide?
When GLP-1 medications are discontinued, caloric intake often returns toward previous patterns. Fat mass begins rebuilding, and leptin levels climb back toward their pre-treatment, resistance-inducing baseline. Without the sustained leptin reduction that the medication was helping to maintain, the brain's receptors re-enter their desensitized state, compensatory hunger mechanisms reactivate, and metabolic rate adjusts downward. This is why obesity medicine specialists now emphasize long-term management rather than short-term treatment (Brandfon et al., 2023).
Q5: Can lifestyle changes really reduce leptin as effectively as medication?
Yes—when truly intensive. Research shows that comprehensive programs combining significant caloric restriction, structured aerobic and resistance exercise, behavioral counseling, adequate sleep, and stress management can reduce circulating leptin by 40–50% in participants who lose 10–15% of their body weight. The biological outcome is comparable to what medications or bariatric surgery produce. The challenge is sustaining this level of behavioral change over the long term, which is why combining lifestyle modifications with pharmacological support often produces the best outcomes for many patients (Zhao et al., 2024).
Q6: Do genetics influence my leptin levels and resistance?
Yes, and this is an active area of research. Variations in the LEP gene (which governs leptin production) and the LEPR gene (which governs receptor function) have been associated with increased obesity risk and altered metabolic responses (Durak et al., 2025). Individuals carrying certain variants may produce leptin abnormally or have receptors that are inherently less sensitive—potentially explaining why some people develop severe obesity early in life or respond differently to standard interventions. Genetic testing in obesity medicine is still developing but holds promise for more personalized treatment guidance.
Q7: Is leptin resistance reversible?
Yes—and this is one of the most hopeful messages in obesity research. While severe leptin resistance can take months or years to meaningfully reverse, sustained weight loss through lifestyle change, medication, surgery, or a combination of all three does restore leptin sensitivity over time. The key factors appear to be the degree of leptin reduction achieved, the duration it is maintained, and the overall metabolic environment created by anti-inflammatory diet, exercise, and sleep (Hu et al., 2025). The biology is not fixed; it is responsive.
Clinical pearls.
1. The Paradoxical Nature of Leptin Resistance
Scientific Tone: In obesity, hyperleptinemia fails to suppress appetite or stimulate energy expenditure due to the desensitization and downregulation of central leptin receptors (LEPR) within the arcuate nucleus of the hypothalamus. This establishes a state of neuroendocrine resistance where elevated peripheral adiposity paradoxically mimics central starvation signaling.
Having obesity doesn't mean you lack the "fullness hormone" leptin—it actually means your body is making too much of it. Because the brain is constantly flooded with leptin, it tunes out the signal. Your brain genuinely believes you are starving, which triggers intense hunger and slows your metabolism, despite having plenty of stored energy.
2. Leptin Reduction as a Weight Loss Prerequisite
Scientific Tone: A critical metabolic reset requires a significant, sustained reduction in circulating serum leptin levels, rather than a mere passive decline proportional to adiposity reduction. According to Zhao et al. (2024), profound leptin reduction is an obligate requirement for restoring hypothalamic receptor sensitivity and establishing a durable metabolic set-point.
Losing weight isn't just about cutting calories; it's about giving your brain a biological "volume adjustment." To fix leptin resistance, your overall leptin levels have to drop significantly so your brain can reset. Think of it like turning down blaring music—only when the volume is lowered can your brain finally "hear" the fullness signals again.
3. The Reversibility of Receptor Sensitivity
Scientific Tone: Hypothalamic leptin resistance is a reversible pathology, provided the systemic inflammatory load is mitigated and a "leptin-permissive state" is maintained. Reversal requires prolonged downregulation of signaling to allow receptor recalibration, alongside the suppression of pro-inflammatory cytokines that disrupt intracellular leptin pathways.
Leptin resistance is not a permanent life sentence; your body's biology is highly adaptable. By achieving steady weight loss and lowering inflammation, you can actually repair the communication between your fat cells and your brain, making your body naturally better at regulating your appetite over time.
4. Why Weight Regain Occurs Post-GLP-1 Cessation
Scientific Tone: Discontinuation of GLP-1 or dual GIP/GLP-1 receptor agonist therapy often induces rapid weight rebound because peripheral leptin levels abruptly rise back toward the pre-treatment, resistance-inducing baseline before permanent hypothalamic recalibration can occur, reactivating compensatory orexigenic (hunger-stimulating) pathways.
Many people regain weight after stopping medications like Ozempic or Mounjaro because the underlying hormonal imbalance hasn't permanently changed. Once the medication is gone, leptin levels spike back up to their old, elevated baseline, throwing the brain right back into a state of leptin resistance and triggering intense, biological hunger.
5. The Necessity of "Intensive" Lifestyle Intervention
Scientific Tone: Casual lifestyle modifications are insufficient to alter leptin dynamics. Reversing leptin resistance requires intensive, multi-component intervention—combining caloric restriction, structured resistance and aerobic training, and sleep optimisation—to yield a 40–50% reduction in circulating leptin and downregulate systemic inflammation.
A casual "eat a bit less and walk a bit more" approach won't cut it when trying to reset your hormones. To truly fix leptin resistance naturally, you need an intensive, structured routine. Combining targeted exercise, an anti-inflammatory diet, deep sleep, and stress management creates a powerful synergy that forces your leptin levels down and fixes your metabolism.
6. Genetic Variations Dictate Clinical Outcomes
Scientific Tone: Polymorphisms within the LEP and LEPR genes dictate individual baselines for leptin production and receptor binding affinity. Patients harboring adverse genetic variants display heightened vulnerability to early-onset obesity and metabolic resistance, necessitating highly individualized, aggressive clinical strategies.
Your DNA plays a massive role in how your body handles weight. Variations in your weight-regulating genes mean your brain receptors might naturally be less sensitive to leptin than someone else's. If you struggle more than others on the same diet, it's a reflection of your unique genetic blueprint, not a lack of willpower.
A Clinician’s Perspective
As clinicians, we are witnessing a major shift in how obesity is understood and treated. For many years, patients struggling with weight were often given oversimplified advice centered almost entirely on calorie restriction and personal discipline. Yet modern metabolic research increasingly shows that obesity is deeply rooted in complex biological systems involving hormones, neurocircuitry, inflammation, genetics, sleep physiology, and environmental influences. Leptin sits at the center of many of these pathways.
In clinical practice, one of the most important lessons is that the body actively defends its existing weight. Patients frequently describe intense hunger, fatigue, cravings, and weight regain after dieting—not because they “lack motivation,” but because powerful adaptive mechanisms are working to restore lost weight. Understanding leptin resistance and metabolic adaptation helps explain why long-term weight management can be extraordinarily difficult even in highly motivated individuals.
Equally important, this emerging science is helping reduce stigma. Obesity should not be viewed as a simple failure of willpower, but as a chronic, relapsing metabolic disease that deserves evidence-based medical care, compassion, and long-term support. Lifestyle intervention remains foundational, but for many patients, medications such as GLP-1 receptor agonists, structured behavioral therapy, or bariatric surgery may be medically appropriate tools—not shortcuts.
Perhaps most encouraging is that leptin biology is not fixed. Sustained improvements in sleep, nutrition quality, physical activity, stress management, and body composition can gradually improve metabolic health and restore healthier signaling pathways over time. The future of obesity medicine is increasingly personalized, combining lifestyle medicine, pharmacotherapy, behavioral science, and precision metabolic care to help patients achieve durable, realistic, and healthier outcomes.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with qualified healthcare professionals before starting any weight-loss treatment or making significant changes to your health regimen.
Related Articles
References
Brandfon, S., Eylon, A., Khanna, D., & Parmar, M. S. (2023). Advances in anti-obesity pharmacotherapy: Current treatments, emerging therapies, and challenges. Cureus, 15(10), e46623. https://doi.org/10.7759/cureus.46623
Durak, S., Aksoyer Sezgin, S. B., Celik, F., et al. (2025). The investigation of leptin (LEP) and leptin receptor (LEPR) gene variations in obese patients. Clinical and Translational Metabolism, 23, 6. https://doi.org/10.1007/s12018-025-09308-8
Hu, W., Zhu, H., & Gong, F. (2025). Leptin and leptin resistance in obesity: Current evidence, mechanisms and future directions. Endocrine Connections, 14(9), Article e25-0521. https://doi.org/10.1530/EC-25-0521
Obradovic, M., Sudar-Milovanovic, E., Soskic, S., Essack, M., Arya, S., Stewart, A. J., Gojobori, T., & Isenovic, E. R. (2021). Leptin and obesity: Role and clinical implication. Frontiers in Endocrinology, 12, 585887. https://doi.org/10.3389/fendo.2021.585887
Perakakis, N., & Mantzoros, C. S. (2024). Evidence from clinical studies of leptin: Current and future clinical applications in humans. Metabolism: Clinical and Experimental, 161, 156053. https://doi.org/10.1016/j.metabol.2024.156053
Vilariño-García, T., Polonio-González, M. L., Pérez-Pérez, A., Ribalta, J., Arrieta, F., Aguilar, M., Obaya, J. C., Gimeno-Orna, J. A., Iglesias, P., Navarro, J., Durán, S., Pedro-Botet, J., & Sánchez-Margalet, V. (2024). Role of leptin in obesity, cardiovascular disease, and type 2 diabetes. International Journal of Molecular Sciences, 25(4), 2338. https://doi.org/10.3390/ijms25042338
Zhao, S., Li, N., Xiong, W., Li, G., He, S., Zhang, Z., Zhu, Q., Jiang, N., Ikejiofor, C., Zhu, Y., Wang, M. Y., Han, X., Zhang, N., Solis-Herrera, C., Kusminski, C., An, Z., Elmquist, J. K., & Scherer, P. E. (2024). Leptin reduction as a required component for weight loss. Diabetes, 73(2), 197–210. https://doi.org/10.2337/db23-0571