How Insulin Resistance Accelerates Cardiovascular Aging
Insulin resistance is a silent saboteur. Read the latest research on vascular stiffening, endothelial damage, and metabolic interventions to reverse heart aging.
DIABETESHEART
Dr. T.S. Didwal, M.D.
4/29/202616 min read
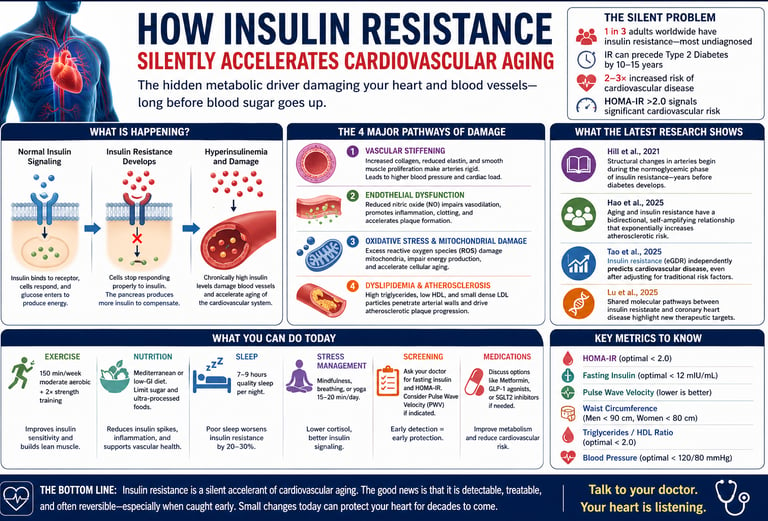
Insulin resistance accelerates cardiovascular aging by damaging blood vessels long before diabetes develops. It causes arterial stiffening, reduces nitric oxide (leading to poor vessel relaxation), increases oxidative stress, and disrupts lipid metabolism. Even with normal blood sugar levels, elevated insulin can silently raise heart disease risk. Early detection using HOMA-IR and targeted interventions—especially exercise, diet, sleep optimisation, and medications such as metformin or GLP-1 agonists—can significantly slow or reverse this process
Key Mechanisms
Four ways insulin resistance accelerates cardiovascular aging:
Arterial stiffening from structural remodeling
Endothelial dysfunction due to nitric oxide depletion
Oxidative stress and mitochondrial damage
Atherogenic dyslipidemia (high triglycerides, low HDL, small dense LDL)
Key Factors Driving Cardiovascular Damage
Hyperinsulinemia
Promotes chronic vascular inflammation
Accelerates early atherosclerotic changes
Reduced Nitric Oxide
Impairs vasodilation
Decreases arterial flexibility and increases vascular tone
Oxidative Stress
Damages endothelial cells
Contributes to mitochondrial dysfunction and vascular aging
Dyslipidemia
Increases triglycerides and small dense LDL particles
Accelerates plaque formation and progression of atherosclerosis
Takeaway
These interconnected mechanisms explain how insulin resistance silently drives cardiovascular disease—even before symptoms or abnormal glucose levels appear.
Why Insulin Resistance Demands Early Action
Insulin resistance (IR) should be recognized as a primary cardiovascular disease driver—not merely a precursor to diabetes. Even in normoglycemic individuals, compensatory hyperinsulinemia initiates endothelial injury, vascular inflammation, and early atherogenesis (Caturano et al., 2024; Fazio et al., 2024).
Standard screening tools are insufficient. Normal fasting glucose and HbA1c often mask years of underlying metabolic dysfunction. Incorporating fasting insulin and calculating HOMA-IR enables earlier identification of high-risk patients (Fazio et al., 2024).
Vascular damage begins early and progresses silently. Arterial stiffening—detectable via Pulse Wave Velocity—can develop during the insulin-resistant, non-diabetic phase, reflecting structural remodeling long before clinical events (Hill et al., 2021).
Endothelial dysfunction is the central mechanistic link. Reduced bioavailability of Nitric Oxide promotes vasoconstriction, thrombosis, and plaque instability, accelerating cardiovascular aging (Caturano et al., 2024).
At the cellular level, IR accelerates biological aging. Mitochondrial dysfunction, oxidative stress, and impaired autophagy create a pro-senescent environment that compounds cardiovascular risk over time (Li et al., 2024; Lu et al., 2025).
Importantly, this trajectory is modifiable. Structured exercise, targeted nutrition, and early pharmacologic intervention—when indicated—can restore insulin sensitivity and meaningfully reduce long-term cardiovascular risk (Hao et al., 2025; Tao et al., 2025).
Clinical takeaway: By the time dysglycemia appears, vascular aging is already well underway. Identifying and treating insulin resistance early offers a critical opportunity to alter the natural history of cardiovascular disease.
What You Will Learn in This Article
Insulin resistance is not just a blood sugar problem — it is one of the most powerful accelerators of cardiovascular aging known to modern medicine. In this evidence-based guide, you will discover the molecular mechanisms behind vascular stiffening, why standard glucose tests often miss insulin resistance, how aging and metabolic dysfunction feed each other in a dangerous cycle, and what specific lifestyle and pharmacological interventions can reverse the damage before it becomes permanent.
Imagine sending a text message to a friend who has turned off notifications. You keep sending messages — your phone works perfectly — but nothing goes through. This is essentially what happens in your body when insulin resistance develops. Your pancreas produces insulin (the message), but your cells progressively stop listening. To compensate, the pancreas sends more and more insulin. The result is a state called hyperinsulinemia — chronically elevated insulin levels that silently damage your heart and blood vessels long before any blood sugar abnormality appears on a standard lab test.
According to Fazio et al. (2024), insulin resistance and hyperinsulinemia represent a critically underestimated cardiovascular risk factor — one that most clinicians and patients overlook because fasting glucose and HbA1c appear normal for years, even decades, while vascular damage accumulates underneath. By the time diabetes is diagnosed, the heart may already be years — or even decades — older than its chronological age.
This article synthesizes the most current peer-reviewed evidence on this topic, drawing from groundbreaking research published in Frontiers in Endocrinology, Cardiovascular Diabetology, Metabolites, and International Journal of Molecular Sciences. Whether you are a patient trying to understand your risk, a caregiver supporting a loved one, or simply someone who wants to age with a healthy heart, this guide is for you.
5 Critical Clinical Insights Every Patient Should Know
These evidence-based insights translate complex research into practical actions you can discuss with your physician.
1. Screen Beyond Blood Sugar: Ask for HOMA-IR
Normal fasting glucose or HbA1c does not exclude cardiometabolic risk. Insulin resistance often develops silently for 10–15 years before diabetes is diagnosed, during which elevated insulin levels (hyperinsulinemia) begin damaging blood vessels. Measuring fasting insulin and calculating HOMA-IR provides earlier detection.
Clinical signal: HOMA-IR >2.0 or fasting insulin >12 mIU/mL suggests increased cardiovascular risk—even when glucose appears normal (Fazio et al., 2024).
2. Protect Your Arteries Early: Insulin Resistance Drives Stiffening
Healthy arteries are elastic. Insulin resistance disrupts this by increasing collagen deposition and reducing nitric oxide, leading to progressive arterial rigidity. This process—detectable using Pulse Wave Velocity—often begins before symptoms or diabetes develop.
Why it matters: Arterial stiffness increases cardiac workload and is an early marker of cardiovascular aging (Hill et al., 2021).
3. Aging + Insulin Resistance = Exponential Risk
Aging and insulin resistance amplify each other. As metabolic function declines with age, insulin signaling worsens; in turn, insulin resistance accelerates biological aging.
Key insight: Cardiovascular risk rises exponentially, not gradually, in older adults with insulin resistance—making early intervention in midlife critical (Hao et al., 2025).
4. The Real Damage Happens at the Cellular Level
Insulin resistance accelerates biological aging through mitochondrial dysfunction, oxidative stress, and impaired cellular repair (autophagy).
Clinical implication: Therapies such as Metformin and GLP-1 receptor agonists may provide benefits beyond glucose control by improving cellular energy function and reducing metabolic stress (Li et al., 2024).
5. Exercise Is the Most Potent First-Line Therapy
Structured physical activity is the most effective way to improve insulin sensitivity. Skeletal muscle is the body’s primary site for glucose uptake, and resistance training expands this capacity.
Evidence-based prescription:
≥150 minutes/week moderate aerobic activity
≥2 sessions/week resistance training
Takeaway: Specific, consistent exercise delivers measurable metabolic improvement within weeks—far outperforming vague advice to “stay active.”The Science Explained:
How Insulin Resistance Ages Your Heart and Arteries
Understanding how insulin resistance harms your cardiovascular system helps make sense of why specific interventions work and why early action matters so much. The damage unfolds through four interrelated pathways.
Pathway 1: Vascular Stiffening and Structural Remodeling
Insulin-resistant states alter the very composition of arterial walls. They promote increased collagen deposition, reduce elastin content, and stimulate vascular smooth muscle cell proliferation. The net result is arteries that progressively lose their natural springiness. The large arteries — particularly the aorta — become rigid, forcing the heart to work significantly harder with every beat. Over years, this excess workload leads to left ventricular hypertrophy and, eventually, heart failure (Hill et al., 2021). Pulse Wave Velocity (PWV) measurement can detect this stiffening years before symptoms arise.
Pathway 2: Endothelial Dysfunction and Nitric Oxide Depletion
The endothelium — the single-cell-thick lining of every blood vessel in your body — is extraordinarily sensitive to metabolic dysfunction. Insulin resistance impairs endothelial function primarily by depleting nitric oxide (NO), a signaling molecule that keeps blood vessels relaxed, prevents clot formation, and inhibits atherosclerotic plaque growth. With reduced NO, vessels constrict more easily, platelets aggregate more readily, and plaques form and progress faster. Simultaneously, systemic inflammation rises, increasing circulating pro-inflammatory cytokines that further destabilize plaques, making them more likely to rupture (Caturano et al., 2024).
Pathway 3: Oxidative Stress and Mitochondrial Failure
Insulin-resistant cells generate excessive reactive oxygen species (ROS) — damaging molecules that attack cellular structures. This oxidative burden is particularly destructive to mitochondria, the energy-producing organelles inside heart muscle cells and endothelial cells. As mitochondrial function deteriorates, these cells generate less energy, accumulate damage faster, and enter premature senescence. The result is accelerated cardiovascular aging at the cellular level — a process that is largely invisible on standard blood tests but detectable through biomarkers like fasting insulin (Lu et al., 2025).
Pathway 4: Dyslipidemia and Coronary Artery Disease Risk
Insulin resistance profoundly disrupts lipid metabolism. It promotes elevated triglycerides, suppresses HDL cholesterol ("good" cholesterol), and shifts LDL particles toward smaller, denser forms that penetrate arterial walls more easily. Tao et al. (2025) demonstrated in a nationwide prospective cohort study that insulin resistance — quantified by estimated glucose disposal rate (eGDR) — independently predicts cardiovascular disease incidence, even after controlling for traditional risk factors. This finding establishes insulin resistance itself as a modifiable cardiovascular risk factor, not merely a diabetes precursor.
What the Latest Research Is Telling Us
The past three years have brought remarkable advances in our understanding of the insulin resistance–cardiovascular aging axis. Here is a balanced synthesis of the most impactful studies.
Cardiovascular Stiffening and Disease Mechanisms: The Foundational Framework
This landmark mechanistic study buy Hill et al. (2021) established the molecular chain of events connecting hyperinsulinemia to structural arterial changes. By characterizing how insulin signaling dysfunction activates pathways that promote vascular smooth muscle cell proliferation and extracellular matrix deposition, the researchers established the biological plausibility for cardiovascular interventions targeting metabolic dysfunction at the earliest possible stage. Critically, the study demonstrated that these structural changes — arterial wall thickening and stiffening — can begin during the normoglycemic phase of insulin resistance, years before any glucose abnormality is detectable. This finding has profound implications for how we screen and intervene in at-risk populations.
Key clinical implication: Waiting for blood sugar elevation before addressing insulin resistance means cardiovascular damage has already been accumulating for years. Structural arterial changes may be partially irreversible, reinforcing the case for early, proactive metabolic screening.
Aging and Insulin Resistance: A Bidirectional, Self-Amplifying Relationship
Investigation by Hao et al. (2025) in Metabolites is one of the most comprehensive explorations of the age–insulin resistance interaction published to date. The researchers documented that aging impairs insulin signaling at multiple levels simultaneously: glucose transporter translocation becomes sluggish, mitochondrial oxidative capacity declines, and cellular repair mechanisms become less efficient. Meanwhile, the accumulating metabolic dysfunction accelerates biological aging beyond what calendar years alone would produce. In older adults with established insulin resistance, atherosclerotic risk compounds exponentially — not merely additively — compared to age-matched peers without metabolic dysfunction. This bidirectional relationship means that preventing insulin resistance in younger and middle-aged adults effectively pays a cardiovascular dividend for decades.
Key clinical implication: Aggressive lifestyle intervention in patients aged 30–55 with insulin resistance prevents the entrenchment of metabolic dysfunction and delivers greater lifetime cardiovascular protection than later-stage pharmacological intervention.
eGDR as a Cardiovascular Predictor: A Nationwide Prospective Cohort Study
Using data from a large nationwide prospective cohort,Tao et al. (2025).demonstrated that the estimated glucose disposal rate (eGDR) — a clinically calculable metric derived from waist circumference, HbA1c, and hypertension status — is a powerful independent predictor of incident cardiovascular disease. Importantly, this predictive association held after adjustment for traditional cardiovascular risk factors including blood pressure, cholesterol, and smoking status. This research provides clinicians with a practical, no-cost tool for cardiovascular risk stratification using information already available in the patient record.
Key clinical implication: eGDR can be calculated at any clinic visit with existing patient data, offering an accessible way to identify insulin-resistant patients at elevated cardiovascular risk before a diabetes diagnosis is made.
Bioinformatics Insights into Coronary Heart Disease and Insulin Resistance
Using advanced bioinformatics approaches including gene co-expression network analysis, Lu et al. (2025) identified shared molecular signatures between insulin resistance and coronary heart disease. The study identified specific hub genes and molecular pathways that are dysregulated in both conditions, providing evidence that the two disorders share deep biological roots rather than being sequentially linked conditions. This genomic perspective opens promising therapeutic avenues — targeting these shared pathways may simultaneously improve insulin sensitivity and reduce coronary risk, rather than requiring separate treatments for each condition.
Key clinical implication: The shared molecular architecture of insulin resistance and coronary artery disease supports the use of metabolic therapies (GLP-1 agonists, SGLT-2 inhibitors) as cardiovascular disease treatments in their own right, not merely as glucose-lowering agents.
The Cardiovascular Consequences: What Happens When Insulin Resistance Goes Untreated
Atherosclerosis and Plaque Formation
Insulin resistance creates a pro-atherosclerotic environment through multiple mechanisms. Elevated insulin levels directly stimulate vascular smooth muscle cell proliferation, promoting atherosclerotic plaque development (Hill et al., 2021). Additionally, insulin resistance impairs the clearance of atherogenic lipoproteins, allowing them to accumulate in arterial walls where they undergo oxidation and inflammatory processing.
The atherosclerotic plaques that develop in insulin-resistant individuals tend to be more lipid-rich, more inflammatory, and more unstable—characteristics associated with increased risk of acute plaque rupture and myocardial infarction. The interaction between insulin resistance and atherogenesis appears to be particularly problematic in aging populations, where multiple additional risk factors often coexist (Hao et al., 2025).
Hypertension and Left Ventricular Changes
Insulin resistance is intimately linked with hypertension development. Hyperinsulinemia increases sympathetic nervous system activation, promotes sodium retention by the kidneys, and induces endothelial dysfunction—all of which elevate blood pressure. The resulting hypertension, combined with cardiovascular stiffening from insulin resistance, promotes left ventricular hypertrophy and diastolic dysfunction.
Over time, these changes can progress to heart failure with preserved ejection fraction (HFpEF), a condition increasingly common in insulin-resistant populations and notoriously difficult to treat. The contribution of insulin resistance to heart failure development has become increasingly appreciated in recent years, with recognition that metabolic dysfunction represents a primary driver of HFpEF pathophysiology.
Thrombotic Complications
Insulin-resistant states promote a prothrombotic environment by increasing platelet reactivity, elevating procoagulant factors, and reducing anticoagulant mechanisms. This increased thrombotic tendency, combined with the plaque instability promoted by insulin resistance, substantially increases the risk of acute thrombotic events, including stroke and myocardial infarction.
Practical Applications: What You Can Do Today
Translating evidence into action—these are clinically grounded steps to reduce insulin resistance and protect cardiovascular health.
Exercise
Aim for ≥150 minutes/week of moderate aerobic activity (e.g., brisk walking, cycling)
Add 2 sessions/week of resistance training
Enhances glucose uptake independent of insulin
Builds metabolically active lean muscle
Timeline: Improvements begin within 4–6 weeks
Nutrition
Follow a Mediterranean or low-glycaemic-index diet
Reduce ultra-processed foods and added sugars
Blunts post-meal insulin spikes
Lowers systemic inflammation and supports vascular repair
Timeline: Lipid changes in 6–8 weeks, insulin resistance improves in 3–6 months
Sleep
Target 7–9 hours of quality sleep nightly
Evaluate for sleep apnea if symptoms exist (snoring, fatigue)
Sleep deprivation can impair insulin signaling by 20–30%
Timeline: Benefits begin immediately with sleep correction
Stress Reduction
Practice mindfulness, yoga, or relaxation techniques (15–20 min/day)
Reduces chronic cortisol elevation, a driver of insulin resistance
Helps limit visceral fat accumulation
Timeline: Hormonal balance improves over 8–12 weeks
Screening & Monitoring
Request fasting insulin and calculate HOMA-IR
Consider Pulse Wave Velocity if vascular aging is suspected
Enables early detection before irreversible damage
Timeline: Actionable insights available immediately
Pharmacological Support (When Needed)
Discuss options like Metformin, GLP-1 receptor agonists, or SGLT-2 inhibitors
Improve mitochondrial efficiency and reduce oxidative stress
Proven cardiovascular outcome benefits in high-risk individuals
Timeline: Risk reduction over 1–3 years
The Exercise Prescription: Specifics Matter
🔹 Aerobic Training
30 minutes/day, 5 days/week
Activities: walking, cycling, swimming, jogging
Moderate intensity: able to speak, but not sing
Improves insulin sensitivity in liver and fat tissue
🔹 Resistance Training
2 sessions/week, 20–30 minutes each
Target major muscle groups: legs, back, chest, shoulders
Exercises: squats, push-ups, lunges (even bodyweight is effective)
Increases muscle mass—the primary site of glucose disposal
🔹 Movement Breaks
Break prolonged sitting every 30 minutes
Add 2–3 minutes of light movement (walking, stretching)
Reduces post-meal glucose spikes and chronic hyperinsulinemia
Especially beneficial even in those already meeting exercise targets
Key Takeaway
Consistency and specificity—not intensity alone—drive metabolic improvement. Small, structured changes applied daily can significantly reduce insulin resistance and slow cardiovascular aging
Frequently Asked Questions
1. Can insulin resistance be completely reversed, or only managed?
In many cases, insulin resistance can be significantly improved—and even reversed in early stages. The key determinant is timing and consistency of intervention. Structured exercise, weight reduction (especially visceral fat loss), and dietary modification can restore insulin sensitivity at the cellular level. However, in long-standing or advanced metabolic disease, it may be more realistic to control and mitigate rather than fully reverse. Early action offers the greatest chance of reversal.
2. My doctor says my blood sugar is normal. Can I still have insulin resistance?
Yes—this is extremely common. Blood glucose often remains normal for years because the pancreas compensates by producing more insulin. This state of hyperinsulinemia can silently damage blood vessels long before glucose rises. Measuring fasting insulin and calculating HOMA-IR helps detect this earlier phase.
3. What is arterial stiffness, and should I be concerned?
Arterial stiffness refers to the loss of elasticity in blood vessels, making them less able to expand and buffer blood flow. This increases cardiac workload and contributes to hypertension and heart disease. It can be assessed using Pulse Wave Velocity. Importantly, it often develops before symptoms, making it a valuable early marker of cardiovascular aging.
4. Are GLP-1 medications like semaglutide useful for people without diabetes?
Medications such as Semaglutide are increasingly used beyond diabetes, particularly in obesity and high cardiometabolic risk. They improve insulin sensitivity, promote weight loss, and have demonstrated cardiovascular benefits. However, their use should be individualized and medically supervised, as long-term data in non-diabetic populations is still evolving.
5. Does the type of fat matter—is belly fat more dangerous?
Yes. Visceral fat (abdominal fat) is metabolically active and strongly linked to insulin resistance, inflammation, and cardiovascular disease. Unlike subcutaneous fat, it releases inflammatory cytokines and free fatty acids directly into the portal circulation, worsening metabolic dysfunction. Reducing waist circumference is therefore a key therapeutic target.
6. How does poor sleep worsen insulin resistance and cardiovascular risk?
Sleep deprivation disrupts hormonal balance, increasing cortisol and impairing insulin signaling—reducing insulin sensitivity by up to 20–30% even after short-term sleep loss. Chronic sleep issues, including obstructive sleep apnea, further increase inflammation, blood pressure, and cardiovascular risk. Improving sleep quality is a rapid and effective metabolic intervention.
7. At what age should I start worrying about insulin resistance and cardiovascular aging?
Insulin resistance can begin as early as the third decade of life, particularly in individuals with sedentary lifestyles, poor diet, or genetic predisposition. Screening becomes especially relevant after age 30–35 in at-risk individuals.
Clinical insight: The earlier insulin resistance is identified, the greater the opportunity to prevent long-term vascular damage and preserve cardiovascular health.
Key Takeaway
Insulin resistance is common, often silent, and highly modifiable. Understanding these fundamentals empowers both patients and clinicians to intervene early—when the greatest benefit is still achievable.Your Heart Is Listening — Start the Conversation Today
Insulin resistance is largely silent. But it is not invisible — and it is not inevitable. The science is clear: early identification and targeted intervention can protect your cardiovascular health for decades. Take this article to your next appointment. Ask for HOMA-IR testing. Start the conversation your heart deserves.
Clinical Pearls on Insulin Resistance & Cardiovascular Aging
1. Screen Beyond Glucose: Fasting Insulin and HOMA-IR
The Pearl: Do not rely solely on normal Fasting Plasma Glucose (FPG) or HbA1c to rule out significant cardiovascular risk. Insulin resistance (IR) often precedes Type 2 Diabetes by years, and patients are at high cardiovascular risk during this hyperinsulinemic, normoglycemic phase (Fazio et al., 2024).
Actionable Insight: Routinely request Fasting Insulin (FI) and calculate the HOMA-IR (Homeostasis Model Assessment-Insulin Resistance) index. A HOMA-IR > 2.0 or FI > 12 mIU/mL is a strong signal for aggressive lifestyle intervention, even if HbA1c is normal.
2. IR Drives Arterial Stiffening (Vascular Aging)
The Pearl: View insulin resistance not just as a metabolic problem, but as a primary driver of accelerated vascular aging (Hill et al., 2021). IR promotes collagen deposition and reduces NO (nitric oxide) availability, causing arterial stiffening.
Actionable Insight: Increased Arterial Stiffness (e.g., measured via Pulse Wave Velocity) in a non-diabetic patient should immediately trigger a deep investigation for underlying insulin resistance, as this stiffening is an early and often irreversible consequence.
3. The Bidirectional Risk: Age Multiplies IR's Impact
The Pearl: The relationship between aging and IR is synergistic (Hao et al., 2025). Advanced age not only makes the body more insulin-resistant but also dramatically amplifies the atherosclerotic consequences of existing IR
Actionable Insight: Early, aggressive intervention (especially lifestyle) in younger and middle-aged patients with IR is critical. Preventing metabolic dysfunction from becoming entrenched saves more years of cardiovascular health than intervening late.
4. Biological Aging is the Mediator (The Core Mechanism)
The Pearl: Insulin resistance doesn't just raise risk—it directly accelerates biological aging (Li et al., 2024), which is what ultimately drives CVD mortality. The mechanism involves mitochondrial dysfunction, cellular senescence, and impaired autophagy.
Actionable Insight: Interventions like Metformin and GLP-1 agonists are effective because they don't just lower glucose; they improve mitochondrial function and reduce cellular stress, effectively acting as "anti-aging" interventions that lower CVD risk.
5. Exercise is the Most Potent Insulin Sensitizer
The Pearl: Of all non-pharmacological interventions, physical activity is arguably the fastest and most powerful tool to reverse insulin resistance. It enhances glucose uptake in muscles independently of insulin, improving peripheral sensitivity immediately.
Actionable Insight: Prescribe a specific exercise regimen—not just general advice. Recommend a combination of 150 minutes/week of moderate-intensity aerobic exercise plus 2 sessions/week of resistance training. Resistance training is essential as it builds muscle mass, the primary site of glucose disposal.
Author’s Note
This article was written to shift a critical misconception in modern medicine: that cardiometabolic risk begins when blood sugar rises. In reality, the pathological process often starts much earlier—with insulin resistance and compensatory hyperinsulinemia silently affecting vascular biology for years, if not decades, before conventional markers become abnormal.
As a clinician, I have repeatedly encountered patients with “normal” laboratory reports who nonetheless exhibit clear signs of metabolic dysfunction—central adiposity, elevated triglycerides, low HDL, or early hypertension. What is often missing in these evaluations is a deeper look at insulin dynamics, particularly through tools such as HOMA-IR. By the time fasting glucose or HbA1c rises, the underlying vascular and cellular changes are frequently already established.
The intent here is not to overmedicalize risk, but to identify a reversible window of opportunity. Insulin resistance represents one of the few upstream drivers of cardiovascular disease that can be meaningfully improved—often through non-pharmacological strategies such as structured exercise, nutritional refinement, sleep optimization, and stress modulation. When necessary, evidence-based pharmacological tools can further support this process.
Importantly, the science in this field is evolving. While emerging therapies show promise in modifying both metabolic and cardiovascular outcomes, they should complement—not replace—foundational lifestyle interventions.
For clinicians, this is a call to expand screening beyond glucose-centric models. For patients, it is reassurance that early detection offers leverage, not alarm.
The central message is simple but powerful: cardiovascular aging is not merely a consequence of time—it is, to a significant extent, a consequence of metabolic health, and it is modifiable
Last updated on 29th April 2026
Related Article
Your Cholesterol Isn’t the Whole Story: The Hormone Imbalances Driving Heart Disease
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Remnant Cholesterol: The Hidden Link Between Insulin Resistance, Type 2 Diabetes, and Heart Disease
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
Why Belly Fat Causes Insulin Resistance: Portal Theory Explained Simply
References
Fazio, S., Mercurio, V., Tibullo, L., Fazio, V., & Affuso, F. (2024). Insulin resistance/hyperinsulinemia: An important cardiovascular risk factor that has long been underestimated. Frontiers in Cardiovascular Medicine, 11, 1380506. https://doi.org/10.3389/fcvm.2024.1380506
Hao, X., Tu, S., Pan, D., Liao, W., Yang, L., Wang, S., & Sun, G. (2025). Relationship of ageing to insulin resistance and atherosclerosis. Metabolites, 15(9), 613. https://doi.org/10.3390/metabo15090613
Hill, M. A., Yang, Y., Zhang, L., Sun, Z., Jia, G., Parrish, A. R., & Sowers, J. R. (2021). Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism: Clinical and Experimental, 119, 154766. https://doi.org/10.1016/j.metabol.2021.154766
Li, X., Wang, J., Zhang, M., Li, X., Fan, Y., Zhou, X., Sun, Y., & Qiu, Z. (2024). Biological aging mediates the associations of metabolic score for insulin resistance with all-cause and cardiovascular disease mortality among US adults: A nationwide cohort study. Diabetes, Obesity & Metabolism, 26(9), 3552–3564. https://doi.org/10.1111/dom.15694
The Molecular and Metabolic landscape of Insulin Resistance in Aging-Related Cardiovascular Diseases. (2025). Aging and Disease. https://doi.org/10.14336/ad.2025.1108
Ye, C., Dou, C., Liu, D., et al. (2025). Multivariate genome-wide analyses of insulin resistance unravel novel loci and therapeutic targets for cardiometabolic health. Nature Communications, 16, 10057. https://doi.org/10.1038/s41467-025-64985-9
Caturano, A., Galiero, R., Vetrano, E., Sardu, C., Rinaldi, L., Russo, V., Monda, M., Marfella, R., & Sasso, F. C. (2024). Insulin–heart axis: Bridging physiology to insulin resistance. International Journal of Molecular Sciences, 25(15), 8369. https://doi.org/10.3390/ijms25158369
Lu, X., Liu, M., Song, Y., Lin, S., Zhou, X., Zeng, H., Li, A., Li, H., Xie, X., Lin, S., & Wu, S. (2025). Insulin resistance and its association with coronary heart disease: Insights from bioinformatics analysis. Frontiers in Endocrinology, 16, 1730801. https://doi.org/10.3389/fendo.2025.1730801
Tao, S., Yu, L., Li, J., et al. (2025). Insulin resistance quantified by estimated glucose disposal rate predicts cardiovascular disease incidence: A nationwide prospective cohort study. Cardiovascular Diabetology, 24, 161. https://doi.org/10.1186/s12933-025-02672-1