Sarcopenia and the Mobility Crisis: Why Muscle Loss Threatens Independence
Protect your "metabolic sink." Learn how reversing Sarcopenia prevents falls, fractures, and diabetes. A comprehensive guide to musculoskeletal health in 2025.
SARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/10/202616 min read
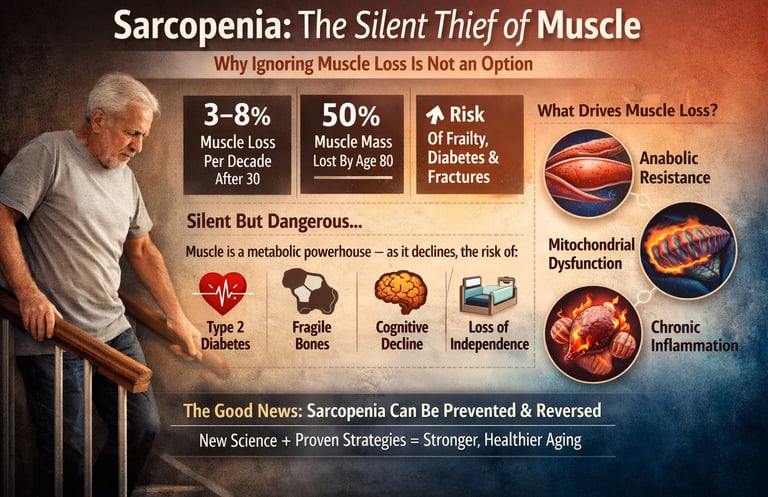
Sarcopenia is an age-related loss of muscle mass, strength, and function that increases the risk of falls, diabetes, and disability. It is driven by anabolic resistance, inflammation, and inactivity, but can be prevented and treated with resistance training, adequate protein intake, and early clinical screening.
10–16%Adults Over 60 Affected
3–8% Muscle Loss Per Decade After 30
50%Muscle Mass Lost by Age 80
40B+Annual Economic Burden (Global)
Sarcopenia rarely announces itself loudly. It begins quietly—subtle fatigue when climbing stairs, a slower walking pace, a growing reliance on handrails. What appears to be “normal aging” is, in many cases, a progressive and clinically significant loss of skeletal muscle mass, strength, and function. By the time it becomes obvious, substantial physiological decline has already occurred. Research suggests that adults can lose approximately 3–8% of muscle mass per decade after the age of 30, with acceleration after 60, ultimately contributing to frailty, metabolic dysfunction, and loss of independence (Tu et al., 2025; Liu et al., 2025).
This is not merely a musculoskeletal issue—it is a systemic metabolic disease. Skeletal muscle is the body’s largest glucose reservoir and a key regulator of insulin sensitivity, energy expenditure, and inflammatory balance. As muscle declines, the risk of type 2 diabetes, cardiovascular disease, falls, fractures, and mortality rises in parallel (Khan et al., 2025; Mao et al., 2025). At the cellular level, this process is driven by anabolic resistance, mitochondrial dysfunction, chronic low-grade inflammation, and dysregulation of critical growth pathways such as IGF-1/Akt/mTOR (Tu et al., 2025; Gao et al., 2025).
The critical shift in modern medicine is this: sarcopenia is no longer viewed as inevitable—it is diagnosable, preventable, and, to a meaningful extent, reversible. With advances in exercise science, nutrition, and emerging therapeutics, we now have the tools to intervene earlier and more effectively than ever before (Liu et al., 2025).
Evidence-Based Ways to Prevent and Reverse Sarcopenia
Perform resistance training 2–3 times per week
Progressive overload is the most effective strategy to build and preserve muscle.Increase protein intake to 1.2–1.6 g/kg/day
Focus on high-quality, leucine-rich protein sources.Distribute protein evenly across meals
Aim for 25–35 g per meal to maximize muscle protein synthesis.Correct vitamin D deficiency
Maintain serum 25(OH)D levels above 50 nmol/L.Consider creatine supplementation
Enhances strength and muscle mass when combined with exercise.Stay physically active daily
Avoid prolonged sedentary behavior to reduce muscle breakdown.Screen early using SARC-F or grip strength testing
Early detection enables timely intervention and better outcomes.
Clinical pearls
1. The "Anabolic Threshold" (Protein Distribution)
Scientific: In older adults, anabolic resistance necessitates a higher per-meal leucine threshold (approx. 3g) to trigger the $mTORC1$ pathway. A skewed protein distribution (e.g., 10g at breakfast, 70g at dinner) fails to optimize 24-hour muscle protein synthesis (MPS) compared to an even distribution.
Think of your muscle like a light switch that needs a certain amount of pressure to turn on. If you only eat a little protein at breakfast, you never "flip the switch." You need about 30g of high-quality protein at every meal to tell your body it’s time to build muscle.
2. The Muscle-Bone Crosstalk (Osteosarcopenia)
Scientific: Skeletal muscle is an endocrine organ that secretes myokines (like Irisin and IL-6), which directly modulate osteoblast activity. Mechanical loading through resistance training is not just a structural stressor but a biochemical signal that preserves bone mineral density (BMD).
Your muscles and bones are constantly "talking" to each other. When you strengthen a muscle, it sends a chemical signal to the nearby bone telling it to get stronger, too. You can’t truly fix "weak bones" without also addressing "weak muscles."
3. Power vs. Strength (The Type II Fiber Crisis)
Scientific: Age-related atrophy preferentially targets Type II (fast-twitch) glycolytic fibers over Type I (slow-twitch) oxidative fibers. This leads to a disproportionate loss of power (force x velocity) compared to maximal strength, which is the primary driver of fall-related injuries.
There is a difference between being "strong" and being "fast." Sarcopenia steals your "fast" muscles first—the ones that help you catch your balance if you trip. To stay safe, you don't just need to lift heavy things; you need to practice moving with a bit of "pep" and speed.
4. Myosteatosis: The "Marbling" Effect
Scientific: Myosteatosis—the infiltration of inter- and intramuscular adipose tissue—is a more potent predictor of metabolic dysfunction than low muscle mass alone. Fat within the muscle promotes local inflammation and impairs the contractile quality of the fibers.
It’s not just about how much muscle you have, but how "clean" that muscle is. Just like a steak can be "marbled" with fat, human muscle can store fat internally as we age. This "marbled" muscle is weaker and causes more inflammation in the body than lean, "solid" muscle.
5. The "Metabolic Sink" (Glycemic Control)
Scientific: Skeletal muscle is responsible for over 80% of postprandial glucose disposal. Sarcopenia reduces the primary "metabolic sink" for circulating glucose, directly contributing to insulin resistance and the progression of Type 2 Diabetes, regardless of total body fat percentage.
Your muscles are your body’s primary engine for burning sugar. When you lose muscle, you lose your biggest "storage tank" for the carbohydrates you eat. Keeping your muscles big and active is one of the best ways to keep your blood sugar naturally low.
The Molecular Machinery Behind Muscle Loss
To fight sarcopenia effectively, it helps to understand why muscles deteriorate in the first place. The science, while complex, tells a coherent story — and it begins at the cellular level.
Protein Turnover Imbalance
Healthy muscles exist in a state of constant renewal: proteins are built (muscle protein synthesis, or MPS) and broken down (muscle protein breakdown, or MPB) in a carefully balanced cycle. In sarcopenia, this equilibrium tips toward breakdown. Ageing impairs the sensitivity of muscle to anabolic triggers — particularly dietary protein and exercise — a phenomenon called anabolic resistance.
According to Tu et al. (2025), dysregulation of core signalling pathways — particularly the IGF-1/PI3K/Akt/mTOR axis (which promotes muscle growth) and the myostatin pathway (which suppresses it) — lies at the heart of sarcopenic muscle loss. When mTORC1 signalling weakens with age, cells lose their ability to ramp up protein synthesis in response to food and exercise, accelerating net muscle loss
Key Takeaway — Tu et al. (2025)
Sarcopenia is driven by multi-pathway molecular dysfunction — impaired IGF-1/mTOR signalling, elevated myostatin activity, mitochondrial dysfunction, and chronic inflammation ("inflammaging") all simultaneously accelerate muscle wasting. Effective treatment must target several of these mechanisms at once, not just one in isolation.
Mitochondrial Decline and Oxidative Stress
Mitochondria — the powerhouses of muscle cells — become increasingly dysfunctional with age. This leads to reduced energy production (ATP), impaired muscle contraction efficiency, and heightened production of reactive oxygen species (ROS). The resulting oxidative damage further accelerates protein breakdown and satellite cell (muscle stem cell) dysfunction (Tu et al., 2025).
Chronic Low-Grade Inflammation ("Inflammaging")
Elevated circulating levels of pro-inflammatory cytokines — particularly TNF-α, IL-6, and IL-1β — are a hallmark of ageing. These inflammatory signals directly suppress muscle protein synthesis and activate catabolic pathways, creating a biochemical environment hostile to muscle maintenance (Gao et al., 2025).
Sarcopenia and the Musculoskeletal System: A Two-Way Struggle
Sarcopenia does not occur in isolation — it is deeply intertwined with the entire musculoskeletal system. Bones, tendons, cartilage, and adipose tissue all interact with skeletal muscle through a complex web of biochemical signals.
Mao et al. (2025) provide a comprehensive mapping of these interactions, highlighting the emerging concept of osteosarcopenia — the co-occurrence of sarcopenia and osteoporosis, which dramatically elevates fracture risk and functional decline (Mao et al., 2025). Muscle and bone are not independent structures; they communicate through shared signalling molecules called myokines (released by muscle) and osteokines (released by bone). When muscle mass falls, the mechanical and biochemical stimulation that keeps bones strong also diminishes — setting off a destructive spiral.
Key Takeaway — Mao et al. (2025)
Sarcopenia is a systemic musculoskeletal disease, not merely a muscle problem. Muscle-bone crosstalk via myokines and osteokines means that preserving muscle mass simultaneously protects bone density, joint health, and metabolic function. Interventions targeting muscle health have ripple benefits across the entire musculoskeletal system.
Additionally, myosteatosis — the infiltration of fat into muscle tissue — is increasingly recognised as a driver of both sarcopenia and insulin resistance. Muscle fat infiltration impairs contractile function, reduces metabolic efficiency, and promotes further inflammation
Diagnosing Sarcopenia: When and How to Get Tested
One of sarcopenia's greatest challenges is that it is chronically underdiagnosed. Many people — and even some clinicians — mistake its early signs (fatigue, weakness, slower walking speed) for "normal ageing." They are not. They are warning signs that warrant formal assessment.
Who Should Be Screened Early?
Diabetes
CKD
Sedentary adults
Post-menopausal women
Current Diagnostic Criteria
The two major international frameworks — the European Working Group on Sarcopenia in Older People (EWGSOP2) and the Asian Working Group for Sarcopenia (AWGS 2019) — both use a three-component definition:
Key Components of Sarcopenia Diagnosis
Low Muscle Mass
What is measured: Skeletal Muscle Index (SMI)
Common tools: DEXA scan, Bioelectrical Impedance Analysis (BIA)
Low Muscle Strength
What is measured: Handgrip strength
Common tool: Handheld dynamometer
Poor Physical Performance
What is measured: Functional mobility (e.g., walking speed, chair stand ability)
Common tools:
Short Physical Performance Battery (SPPB)
Timed Up and Go (TUG) test
Liu et al. (2025) emphasise that screening should begin at age 60 in the general population and earlier (45–50) in those with metabolic conditions, physical inactivity, or malnutrition. Simple community-based tools like the SARC-F questionnaire can flag at-risk individuals without any specialist equipment.
Clinical Decision Framework
Step 1: Screen (SARC-F)
Step 2: Confirm (DEXA + grip strength)
Step 3: Stratify severity
Step 4: Intervention ladder
Traditional Interventions: The Evidence-Based Pillars
Resistance Training: The Gold Standard
If there is one intervention that consistently tops the evidence hierarchy for sarcopenia, it is progressive resistance training (PRT). This involves exercises — using body weight, machines, free weights, or resistance bands — that systematically challenge muscles to grow stronger over time.
Khan et al. (2025) provide a compelling clinical overview of resistance training's mechanisms: it directly activates mTORC1 signalling, stimulates satellite cell proliferation, enhances mitochondrial biogenesis, and improves insulin sensitivity. Crucially, resistance training also preserves muscle quality (contractile protein content and neuromuscular function), not just muscle mass
Key Takeaway — Khan et al. (2025)
Progressive resistance training is the single most effective intervention for sarcopenia prevention and treatment. Even older adults initiating PRT for the first time demonstrate significant gains in muscle mass, strength, and function. The minimum effective dose appears to be 2–3 sessions per week at moderate-to-high intensity, with progressive overload. The metabolic benefits extend well beyond muscle — improving glycaemic control, lipid profiles, and cardiovascular risk.
For patients unable to perform high-intensity exercise, blood flow restriction training (BFR) — applying cuffs to the limbs to restrict venous return during low-load exercise — has emerged as a powerful alternative, producing significant hypertrophy gains at much lower resistance loads (Liu et al., 2025).
Nutritional Strategies
Resistance training and nutrition are inseparable partners in sarcopenia management. The most evidence-supported nutritional strategies include:
Adequate protein intake: Current guidelines recommend 1.2–1.6 g of protein per kg of body weight per day for older adults — substantially higher than the 0.8 g/kg/day RDA designed to prevent deficiency, not optimise muscle health.
Leucine enrichment: This branched-chain amino acid is the primary trigger for mTORC1-mediated muscle protein synthesis. Foods rich in leucine include eggs, meat, fish, dairy, and soy.
Omega-3 fatty acids: EPA and DHA reduce inflammaging cytokines and may directly enhance anabolic signalling in muscle (Gao et al., 2025).
Vitamin D: Deficiency is highly prevalent in older adults and independently associated with muscle weakness. Supplementation at 800–2,000 IU/day is widely recommended in at-risk individuals.
Creatine monohydrate: A cost-effective supplement with robust evidence for enhancing the muscle-building effects of resistance training in older adults (Liu et al., 2025).
Key Takeaway — Liu et al. (2025)
Therapeutic advances in sarcopenia management highlight that no single intervention is sufficient. The most effective approach combines resistance training, optimised protein intake (with leucine emphasis), vitamin D, and creatine in a synergistic, patient-tailored protocol. Personalised medicine frameworks — accounting for genetics, gut microbiome, comorbidities, and lifestyle — are rapidly replacing one-size-fits-all guidelines.
Frontiers in Non-Drug Treatment: Beyond Pills and Protein
While resistance training and nutrition remain the backbone of sarcopenia management, a rapidly expanding toolkit of non-pharmacological interventions is opening new avenues for patients who cannot fully engage with conventional approaches.
Electrical Muscle Stimulation (EMS)
Neuromuscular electrical stimulation (NMES) — applying mild electrical currents to elicit muscle contractions — has shown promising results for frail elderly patients confined to beds or wheelchairs. Whole-body EMS suits are increasingly being studied for their ability to recruit large muscle groups simultaneously with minimal physical effort (Kuang et al., 2025).
Photobiomodulation and Vibration Therapy
Whole-body vibration (WBV) therapy involves standing on a vibrating platform, which stimulates reflex muscle contractions and has been shown to modestly improve lower limb strength and balance in older adults. Photobiomodulation (low-level laser therapy) may promote mitochondrial activity in muscle cells, though evidence remains in early stages (Kuang et al., 2025).
Traditional Mind-Body Practices
Tai Chi and yoga deserve special mention. Both combine resistance elements, balance training, and stress reduction, with Tai Chi in particular showing clinically meaningful improvements in fall risk, balance, and functional strength in sarcopenic patients. These practices also offer crucial psychosocial benefits, addressing the isolation and depression that often accompany physical decline in older adults (Kuang et al., 2025).
Key Takeaway — Kuang et al. (2025)
Non-drug treatments for sarcopenia are experiencing a renaissance. Whole-body EMS, vibration platforms, photobiomodulation, and mind-body practices offer clinically validated, accessible adjuncts to conventional exercise and nutrition — particularly valuable for frail, institutionalised, or mobility-limited patients. Combining these modalities with traditional resistance training produces superior outcomes to either approach alone.
Section 07Personalized Medicine: The Future of Sarcopenia Care
The most exciting frontier in sarcopenia management is the move toward truly individualised treatment — where interventions are tailored not just to age and diagnosis, but to an individual's genetic makeup, biomarker profile, gut microbiome composition, and even their specific pattern of molecular dysfunction.
Emerging Pharmacological Therapies
Several drug candidates are progressing through clinical trials (Gao et al., 2025; Liu et al., 2025):
Myostatin inhibitors (e.g., bimagrumab): Block the protein that suppresses muscle growth; early trials show significant lean mass gains.
Selective androgen receptor modulators (SARMs): Tissue-specific anabolic effects with potentially fewer side effects than testosterone.
GLP-1 receptor agonists: Beyond their diabetes and obesity applications, GLP-1 drugs may protect muscle mass during weight loss — a critical concern in the era of semaglutide.
Senolytic agents: Drugs that selectively clear senescent ("zombie") cells, which accumulate with age and release pro-inflammatory signals that drive muscle wasting.
The Gut-Muscle Axis
One of the most surprising recent discoveries is the intimate relationship between the gut microbiome and skeletal muscle health. Short-chain fatty acids produced by gut bacteria modulate inflammation, energy metabolism, and even satellite cell function. Dysbiosis (imbalanced gut flora) is now linked to accelerated sarcopenia, and probiotic/prebiotic interventions are being actively studied as adjunct therapies (Gao et al., 2025).
Key Takeaway — Gao et al. (2025)
The pathogenesis of sarcopenia is multifactorial and deeply interconnected with systemic biology. Emerging treatment strategies — including senolytics, myostatin blockade, gut microbiome modulation, and stem cell therapies — promise to dramatically expand our therapeutic arsenal. The next decade of sarcopenia care will be defined by precision medicine: matching the right intervention to the right patient at the right time.
An Editorial Perspective
Sarcopenia is not aging—it is pathology.
The long-held belief that muscle loss is an inevitable consequence of aging is now scientifically obsolete. Sarcopenia represents a progressive, diagnosable, and treatable disease state, with clear molecular drivers including anabolic resistance, mitochondrial dysfunction, and chronic inflammation (Tu et al., 2025; Gao et al., 2025).Skeletal muscle is a central metabolic organ—not just for movement.
Accounting for nearly 40% of body mass, muscle is the primary site of glucose disposal, insulin sensitivity, and metabolic regulation. Its decline directly accelerates type 2 diabetes, cardiovascular disease, and frailty syndromes (Khan et al., 2025).The muscle–bone–metabolism axis reframes chronic disease.
Emerging concepts like osteosarcopenia highlight that muscle loss drives bone fragility, while myosteatosis fuels insulin resistance—positioning sarcopenia as a systems-level disorder, not an isolated condition (Mao et al., 2025).Anabolic resistance is the clinical turning point.
Aging muscle becomes less responsive to protein and exercise stimuli, largely due to impaired IGF-1/Akt/mTOR signaling. This creates a “blunted anabolic environment,” requiring higher-quality protein and progressive resistance stimuli to overcome (Tu et al., 2025).Resistance training is not optional—it is therapeutic.
Progressive resistance training (PRT) remains the most potent intervention, capable of reversing key molecular deficits, restoring muscle mass, and improving metabolic health—even in advanced age (Khan et al., 2025).Nutrition must evolve beyond the RDA paradigm.
Protein recommendations for older adults must shift toward 1.2–1.6 g/kg/day, with emphasis on leucine-rich sources and strategic timing to optimize muscle protein synthesis (Liu et al., 2025).The future is precision muscle medicine.
Advances in myostatin inhibition, GLP-1 modulation, senolytics, and the gut–muscle axis are redefining therapeutic possibilities. The next decade will likely transform sarcopenia care into a personalized, biomarker-driven discipline (Gao et al., 2025).The clinical message is urgent and actionable.
Early screening, structured resistance training, and targeted nutrition can delay, halt, and even reverse sarcopenia—making muscle preservation one of the most powerful interventions in modern preventive medicine.
Practical Applications: What You Can Do Starting Today
Start Resistance Training
2–3 sessions per week of progressive resistance exercise is the most evidence-supported intervention available. Begin with bodyweight squats, wall push-ups, and chair stands if you are new to exercise. Gradually add resistance bands or light weights. Consult a physiotherapist for a personalised programme
Optimise Protein Intake
Aim for 25–35g of high-quality protein at each main meal — not all at dinner. Include leucine-rich foods: eggs, Greek yoghurt, cottage cheese, chicken, fish, or tofu. Consider whey protein supplementation post-exercise if dietary targets are hard to meet.
Check Your Vitamin D
Ask your doctor for a 25(OH)D blood test. Deficiency (below 50 nmol/L) is extremely common and strongly linked to muscle weakness. If deficient, supplementation of 1,000–2,000 IU/day alongside dietary sources can meaningfully improve muscle function within months.
Incorporate Mind-Body Movement
Tai Chi, yoga, and Pilates provide resistance, balance, and flexibility training in a low-impact format. Even 20 minutes, three times weekly, can meaningfully reduce fall risk and improve functional strength — particularly important for those with joint pain or mobility limitations.
Nourish Your Gut
Eat a fibre-rich, plant-diverse diet to support a healthy gut microbiome — and by extension, muscle health. Include fermented foods (yoghurt, kefir, kimchi) regularly. Minimise ultra-processed foods, which drive gut dysbiosis and systemic inflammation.
Request a Sarcopenia Screening
If you are over 60, or have risk factors (low activity, chronic illness, poor nutrition), ask your GP or geriatrician for a formal assessment. Simple tools like the SARC-F questionnaire and handgrip dynamometry are widely available and can identify risk before significant decline occurs.
Frequently Asked Questions About Sarcopenia
1. At what age does sarcopenia typically begin, and is it inevitable?
Muscle mass begins declining as early as age 30, at a rate of approximately 3–8% per decade. The rate accelerates significantly after age 60–65. However, sarcopenia is absolutely not inevitable — it is a modifiable condition. Regular resistance exercise, adequate protein intake, and active lifestyle maintenance can substantially slow, halt, and even partially reverse muscle loss at any age. Think of muscle mass like a savings account: the earlier you invest, the more you have to draw on later (Tu et al., 2025; Liu et al., 2025).
2. Can I still build muscle in my 70s or 80s?
Yes — and the research is unequivocal on this point. While older adults experience anabolic resistance (reduced response to exercise and protein), they are by no means incapable of building muscle. Numerous clinical trials have demonstrated meaningful hypertrophy and strength gains in adults in their 70s, 80s, and even 90s in response to progressive resistance training. The key is consistency, progressive overload, and adequate protein intake (particularly leucine-rich protein) around exercise sessions (Khan et al., 2025).
3. How is sarcopenia different from just "feeling weak" or normal ageing?
Sarcopenia is a clinically diagnosable condition with specific measurable thresholds for muscle mass, strength, and physical performance. The diagnosis requires objective assessment — typically a DEXA scan or bioelectrical impedance analysis (BIA) for muscle mass, plus handgrip dynamometry and functional tests (e.g., gait speed, chair stand test). Normal age-related changes exist on a continuum, but sarcopenia represents a pathological acceleration of that decline that significantly raises the risk of falls, fractures, disability, and mortality (Tu et al., 2025).
4. Does sarcopenia affect only the elderly?
While sarcopenia predominantly affects older adults, it can occur at any age in the context of chronic disease, prolonged bed rest, malnutrition, or sedentary lifestyle. Secondary sarcopenia — driven by conditions such as cancer, HIV, chronic kidney disease, or heart failure — can affect people in their 30s and 40s. Physical inactivity is perhaps the greatest accelerant: even young people who are highly sedentary show accelerated muscle loss compared to their active peers (Gao et al., 2025).
5. What are the early warning signs I should watch for?
Early sarcopenia often manifests subtly. Warning signs include: difficulty rising from a chair without using arms, reduced walking speed (taking longer to cross a room or street), declining grip strength, unexpected fatigue during daily activities, increased difficulty with stairs, frequent falls or near-falls, unintentional weight loss, and general feelings of physical weakness. The validated SARC-F questionnaire — which takes under two minutes — can be a useful first self-screening tool before consulting a doctor (Liu et al., 2025; Tu et al., 2025).
6. Are there medications or supplements specifically approved for sarcopenia?
Currently, no drug is specifically licensed for sarcopenia in most countries. Testosterone and anabolic steroids have evidence for muscle gain but carry significant side effect profiles. Vitamin D supplementation is widely recommended for deficient individuals. Creatine monohydrate has robust evidence as a safe, inexpensive supplement that enhances the effects of resistance training. Several promising agents — including myostatin inhibitors (e.g., bimagrumab), SARMs, and senolytics — are progressing through clinical trials and may reach clinical practice within this decade (Liu et al., 2025; Gao et al., 2025).
7. How does sarcopenia interact with conditions like diabetes or osteoporosis?
The interactions are profound and bidirectional. Sarcopenia worsens insulin resistance (since skeletal muscle is the body's primary site of glucose disposal), accelerating type 2 diabetes progression. Conversely, diabetes-associated inflammation and poor glycaemic control accelerate muscle wasting. With osteoporosis, muscle and bone loss co-occur through shared hormonal and mechanical pathways — a dangerous combination termed "osteosarcopenia" — which dramatically elevates fracture risk. Treating sarcopenia thus has cascading benefits for multiple comorbidities simultaneously (Mao et al., 2025; Khan et al., 2025).
Author’s Note (Clinician Perspective)
As a physician working at the intersection of internal medicine, metabolism, and exercise science, I have increasingly come to view sarcopenia not as an isolated geriatric concern, but as a central driver of cardiometabolic disease and functional decline across the lifespan. What makes sarcopenia particularly dangerous is its invisibility in early stages—patients often present only after significant muscle loss has already occurred.
This article was written to bridge a critical gap: translating rapidly evolving molecular and clinical research into practical, actionable strategies that both clinicians and patients can implement. The emerging evidence is clear—skeletal muscle is medicine. It is not merely structural tissue, but a dynamic endocrine and metabolic organ that influences insulin sensitivity, inflammation, and longevity.
The most important clinical shift is this: we now have the tools to intervene early and effectively. Resistance training, optimized protein intake, and targeted lifestyle strategies are not adjuncts—they are foundational therapies. Future advances in pharmacology and precision medicine will expand our options, but the cornerstone of sarcopenia management will remain rooted in lifestyle as first-line treatment.
My goal is simple: to reframe muscle health as a primary clinical priority, not an afterthought—because preserving muscle is, in many ways, preserving independence, metabolic health, and quality of life
Take Control of Your Muscle Health Today
Sarcopenia is preventable. It is treatable. And the best time to act is now — whether you are 40 or 80. Share this guide with someone who needs it, bookmark it for reference, or take our quick sarcopenia self-assessment.
Disclaimer: This article is for educational purposes only and does not constitute medical advice.
Always consult a qualified healthcare professional before making changes to your exercise, diet, or medication regimen.
Related Articles
Sarcopenic Obesity: How to Lose Fat Safely Without Losing Muscle | DR T S DIDWAL
Why We Age: The Hidden Role of Chronic Inflammation in Accelerating Aging | DR T S DIDWAL
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
References
Gao, Y., Liu, D., Xiao, Q., Huang, S., Li, L., Xie, B., … Liu, Y. (2025). Exploration of pathogenesis and cutting-edge treatment strategies of sarcopenia: A narrative review. Clinical Interventions in Aging, 20, 659–684. https://doi.org/10.2147/CIA.S517833
Khan, M. S., Yadav, A., & Sharma, R. (2025). Role of resistance training in metabolic health and chronic disease prevention: A clinical perspective. Experimental Gerontology, 188, 112345. https://doi.org/10.1016/j.exger.2025.112345
Kuang, Q.-F., Ni, Y.-Q., & Liu, Y.-S. (2025). Frontiers in nondrug treatment of sarcopenia: A review of pathological mechanisms and the latest treatment strategies. Aging Medicine, 8, 200–209. https://doi.org/10.1002/agm2.70011
Liu, X., Chen, X., & Cui, J. (2025). Therapeutic advances in sarcopenia management: From traditional interventions to personalized medicine. Clinical Nutrition, 51, 187–197. https://doi.org/10.1016/j.clnu.2025.06.007
Mao, X., Lv, K., Qi, W., et al. (2025). Research progress on sarcopenia in the musculoskeletal system. Bone Research, 13, 78. https://doi.org/10.1038/s41413-025-00455-8
Tu, S., Hao, X., Xu, S., Jin, X., Liao, W., Xia, H., Wang, S., & Sun, G. (2025). Sarcopenia: Current insights into molecular mechanisms, diagnostics, and emerging interventional approaches. International Journal of Molecular Sciences, 26(14), 6740. https://doi.org/10.3390/ijms26146740