Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained
Uncover the major sarcopenia risk factors—from inactivity and chronic disease (diabetes, CKD) to malnutrition. See the full list of high-risk patients and how to intervene early.
SARCOPENIA
DR T S DIDWAL MD
5/27/202617 min read
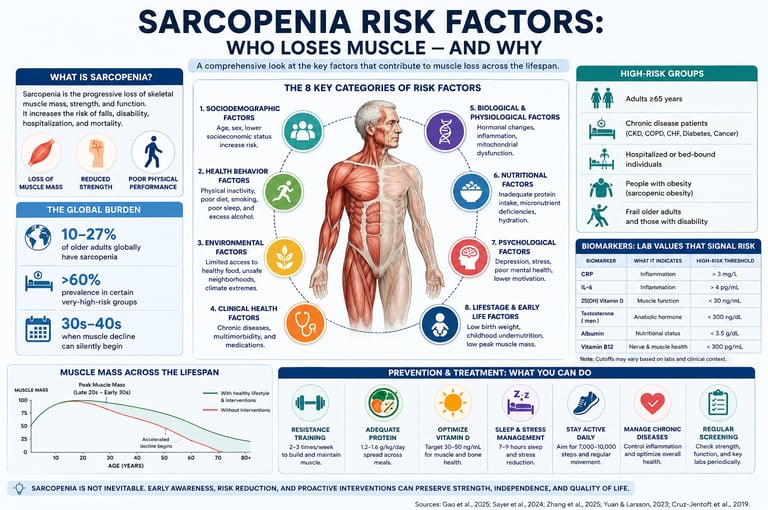
Sarcopenia risk factors include physical inactivity (the most modifiable), inadequate protein intake (<1.2 g/kg/day), chronic diseases (diabetes, CKD, heart failure, cancer), aging after 60, low vitamin D, smoking, and sarcopenic obesity. Muscle loss often begins silently in the 30s–40s, with peak muscle mass in young adulthood determining later-life risk (Gao et al., 2025).
Key Risk Categories:
Lifestyle: Inactivity, poor protein intake, smoking, poor sleep
Medical: Chronic inflammation, anabolic resistance from diabetes/CKD
Other: Low BMI, social isolation, low socioeconomic status
Best Prevention: Progressive resistance training 2–3×/week + 1.2–1.6 g/kg protein daily can prevent and reverse sarcopenia even in adults over 80.
Key Takeaways
1. Sarcopenia is a Life-Course Condition
Muscle loss begins subtly in the 30s–40s, well before clinical manifestation in later decades. Peak muscle mass attained in young adulthood serves as the primary determinant of sarcopenic risk in old age (Gao et al., 2025). Early identification and intervention during midlife offer the greatest window for prevention.
2. Physical Inactivity is the Most Modifiable Driver
Sedentary behavior represents the single strongest modifiable risk factor for sarcopenia. Progressive resistance training performed 2–3 times per week is the most effective intervention for preserving and restoring muscle mass, strength, and function across all age groups, including frail older adults (Sayer et al., 2024).
3. Chronic Diseases Accelerate Muscle Wasting Through Shared Pathways
Conditions such as type 2 diabetes, chronic kidney disease, heart failure, and cancer promote sarcopenia via chronic inflammation (↑IL-6, TNF-α), anabolic resistance, oxidative stress, and mitochondrial dysfunction. Optimal disease management is therefore essential for mitigating disease-associated muscle loss.
4. Adequate Protein Intake and Distribution Matter
Protein requirements increase with age and chronic illness (1.2–1.6 g/kg/day recommended). Evenly distributing high-quality protein (≥25–30 g per meal) maximizes muscle protein synthesis by overcoming anabolic resistance, significantly outperforming bolus intake patterns.
5. Multimodal Assessment Improves Risk Stratification
Beyond age and BMI, clinicians should evaluate grip strength, chair stand performance, inflammatory markers (CRP, IL-6), nutritional indices (albumin, prealbumin), and vitamin D status. Sarcopenic obesity — high fat mass with low muscle mass — carries particularly high metabolic and functional risk and is frequently overlooked.
6. Sarcopenia Remains Reversible with Targeted Intervention
Even in advanced age (80+ years), progressive resistance training combined with optimized protein nutrition, vitamin D repletion, and chronic disease control can produce clinically meaningful gains in muscle mass and strength. Early action yields substantially better outcomes than late-stage treatment.
Sarcopenia rarely begins with a dramatic event. More often, it starts silently — a little less strength climbing stairs, slower recovery after illness, difficulty carrying groceries, or feeling unusually fatigued after routine activity.
By the time noticeable weakness appears, substantial muscle loss may already have occurred. Modern research now shows that sarcopenia is not simply an unavoidable consequence of aging, but a complex and potentially preventable muscle disease influenced by lifestyle, chronic illness, inflammation, nutrition, hormones, and even early-life health exposures (Gao et al., 2025; Sayer et al., 2024).
In fact, measurable declines in muscle mass and strength can begin as early as the fourth decade of life, especially in physically inactive individuals. The consequences extend far beyond appearance or mobility. Sarcopenia is strongly associated with frailty, falls, insulin resistance, hospitalization, disability, cardiovascular disease, and premature mortality (Yuan & Larsson, 2023).
Emerging evidence also links muscle health to immune function, cognitive resilience, and healthy longevity. According to recent international consensus guidelines, muscle strength is now considered one of the most important biomarkers of healthy aging (Sayer et al., 2024).
Understanding who is at risk — and why — is therefore essential not only for preserving mobility, but for protecting long-term metabolic and overall health.You might think muscle loss is simply what happens when you get old — an inevitable, unstoppable slide. But that picture is incomplete.
Sarcopenia, the progressive loss of skeletal muscle mass, strength, and function, can begin silently in your 30s or 40s, and by the time symptoms become obvious, years of preventable decline may already have occurred.
What Exactly Is Sarcopenia?
Sarcopenia is formally defined as the progressive, generalized loss of skeletal muscle mass accompanied by reduced muscle strength and/or physical performance. It is not simply "getting thin" — it reflects a fundamental breakdown in the body's ability to maintain and regenerate muscle tissue.
Two major international bodies define and diagnose it somewhat differently:
EWGSOP2 (European Working Group on Sarcopenia in Older People): Diagnoses sarcopenia primarily based on low muscle strength (e.g., low grip strength or chair stand performance), with reduced muscle quantity and quality providing confirmation (Sayer et al., 2024).
AWGS (Asian Working Group for Sarcopenia): Uses age-related muscle mass loss combined with either low muscle strength or poor physical performance, with slightly different cutoff values tuned for Asian populations.
Clinical Pearl — Strength, Not Mass
According to EWGSOP2, low muscle strength is a more reliable predictor of disability and mortality than low muscle mass alone. This is why grip strength testing and the 5-times chair stand test are central to modern diagnostic algorithms (Sayer et al., 2024).
Sarcopenia exists on a spectrum: it can be presarcopenic (low mass only), sarcopenic (low mass plus low strength or function), or severe sarcopenia (all three deficits present). The earlier it is caught on this spectrum, the more reversible it is.
Why Understanding Risk Factors Changes Everything
Here is the critical insight that most people miss: peak muscle mass, reached in your late 20s to early 30s, is your single biggest determinant of how much muscle you will have in old age. A person who builds a high peak and declines at an average rate will still have adequate muscle at 75. A person who starts low — due to poor nutrition, inactivity, or illness — may cross into sarcopenia territory decades earlier.
A 2025 meta-analysis of longitudinal studies (Gao et al., 2025) confirmed that sarcopenia is truly a life-course condition. Interventions at any age matter, but the window of greatest impact is in midlife, before the accelerating decline of the 60s begins.
The Eight Key Categories of Sarcopenia Risk Factors
Based on the latest systematic reviews (Zhang et al., 2025; Gao et al., 2025), risk factors cluster into eight well-defined domains. Understanding which category applies to you helps prioritize which interventions will have the greatest impact.
1. Sociodemographic Factors
These are largely fixed, but awareness allows earlier intervention:
Age: The strongest single predictor. Risk rises steeply after 60, though the biological foundation for decline was laid decades earlier.
Sex: Men typically show greater absolute muscle loss (due to higher baseline mass), but women experience an accelerated phase around menopause driven by estrogen withdrawal and associated reductions in physical activity.
Socioeconomic status: Lower socioeconomic status reduces access to nutritious food, gym facilities, healthcare, and safe outdoor spaces — all of which protect muscle health.
2. Health Behavior Factors (Most Modifiable)
This is where your effort has the most direct impact.
Physical Inactivity
The single most modifiable risk. Muscle tissue that goes unstimulated — especially through resistance loading — atrophies rapidly (Sayer et al., 2024).
Inadequate Protein Intake
Muscles require amino acids from dietary protein for ongoing repair and synthesis. Insufficient intake accelerates net protein catabolism.
Smoking
Accelerates muscle loss through systemic inflammation, oxidative stress, and impaired satellite cell (muscle stem cell) function.
Sleep Dysregulation
Both too little (<7 hrs) and too much (>9 hrs) sleep are associated with greater sarcopenia risk — disrupting growth hormone release and inflammatory balance.
3. Health Condition Factors
Chronic diseases do not simply coexist with sarcopenia — they actively drive it through overlapping biological pathways including chronic low-grade inflammation, anabolic resistance, and reduced physical capacity (Sayer et al., 2024).
Type 2 diabetes: A particularly powerful driver. Insulin resistance impairs muscle protein synthesis, while chronic hyperglycemia damages motor neurons and promotes oxidative muscle stress.
Chronic kidney disease (CKD): Uremic toxins directly suppress muscle protein synthesis, and dialysis patients face extraordinarily high sarcopenia rates — exceeding 60% in some studies (Yuan & Larsson, 2023).
Heart failure: Reduced cardiac output limits oxygen and nutrient delivery to muscles; systemic inflammation and immobility compound the effect.
Cancer (especially GI cancers): Triggers profound cachexia — a severe inflammatory wasting syndrome that accelerates sarcopenia far beyond normal aging rates.
Cognitive impairment and dementia: Creates a bidirectional feedback loop: cognitive decline reduces purposeful activity and dietary awareness, which worsens muscle health, which in turn may worsen cognition.
Depression: Reduces motivation, activity, and often appetite — all of which erode muscle health.
4. Anthropometric Factors
Low BMI (<18.5): Associated with approximately four times the risk of sarcopenia compared to normal BMI. Underweight individuals often lack the nutritional reserves to maintain muscle mass (Gao et al., 2025).
Sarcopenic obesity: Counterintuitively, people with a high BMI can also develop sarcopenia. Excess fat tissue produces inflammatory cytokines that degrade muscle — a particularly dangerous combination for metabolic health and disability risk.
Small calf circumference: A simple, low-tech proxy for reduced lower-extremity muscle mass. Values below 31 cm in older adults have been associated with sarcopenia risk across multiple populations.
Don't Assume a Healthy Weight Means Healthy Muscles
A "normal" BMI does not rule out sarcopenia. Body composition analysis — not weight alone — is necessary to identify low muscle mass, particularly in people with a normal or high BMI who are physically inactive.
5. Biomarker Factors
Laboratory values can reveal subclinical muscle wasting and inflammatory drivers before clinical symptoms appear (see full table in Section 5).
6. Early Life Factors
Muscle health is a life-course issue (Gao et al., 2025). Birth weight is a proxy for intrauterine nutrition and growth. Low birth weight is associated with impaired muscle fiber development and a lower peak muscle mass ceiling in adulthood. Poor childhood growth — from malnutrition, recurrent illness, or developmental disadvantage — compounds this effect. The lower your peak muscle mass in young adulthood, the less reserve you have against age-related decline.
7. Psychosocial Factors
Social isolation, loneliness, and chronic life stress reduce self-care motivation, activity levels, and dietary quality. Longitudinal data suggests that older adults with strong social connections maintain significantly better physical function — partly through more consistent physical activity and better dietary habits (Zhang et al., 2025).
8. Living Environment Factors
Access matters. People in "food deserts" (neighbourhoods lacking fresh, affordable food) struggle to meet protein and micronutrient needs. Those without safe walking routes, parks, or affordable gym access face structural barriers to physical activity. Nursing home and hospital environments dramatically restrict movement, creating rapid, environment-driven muscle loss.
High-Risk Groups: A Structured Screening Framework
Not everyone faces equal risk. The following framework — synthesized from Zhang et al. (2025) and Yuan & Larsson (2023) — helps clinicians and individuals prioritize screening and early intervention.
Very High Risk Group (Adults 80+; patients with cancer, CKD on dialysis, multimorbidity, or nursing home residents):
Driving Factors: Severe anabolic resistance, chronic inflammation, immobility, and high catabolism.
Recommended Action: Conduct an immediate nutritional and exercise assessment; consider a specialist referral.
High Risk Group (Adults 65–79 who are physically inactive; individuals with diabetes, heart failure, dementia, or depression):
Driving Factors: Disease-driven muscle wasting, low anabolic hormone levels, and reduced physical activity.
Recommended Action: Implement grip strength screening, review dietary protein, and initiate a structured resistance training program.
High Lifestyle Risk Group (Current smokers; adults underweight with a BMI less than 18.5; heavy alcohol users):
Driving Factors: High oxidative stress, chronic nutritional deficits, and an elevated inflammatory burden.
Recommended Action: Prioritize smoking cessation, nutritional rehabilitation, and targeted resistance training.
Moderate Risk Group (Adults 60–64 with a sedentary lifestyle; chronic inflammatory conditions; post-surgical or hospitalized patients):
Driving Factors: Inactivity-driven muscle atrophy and the catabolic stress of surgery or acute illness.
Recommended Action: Ensure early mobilisation post-hospitalisation, optimize dietary protein intake, and provide activity counseling.
Moderate-Low Risk Group (Adults 50–59 with a poor diet and sedentary lifestyle; individuals with poor sleep quality):
Driving Factors: Early-stage anabolic resistance and subclinical low-grade inflammation.
Recommended Action: Provide lifestyle counseling, promote increased physical activity, and conduct a baseline dietary protein assessment.
Biomarkers: Lab Values That Signal Sarcopenia Risk
A targeted panel of blood and urine markers can detect subclinical sarcopenia risk well before a patient loses measurable muscle mass. These are especially useful for monitoring high-risk inpatient and outpatient populations.
Serum Albumin:
Indicates: Baseline nutritional and systemic protein status.
Risk Signal: Values less than 3.5 g/dL
Clinical Significance: Reflects visceral protein insufficiency and hepatic synthetic capacity; strongly associated with poor skeletal muscle outcomes.
Prealbumin (Transthyretin):
Indicates: Short-term, acute nutritional status.
Risk Signal: Values less than 15 mg/dL
Clinical Significance: Serves as a much earlier indicator of protein malnutrition than albumin due to its shorter half-life; highly useful for tracking response to acute nutritional interventions.
CRP (C-Reactive Protein):
Indicates: Systemic, low-grade inflammatory burden.
Risk Signal: Values greater than 5 mg/L (or elevated high-sensitivity hs-CRP).
Clinical Significance: Chronic elevations accelerate muscle protein breakdown via NF\kappa-driven systemic inflammatory pathways.
IL-6 (Interleukin-6):
Indicates: Pro-inflammatory cytokine activity.
Risk Signal: Elevated above standard laboratory reference ranges.
Clinical Significance: Directly activates the ubiquitin-proteasome pathway to degrade myofibrillar proteins; chronic elevation impairs muscle-specific satellite cell function and regeneration.
Serum Creatinine:
Indicates: Indirect muscle mass proxy (when kidney function is stable).
Risk Signal: Low values relative to demographics.
Clinical Significance: Derived from creatine phosphate breakdown in skeletal muscle; unexpectedly low levels often reflect reduced baseline muscle mass rather than superior clearance or improved renal function.
25-OH Vitamin D:
Indicates: Systemic Vitamin D status.
Risk Signal: Values less than 20 ng/mL
Clinical Significance: Targets Vitamin D receptors located directly on skeletal muscle cells; deficiency impairs type II muscle fiber synthesis, strength, and structural function.
Testosterone / IGF-1:
Indicates: Core systemic anabolic hormone signaling.
Risk Signal: Values dropping below age-adjusted clinical reference ranges.
Clinical Significance: Both hormones serve as primary up-regulators of muscle protein synthesis; their physiological decline accelerates sarcopenia—particularly post-menopause and in hypogonadal men.
How Chronic Disease , Muscle Loss: The Shared Mechanisms
It is not coincidence that diabetes, CKD, heart failure, and cancer all appear on the high-risk sarcopenia list. They share a set of converging biological pathways that assault muscle tissue from multiple directions simultaneously.
Chronic Low-Grade Inflammation ("Inflammaging")
Aging itself produces a low-level inflammatory state, often called "inflammaging." Chronic diseases pour accelerant on this fire. Elevated TNF-α and IL-6 activate the ubiquitin-proteasome pathway, the cellular machinery that degrades muscle proteins, and simultaneously suppress satellite cells — the stem cells responsible for muscle repair. According to a 2025 landmark review (Mao et al., 2025), disruption of these pathways is now considered central to sarcopenia pathogenesis.
Anabolic Resistance
In healthy young muscle, dietary protein triggers a robust spike in muscle protein synthesis via the mTORC1 signaling pathway. In chronic disease — and in aging alone — this anabolic response is blunted. More protein is needed to achieve the same stimulatory effect. This is why protein recommendations for older adults and those with chronic illness are set higher than for younger, healthy individuals.
Mitochondrial Dysfunction
Muscle is among the most metabolically active tissue in the body. When mitochondria — the energy-generating organelles within muscle cells — become dysfunctional (a hallmark of diabetes, CKD, and heart failure), ATP production falls, oxidative stress rises, and the energetic cost of maintaining muscle becomes unsustainable. The result is accelerated fiber atrophy and a shift toward weaker, slower muscle fiber types (Nguyen et al., 2026).
Prevention & Treatment: A Practical Protocol
The research consensus is unambiguous: sarcopenia is not inevitable, and it is largely reversible with targeted lifestyle intervention — even in very old age (Sayer et al., 2024). The following evidence-based protocol integrates the best available 2025 data.
Evidence-Based Sarcopenia Prevention Checklist
Resistance Training 2–3×/week: Progressive overload is the #1 intervention. Compound movements (squats, rows, presses) that load multiple large muscle groups simultaneously are most efficient. Even chair-based exercises produce meaningful benefit in frail older adults.
Protein intake 1.0–1.2 g/kg/day (minimum): Many experts recommend 1.2–1.6 g/kg/day for those with active disease or in rehabilitation. Distribute protein across meals (≥25–30 g per meal) to maximize muscle protein synthesis per feeding.
Optimize Vitamin D: Target serum 25-OH vitamin D levels of 30–50 ng/mL. Supplement if deficient; combined with resistance training, vitamin D supplementation improves muscle strength outcomes.
Manage chronic conditions aggressively: Optimized diabetes control (HbA1c targets), heart failure management, and CKD nutrition protocols all slow the disease-driven component of sarcopenia.
Prioritize sleep quality: Aim for 7–8 hours per night. Growth hormone — released primarily during deep sleep — is a key driver of overnight muscle protein synthesis.
Quit smoking: Even in older adults, smoking cessation significantly reduces systemic inflammation within weeks, removing a chronic muscle-wasting stimulus.
Address social isolation: Group exercise classes, walking programs, and community-based nutrition support all deliver muscle health benefits partly by creating accountability and improving dietary quality.
Request targeted screening if high-risk: Ask your doctor about grip strength testing, the 5-times chair stand test, or a DEXA scan for body composition if you fall into a high-risk group.
Key Evidence: Resistance Training in Old Age
A comprehensive 2024 Nature Reviews Disease Primers analysis (Sayer et al., 2024) confirms that progressive resistance training produces significant gains in muscle mass, strength, and physical performance in adults over 65 — including those in their 80s and 90s. It is never too late to start.
Protein Timing and Distribution
The distribution of protein intake matters as much as the total. Eating the majority of daily protein in a single meal (e.g., a large dinner) is significantly less effective at stimulating muscle protein synthesis than spreading it across three or four meals. Aim for at least 25–30 g of high-quality protein at breakfast and lunch, not just at dinner.
What About Supplements?
Creatine monohydrate (3–5 g/day) has the most consistent evidence base for augmenting resistance training benefits in older adults. Leucine-enriched essential amino acid supplements can help those unable to meet protein targets through diet alone. Omega-3 fatty acids show early promise for reducing anabolic resistance, though large-scale trial data remains limited. Always discuss supplementation with your healthcare provider.
Common Myths & Mistakes About Sarcopenia Risk
❌ Myth: Sarcopenia only happens to very old people."
✅ Reality: Muscle mass peaks in the late 20s. Measurable decline begins in the 30s–40s and accelerates around 60. Waiting until old age to address muscle health misses the most impactful prevention window (Gao et al., 2025).
❌ Myth: "If I'm not visibly thin or weak, I don't have sarcopenia."
✅ Reality Sarcopenic obesity — normal or high BMI with low muscle mass — is increasingly common and often missed without body composition testing. Muscle quality (fat infiltration) can be poor even when size appears normal.
❌ Myth: Cardio exercise is enough to protect muscles."
✅ Reality Aerobic exercise has cardiovascular benefits, but provides a much weaker stimulus for muscle mass preservation than resistance training. Walking alone will not stop sarcopenia. Progressive strength training is essential (Sayer et al., 2024).
❌ Myth: "High protein is dangerous for the kidneys."
✅ Reality: In individuals with normal kidney function, intakes of 1.2–1.6 g/kg/day are safe and beneficial. Protein restriction is only warranted in established CKD — and even then, current evidence suggests adequate protein may still be important if closely monitored by a nephrologist.
❌ Myth: "Sarcopenia is irreversible once diagnosed."
✅ Reality Numerous clinical trials demonstrate significant muscle mass and strength recovery with targeted resistance training and protein optimization — even in adults over 80. Reversibility is real, though the magnitude of gain decreases with advancing age and disease burden.
Frequently Asked Questions
Can young or middle-aged adults develop sarcopenia?
Yes. While the diagnosis is most common in adults over 65, sarcopenia can begin in the 30s — particularly in those who are sedentary, chronically ill, malnourished, or have a history of low birth weight or poor childhood nutrition. The process is gradual and often invisible until a critical threshold is crossed.
Why do some people lose muscle faster than others with age?
Rate of loss is determined by genetics (baseline muscle fiber type, hormone sensitivity), hormonal milieu (testosterone, estrogen, IGF-1 levels), dietary quality, physical activity habits, presence of chronic diseases, sleep quality, and cumulative lifetime exposure to inflammatory stressors. Lifestyle and metabolic health explain the majority of individual variation.
Is sarcopenia more common in men or women?
Men typically show a greater absolute decline due to their higher baseline muscle mass. However, women experience an accelerated phase of loss around menopause linked to estrogen withdrawal. Post-menopausal women who are physically inactive face particularly rapid progression. In very old age (80+), rates converge between sexes.
How is sarcopenia different from frailty?
Frailty is a broader geriatric syndrome defined by weakness, weight loss, exhaustion, low activity, and slow gait speed — it reflects a general loss of physiological reserve across multiple systems. Sarcopenia specifically refers to loss of skeletal muscle mass and strength. They overlap substantially, but not every sarcopenic person is frail, and frailty can occur without sarcopenia.
Do overweight or obese individuals get sarcopenia?
Yes — this is called sarcopenic obesity. Excess adipose tissue produces pro-inflammatory cytokines (TNF-α, IL-6) that accelerate muscle catabolism. Despite normal or elevated body weight, muscle mass and function can be critically low. Sarcopenic obesity carries particularly high risks for metabolic disease, disability, and poor surgical outcomes.
What is the single most important thing I can do to prevent sarcopenia?
Engage in progressive resistance training 2–3 times per week. This is the most robustly evidenced intervention across all ages. Combined with adequate protein intake (≥1.0–1.2 g/kg/day), this protocol halts and partially reverses sarcopenia — even in those who are already diagnosed.
What lab tests help identify sarcopenia risk early?
Key markers include serum albumin (nutritional reserve), prealbumin (short-term protein status), CRP and IL-6 (inflammatory burden), 25-OH vitamin D, and sex hormone levels (testosterone or estradiol). Low serum creatinine may also reflect reduced muscle mass. These can flag high-risk individuals before functional decline becomes apparent.
How is sarcopenia diagnosed in practice?
Clinical diagnosis typically involves a grip strength dynamometer test and/or 5-times chair stand test to assess muscle strength, combined with body composition analysis (DEXA or BIA) to quantify muscle mass, and gait speed or Short Physical Performance Battery (SPPB) to assess function. The EWGSOP2 algorithm (confirmed sarcopenia = low strength + low mass) is the most widely used diagnostic framework.
Are there medications approved for sarcopenia?
As of 2025, no pharmacological therapy is approved specifically for sarcopenia. Research on myostatin inhibitors, selective androgen receptor modulators (SARMs), and activin receptor blockers is ongoing, but none have yet cleared regulatory approval for this indication. Resistance training with adequate protein remains the gold-standard treatment (Tu et al., 2025).
How quickly can sarcopenia develop during hospitalization?
Muscle loss during acute illness and hospitalization can be dramatic. Studies document losses of 1–2 kg of lean mass in just 5–10 days of bed rest in older adults — driven by immobility, reduced protein intake, and acute-phase inflammatory responses. Early mobilization and nutritional support during hospitalization are therefore clinical priorities.
Conclusion: The Muscle Health Investment Mindset
Sarcopenia is not an inevitable tax on aging — it is a modifiable, largely preventable condition whose trajectory is shaped by choices made across an entire lifetime. The evidence from 2025 and beyond is clear: your risk is determined by at least eight intersecting categories of factors, from the household you were born into, to what you eat today, to whether you have a chronic disease being optimally managed.
The single most empowering takeaway from this body of research is the centrality of resistance training. No pill, powder, or procedure matches its muscle-preserving power. Combined with adequate protein, optimized chronic disease management, and attention to sleep and smoking, it forms a protocol capable of reversing functional muscle loss at any age.
✅ Your 5-Step Action Plan
1. Assess your risk tier using the table above.
2. Start or upgrade resistance training — 2–3 sessions/week of compound exercises.
3. Audit your protein intake — target ≥1.0 g/kg/day, distributed across meals.
4. Ask your doctor to check vitamin D, albumin, and inflammatory markers if you are in a high-risk group.
5. Manage chronic conditions aggressively — diabetes, CKD, and heart failure are muscle health problems, not just metabolic ones.
This information is for educational purposes only and should not replace professional medical advice. Always consult with your healthcare provider for personalized recommendations based on your individual health status and risk factors.
Related Articles
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | Dr T.S. DIDWAL
Prevent Sarcopenia & Osteoporosis: Your Guide to Strong Bones & Muscles | DR T S DIDWAL
How Sarcopenia Is Diagnosed: Tests, Criteria, and Early Warning Signs Explained | DR T S DIDWAL
References
Chen, L. K., Woo, J., Assantachai, P., Arai, H., Chou, M. Y., Chang, C. I., Chen, L. Y., Huang, S. T., Liew, N. Y., Lim, J. P., Lim, W. S., Peng, L. N., Tai, B. C., Tong, C. S., Wang, T., Won, C. W., Wu, C. H., Wu, I. C., Yeo, W. Y., ... Akishita, M. (2020). Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. Journal of the American Medical Directors Association, 21(3), 300–307. https://doi.org/10.1016/j.jamda.2019.12.012
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., Cooper, C., Rolland, Y., Sayer, A. A., Schneider, S. M., Sieber, C. C., Topinkova, E., Vandewoude, M., Visser, M., Zamboni, M., & Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2). (2019). Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Deutz, N. E., Bauer, J. M., Barazzoni, R., Biolo, G., Boirie, Y., Bosy-Westphal, A., Cederholm, T., Cruz-Jentoft, A. J., Krznariç, Z., Nair, K. S., Singer, P., Teta, D., Tipton, K., & Calder, P. C. (2014). Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clinical Nutrition, 33(6), 929–936. https://doi.org/10.1016/j.clnu.2014.04.007
Gao, Y., Huang, Y., An, R., Yang, Y., Chen, X., & Wan, Q. (2025). Risk factors for sarcopenia in community setting across the life course: A systematic review and meta-analysis of longitudinal studies. Archives of Gerontology and Geriatrics, 133, Article 105807. https://doi.org/10.1016/j.archger.2025.105807
Mao, X., Lv, K., Qi, W., Chang, Z., Wang, S., Zhou, Z., Zhao, Y., & Gao, Y. (2025). Research progress on sarcopenia in the musculoskeletal system. Bone Research, 13(1), Article 78. https://doi.org/10.1038/s41413-025-00455-8
Nguyen, T. T., Dao, T., Nguyen, H. T., Le, P. H., Tran, K. D., & Kim, S. W. (2026). Sarcopenia and muscle aging: Updated insights into molecular mechanisms and translational therapeutics. Endocrinology and Metabolism, 41(1), 57–85. https://doi.org/10.3803/EnM.2025.2656
Sayer, A. A., Cooper, R., Arai, H., Avendaño, M., Beard, J. R., Cawthon, P. M., Clegg, A., Fielding, R. A., Gutiérrez-Robledo, L. M., Landi, F., Lane, N. E., Martin, F. C., Reginster, J. Y., Rodriguez-Mañas, L., Rolland, Y., Shardell, M., Studenski, S. A., Visser, M., von Haehling, S., ... Cesari, M. (2024). Sarcopenia. Nature Reviews Disease Primers, 10(1), Article 68. https://doi.org/10.1038/s41572-024-00550-w
Tu, S., Hao, X., Xu, S., Jin, X., Liao, W., Xia, H., Wang, S., & Sun, G. (2025). Sarcopenia: Current insights into molecular mechanisms, diagnostics, and emerging interventional approaches. International Journal of Molecular Sciences, 26(14), 6740. https://doi.org/10.3390/ijms26146740
Yuan, S., & Larsson, S. C. (2023). Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism: Clinical and Experimental, 144, Article 155533. https://doi.org/10.1016/j.metabol.2023.155533
Zhang, S., Yang, X., An, N., Lv, M., Yang, L., Liu, R., Hu, S., Chen, W., Feng, W., & Mao, Y. (2025). Risk factors and predictive models for sarcopenia in older adults. Aging Medicine, 8(3), 192–199. https://doi.org/10.1002/agm2.70012