How Sarcopenia Is Diagnosed: Tests, Criteria, and Early Warning Signs Explained
Diagnose sarcopenia using strength, muscle mass, and performance tests such as grip dynamometry, DXA, and gait speed. Learn early warning signs, diagnostic criteria, and how early detection can help reverse age-related muscle loss
SARCOPENIA
6/25/202619 min read
Sarcopenia is the age-related loss of muscle strength, mass, and function, diagnosed under ICD-10-CM M62.84. Modern frameworks like EWGSOP2 and AWGS 2025 diagnose it using grip strength or chair stand tests plus muscle mass measured by DXA. Strength loss often occurs before muscle loss. SARC-F questionnaires screen for risk, but objective testing is required for diagnosis.
Key points
1. Sarcopenia now has multiple competing diagnostic frameworks
EWGSOP2, AWGS 2019/2025, GLIS, SDOC, and FNIH all define sarcopenia differently. Using SDOC vs EWGSOP2 can change low grip strength prevalence from 20.7% to 3.5% in the same patients. Ask your clinician which guideline they used.
2. Strength loss comes before muscle loss
Declining muscle strength, called dynapenia, typically shows up before measurable muscle mass loss. That's why a grip strength test can catch sarcopenia early, before major physical decline.
3. Strength is the primary diagnostic gateway in modern guidelines
Most frameworks test muscle strength first. Common grip strength cutoffs: EWGSOP2 <27 kg men/<16 kg women, AWGS <28 kg men/<18 kg women, SDOC <35.5 kg men. A chair stand >15 seconds also indicates weakness.
4. AWGS 2025 made a major shift: performance is no longer diagnostic
Under the new 2025 Asian and GLIS frameworks, diagnosis = low muscle mass AND low strength only. Gait speed and SPPB are now outcome measures to track severity, not criteria to confirm sarcopenia. "Severe sarcopenia" was removed.
5. DXA is the clinical gold standard for muscle mass, but it has limits
DXA estimates appendicular skeletal muscle mass and is fast and reproducible. But it measures lean mass, not just muscle, so it tends to overestimate true muscle compared to MRI. BIA, ultrasound, CT, and D3-creatine are alternatives.
6. SARC-F screens risk but doesn't diagnose
The 5-question SARC-F flags probable sarcopenia at ≥4 points. SARC-CalF adds calf circumference for better sensitivity. These tools favor specificity, so a negative score in high-risk people isn't fully reassuring. Objective strength/mass testing is needed to confirm.
7. Population-specific cutoffs matter
Asian adults, especially women, have lower absolute muscle mass at similar strength levels. AWGS uses different cutoffs than European EWGSOP2. Using the wrong reference range can misclassify you.
8. Sarcopenia is a diagnosable, billable condition with real consequences
ICD-10-CM code M62.84 makes it an official disease. It’s linked to 29-51% higher mortality risk, 1.62x odds of recurrent falls, and higher rates of fractures, malnutrition, and depression. But it’s also one of the more reversible age-related conditions with progressive resistance training and ≥1.2 g/kg/day protein.
You used to carry both grocery bags up the stairs without thinking about it. Now you find yourself setting one down halfway up, or gripping the railing a little tighter than you remember needing to. Maybe a jar lid that used to twist off easily now needs your spouse's help. Maybe your doctor mentioned, almost in passing, that you seem to be "losing muscle."
If any of that sounds familiar, you are not imagining it, and you are not just "getting older" in some vague, untreatable way. You may be looking at the early signs of sarcopenia — the progressive, age-related loss of skeletal muscle mass, strength, and physical function that the World Health Organization now recognizes with its own diagnostic code (ICD-10-CM M62.84).
Here is what makes sarcopenia diagnosis genuinely confusing, even for clinicians: there isn't one universal test with one universal cutoff. Depending on which guideline a clinic uses, you could be told you have sarcopenia — or told you don't — based on the exact same grip strength reading. In one comparative study of older inpatients, the European criteria flagged 10.2% of patients as having low grip strength, while the American SDOC criteria flagged 19.4% of the same patients. That's not a rounding error. That's a fundamentally different diagnostic philosophy, and it matters enormously for how you interpret your own results.
What is Sarcopenia,
Exactly not simply a symptom of aging — defined by declining muscle strength, declining muscle mass or quality, and, in more advanced stages, declining physical performance.¹
The term comes from the Greek sarx (flesh) and penia (loss) — literally, "poverty of flesh." It was first proposed as a research concept in 1989 and has since evolved into a formally diagnosable, billable medical condition.²
Three things are worth understanding before you look at any test result:
Strength loss (dynapenia) usually shows up before mass loss. A person can lose meaningful grip or leg strength well before a scan shows reduced muscle tissue, which is exactly why most modern guidelines test strength first.³
Muscle quality matters as much as muscle quantity. Two people can have identical muscle mass on a scan and very different strength, because fat infiltration, fibrosis, and neuromuscular changes affect how well that muscle actually functions.⁴
Sarcopenia is not exclusive to old age. It can begin in your 40s and 50s, particularly with sedentary behavior, chronic disease, or hormonal change — which is part of why the newest 2025 Asian guidelines extended screening down to age 50.⁵
Why Diagnosis Is More Complicated Than It Sounds
This is the part most articles skip, and it's the part that actually determines whether your results mean anything useful.
Unlike, say, diagnosing diabetes (where fasting glucose cutoffs are globally standardized), sarcopenia has at least five competing diagnostic frameworks, each built from different population data, different statistical methods, and different clinical priorities:
Framework Year Origin Core Philosophy EWGSOP2 2019 Europe Strength-first; mass confirms AWGS 2025 2025 Asia-Pacific Mass + strength concurrently; performance is an outcome, not a diagnostic criterion GLIS 2024–2025 Global consortium Adds muscle-specific strength (strength relative to mass) SDOC 2020 United States (FNIH-funded) Strength + gait speed only; explicitly excludes DXA mass as a criterion FNIH 2014 United States Early evidence-based cutoffs from pooled cohort data
Why does this matter to you? Because a 2023 head-to-head comparison study found that switching from EWGSOP2 to SDOC cutoffs on the same patients changed the proportion classified as having low grip strength from 3.5% to 20.7%.⁶ That is roughly a six-fold difference in diagnosed prevalence, purely from which ruler you use to measure the same stick.
This isn't a flaw you need to fear — it's a feature you need to understand. Each framework was built to answer a slightly different clinical question (Who is at risk of disability? Who needs intervention now? Who fits a research trial?). Your interpretation of "do I have sarcopenia" should always include "according to which criteria, and why those criteria were chosen for me."
Clinical pearl: If two clinics give you different verdicts from similar numbers, that's not necessarily a contradiction — it's likely because they applied different consensus cutoffs. Ask which guideline was used.
Who Should Be Screened
Talk to your doctor about sarcopenia screening if any of the following apply to you:
You are 60 or older (or 50+, under the newer Asian midlife criteria)
You've had unintentional weight loss in the past 6–12 months
You feel noticeably weaker than you did a year or two ago
You struggle to climb a flight of stairs or rise from a low chair without using your arms
You've fallen more than once in the past year
You live with a chronic condition such as type 2 diabetes, chronic kidney disease, heart failure, COPD, or a chronic inflammatory disease
Your activity level has dropped significantly (illness, injury, retirement, bed rest)
You've had a recent hospitalization, especially one involving bed rest
If two or more of these apply, screening typically takes less than 10 minutes and can be done at a routine appointment.
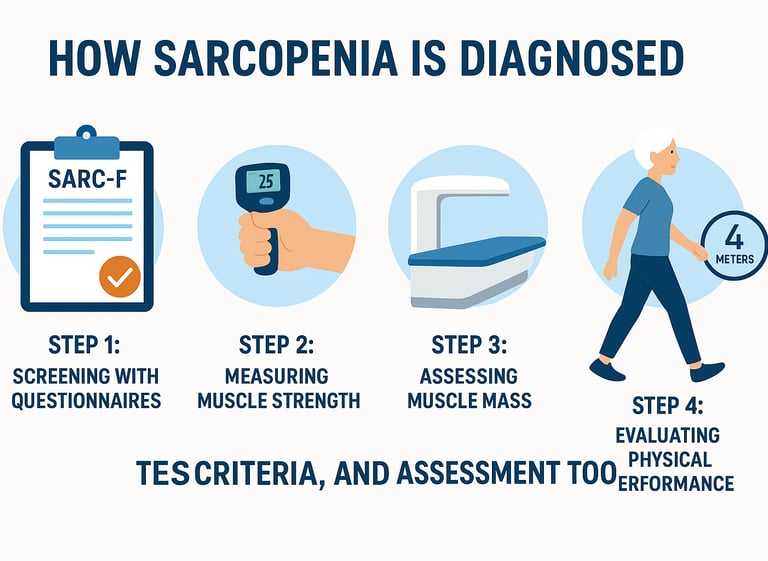
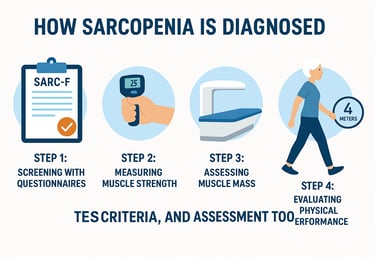
Step 1: Screening Questionnaires
Before any equipment comes out, most clinical pathways start with a quick questionnaire.
SARC-F is a five-item self-report tool covering:
Strength (difficulty lifting/carrying 10 lbs)
Assistance walking across a room
Rising from a chair
Climbing a flight of stairs
Falls in the past year
Each item scores 0–2, for a maximum of 10. A total score of 4 or higher suggests probable sarcopenia and warrants further testing.⁷
SARC-CalF adds a sixth component: calf circumference, measured around the widest part of the calf. Adding this measurement meaningfully improves sensitivity, particularly in people whose strength loss hasn't yet produced obvious symptoms.⁸
Important interpretive note: SARC-F is intentionally built to favor specificity over sensitivity — meaning it misses some true cases (especially early, "pre-sarcopenic" presentations) rather than over-flagging healthy people. A negative SARC-F score in someone with strong risk factors (e.g., recent hospitalization, unintentional weight loss) should not be treated as fully reassuring. Questionnaires screen for risk; they do not diagnose anything on their own.
Step 2: Measuring Muscle Strength
This is where objective measurement begins, and under nearly every current framework, strength is now the primary diagnostic gateway.
Grip Strength (Handgrip Dynamometry)
You squeeze a calibrated handheld dynamometer as hard as you can, typically three times per hand, with the highest reading recorded.
Why grip strength, of all things? It's not really about your hands. Grip strength correlates strongly with whole-body strength and has been validated across dozens of large cohort studies as a predictor of falls, hospitalization, disability, and mortality — making it one of the most extensively validated single measurements in all of geriatric medicine.⁹
Common cutoffs
EWGSOP2 (2019) (European Working Group on Sarcopenia in Older People)
Men: Less than 27 kg
Women: Less than 16 kg
AWGS 2019 (Asian Working Group for Sarcopenia)
Men: Less than 28 kg
Women: Less than 18 kg
AWGS 2025 (Asian Working Group for Sarcopenia - Updated)
Men: Less than 28 kg (for individuals aged 65 years or older)
Women: Less than 18 kg (for individuals aged 65 years or older)
SDOC (Sarcopenia Definition and Outcomes Consortium)
Men: Less than 35.5 kg
Women: Varies (frequently adjusted based on Body Mass Index)
FNIH (Foundation for the National Institutes of Health)
Men: Less than 26 kg
Women: Less than 16 kg
What affects validity: Dynamometer brand and calibration, hand position, whether the test is seated or standing, prior stroke or arthritis in the hand, and even time of day can all shift readings by several kilograms. If your result sits close to a cutoff, ask whether the measurement was repeated and which device was used — borderline values deserve a retest, not an automatic label.
Chair Stand Test (Five-Times Sit-to-Stand)
You stand up from a chair without using your arms, five times in a row, as quickly as you safely can.
Cutoff: Taking longer than 15 seconds (some frameworks use 12 seconds) suggests significant lower-body weakness.¹⁰
This test is cheap, requires no equipment beyond a chair and stopwatch, and correlates well with quadriceps strength — but it's also influenced by knee osteoarthritis, balance confidence, and footwear, which can make a strong person look "slow" for reasons unrelated to muscle.
Step 3: Measuring Muscle Mass
If strength testing is abnormal, the next step under most (though not all — see SDOC below) frameworks is measuring how much muscle tissue you actually have.
DXA (Dual-Energy X-ray Absorptiometry)
DXA is widely described as the clinical gold standard for estimating appendicular skeletal muscle mass (the muscle in your arms and legs), because it's fast, low-radiation, and reproducible across most clinical settings.¹¹
But "gold standard" doesn't mean "perfect," and this matters for interpretation. DXA doesn't directly measure muscle — it estimates "lean mass" by subtracting fat and bone mineral content from total body mass. Comparative research against MRI has shown that DXA tends to overestimate true muscle mass, especially in older adults, because lean mass includes non-contractile tissue like connective tissue and water content that DXA can't separate out from actual muscle fiber.¹² This is a genuine limitation, not a nitpick — it's part of why researchers are actively developing alternatives.
Common Appendicular Skeletal Muscle Mass (ASM) Cutoffs: Quick Clinical Summary
EWGSOP2 (2019) uses a height-adjusted ASM index (ASM/height²).
Men: < 7.0 kg/m²
Women: < 5.5 kg/m²
AWGS 2019 also uses a height-adjusted ASM index (ASM/height²).
Men: < 7.0 kg/m²
Women: < 5.7 kg/m²
DXA-specific cutoff for women: < 5.4 kg/m²
AWGS 2025 retains ASM/height² but officially incorporates ASM/BMI as an alternative measure to better account for body size and adiposity.
Uses population-specific thresholds.
Provides separate reference values for:
Middle-aged adults (50–64 years)
Older adults (≥65 years)
Muscle Mass Assessment Tools: Key Points
DXA (Dual-Energy X-ray Absorptiometry)
Widely used reference method for measuring ASM.
Relatively accurate, but may overestimate true muscle mass.
BIA (Bioelectrical Impedance Analysis)
Portable, inexpensive, and widely available.
Results are highly influenced by hydration status, recent exercise, and fluid balance.
Best used with standardized testing conditions.
Ultrasound
Radiation-free and increasingly accessible.
Measures both muscle quantity and muscle quality (echo intensity).
Useful for detecting fatty infiltration and muscle deterioration.
CT and MRI
Considered the most accurate imaging methods for muscle assessment.
Provide detailed evaluation of muscle size and quality.
Limited by cost, availability, and radiation exposure (CT).
D3-Creatine (D3-Cr) Dilution
Emerging technique for estimating total-body muscle mass without imaging.
Shows strong associations with falls, fractures, disability, and mortality.
Currently used mainly in research but may play a larger role in future sarcopenia guidelines.
Clinical Pearl
Muscle strength and physical performance remain the most clinically meaningful indicators of sarcopenia. Muscle mass measurements help confirm diagnosis, but muscle function often predicts disability, falls, hospitalization, and mortality more accurately than muscle quantity alone.Step
4: Assessing Physical Performance
This is the step where the diagnostic frameworks diverge most sharply from each other — and where the 2025 update matters most.
Gait Speed
Walked over a measured 4-meter distance at your normal pace.
Cutoff: Speed slower than 0.8 m/s has traditionally indicated severe sarcopenia under EWGSOP2.¹⁷
Short Physical Performance Battery (SPPB)
A composite score (0–12) combining balance testing, a timed walk, and the chair stand test — widely used in geriatric research as a broader marker of functional reserve.
The Big 2025 Shift: Performance as Outcome, Not Diagnosis
Here is the single most important update for anyone reading older sarcopenia articles in 2026: the newly updated AWGS 2025 consensus, aligning with the GLIS framework, has removed physical performance from the diagnostic criteria entirely.¹⁸
Under the new model:
Diagnosis = concurrent low muscle mass AND low muscle strength. That's it. Two criteria, not three.
Physical performance (gait speed, chair stand, SPPB) is reclassified as an outcome measure — something you track to gauge severity, monitor treatment response, and guide intervention intensity, but not something used to confirm or rule out the diagnosis itself.
The reasoning is conceptual, not just statistical: functional decline is now understood as a downstream consequence of muscle mass and strength loss, not a separate, parallel diagnostic pillar. Measuring it as a third "vote" risked diagnosing people too late, after function had already deteriorated — missing the optimal window for intervention.¹⁹
The category of "severe sarcopenia" (previously defined by adding poor performance to confirmed sarcopenia) has also been removed under AWGS 2025 and GLIS, replaced with a continued "possible sarcopenia" category for resource-limited settings to flag people for early intervention before formal confirmation.²⁰
What this means practically: If you were diagnosed (or ruled out) under the old three-pillar EWGSOP2/AWGS 2019 system, and you get retested under AWGS 2025, your classification could change — not because your muscles changed, but because the diagnostic architecture changed underneath you. This is a real, current source of confusion in clinics transitioning between guideline versions in 2025–2026, and it's worth specifically asking your provider which version they're using.
Major Sarcopenia Diagnostic Frameworks: Quick Clinical Summary
EWGSOP2 (2019, Europe)
Uses a strength-first approach.
Low muscle strength suggests sarcopenia, which is then confirmed with low muscle mass.
Physical performance is used to grade severity.
Most widely adopted framework in Europe.
AWGS 2019 (Asia)
Diagnosis requires assessment of muscle mass, strength, and physical performance.
Uses Asian-specific cutoffs reflecting regional body composition differences.
AWGS 2025 (Updated)
Assesses muscle mass and strength concurrently.
Introduces ASM/BMI as an alternative to ASM/height².
Removes the "severe sarcopenia" category.
Expands screening to adults aged 50–64 years.
GLIS (2024–2025, Global)
First internationally harmonized sarcopenia definition.
Incorporates strength, muscle mass, and muscle-specific strength (strength ÷ muscle mass).
Aims to unify regional diagnostic approaches.
SDOC (2020, United States)
Focuses exclusively on grip strength and gait speed.
Does not require muscle mass measurement.
Based on evidence suggesting DXA-measured lean mass adds little predictive value once strength and walking speed are known.
FNIH (2014, United States)
Combines muscle strength and muscle mass assessment.
Provided many of the foundational cutoffs used in later guidelines.
Key Clinical Insight
There remains significant debate about whether low muscle mass is essential for diagnosis.
European and Asian guidelines generally require muscle mass assessment.
The SDOC framework argues that weakness and slow walking speed are stronger predictors of adverse outcomes than muscle mass alone.
How to Interpret Results
No Sarcopenia: Normal strength and muscle mass.
Possible/Probable Sarcopenia: Low strength only; often the earliest and most treatable stage.
Confirmed Sarcopenia: Low strength plus low muscle mass.
Severe Sarcopenia: Confirmed sarcopenia with poor physical performance (EWGSOP2 and AWGS 2019 only)
.
Mistakes and Myths
Myth 1: "A bathroom body-fat scale can diagnose sarcopenia." Consumer BIA scales estimate whole-body composition, not appendicular skeletal muscle specifically, and are far more hydration-sensitive than clinical-grade BIA. They can be a useful trend-tracking tool, not a diagnostic instrument.
Myth 2: "If my muscle mass scan is normal, I don't have sarcopenia." Under EWGSOP2's strength-first model, you can have "probable sarcopenia" from low strength alone, even with normal-looking mass — and under the newer functional-sarcopenia concept introduced by the Korean Working Group in 2023, people with low strength and poor performance but normal mass are increasingly recognized as a distinct risk group.³⁸ Mass alone is not the full picture in either direction.
Myth 3: "Sarcopenia only happens to frail, very elderly people." It can begin in midlife, which is precisely why AWGS 2025 extended validated cutoffs down to ages 50–64.³⁹
Myth 4: "One slow walking test means I have severe sarcopenia." Under the newest AWGS 2025/GLIS framework, gait speed is no longer a diagnostic criterion at all — it's an outcome/severity measure. A single slow walk should prompt further strength and mass testing, not an automatic severe diagnosis.
Myth 5: "All grip strength cutoffs are basically the same number." As shown above, they range from roughly 26–35.5 kg for men depending on the framework — not a trivial difference.
Myth 6: "DXA is flawless because it's the gold standard." "Gold standard" in this context means "most widely validated and clinically practical," not "without measurement error." DXA's tendency to overestimate true muscle mass relative to MRI and D3-Cr is well documented and is actively driving research into alternatives.
What Happens After Diagnosis
A sarcopenia diagnosis is not a life sentence — it's increasingly described in the literature as one of the more reversible age-related conditions, provided action is taken.
Exercise Interventions
Progressive resistance training is the single most evidence-backed intervention for building muscle mass and strength in older adults, with meta-analyses consistently showing meaningful gains in both strength and lean mass even in adults over 80.⁴⁰ A basic, sustainable starting structure:
2–3 sessions per week
Major muscle groups (legs, back, chest, core)
Progressive overload — gradually increasing resistance as strength improves
Supervised initially if you're new to resistance training or have balance concerns
Nutritional Support
Protein intake of at least 1.2 g/kg body weight per day is the most consistently cited target in current guidelines for adults at risk of or diagnosed with sarcopenia.⁴¹
Distributing protein across meals (roughly 25–30g per meal) appears to support muscle protein synthesis more effectively than concentrating it in one meal.
Vitamin D sufficiency is also commonly assessed, given its role in muscle function.
Medical Management
Optimizing underlying chronic conditions (diabetes, heart failure, CKD, COPD) that accelerate muscle loss
Medication review for drugs that can worsen muscle wasting or balance
As of 2026, there remains no FDA-approved pharmacological treatment specifically for sarcopenia, though several agents (myostatin inhibitors, SARMs, and others) are in active clinical trials.⁴²
Safety note: Starting a new resistance training program after a sarcopenia diagnosis — especially if you have cardiovascular disease, recent fractures, or significant balance impairment — should be done under guidance from a physical therapist or physician-supervised program, at least initially.
Frequently Asked Questions
1. How is sarcopenia diagnosed in a doctor's office? Most pathways start with a SARC-F questionnaire, followed by an objective grip strength or chair stand test. If those suggest weakness, your provider assesses muscle mass (via DXA, BIA, or sometimes ultrasound) and may layer on a gait speed or SPPB assessment, depending on which guideline framework they follow.
2. What is considered a low grip strength for sarcopenia? Under EWGSOP2 (2019), a grip strength below 27 kg in men and below 16 kg in women suggests probable sarcopenia. Other frameworks, including AWGS and SDOC, use different cutoffs (up to 28 kg for men and 35.5 kg under SDOC's broader definition), so the "low" threshold genuinely depends on which guideline is applied.
3. Can blood tests diagnose sarcopenia? Not directly. There is no single blood biomarker currently validated for clinical diagnosis, though research is actively exploring myokines like IL-6, irisin, myostatin, and IGF-1 as future diagnostic or monitoring tools.⁴³ Blood work is more often used to rule out contributing causes (thyroid disease, vitamin D deficiency, inflammatory markers) than to diagnose sarcopenia itself.
4. Is a DXA scan necessary to diagnose sarcopenia? Under EWGSOP2, AWGS, and GLIS, yes — a mass measurement (DXA, BIA, or imaging) is required to move from "probable" to "confirmed" sarcopenia. Under the SDOC framework, no — SDOC deliberately built its definition around grip strength and gait speed alone, having found DXA lean mass didn't independently add predictive value in their analysis.
5. What's the difference between sarcopenia and frailty? They overlap heavily but aren't identical. Sarcopenia specifically refers to muscle mass, strength, and (in older frameworks) performance loss. Frailty is a broader clinical syndrome incorporating weight loss, exhaustion, slowness, weakness, and low activity across multiple body systems — sarcopenia is often described as a key physical contributor to frailty, not a synonym for it.
6. Can sarcopenia be diagnosed before age 60? Yes. The newly updated AWGS 2025 consensus introduced validated diagnostic cutoffs specifically for adults aged 50–64, reflecting evidence that muscle health decline can begin meaningfully earlier than previously assumed, particularly in people with chronic disease or sedentary lifestyles.
7. How accurate is the SARC-F questionnaire on its own? SARC-F is a useful, quick screening tool but is intentionally weighted toward specificity over sensitivity, meaning it can miss earlier or subtler cases. It should prompt further objective testing when positive, and a negative score in a high-risk individual shouldn't be treated as fully reassuring on its own.
8. Why did gait speed get removed from the diagnostic criteria? Under the 2025 AWGS update and the aligned GLIS framework, physical performance (gait speed, chair stands, SPPB) is now classified as an outcome measure rather than a diagnostic one. The reasoning is that functional decline is increasingly understood as a downstream consequence of muscle mass and strength loss rather than an independent diagnostic pillar — and waiting for functional decline to appear risked missing the earlier window for effective intervention.
9. Can I have normal muscle mass but still have sarcopenia? Possibly, under emerging "functional sarcopenia" definitions, such as the one introduced by the 2023 Korean Working Group on Sarcopenia, which describes people with low strength and poor performance despite normal-appearing muscle mass.⁴⁴ This remains a regionally specific, evolving concept rather than a universally adopted diagnostic category.
10. Are home grip strength devices reliable for self-screening? Consumer dynamometers can give you a useful trend over time if you're consistent with technique (same hand position, three attempts, best of three recorded), but they vary in calibration accuracy compared to clinical-grade devices. Treat a concerning home reading as a reason to get a clinical-grade test, not as a final diagnosis.
11. Does sarcopenia diagnosis differ by ethnicity? Yes, significantly. Asian populations — particularly women — tend to have lower absolute appendicular muscle mass at comparable strength and health levels than Western reference populations, which is why AWGS cutoffs are calculated separately from EWGSOP2's. Even within Asia, country-specific research (e.g., Indonesia-specific cutoffs published in 2024–2025) suggests further regional tailoring may be needed.
12. How often should sarcopenia testing be repeated? There's no single universal interval, but many geriatric practices reassess every 6–12 months for diagnosed or high-risk patients, and sooner after a hospitalization, major illness, or significant weight change, since muscle strength and mass can shift meaningfully over those timeframes.
Conclusion and Action Steps
Sarcopenia diagnosis isn't a single test — it's a structured process, and as you've now seen, it's a process that two equally credentialed experts following two different (equally legitimate) guidelines could interpret differently from your exact same numbers. That's not a reason to dismiss the diagnosis; it's a reason to engage with your results actively rather than passively accepting a label.
Your practical next steps:
If you have risk factors, ask for a SARC-F screen at your next appointment — it takes about five minutes.
If screening is positive, request an objective strength test (grip dynamometry or chair stand) and ask which cutoff values are being applied.
If strength is low, ask which muscle mass method (DXA, BIA, or ultrasound) is available and appropriate for you, and ask your provider to explain your specific number relative to the cutoff — not just whether you "passed" or "failed."
Regardless of your result, start (or maintain) progressive resistance training and aim for at least 1.2 g/kg of protein daily if you're in an at-risk category — these are the two interventions with the strongest evidence behind them.
Reassess periodically, especially after illness, hospitalization, or major changes in activity or weight.
Sarcopenia is one of the relatively few age-related conditions where early, accurate diagnosis genuinely changes the trajectory. Don't let an unfamiliar acronym or a confusing cutoff number stop you from asking the next question. Talk to your doctor, ask which framework they're using, and start building strength today.
This article is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider for personalized guidance, especially before starting a new exercise or nutrition program.
Related Articles
Walking and Sarcopenia: Can It Prevent Muscle Loss? The Science-Backed Truth | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | Dr T.S. DIDWAL
Prevent Sarcopenia & Osteoporosis: Your Guide to Strong Bones & Muscles | DR T S DIDWAL
References
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., et al. (2019). Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing, 48(1), 16–31. https://doi.org/10.1093/ageing/afy169
Cruz-Jentoft, A. J., Baeyens, J. P., Bauer, J. M., et al. (2010). Sarcopenia: European consensus on definition and diagnosis. Age and Ageing, 39(4), 412–423. https://doi.org/10.1093/ageing/afq034
Cruz-Jentoft et al. (2019), as above.
Voulgaridou, G., Tyrovolas, S., Detopoulou, P., et al. (2024). Diagnostic Criteria and Measurement Techniques of Sarcopenia: A Critical Evaluation. Nutrients, 16(3), 436. https://doi.org/10.3390/nu16030436
Jianghan et al. (2026). Interpretation of A Focus Shift From Sarcopenia to Muscle Health in the AWGS 2025 Consensus Update. Aging Medicine. https://doi.org/10.1002/agm2.70082
Westbury, L. D., et al. (2023). Recent sarcopenia definitions—prevalence, agreement and mortality associations among men. Journal of Cachexia, Sarcopenia and Muscle. https://doi.org/10.1002/jcsm.13160
Cruz-Jentoft et al. (2019), as above.
Voulgaridou et al. (2024), as above.
Studenski, S. A., Peters, K. W., Alley, D. E., et al. (2014). The FNIH sarcopenia project. Journals of Gerontology: Series A, 69(5), 547–558. https://doi.org/10.1093/gerona/glu010
Cruz-Jentoft et al. (2019), as above.
Dent, E., Woo, J., Scott, D., & Hoogendijk, E. O. (2021). Sarcopenia measurement in research and clinical practice. European Journal of Internal Medicine, 90, 1–9. https://doi.org/10.1016/j.ejim.2021.06.003
Wimer, L., Goncharova, E., Galkina, S., et al. (2023). The D3-creatine dilution method non-invasively measures muscle mass in mice. Aging Cell. https://doi.org/10.1111/acel.13897
Dent et al. (2021), as above.
Voulgaridou et al. (2024), as above.
Estimating Muscle Mass Using D3-Creatine Dilution: A Narrative Review of Clinical Implications. (2024). Journals of Gerontology: Series A. PMID: 38135279.
Wimer et al. (2023), as above.
Cruz-Jentoft et al. (2019), as above.
Jianghan et al. (2026), as above.
Jianghan et al. (2026), as above.
Jianghan et al. (2026), as above.
Bhasin, S., Travison, T. G., Manini, T. M., et al. (2020). Sarcopenia Definition: The Position Statements of the Sarcopenia Definition and Outcomes Consortium. Journal of the American Geriatrics Society, 68, 1410–1418. PMID: 32150289.
Bhasin et al. (2020), as above.
Boshnjaku, A., & Krasniqi, E. (2024). Diagnosing sarcopenia in clinical practice: international guidelines vs. population-specific cutoff criteria. Frontiers in Medicine, 11, 1405438. https://doi.org/10.3389/fmed.2024.1405438
Dent et al. (2021), as above.
Bhasin et al. (2020), as above.
Sarcopenia defined by GLIS predicts adverse postoperative outcomes in gastric cancer patients. (2025). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC11995652/
Chen, L. K., Liu, L. K., Woo, J., et al. (2014). Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. Journal of the American Medical Directors Association, 15(2), 95–101. https://doi.org/10.1016/j.jamda.2013.11.025
Indonesian optimal sarcopenia cutoff values of calf circumference, muscle strength, and physical performance. (2024–2025). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12311804/
Performance of the EWGSOP2 Cut-Points of Low Grip Strength for Identifying Sarcopenia and Frailty Phenotype. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8037004/
Westbury et al. (2023), as above.
Performance of the EWGSOP2 Cut-Points, as above.
Sarcopenia Definition and Outcomes Consortium 2020 Definition: Association and Discriminatory Accuracy with Disability in the Canadian Longitudinal Study on Aging. (2023). Journals of Gerontology: Series A, 78(9), 1597. https://academic.oup.com/biomedgerontology/article/78/9/1597/7179735
Wimer et al. (2023), as above.
Estimating Muscle Mass Using D3-Creatine Dilution, as above (note 15).
Dent et al. (2021), as above.
Sarcopenia Definitions and Outcomes Consortium (SDOC) Criteria are Strongly Associated With Malnutrition, Depression, Falls, and Fractures in High-Risk Older Persons. (2020). Journal of the American Medical Directors Association. PMID: 32771358.
Sarcopenia defined by GLIS predicts adverse postoperative outcomes, as above (note 26).
Prevalence and Fall Risk of Sarcopenia Based on the 2023 Korean Working Group on Sarcopenia Criteria. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12194967/
2025 AWGS Sarcopenia Guideline and Wake-up Call for Asian Gerontologists and Geriatricians. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12766309/
Voulgaridou et al. (2024), as above.
Voulgaridou et al. (2024), as above.
Sayer, A. A., Cooper, R., Arai, H., et al. (2024). Sarcopenia. Nature Reviews Disease Primers, 10(1), 68. https://doi.org/10.1038/s41572-024-00550-w
Definition and diagnosis of sarcopenia: Asia-Pacific perspectives. (2025). Osteoporosis and Sarcopenia, 11(2 Suppl), 2–10. https://doi.org/10.1016/j.afos.2025.05.004
Prevalence and Fall Risk of Sarcopenia Based on the 2023 Korean Working Group on Sarcopenia Criteria, as above (note 38).
Additional foundational sources:
Fielding, R. A., Vellas, B., Evans, W. J., et al. (2011). Sarcopenia: an undiagnosed condition in older adults. Journal of the American Medical Directors Association, 12(4), 249–256. https://doi.org/10.1016/j.jamda.2011.01.003
A focus shift from sarcopenia to muscle health in the Asian Working Group for Sarcopenia 2025 Consensus Update. PubMed. PMID: 41188603.
Sarcopenia in Ageing and Chronic Illness: Trial Endpoints and Regulatory Issues. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146653/
Global Leadership Initiative in Sarcopenia (GLIS) project overview. ESCEO. https://www.esceo.org/glis