Sarcopenic Obesity: How to Lose Fat Safely Without Losing Muscle
Learn how to treat sarcopenic obesity with evidence-based strategies for fat loss and lean mass preservation—protein, resistance training, and GLP-1 safety.
OBESITYSARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
1/22/202613 min read
If you’ve ever seen an older adult lose weight yet become weaker, slower, and more fragile, you’ve witnessed one of the most dangerous paradoxes in modern medicine: fat loss without muscle protection. This is the central challenge of sarcopenic obesity—a condition where visceral obesity coexists with low muscle mass and reduced strength, creating a high-risk metabolic and functional phenotype. Unlike simple obesity, sarcopenic obesity is strongly linked to mobility disability, insulin resistance, falls, and cardiometabolic complications, even when BMI appears “moderately elevated” or deceptively normal (Axelrod et al., 2023).
The biology is more complex than calories in versus calories out. Aging muscle develops anabolic resistance, meaning the same protein intake and exercise stimulus that once triggered robust muscle protein synthesis may no longer produce the same rebuilding response. Meanwhile, expanding visceral fat behaves like an endocrine organ, amplifying chronic inflammation and accelerating functional decline. This creates an urgent clinical priority: frailty prevention must become a core goal of weight management, not an afterthought (Glavas & Scott, 2025).
What makes sarcopenic obesity especially urgent today is the popularity of rapid weight-loss strategies—including aggressive calorie restriction and incretin-based therapies. While GLP-1 receptor agonists can deliver substantial fat reduction and metabolic benefits, they may also worsen sarcopenia if lean mass preservation is not treated as a co-therapy (Chen & Batsis, 2025). The goal is no longer simply “weight loss,” but body recomposition: reducing visceral adiposity while protecting skeletal muscle, strength, and independence.
Encouragingly, sarcopenic obesity is not fixed. Older adults can transition between sarcopenia, obesity, and recovery states depending on training, nutrition, and illness burden—making targeted interventions both realistic and essential (Xu et al., 2026). In this guide, you’ll learn the science-backed approach to losing fat without losing muscle—safely, strategically, and sustainably.
Clinical pearls
1. The "BMI Blind Spot": Never rely on BMI alone for older adults. A "stable" weight often masks weight cycling, where a patient loses 5 lbs of muscle and gains 5 lbs of fat. Always use waist circumference or BIA/DXA to uncover "hidden" adiposity.
2. Prioritise "Anabolic Thresholds": Older muscles are "anabolically resistant." To trigger muscle protein synthesis, patients must hit a threshold of 25–30g of high-quality protein per meal (specifically rich in the amino acid Leucine). Spreading protein thin (e.g., 5g at breakfast, 50g at dinner) is significantly less effective than even distribution.
3. Exercise Hierarchy: While aerobic exercise is vital for heart health, progressive resistance training (PRT) is the non-negotiable "medicine" for sarcopenic obesity. Without a mechanical load on the muscle, nutritional and pharmacological interventions often fail to prevent lean mass loss during weight reduction.
4. The GLP-1 "Muscle Tax": When prescribing GLP-1 receptor agonists, treat "muscle preservation" as a co-therapy. Monitor grip strength or gait speed at every follow-up. If functional strength declines, the dosage may need adjustment or the protein/resistance training requirements must be intensified.
5. The "Inflammaging" Link: View adipose tissue as an endocrine organ, not just a storage site. Visceral fat secretes pro-inflammatory cytokines (like IL-6 and TNF-$\alpha$) that directly "poison" muscle fibers. Reducing fat is not just about aesthetics; it is a primary strategy to lower systemic inflammation and "unlock" muscle growth potential.
Sarcopenic Obesity: Emerging Mechanisms, Clinical Management, and Future Therapeutic Approaches
What Is Sarcopenic Obesity? Defining the Condition
Sarcopenic obesity occurs when individuals simultaneously experience muscle loss (sarcopenia) and excess adiposity (obesity). This paradoxical condition means someone can have both low muscle mass and high body fat percentage—often appearing deceptively "normal" in terms of weight while harboring serious metabolic dysfunction.
The prevalence of sarcopenic obesity is particularly concerning in aging populations, with recent research highlighting its role in mobility disability, metabolic complications, and reduced quality of life. Understanding this condition requires examining its underlying mechanisms, epidemiological patterns, and therapeutic potential.
Sarcopenic Obesity Diagnosis
To diagnose sarcopenic obesity, clinicians confirm two key problems occurring together:
low muscle strength and/or low muscle mass + high body fat (adiposity).
Below are the most widely used clinical screening markers and cut-off criteria, presented in a clear, point-based format.
1) Muscle Strength (Earliest & Most Important Warning Sign)
Handgrip Strength (Primary Test)
Men: grip strength < 27 kg
Women: grip strength < 16 kg
Chair Stand Test (Alternative Functional Test)
≥ 15 seconds to complete 5 chair rises
Why this matters: Low strength often appears before measurable muscle mass loss, making it a sensitive early marker of sarcopenia.
2) Muscle Mass (DXA-Based Skeletal Muscle Index Cut-Off)
Appendicular Skeletal Muscle Mass Index (ASMI via DXA)
(= lean mass of arms + legs ÷ height²)
Men: < 7.0 kg/m²
Women: < 5.5 kg/m²
Clinical note: ASMI is widely used in geriatric medicine and research to define low muscle quantity.
3) Adiposity (Preferred Over BMI for Diagnosing Sarcopenic Obesity)
Body Fat Percentage (Recommended Marker)
Men: ≥ 25% total body fat
Women: ≥ 35% total body fat
Why fat% beats BMI: BMI often misses sarcopenic obesity because many older adults have normal or mildly elevated BMI despite significant muscle loss and high visceral fat.
4) Ethnic Adjustments (Important for Accurate Diagnosis)
Asian Populations
Often require stricter muscle mass cut-offs due to higher metabolic risk at lower body weight
Example: Women ASMI < 5.4 kg/m² (DXA-based)
Black / African Descent Populations
Tend to have higher baseline muscle mass
Standard cut-offs may underdiagnose sarcopenia
Higher thresholds may be more appropriate depending on population norms
Key point: Ethnic-specific cut-offs improve diagnostic accuracy and reduce under-recognition.
5) Advanced Imaging (Gold Standard in Research)
While DXA is commonly used, research settings often use:
CT or MRI at the L3 lumbar vertebra
Precisely measures skeletal muscle area
Detects myosteatosis (fat infiltration into muscle)
Provides a superior assessment of muscle quality, not just muscle quantity
Clinical relevance: Myosteatosis strongly predicts weakness, disability, insulin resistance, and poor outcomes.
The Emerging Mechanisms of Sarcopenic Obesity
Understanding the Pathophysiology
According to Axelrod, Dantas, and Kirwan (2023), sarcopenic obesity involves complex interactions between muscle protein metabolism, inflammatory pathways, and adipose tissue dysfunction. Their research in Metabolism reveals that emerging mechanisms underlying this condition extend far beyond simple caloric imbalance.
Key mechanisms include:
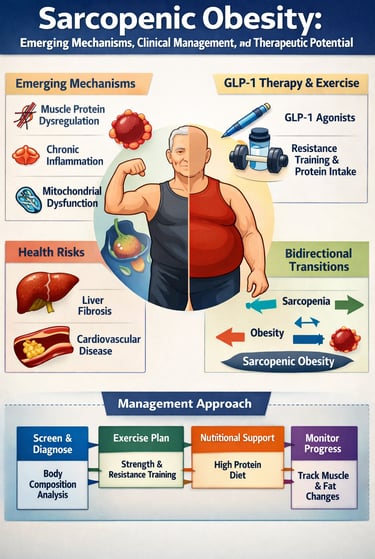
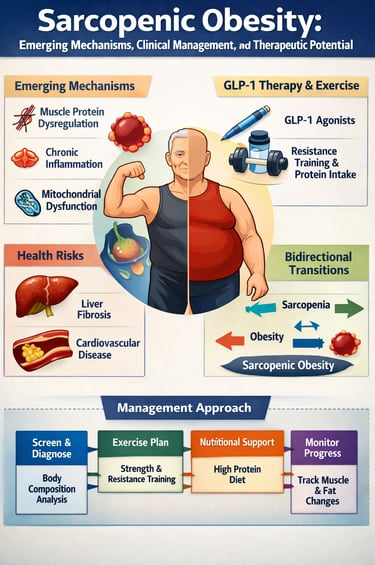
The authors identify muscle protein synthesis dysregulation as a primary driver, where aging combined with excessive fat accumulation impairs the body's ability to build and maintain muscle tissue. Simultaneously, chronic inflammation associated with adipose tissue overexpansion creates a hostile environment for muscle preservation. Additionally, mitochondrial dysfunction in both muscle and fat tissue compromises cellular energy production and metabolic efficiency. Their work emphasizes that therapeutic potential lies in targeting these specific mechanisms rather than treating obesity and sarcopenia independently.
Takeaway: Understanding the pathogenesis of sarcopenic obesity is essential for developing targeted interventions that address the root causes rather than symptoms alone.
Hormonal Decline and Sarcopenic Obesity: Why Aging Causes Fat Gain and Muscle Loss
The age-related decline in key sex hormones is one of the strongest biological drivers of the “fat-for-muscle swap” seen in older adults. This hormonal shift contributes directly to sarcopenic obesity, where muscle mass and strength decline while visceral (abdominal) fat increases, creating a high-risk metabolic and functional state. Below is a clear, SEO-optimized breakdown of how these endocrine changes accelerate muscle wasting, central fat accumulation, inflammation, and insulin resistance.
1) Testosterone Decline (Andropause)
Impact on Muscle: Lower testosterone reduces muscle protein synthesis and weakens satellite cell activity, limiting muscle repair and accelerating age-related muscle loss.
Impact on Fat: Testosterone normally suppresses fat storage. When it declines, visceral fat increases, along with systemic inflammation, worsening metabolic dysfunction
.
2) Estrogen Decline (Menopause)
Impact on Muscle: Estrogen helps protect muscle tissue. Its decline reduces muscle quality, strength output, and force generation.
Impact on Fat: Menopause promotes a shift from gynoid fat (hips/thighs) to android fat (abdominal/central)—a distribution strongly linked to insulin resistance and cardiometabolic risk.
3) Growth Hormone (GH) and IGF-1 Decline (Somatopause)
Aging reduces the GH/IGF-1 axis, weakening the body’s ability to:
preserve lean muscle mass
recover from training
regenerate tissues efficiently
This makes resistance training adaptation slower and increases vulnerability to sarcopenia.
4) DHEA Decline (Loss of a Key Anabolic Precursor)
Dehydroepiandrosterone (DHEA) drops sharply with age.
Low DHEA levels are consistently associated with:
increased fat mass
decreased muscle strength
reduced metabolic resilience in both men and women
5) Insulin Resistance (The Hormonal “Amplifier”)
As sex hormones fall, insulin sensitivity often declines, creating a vicious cycle:
easier fat storage
weaker anabolic response to dietary protein
reduced muscle-building signaling
This accelerates both obesity progression and muscle breakdown, fueling sarcopenic obesity.
The GLP-1 Revolution: Incretin Therapies for Sarcopenic Obesity
The 2025 research by Chen and Batsis published in Diabetes addresses a critical clinical question: how should incretin therapies—particularly GLP-1 receptor agonists—be utilized in patients with sarcopenic obesity?
This review reveals both significant therapeutic potential and notable challenges when using these medications. GLP-1 receptor agonists have revolutionized obesity treatment by promoting weight loss and improving metabolic health. However, Chen and Batsis (2025) highlight that these medications can accelerate muscle loss if not combined with appropriate resistance exercise and adequate protein intake.
Clinical perspectives include:
Healthcare providers must now balance the metabolic benefits of incretin therapies against their potential to worsen sarcopenia. The authors recommend combining GLP-1 agonists with nutritional interventions emphasizing protein optimization and structured resistance training to preserve lean mass while reducing fat. This integrated approach represents the future of sarcopenic obesity management in the era of incretin therapies.
Takeaway: While GLP-1 medications are effective for weight reduction, concurrent muscle-preserving strategies are essential in sarcopenic obesity populations.
Bidirectional Transitions: The Dynamic Nature of Sarcopenic Obesity
How Sarcopenia, Obesity, and Sarcopenic Obesity Interact
Groundbreaking research by Xu et al. (2026) published in the Chinese Medical Journal provides unprecedented insight into how individuals transition between sarcopenia, obesity, and sarcopenic obesity over time. This transitional patterns research challenges the static view of these conditions.
Using data from the CHARLS study (China Health and Retirement Longitudinal Study), the authors tracked older adults and identified bidirectional transitions—meaning individuals don't simply progress in one direction but can move between states. Some participants with sarcopenia develop obesity (creating sarcopenic obesity), while others with sarcopenic obesity improve in one dimension while declining in another.
Key epidemiological findings:
The study reveals that transitional patterns are common, with significant proportions of older adults experiencing multiple transitions. This discovery suggests that interventions must be dynamic and responsive to changing metabolic conditions rather than assuming static disease states. The CHARLS study demonstrates that factors influencing these transitions include lifestyle modifications, physical activity levels, and nutritional status changes.
Takeaway: Sarcopenic obesity is not a fixed condition; understanding transitional patterns helps predict who will benefit most from specific interventions.
Hepatic Complications: Sarcopenic Obesity and Liver Fibrosis
Cross-Sectional Analysis of Metabolic and Hepatic Health
Recent 2026 research by Ichikawa et al. published in Diagnostics reveals critical associations between sarcopenic obesity–related scores and liver fibrosis in patients with steatotic liver disease. This study expands our understanding of how sarcopenic obesity extends beyond musculoskeletal health to affect vital organs.
The research identifies specific scoring systems for sarcopenic obesity and correlates these with hepatic fibrosis markers. Patients with elevated sarcopenic obesity scores demonstrated higher prevalence of liver fibrosis, suggesting that the metabolic dysfunction characterizing sarcopenic obesity directly impacts hepatic health.
Clinical implications include:
Patients with sarcopenic obesity require comprehensive metabolic assessment including liver function evaluation. The presence of steatotic liver disease (fatty liver) combined with sarcopenic obesity creates a particularly vulnerable metabolic phenotype. Healthcare providers should implement hepatic screening protocols for all individuals identified with sarcopenic obesity, as liver fibrosis progression may accelerate without intervention.
Takeaway: Sarcopenic obesity has systemic metabolic consequences; liver health assessment should be integral to comprehensive sarcopenic obesity management.
Cardiovascular Risk: Sarcopenic Obesity and Atherosclerosis
Current Status and Research Progress on Vascular Complications
Yang et al. (2025) published comprehensive research in the Journal of Clinical Medicine examining the association between sarcopenic obesity and atherosclerosis. This review synthesizes current knowledge while identifying research challenges and future directions.
The authors establish that sarcopenic obesity creates a particularly pro-atherogenic metabolic environment through multiple mechanisms. Visceral adiposity associated with sarcopenic obesity produces inflammatory cytokines that promote atherosclerosis development. Simultaneously, reduced muscle mass diminishes the protective metabolic effects of muscle, which normally produces anti-inflammatory compounds and regulates glucose metabolism.
Cardiovascular research highlights:
The association between sarcopenic obesity and atherosclerosis appears stronger than either condition alone, suggesting synergistic negative effects. Low muscle mass impairs endothelial function, while excess adiposity promotes atherosclerotic plaque development. Yang et al. recommend early cardiovascular screening for all sarcopenic obesity patients and aggressive risk factor modification including physical activity, nutritional optimization, and when appropriate, pharmacological interventions.
Takeaway: Sarcopenic obesity significantly elevates cardiovascular disease risk; this must influence clinical assessment and treatment priorities.
Expert Management Strategies: Pathogenesis, Epidemiology, and Treatment
Comprehensive Review of Clinical Approaches
Glavas and Scott (2025), writing in the Expert Review of Endocrinology & Metabolism, provide authoritative guidance on sarcopenic obesity management in older adults. Their review synthesizes pathogenesis understanding with practical epidemiology data and evidence-based management strategies.
The authors emphasize that sarcopenic obesity management requires a multidisciplinary approach addressing multiple physiological systems simultaneously. They detail how understanding pathogenesis—including myostatin activation, insulin resistance, mitochondrial dysfunction, and chronic inflammation—informs clinical decision-making.
Expert management recommendations:
Resistance training forms the cornerstone of intervention, providing both muscle strengthening and metabolic benefits. Concurrent nutritional optimization emphasizing high-quality protein intake (1.2-1.6 g/kg body weight daily) supports muscle protein synthesis. Metabolic medications including metformin, GLP-1 agonists, and emerging therapies must be selected considering their effects on muscle mass preservation. The authors advocate for individualized assessment of each patient's specific combination of sarcopenia severity and obesity degree to tailor interventions appropriately.
Takeaway: Sarcopenic obesity management demands comprehensive, individualized approaches integrating exercise, nutrition, and pharmacology.
Clinical Characterization: The SARA-OBS Trial
Multicenter Observational Evidence from Older Adults at Risk
The SARA-OBS trial, conducted by Fielding, Rolland, Bruyere, and colleagues (2025) and published in BMC Geriatrics, provides crucial clinical characterization of sarcopemia and sarcopenic obesity in patients aged 65 and older who face mobility disability risk. This multicenter observational trial represents one of the most comprehensive real-world assessments of these conditions.
The SARA-OBS study established detailed clinical criteria for identifying and classifying sarcopenia and sarcopenic obesity in high-risk older populations. By following participants across multiple centers, researchers documented the prevalence of these conditions, their relationship to mobility outcomes, and how different assessment methods capture disease severity.
Key SARA-OBS findings:
The trial revealed that sarcopenic obesity affects a substantial proportion of older adults "at risk of mobility disability," and that those with sarcopenic obesity experience particularly rapid functional decline. Importantly, the study demonstrated that standard weight-based assessment misses many cases—individuals who appear overweight or normal-weight by BMI standards may harbor significant sarcopenic obesity. The researchers emphasize the critical need for body composition assessment beyond simple weight measurements, including muscle mass evaluation via imaging or bioelectrical impedance analysis.
Takeaway: The SARA-OBS trial confirms that sarcopenic obesity is both prevalent and serious in older adults; clinical assessment requires advanced body composition analysis beyond traditional metrics.
Comprehensive FAQ: Your Questions About Sarcopenic Obesity Answered
What's the difference between sarcopenia, obesity, and sarcopenic obesity?
Sarcopenia involves muscle loss, often accompanied by normal or reduced body weight. Obesity means excess body fat often with normal muscle mass. Sarcopenic obesity combines both—low muscle mass with high body fat, creating metabolic dysfunction more severe than either condition alone.
How is sarcopenic obesity diagnosed?
Diagnosis requires body composition analysis including muscle mass assessment (via DXA, CT, or bioelectrical impedance) combined with adiposity measures. Various scoring systems and diagnostic criteria exist; your healthcare provider should use standardized approaches aligned with established guidelines.
Can sarcopenic obesity be reversed?
Yes, research shows bidirectional transitions are possible. Combining resistance exercise, nutritional optimization, and appropriate pharmacological therapy can improve both muscle mass and fat reduction. However, early intervention is more effective than late-stage treatment.
Are GLP-1 medications safe for sarcopenic obesity patients?
GLP-1 agonists are effective for weight loss but can accelerate muscle loss if used without accompanying resistance training and adequate protein intake. They're safe when combined with proper muscle-preserving strategies.
What role does nutrition play in managing sarcopenic obesity?
Protein optimization is essential—older adults with sarcopenic obesity typically need 1.2-1.6 grams of protein per kilogram of body weight daily. Beyond protein, overall caloric balance and micronutrient adequacy support muscle maintenance while achieving fat loss.
Does sarcopenic obesity affect organs besides muscles?
Yes, research shows associations with liver fibrosis in steatotic liver disease and increased atherosclerosis risk. Systemic inflammation underlying sarcopenic obesity affects multiple organs, making comprehensive health screening essential.
What exercise is best for sarcopenic obesity?
Resistance training 2-3 times weekly, combined with aerobic activity, provides optimal results. Progressive strength training targeting major muscle groups preserves and builds lean mass while cardiovascular exercise supports metabolic health.
Key Takeaways: What You Need to Know About Sarcopenic Obesity
Sarcopenic obesity is a distinct condition combining muscle loss and excess fat, creating metabolic risks exceeding either condition alone.
Emerging mechanisms including muscle protein synthesis dysregulation, mitochondrial dysfunction, and chronic inflammation drive the condition and suggest targeted interventions.
Modern therapies like GLP-1 agonists effectively reduce weight but require concurrent muscle-preserving strategies to prevent sarcopenia worsening.
Bidirectional transitions between sarcopenia, obesity, and sarcopenic obesity are common, suggesting dynamic disease processes requiring adaptive management.
Systemic complications extend beyond muscles—liver fibrosis and atherosclerosis risk are significantly elevated, requiring comprehensive screening.
Effective management demands multidisciplinary approaches integrating resistance exercise, nutritional optimization, and selective pharmacotherapy.
Proper diagnosis requires body composition analysis, not weight-based assessment alone, as many affected individuals appear normal weight
.
Call to Action: Take Control of Your Metabolic Health
Understanding sarcopenic obesity empowers you to take proactive steps toward better health. Whether you're concerned about your muscle mass, managing weight challenges, or seeking preventive strategies:
Consider scheduling a comprehensive health assessment with a healthcare provider who understands sarcopenic obesity. Request body composition analysis beyond standard weight measurements. Discuss how resistance training and nutritional optimization might benefit your specific situation. If appropriate for your circumstances, explore whether pharmacological therapies could support your health goals.
Don't wait for advanced complications of sarcopenic obesity to develop. The research clearly demonstrates that early intervention—combining exercise, nutrition, and appropriate medical management—can reverse sarcopenic obesity and restore metabolic health. Your muscles are metabolic powerhouses; preserving them while achieving healthy body composition creates the foundation for long-term wellness.
Author’s Note
Sarcopenic obesity is one of the most clinically underdiagnosed yet biologically important conditions in modern aging medicine. It is not merely “weight gain with aging,” but a dual disorder—progressive muscle loss combined with excess (often visceral) adiposity—that amplifies insulin resistance, chronic inflammation, frailty, falls, cardiometabolic disease, and loss of independence.
This article was written to bridge the gap between research evidence and real-world clinical decision-making, especially in an era where rapid weight-loss strategies (including GLP-1 receptor agonists) are increasingly common. While fat reduction can dramatically improve metabolic outcomes, preserving skeletal muscle remains essential because muscle is not only a movement tissue, but also a key endocrine and metabolic organ.
The goal of this review-style guide is to help clinicians, health professionals, and educated readers understand why sarcopenic obesity develops, how it evolves over time, how it impacts multiple organs, and how to design management strategies that are both scientifically grounded and functionally meaningful. Most importantly, it reinforces a central principle: successful obesity treatment in older adults must prioritize strength, protein adequacy, and functional capacity—not the scale alone.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Losing Weight but Weak? Hidden Sarcopenic Obesity Risks Explained | DR T S DIDWAL
How to Prevent and Reverse Muscle Wasting in Chronic Disease (2025 Guide) | DR T S DIDWAL
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Who Gets Sarcopenia? Key Risk Factors & High-Risk Groups Explained | DR T S DIDWAL
Sarcopenia: The Complete Guide to Age-Related Muscle Loss and How to Fight It | DR T S DIDWAL
Best Exercises for Sarcopenia: Strength Training Guide for Older Adults | DR T S DIDWAL
Vitamin D Deficiency and Sarcopenia: The Critical Connection | DR T S DIDWAL
References
Axelrod, C. L., Dantas, W. S., & Kirwan, J. P. (2023). Sarcopenic obesity: Emerging mechanisms and therapeutic potential. Metabolism, 148, 155639. https://doi.org/10.1016/j.metabol.2023.155639
Chen, A. S., & Batsis, J. A. (2025). Treating sarcopenic obesity in the era of incretin therapies: Perspectives and challenges. Diabetes, 74(12), 2179–2190. https://doi.org/10.2337/dbi25-0004
Fielding, R. A., Rolland, Y., Bruyere, O., et al. (2025). Characterizing sarcopenia and sarcopenic obesity in patients aged 65 years and over, at risk of mobility disability: A multicenter observational trial (SARA-OBS). BMC Geriatrics, 25, 590. https://doi.org/10.1186/s12877-025-05895-9
Glavas, C., & Scott, D. (2025). Sarcopenic obesity: Pathogenesis, epidemiology and management in older adults. Expert Review of Endocrinology & Metabolism, 20(6), 461–469. https://doi.org/10.1080/17446651.2025.2543811
Ichikawa, T., Miuma, S., Yamashima, M., Yamamichi, S., Koike, M., Nakano, Y., Yajima, H., Miyazaki, O., Ikeda, T., Okamura, T., Komatsu, N., Kakizoe, M., Tanaka, R., & Miyaaki, H. (2026). Association between sarcopenic obesity–related scores and liver fibrosis in patients with steatotic liver disease: A cross-sectional study. Diagnostics, 16(2), 324. https://doi.org/10.3390/diagnostics16020324
Xu, F., Lin, W., Yue, L., Yue, J., Dong, B., Ge, N., Li, K., & Liu, X. (2026). Bidirectional transitions of sarcopenia, obesity, and sarcopenic obesity: Transitional patterns in older adults from the CHARLS study. Chinese Medical Journal, 139(2), 299–301. https://doi.org/10.1097/CM9.0000000000003925
Yang, K., Yang, W., Si, S.-C., Liu, J., Ma, Y.-X., & Zhao, H. (2025). Research progress on the association between sarcopenic obesity and atherosclerosis: Current status and challenges. Journal of Clinical Medicine, 14(22), 8148. https://doi.org/10.3390/jcm14228148