Testosterone and Longevity in Aging Men: How Hormonal Health Shapes Metabolism, Muscle, and Vitality
Unlock the connection between hormonal optimization and life extension. This evidence-based guide explores the critical link between testosterone and metabolic vitality, synthesizing 2024–2025 clinical data on TRT, PADAM, and long-term health outcomes for aging men.
AGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/18/202618 min read
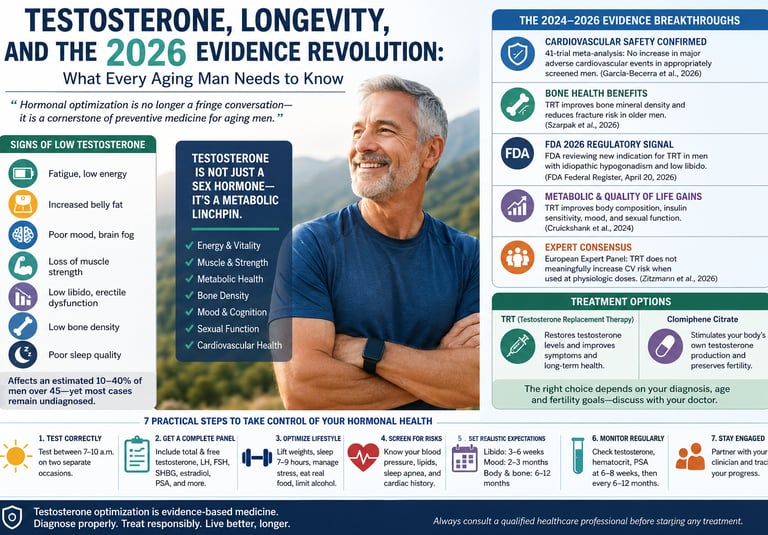
Hormonal optimization is no longer a fringe conversation — it is a cornerstone of preventive medicine for aging men.
For generations, millions of men have quietly accepted fatigue, weight gain, declining strength, low libido, poor sleep, and fading motivation as the unavoidable price of getting older. The narrative has been repeated so often that many no longer question it: testosterone declines with age, energy disappears, metabolism slows, and vitality simply fades away. But the science emerging in 2024–2026 is challenging that assumption with unprecedented force. A growing body of endocrinology and longevity research now suggests that testosterone is not merely a “male sex hormone,” but a central regulator of metabolic health, cardiovascular resilience, bone integrity, cognitive performance, and healthy aging itself (de Silva et al., 2024; Cruickshank et al., 2024).
What makes this moment especially important is that the conversation around testosterone replacement therapy (TRT) is undergoing a dramatic scientific transformation. For years, fear surrounding heart attacks, strokes, and prostate cancer dominated public discussion. Yet newer evidence — including the landmark TRAVERSE-related analyses, a 41-trial meta-analysis, and major European expert statements — is painting a far more nuanced picture. In appropriately screened men with genuine hypogonadism, testosterone therapy may not only improve symptoms, but also potentially reduce aspects of metabolic and skeletal decline associated with aging (García-Becerra et al., 2026; Zitzmann et al., 2026).
At the same time, researchers are uncovering how low testosterone intersects with obesity, insulin resistance, sleep apnea, chronic inflammation, osteoporosis, and even reduced lifespan. Testosterone deficiency is increasingly being viewed not as a cosmetic issue, but as a systemic medical condition with whole-body consequences
The result is what many experts now describe as an evidence revolution in men’s health. In 2026, the question is no longer whether testosterone matters. The real question is this: when aging men lose hormonal health, how much of their future healthspan disappears with it?
Key Takeaways About Testosterone, Longevity, and Healthy Aging
1. Low Testosterone Is Linked to More Than Sexual Symptoms
Testosterone deficiency affects far more than libido. Research shows low testosterone is associated with increased visceral fat, insulin resistance, reduced muscle mass, low bone density, fatigue, mood changes, and higher cardiometabolic risk (de Silva et al., 2024).
2. Modern Evidence Shows TRT Is Safer Than Previously Believed
Large contemporary studies — including a 41-trial meta-analysis and TRAVERSE-related data — found no significant increase in heart attack, stroke, or prostate cancer risk in appropriately screened men receiving physiological testosterone replacement therapy (García-Becerra et al., 2026; Zitzmann et al., 2026).
3. Testosterone Plays a Major Role in Metabolic Health
Declining testosterone contributes to abdominal obesity, metabolic syndrome, and worsening insulin sensitivity. Experts increasingly view hypogonadism as a metabolic disorder, not merely a reproductive condition
4. Bone Health Benefits Are Emerging as a Major TRT Advantage
Newer research suggests testosterone replacement therapy may improve bone mineral density and reduce fracture risk in older men, making hormonal health important for healthy aging and mobility preservation (Szarpak et al., 2026).
5. Fertility-Friendly Alternatives to TRT Exist
Men who wish to preserve fertility may benefit from therapies such as clomiphene citrate, which can stimulate the body’s own testosterone production without suppressing sperm generation (Câmara, 2025).
6. Lifestyle Still Matters — Even With Hormonal Therapy
Resistance training, quality sleep, weight management, stress reduction, and treatment of sleep apnea remain foundational for healthy testosterone levels. TRT works best when combined with evidence-based lifestyle medicine, not as a substitute for it.
TRT is not appropriate for every patient. Men with untreated severe obstructive sleep apnea, markedly elevated hematocrit, active prostate cancer, uncontrolled heart failure, or those actively pursuing fertility require specialized evaluation before therapy is considered
More Than Just a "Male Hormone"
Fatigue that no amount of sleep seems to fix. A waistline that expands despite clean eating. A mood that feels flat, blunted, dimmed. If you are a man over 40 and recognizing yourself in these words, you are not imagining things — and you are far from alone.
Testosterone is frequently dismissed in popular culture as little more than the "aggression hormone" or the driver of youthful athletic performance. In reality, it is a master regulator of the entire male body — governing insulin sensitivity, muscle architecture, bone mineral density, cognitive sharpness, cardiovascular resilience, and emotional equilibrium. When its levels decline, the effects cascade quietly across virtually every organ system.
What makes 2026 a pivotal year for men's hormonal health is not a single discovery, but the convergence of landmark evidence from four continents, a formal U.S. Food and Drug Administration regulatory signal, and the largest cardiovascular meta-analysis in testosterone research history. Together, these developments are rewriting clinical guidelines — and offering real hope to the millions of men who have been told that declining vitality is simply "part of getting older."
This article synthesizes that evidence in plain language, so you can walk into your next doctor's appointment as an informed partner in your own health.
What Is Hypogonadism, and Why Does It Matter?
Hypogonadism — clinically defined as insufficient testosterone production or impaired hormonal action — is not a rare condition. It affects an estimated 10–40% of men over 45, depending on the diagnostic criteria used, yet the majority of cases remain undiagnosed and untreated.
A landmark review by de Silva et al. (2024), published in The Lancet Diabetes & Endocrinology, provides the most comprehensive contemporary map of male hypogonadism: its origins, its diagnostic standards, and its management pathways. The review draws a critical distinction between two forms of the condition. Primary hypogonadism arises from testicular dysfunction — the gland itself fails to produce adequate testosterone despite receiving appropriate hormonal signals from the brain. Secondary hypogonadism originates higher up, in the hypothalamic-pituitary axis, where inadequate signaling means the testes are never properly stimulated. A third category — age-related androgen decline, sometimes termed Partial Androgen Deficiency in Aging Men (PADAM) — represents perhaps the most clinically relevant form for the majority of men seeking answers today (de Silva et al., 2024).
Understanding which form of hypogonadism a man has is not academic hair-splitting. It directly determines which treatment will work, how the body will respond, and what monitoring is required. This is personalized medicine in its most practical form.
PADAM: The Silent Driver of Metabolic Decline
Testosterone levels in men decline at an average rate of roughly 1–2% per year after the age of 30. For many men, this gradual slide crosses a clinical threshold somewhere between their mid-forties and sixties — entering the territory of PADAM. Unlike the abrupt hormonal collapse of menopause in women, this is a slow erosion, which is precisely why it goes undetected for so long.
Pechersky (2025) established groundbreaking evidence that PADAM does not merely accompany metabolic syndrome — it actively drives its development. Androgen deficiency promotes visceral fat accumulation, impairs insulin signaling at the cellular level, raises inflammatory cytokine levels, and disrupts lipid metabolism. The result is a cluster of conditions — central obesity, elevated blood glucose, high triglycerides, low HDL cholesterol, and hypertension — that together constitute metabolic syndrome and dramatically elevate cardiovascular risk.
More recent work by Pechersky (2025) extends this understanding to the prostate gland, clarifying that the relationship between androgens and prostate disease is far more nuanced than the simplistic "testosterone feeds cancer" narrative that has historically deterred both doctors and patients from pursuing treatment. The contemporary model follows a "saturation theory": prostate androgen receptors become saturated at relatively low testosterone concentrations, meaning that restoring testosterone from deficient to physiological levels does not meaningfully increase prostate stimulation beyond what already occurs in the normal range.
The practical upshot is significant: untreated androgen deficiency may itself be a risk factor for worse prostate health outcomes over time — precisely the opposite of the historical assumption.
Zitzmann (2026) argues that many aging men develop a form of “functional testosterone deficiency” driven not only by age itself, but by obesity, insulin resistance, chronic inflammation, poor sleep, and systemic metabolic disease. The paper emphasizes that declining testosterone is often reversible or partially reversible when underlying lifestyle and cardiometabolic factors are treated. Zitzmann highlights that diagnosis should combine symptoms with repeated biochemical testing, and that Testosterone Replacement Therapy (TRT) may benefit carefully selected men after proper cardiovascular, prostate, and fertility evaluation. The article also stresses that resistance exercise, weight reduction, sleep optimization, and metabolic health remain foundational alongside any hormonal therapy.
The TestES Synthesis: Reframing TRT as Chronic Disease Prevention
The single most comprehensive analysis of testosterone replacement therapy (TRT) in recent years comes from Cruickshank et al. (2024), whose TestES evidence synthesis was published in Health Technology Assessment. Spanning randomized controlled trials, observational studies, and real-world data across diverse patient populations, this exhaustive review arrived at conclusions that are both reassuring and clinically actionable.
Sexual function was among the most robustly documented benefits. Improvements in libido, erectile function, and sexual satisfaction emerged consistently within 6–12 weeks of treatment initiation — a timeline now confirmed across multiple trial populations.
Metabolic health improvements followed a longer arc. Reductions in visceral adiposity, improvements in insulin sensitivity, favorable shifts in body composition, and gains in bone mineral density accumulated over months rather than weeks. The TestES team emphasized that TRT functions as what might be called a "metabolic multiplier" — amplifying the benefits of concurrent exercise and dietary improvements rather than replacing them.
Mood and cognition improved significantly in treated men, though these benefits developed more gradually than the sexual function benefits, reflecting distinct neurobiological mechanisms.
Prostate safety, historically the greatest point of concern, was addressed directly. The synthesis found that TRT does not increase prostate cancer incidence in appropriately screened men, and does not accelerate benign prostatic hyperplasia in most patients — though individualized baseline assessment and regular PSA monitoring remain standard of care.
Perhaps most strikingly for healthcare policymakers and payers, the TestES economic analysis found that evidence-based TRT may reduce net healthcare expenditure over time by preventing the downstream costs associated with untreated hypogonadism: cardiovascular events, fragility fractures, metabolic syndrome progression, and lost workplace productivity (Cruickshank et al., 2024).
2026: A Year of Regulatory and Scientific Milestones
The FDA's Historic Signal
On April 20, 2026, the U.S. Food and Drug Administration published a landmark notice in the Federal Register (Docket No. FDA-2025-N-6743) that reflects a fundamental shift in regulatory thinking. Following a December 2025 expert panel convened to review the accumulated evidence, the FDA announced that its preliminary review of published literature suggests TRT may be safe and effective for a new indication: the treatment of low libido in men with decreased libido associated with idiopathic hypogonadism — that is, low testosterone without an identified structural or genetic cause (FDA, 2026).
This is significant for several reasons. Currently approved TRT products carry a labeling limitation explicitly stating that "safety and efficacy of TRT in men with age-related hypogonadism have not been established." The FDA's new notice invites manufacturers to submit supplemental new drug applications targeting this broader population — a regulatory step that, if successful, would formalize evidence-based TRT access for millions of men who currently occupy a clinical gray zone.
The FDA's referenced clinical evidence includes the TRAVERSE-linked data from Pencina et al. (2024), which documented improvements in sexual function and hypogonadal symptoms in men receiving TRT, and the foundational Testosterone Trials (T-Trials) led by Snyder et al. (2016). Together, these provide the evidentiary backbone for a potential expansion of TRT's formal indications — a development that practitioners and patients alike should follow closely.
Bone Health: A Previously Underappreciated Benefit
A 2026 study by Szarpak, Al-Jeabory, Pecold, and Maslyk, published in The Aging Male, adds an important dimension to the TRT benefit profile that has historically received less attention than cardiovascular and sexual outcomes: skeletal health. Their analysis demonstrates that TRT in older men is associated with meaningful improvements in bone mineral density and a measurable reduction in fracture risk — outcomes of enormous practical importance given that osteoporosis-related fractures are a leading cause of disability and mortality in aging men (Szarpak et al., 2026).
This finding reinforces the case for viewing TRT not as a lifestyle intervention but as a bone-protective therapy in appropriately selected men with confirmed androgen deficiency — particularly those with additional osteoporosis risk factors.
Cardiovascular Safety: The Definitive 41-Trial Meta-Analysis
Perhaps the most consequential 2026 publication for clinical practice is the systematic review and meta-analysis by García-Becerra, Arias-Gallardo, Juárez-García et al., published in the International Journal of Impotence Research. Synthesizing data from 41 randomized controlled trials, this is the largest and most rigorous analysis of TRT's cardiovascular and prostate cancer risk profile to date.
The findings are, on balance, profoundly reassuring for appropriately selected patients. The meta-analysis found no significant increase in major adverse cardiovascular events attributable to TRT in men without pre-existing severe cardiovascular disease, and confirmed that TRT does not increase prostate cancer incidence in men with normal baseline PSA and prostate examination (García-Becerra et al., 2026).
These findings are reinforced by a 2026 position statement from the European Expert Panel for Testosterone Research, led by Zitzmann, Rastrelli, Murray et al., published in Andrology. Their analysis synthesizes lessons from the landmark TRAVERSE trial — the largest prospective cardiovascular safety trial of TRT ever conducted — and draws two key clinical conclusions: first, that TRT does not meaningfully increase cardiovascular risk in men with hypogonadism who are appropriately screened; and second, that the historical cardiovascular concerns surrounding testosterone therapy were substantially driven by studies using supraphysiological (above-normal) doses in non-hypogonadal men — a fundamentally different clinical scenario from therapeutic replacement in confirmed deficiency (Zitzmann et al., 2026).
Beyond Testosterone Injections: Clomiphene Citrate as a Fertility-Preserving Alternative
Standard TRT works by introducing exogenous (external) testosterone into the body. This reliably raises serum testosterone levels — but it also suppresses the brain's natural hormonal signaling, leading to reduced sperm production. For men who have completed their families or who have primary testicular disease, this is rarely a concern. For younger men or those hoping to conceive, it is a critical consideration.
Câmara (2025) presents compelling evidence for clomiphene citrate as a fertility-preserving alternative. Rather than replacing testosterone externally, clomiphene works by blocking estrogen receptors at the hypothalamic-pituitary axis — effectively "tricking" the brain into amplifying its own production of the hormones (LH and FSH) that stimulate testicular testosterone and sperm production. The result is a rise in endogenous testosterone without suppressing spermatogenesis.
Clomiphene is not appropriate for all presentations of hypogonadism — it works best in secondary hypogonadism where the pituitary-hypothalamic axis is functional — but for carefully selected patients, it offers a medically sound and evidence-supported path that preserves reproductive options.
Practical Applications: What You Can Do Right Now
Evidence-based medicine is only useful if it translates into real-world action. Here is a practical framework built directly from the 2024–2026 literature.
1. Time your blood draw correctly. Testosterone levels follow a strong circadian rhythm, peaking between 7:00 and 10:00 a.m. Testing in the afternoon can produce artificially low results. Current guidelines require at least two separate early-morning measurements before a diagnosis of hypogonadism is confirmed.
2. Request a complete hormonal panel, not just total testosterone. Free testosterone, LH, FSH, SHBG (sex hormone-binding globulin), estradiol, and prolactin levels all contribute to accurate diagnosis and treatment selection. An isolated total testosterone measurement is insufficient for comprehensive assessment.
3. Optimize the lifestyle foundation before expecting treatment to do all the work. Resistance exercise, adequate sleep (7–9 hours per night), reduction of central adiposity, stress management, and avoidance of excess alcohol all support endogenous testosterone production and amplify the metabolic benefits of TRT when it is initiated. TRT is a multiplier — not a substitute.
4. Discuss fracture risk explicitly with your doctor. The Szarpak et al. (2026) bone health data means that DEXA scan screening for bone mineral density is worth discussing alongside testosterone testing, particularly if you are over 60 or have additional risk factors for osteoporosis.
5. Understand your cardiovascular baseline before starting treatment. The García-Becerra et al. (2026) meta-analysis and the Zitzmann et al. (2026) European position statement both support TRT safety in appropriately screened patients. "Appropriately screened" means knowing your blood pressure, lipid profile, and cardiac history — and sharing these with the prescribing clinician.
6. Set realistic timeline expectations. Sexual function and libido typically improve within 3–6 weeks of adequate testosterone optimization. Mood stabilization follows over 2–3 months. Meaningful changes in body composition, muscle mass, and bone density require 6–12 months of consistent treatment.
7. Maintain ongoing monitoring. Effective and safe TRT is not a "set it and forget it" intervention. Testosterone levels, hematocrit (red blood cell concentration), PSA, and symptom scores should all be reviewed at 6–8 weeks after initiation, then every 6–12 months thereafter.
Frequently Asked Questions
Q1: How do I know if my symptoms are from low testosterone or just normal aging?
Fatigue, reduced libido, mood changes, increased belly fat, and declining muscle mass can all have multiple causes — including thyroid dysfunction, sleep apnea, depression, and vitamin D deficiency. A confirmed biochemical diagnosis (two early-morning low testosterone readings) is required before attributing these symptoms to hypogonadism. Self-diagnosis based on symptoms alone is not sufficient and can lead to unnecessary treatment.
Q2: Will TRT raise my risk of heart attack or stroke?
Based on the best current evidence — including the 41-trial meta-analysis by García-Becerra et al. (2026) and the TRAVERSE trial insights synthesized by Zitzmann et al. (2026) — TRT does not significantly increase cardiovascular risk in men with confirmed hypogonadism who are appropriately screened. In fact, untreated hypogonadism itself is associated with metabolic syndrome and elevated cardiovascular risk. Comprehensive baseline assessment and regular monitoring are essential.
Q3: Does testosterone therapy cause prostate cancer?
Current evidence, including the TestES synthesis by Cruickshank et al. (2024) and the work of Pechersky (2025), does not support the idea that restoring testosterone to physiological levels in deficient men increases prostate cancer incidence. The "saturation model" of prostate receptor biology explains why this is the case. Regular PSA monitoring remains standard practice, not because TRT is inherently dangerous to the prostate, but because ongoing surveillance is good medicine for any man over 45.
Q4: Is TRT appropriate for men who want to have children?
Standard TRT suppresses sperm production and is not the right choice for men planning to conceive. For these men, clomiphene citrate — which stimulates the body's own testosterone and sperm production — is often the preferred evidence-based alternative, as documented by Câmara (2025).
Q5: What does the FDA's 2026 notice mean for my access to TRT?
The April 2026 Federal Register notice signals that the FDA is actively evaluating an expansion of TRT's approved indications to include men with idiopathic hypogonadism (low testosterone without a known structural or genetic cause). This is a regulatory process, not an immediate change in prescribing rules — but it reflects a significant shift in the official U.S. regulatory perspective on TRT, and may ultimately broaden access for men who currently fall outside the narrow existing indications.
Q6: How long would I need to stay on TRT?
Hypogonadism is generally a long-term condition, and most men who respond well to TRT remain on treatment indefinitely. Discontinuation returns testosterone levels to their pre-treatment baseline. Men on clomiphene citrate may retain some improved endogenous production after stopping, though this varies individually.
Q7: Are there natural ways to boost testosterone without medication?
Lifestyle interventions — resistance training, adequate sleep, stress reduction, weight management, and correcting nutritional deficiencies (particularly vitamin D and zinc) — have meaningful but modest effects on testosterone. They are essential companions to any hormonal therapy, but in men with confirmed hypogonadism and significant symptoms, lifestyle alone is rarely sufficient to restore testosterone to optimal levels. The evidence supports treating the deficiency medically while simultaneously optimizing lifestyle.
Clinical pearls
1. Defining Hypogonadism: Root Cause Dictates Treatment
Scientific Perspective: Accurately distinguishing between primary hypogonadism (testicular failure), secondary hypogonadism (hypothalamic-pituitary axis dysfunction), and Partial Androgen Deficiency in Aging Men (PADAM) is clinically mandatory. Because the underlying etiology dictates therapeutic options, diagnostic panels must include LH, FSH, and SHBG to appropriately map the hormonal axis before initiating therapy.
Low testosterone isn't a one-size-fits-all issue. Sometimes the issue is in the testes, and sometimes it's a signaling problem in the brain. Figuring out exactly why your levels are low is the only way your doctor can pick the treatment that will actually work for you.
2. Metabolic Multiplication: TRT is a Scaffolding, Not a Cure
Scientific Perspective: Data from the 2024 TestES evidence synthesis demonstrates that TRT serves as a "metabolic multiplier" rather than a standalone monotherapy. While it actively improves insulin sensitivity and reduces visceral adiposity over a multi-month arc, its clinical efficacy is maximized when paired with concurrent resistance training, nutritional interventions, and sleep optimization.
Think of testosterone therapy as a booster, not a magic pill. It makes your workouts more effective and helps burn belly fat, but it doesn't replace healthy habits. You still need to lift weights, eat well, and sleep 7 to 9 hours a night to get the real longevity benefits.
3. The Prostate "Saturation Theory" Cracks the Historical Narrative
Scientific Perspective: Modern evidence (Pechersky, 2025; García-Becerra et al., 2026) supports the "saturation theory" of prostate biology. Prostate androgen receptors become fully saturated at relatively low serum testosterone concentrations. Therefore, restoring a hypogonadal man to physiological (normal) levels does not increase prostate cancer risk or accelerate benign prostatic hyperplasia (BPH).
For decades, doctors worried that testosterone therapy would "feed" prostate cancer. New research proves this fear was wrong. Your prostate receptors get full at very low levels, meaning bringing your testosterone back up to a normal, healthy range does not increase your risk of prostate cancer.
4. Cardiovascular Safety is Dose and Context Dependent
Scientific Perspective: The massive 41-trial meta-analysis from 2026 confirms no significant increase in major adverse cardiovascular events (MACE) when TRT is used to treat confirmed hypogonadism. Landmark data demonstrates that historical cardiac concerns were largely artifacts of utilizing supraphysiological doses in non-hypogonadal populations, rather than true therapeutic replacement.
Is testosterone bad for your heart? The latest 2026 data says no—as long as you actually have a medical deficiency and take normal, doctor-prescribed doses. The old horror stories about heart risks usually came from people abusing high doses of steroids, not men getting proper medical treatment.
5. Standard TRT Shuts Down Fertility; Clomiphene Preserves It
Scientific Perspective: Exogenous testosterone replacement therapy reliably suppresses the hypothalamic-pituitary-gonadal (HPG) axis via negative feedback, halting endogenous spermatogenesis. For aging men wishing to preserve fertility, clomiphene citrate serves as an evidence-based alternative by blocking estrogen receptors at the pituitary level, thereby stimulating endogenous LH/FSH and preserving sperm production.
If you are taking standard testosterone injections or gels, it signals your brain to stop making its own, which can completely shut down your sperm count. If you still want to have children, ask your doctor about a medication called clomiphene instead. It tricks your brain into boosting your own natural testosterone and keeps your fertility intact
Your 5-Step Engagement Strategy
The evidence is compelling. The regulatory landscape is shifting. And the tools to take action are available today. Here is how to move from awareness to outcomes:
Step 1 — Audit your symptoms honestly. Use a validated screening tool such as the Aging Males' Symptoms (AMS) scale or the ADAM questionnaire, available through your healthcare provider or reputable online medical resources. Score your symptoms before your next appointment.
Step 2 — Book a comprehensive hormonal evaluation. Request early-morning blood tests for total testosterone, free testosterone, LH, FSH, SHBG, estradiol, and PSA. Ask for a full metabolic panel and lipid profile at the same visit. Knowledge is the starting point.
Step 3 — Have a two-way conversation about treatment options. Bring this article. Ask directly about TRT versus clomiphene citrate based on your diagnosis type, age, and family planning goals. Ask about the TRAVERSE trial data and the 2026 FDA notice. An informed patient gets better care.
Step 4 — Commit to the lifestyle foundation. Begin or intensify resistance training — even two sessions per week has documented hormonal benefits. Prioritize sleep quality. Eliminate processed foods and excess alcohol. These are not optional "nice-to-haves"; they are the scaffolding that makes hormonal treatment work.
Step 5 — Stay engaged with the monitoring process. Schedule your follow-up appointment at the time of your first prescription. Mark calendar reminders for your 6-week and 6-month check-ins. Share symptom changes — both positive and negative — with your clinician. Effective TRT is a partnership, not a one-time transaction.
TRT Side Effects
acne,
fluid retention,
erythrocytosis,
gynecomastia,
infertility,
edema,
Clinician’s Perspective
From a modern internal medicine and preventive health perspective, testosterone deficiency should no longer be viewed solely through the narrow lens of sexual dysfunction. The emerging evidence from 2024–2026 strongly suggests that hypogonadism is deeply interconnected with metabolic syndrome, sarcopenia, insulin resistance, osteoporosis, sleep disorders, and cardiovascular health. In clinical practice, many men presenting with fatigue, central obesity, reduced exercise tolerance, low mood, and declining vitality are often experiencing a broader endocrine-metabolic dysfunction rather than “normal aging” alone.
What is equally important is the shift in how clinicians approach Testosterone Replacement Therapy (TRT). Historically, fear surrounding prostate cancer and cardiovascular risk led to widespread undertreatment of symptomatic men. However, contemporary data — including TRAVERSE-related analyses and large meta-analyses — indicate that physiologic testosterone replacement in appropriately screened hypogonadal men appears considerably safer than once believed (García-Becerra et al., 2026; Zitzmann et al., 2026). The key phrase is appropriately screened. Good medicine requires confirming biochemical deficiency, identifying reversible causes, evaluating fertility goals, assessing sleep apnea risk, and maintaining structured follow-up.
Clinicians should also recognize that testosterone optimization is not a standalone intervention. Resistance training, sleep quality, weight reduction, cardiometabolic risk control, and nutritional health remain foundational components of treatment success. In many patients, TRT acts less like a “performance enhancer” and more like a metabolic restoration therapy that helps patients regain the physiological capacity to engage in healthier behaviors.
The most responsible clinical approach is neither indiscriminate prescribing nor reflexive dismissal of symptoms. Instead, it is individualized, evidence-based care grounded in careful diagnosis, realistic expectations, and long-term monitoring.
Medical Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Testosterone Replacement Therapy and clomiphene citrate are prescription medications with potential risks and side effects. Always consult a qualified healthcare professional before initiating any hormonal therapy. Never disregard or delay seeking professional medical advice based on information read in this article.
Related Articles
Hormone Therapy and Sarcopenia: Testosterone, HGH, and Muscle Mass | DR T S DIDWAL
How to Prevent Sarcopenia: Fight Age-Related Muscle Loss and Stay Strong | DR T S DIDWAL
Best Supplements for Sarcopenia: Vitamin D, Creatine, and HMB Explained | DR T S DIDWAL
Testosterone Therapy for Sarcopenia: A Comprehensive Evidence-Based Guide | DR T S DIDWAL
References
Câmara, L. C. (2025). Evidence-based prescription strategies for clomiphene citrate in male hypogonadism and fertility management. Asian Journal of Research in Medical and Pharmaceutical Sciences, 14(1), 1–7. https://doi.org/10.9734/ajrimps/2025/v14i1289
Cruickshank, M., Hudson, J., Hernández, R., Aceves-Martins, M., Quinton, R., Gillies, K., Aucott, L. S., Kennedy, C., Manson, P., Oliver, N., Wu, F., Bhattacharya, S., Dhillo, W. S., Jayasena, C. N., & Brazzelli, M. (2024). The effects and safety of testosterone replacement therapy for men with hypogonadism: The TestES evidence synthesis and economic evaluation. Health Technology Assessment, 28(43), 1–210. https://doi.org/10.3310/JRYT3981
de Silva, N. L., Papanikolaou, N., Grossmann, M., Antonio, L., Quinton, R., Anawalt, B. D., & Jayasena, C. N. (2024). Male hypogonadism: Pathogenesis, diagnosis, and management. The Lancet Diabetes & Endocrinology, 12(10), 761–774. https://doi.org/10.1016/S2213-8587(24)00199-2
Food and Drug Administration. (2026, April 20). Potential new indication for testosterone replacement therapy [Notice]. Federal Register, 91(21002–21003). Docket No. FDA-2025-N-6743. https://www.federalregister.gov/documents/2026/04/20/2026-07615/potential-new-indication-for-testosterone-replacement-therapy
García-Becerra, C. A., Arias-Gallardo, M. I., Juárez-García, J. E., et al. (2026). Cardiovascular and prostate cancer risk associated to testosterone replacement therapy — a systematic review and meta-analysis of 41 randomized controlled trials. International Journal of Impotence Research. https://doi.org/10.1038/s41443-026-01237-4
Zitzmann, M. (2026). Functional testosterone deficiency in aging men. Maturitas. Advance online publication. https://doi.org/10.1016/j.maturitas.2026.01.012
Goulis, D. (2025). Hypogonadism and testosterone replacement: What did we learn from the recent studies? Maturitas, 199, 108369. https://doi.org/10.1016/j.maturitas.2025.108369
Pechersky, A. V. (2025). The influence of partial androgen deficiency in aging men (PADAM) on the development of benign prostatic hyperplasia and prostate cancer. American Research Journal of Urology, 3(1), 1–16. https://www.arjonline.org/papers/arju/v3-i1/1.pdf
Szarpak, L., Al-Jeabory, M., Pecold, J., & Maslyk, M. (2026). Testosterone replacement therapy in older men: Skeletal outcomes and fracture risk. The Aging Male, 29(1). https://doi.org/10.1080/13685538.2026.2655544
Zitzmann, M., Rastrelli, G., Murray, R. D., et al. (2026). Cardiovascular safety of testosterone therapy — Insights from the TRAVERSE trial and beyond: A position statement of the European Expert Panel for Testosterone Research. Andrology, 14, 294–302. https://doi.org/10.1111/andr.70062