Can Resistance Training Reverse Diabetes? The Muscle–mTOR Link
Resistance training activates mTOR to rebuild muscle, reverse sarcopenia, and improve insulin resistance—making it a powerful therapy for diabetes and aging.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/11/202611 min read
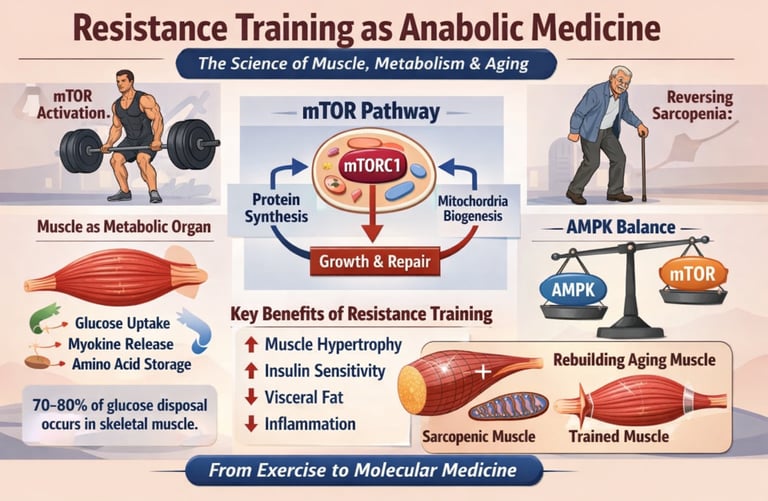
Resistance training acts as anabolic medicine by activating the mechanistic target of rapamycin (mTOR), increasing muscle protein synthesis, and reversing sarcopenia. It improves insulin sensitivity, reduces visceral fat, and enhances metabolic health—making it a cornerstone therapy for aging, type 2 diabetes, and cardiometabolic disease.
What if the most powerful therapy for insulin resistance, sarcopenia, and metabolic aging was not a drug—but a biological signal your body is evolutionarily designed to respond to?
Resistance training is now increasingly recognized not simply as exercise, but as anabolic medicine—a targeted intervention that activates mTOR signaling, enhances muscle protein synthesis, and restores metabolic function at the cellular level. This paradigm shift reframes skeletal muscle as a metabolic and endocrine organ, central to glucose homeostasis, mitochondrial health, and systemic inflammation (Zhao, 2025).
Following a carbohydrate-rich meal, approximately 70–80% of glucose disposal occurs in skeletal muscle, making it the dominant regulator of glycemic control and a key determinant of type 2 diabetes risk. As muscle mass declines with aging and inactivity, this metabolic reservoir diminishes—driving insulin resistance, ectopic fat accumulation, and progressive metabolic dysfunction. This process underlies sarcopenia, a condition now strongly associated with frailty, hospitalization, and increased mortality risk (Govindasamy et al., 2025).
At the molecular level, resistance training activates the mechanistic target of rapamycin complex 1 (mTORC1)—the master regulator of cellular anabolism. This pathway integrates mechanical tension, amino acid availability (particularly leucine), and hormonal signals to stimulate muscle hypertrophy and functional recovery (Behringer et al., 2025). Emerging evidence further demonstrates that resistance training enhances mitochondrial capacity, challenging the traditional view that these adaptations are exclusive to aerobic exercise (Jerez-Martínez & Romero-Arenas, 2026).
Simultaneously, resistance training restores balance within the AMPK–mTOR axis, improving metabolic flexibility and insulin sensitivity in aging muscle (Mingzheng & You, 2025).
This is not simply an exercise—it is precision metabolic therapy grounded in molecular physiology.
Clinical pearls
1. The "Glucose Sponge" Effect
Scientific Perspective: Skeletal muscle is responsible for approximately 80% of postprandial glucose clearance via GLUT4 translocation. Resistance training increases both muscle mass (storage capacity) and insulin sensitivity (efficiency of the "sponge").
Think of your muscles as a storage tank for the sugar in your blood. When you lift weights, you aren't just getting stronger; you are building a bigger, more efficient 'sponge' that soaks up blood sugar, protecting your heart and your pancreas."
2. Overcoming Anabolic Resistance
Scientific Perspective: Ageing is characterized by a blunted MPS (Muscle Protein Synthesis) response to amino acids. To "breach" the leucine threshold and activate mTORC1 in older tissue, higher bolus doses of protein ( 0.4–0.5g/kg per meal) are required compared to younger cohorts.
"As we age, our muscles become 'hard of hearing' to the signal to grow. To get the message through, we need to 'speak louder' by eating more high-quality protein at each meal—especially right after a workout."
3. The Myokine "Pharmacy"
Scientific Perspective: Contracting skeletal muscle acts as an endocrine organ, secreting myokines like IL-6 (which has anti-inflammatory systemic effects) and Irisin (which promotes "browning" of white adipose tissue).
"Your muscles are actually a natural pharmacy. Every time you lift weights, your body 'dispenses' specialized chemicals that travel through your bloodstream to fight inflammation, improve your mood, and help burn stubborn fat."
4. Quality Over "Vanity" (The 1RM Myth)
Scientific Perspective: Hypertrophy can be achieved across a wide spectrum of loading (30%–85% 1RM) provided sets are performed to near-muscular failure. This allows for sarcopenia reversal even in patients with joint limitations that preclude heavy lifting.
"You don't need to lift like a powerlifter to see results. Science shows that using moderate weights—as long as the last few repetitions feel genuinely challenging—is just as effective for building life-saving muscle as lifting heavy iron."
5. The Metformin-mTOR Conflict
Scientific Perspective: Metformin activates AMPK, which can antagonistically inhibit the mTORC1 pathway. While Metformin is vital for glycemic control, clinicians should note it may slightly attenuate the hypertrophic "gains" from resistance training in some populations.
"If you are taking Metformin for blood sugar, it's doing a great job, but it might slightly 'quiet down' your muscle growth signals. Don't stop your medicine, but realize that being extra consistent with your protein and lifting is even more important for you."
6. Sarcopenia as "Metabolic Poverty"
Scientific Perspective: Sarcopenia is not merely a loss of strength; it is a state of "metabolic frailty" where the body loses its primary amino acid reservoir. This reservoir is critical for survival during acute illness or trauma to support immune function and tissue repair.
"Think of your muscle as your body’s 'emergency savings account.' If you get sick or injured, your body draws from that account to heal. Building muscle now ensures you have the 'metabolic wealth' to bounce back quickly if life throws you a curveball."
Resistance Training as Anabolic Medicine: How mTOR Builds Muscle, Reverses Sarcopenia, and Improves Metabolic Health
Your Muscles Are Not Just for Movement — They Are a Metabolic Organ
Why Skeletal Muscle Is Central to Metabolic Health
Skeletal muscle makes up nearly 40% of total body mass, making it the largest organ system in the human body. However, muscle is far more than a mechanical structure—it is a metabolic and endocrine organ that regulates glucose homeostasis, amino acid storage, and systemic inflammation.
After a carbohydrate-rich meal, up to 70–80% of glucose is taken up by skeletal muscle, positioning it as the primary regulator of blood sugar control and insulin sensitivity. Well-trained muscle functions as a metabolic sink, rapidly clearing glucose and reducing pancreatic stress.
By contrast, reduced muscle mass—a hallmark of sarcopenia—leads to prolonged hyperglycemia, increased insulin resistance, and higher risk of type 2 diabetes and cardiometabolic disease.
Clinical Insight:
Loss of skeletal muscle is strongly associated with frailty, metabolic dysfunction, and increased all-cause mortality. Muscle is not optional—it is metabolic infrastructure.
The Science of Muscle Hypertrophy: What Happens When You Lift Weights
Three Mechanisms of Muscle Growth (Behringer et al., 2025).
Muscle hypertrophy occurs during recovery, not during exercise itself. It is driven by three key pathways:
Mechanical Tension: The primary driver. Load-induced mechanotransduction activates signaling pathways (e.g., focal adhesion kinase), stimulating muscle fiber growth and satellite cell activation.
Metabolic Stress: Accumulation of lactate and reactive oxygen species enhances anabolic signaling and cellular swelling.
Muscle Damage and Repair: Eccentric contractions create microtrauma, triggering inflammation and regeneration.
Emerging research shows resistance training also enhances mitochondrial function, challenging the traditional view that only aerobic exercise improves cellular energetics.
mTOR: The Master Regulator of Muscle Growth and Metabolism
Understanding the mechanistic target of rapamycin
At the center of muscle hypertrophy lies mTORC1, the key regulator of protein synthesis and cellular growth. When activated, it increases ribosomal biogenesis and accelerates muscle repair and growth.
What Activates mTOR?
Mechanical load (resistance training)
Amino acids (especially leucine)
Hormonal signals (insulin, IGF-1)
This explains why combining resistance training + protein intake produces maximal anabolic effects.
mTOR vs AMPK: The Metabolic Switch
mTOR operates in balance with AMPK, the cellular energy sensor:
Resistance training → mTOR activation → muscle growth
Aerobic exercise → AMPK activation → Energy efficiency
Optimal metabolic health requires both pathways, but only resistance training drives structural muscle adaptation.
Clinical Insight:
Protein intake of 25–40 g per meal (with ~2.5–3 g leucine) maximizes mTOR activation and muscle protein synthesis.
Sarcopenia: The Hidden Driver of Aging and Metabolic Disease
What Is Sarcopenia?
Sarcopenia is defined by progressive loss of muscle mass, strength, and function. It affects:
10–27% of older adults
50% of institutionalized individuals
It is a major predictor of frailty, disability, hospitalization, and mortality.
Key Mechanisms
Increased protein breakdown (ubiquitin-proteasome pathway)
Elevated myostatin (inhibits muscle growth)
Chronic inflammation (“inflammaging”)
Mitochondrial dysfunction
Anabolic Resistance
Older muscle shows reduced responsiveness to protein and exercise due to impaired mTOR signaling and hormonal decline.
Resistance Training Reverses Sarcopenia and Insulin Resistance
Mechanistic Benefits
Resistance training:
Restores mTOR signaling
Increases muscle protein synthesis
Improves neuromuscular function
Enhances mitochondrial capacity
Reduces systemic inflammation
Metabolic Benefits
Improves insulin sensitivity
Reduces visceral fat
Enhances glucose uptake
Supports type 2 diabetes management
Clinical Bottom Line:
Resistance training is not optional—it is a primary therapy for metabolic disease and aging.
How to Build Muscle and Reverse Sarcopenia: Evidence-Based Training Guide
Training Prescription
Intensity: 60–85% 1RM (8–12 reps)
Volume: 2–4 sets per exercise
Frequency: 2–3 sessions per week
Progression: Gradually increase load, reps, or volume
Progressive Overload
The most critical principle for long-term adaptation—without it, muscle growth plateaus.
For Older Adults
Start with low intensity
Focus on technique and balance
Progress gradually
Prioritize consistency over intensity
“Prescribing Resistance Training for Sarcopenia”
Step 1: Assess (grip strength, gait speed)
Step 2: Start (2x/week, 60% 1RM)
Step 3: Protein target (1.6 g/kg)
Step 4: Progression timeline
Nutrition for Muscle Growth: Protein and Leucine Matter
Optimal Protein Intake (Chen et al 2025)
1.2–1.6 g/kg/day (general health)
1.6–2.0 g/kg/day (muscle gain, aging)
Leucine Threshold
~2.5–3 g per meal required for maximal mTOR activation
Achieved via 25–40 g high-quality protein
Protein Timing
Even distribution across 3–4 meals enhances muscle protein synthesis throughout the day.
Common Myths About Muscle and Aging
Myth 1: Older adults cannot build muscle → FALSE
Myth 2: Light weights are enough → PARTIALLY TRUE
Myth 3: Protein alone reverses sarcopenia → FALSE
Frequently Asked Questions
Q1. How quickly can I expect to see results from resistance training?
Initial improvements in strength typically appear within 2–4 weeks of beginning a consistent program, largely due to neurological adaptations (your nervous system learning to recruit muscle fibers more efficiently). Measurable changes in muscle size generally require 6–12 weeks of progressive training. In older adults, functional improvements such as better balance, easier stair climbing, and reduced fatigue often precede visible changes in body composition.
Q2. I am over 65 — is it safe for me to start resistance training?
Yes, and it is one of the most evidence-supported interventions available to you at this life stage. Multiple clinical trials have demonstrated that resistance training is safe and beneficial for adults in their 70s, 80s, and even 90s. Begin with bodyweight exercises or low-resistance bands, prioritize technique over load, and consider working with a physiotherapist or certified trainer initially. Your doctor can help identify any specific considerations relevant to your health history.
Q3. Do I need to take protein supplements, or can I get enough from food?
Whole food sources of protein — meat, fish, eggs, dairy, legumes — are entirely sufficient for most people. Protein supplements (whey, casein, pea protein) are a convenient way to increase intake but are not superior to food sources with equivalent protein and leucine content. If meeting your protein targets through diet alone is difficult (particularly for older adults or those with reduced appetite), a protein supplement can be a practical addition.
Q4. What is the difference between resistance training and aerobic exercise for metabolic health?
Both are beneficial and mechanistically complementary. Aerobic exercise primarily improves cardiovascular fitness, mitochondrial density in muscle, and fat oxidation. Resistance training builds muscle mass, improves insulin sensitivity through glucose uptake in muscle, strengthens bone, and elevates resting metabolic rate. Current evidence supports the combination of both — with resistance training being the primary driver of structural metabolic improvement, particularly in the context of sarcopenia and insulin resistance.
Q5. Can resistance training help if I have type 2 diabetes?
Yes — meaningfully so. Resistance training improves insulin sensitivity by increasing the mass and metabolic activity of skeletal muscle, which is the body's primary site of glucose disposal. In some clinical studies, the glycemic benefits of resistance training are comparable to those of first-line medications. It is important to discuss exercise planning with your diabetes care team, as blood glucose monitoring and medication adjustments may be warranted.
Q6. I have heard that sarcopenia is inevitable with aging — is that true?
Sarcopenia is common with aging, but it is not inevitable — and it is substantially reversible. The rate of muscle loss accelerates after age 60, but this trajectory can be slowed, halted, or reversed with consistent resistance training and adequate protein intake. Studies have documented significant muscle mass and strength gains in adults in their 70s and 80s through structured exercise programs. Age is not a barrier to adaptation; it is simply a context that requires appropriate programming.
Q7. How does nutrition interact with resistance training for muscle building?
Nutrition and resistance training are synergistic — neither is fully effective without the other. Resistance training creates an anabolic environment (via mTOR activation and satellite cell recruitment), while protein provides the amino acid building blocks that are assembled into new muscle tissue. Carbohydrates support training performance and glycogen replenishment. Total caloric adequacy matters: muscle building is difficult in a significant caloric deficit. Distributing protein evenly across meals — with at least 2.5–3g of leucine per serving — appears to maximize the anabolic response across the day.
To Summarize
We are entering a paradigm shift in medicine. Resistance training is no longer a lifestyle recommendation—it is a first-line therapeutic intervention for cardiometabolic disease, aging, and functional decline. The evidence is no longer emerging; it is established.
Skeletal muscle is not passive tissue—it is metabolic infrastructure. It regulates glucose disposal, insulin sensitivity, and systemic inflammation, making it central to the pathophysiology of conditions like type 2 diabetes and metabolic syndrome.
At the molecular level, resistance training activates the mechanistic target of rapamycin (mTORC1)—the master regulator of anabolism, protein synthesis, and muscle repair. This is not theoretical biology; it is a targetable clinical pathway.
Sarcopenia is not inevitable—it is reversible. Age-related muscle loss reflects anabolic resistance, mitochondrial dysfunction, and chronic inflammation—all of which are directly improved with structured resistance training.
The clinical implications are profound. Resistance training:
Improves insulin sensitivity comparable to pharmacotherapy in some populations
Reduces visceral adiposity and systemic inflammation
Enhances functional independence and reduces fall risk
The synergy with nutrition is critical. Adequate protein intake (1.2–2.0 g/kg/day) with sufficient leucine optimizes mTOR activation and muscle protein synthesis, transforming exercise into a true anabolic intervention.
Importantly, not all exercise is equal. While aerobic training improves cardiovascular fitness, resistance training uniquely drives structural metabolic change—muscle mass, strength, and resting metabolic rate.
A critical nuance for clinicians: therapies like metformin may partially blunt hypertrophic signaling via AMPK activation—highlighting the need for integrated, personalized treatment strategies.
The prescription is clear: progressive resistance training, performed 2–3 times per week, should be considered standard of care in aging, diabetes, and metabolic disease.
The conclusion is unavoidable: resistance training is not fitness—it is molecular medicine, functional longevity therapy, and metabolic rehabilitation combined.
Author’s Note
As a physician working at the intersection of metabolism, aging, and exercise physiology, I have witnessed a profound gap between what modern science understands and what is routinely prescribed in clinical practice. While pharmacotherapy continues to evolve, one of the most powerful interventions available to us—resistance training—remains underutilized, underprescribed, and often misunderstood.
This article was written to help bridge that gap.
The intent is not to position exercise in opposition to medication, but to reframe it within the same clinical hierarchy—as a targeted, dose-dependent intervention with measurable biological effects. The pathways discussed here, particularly the role of the mechanistic target of rapamycin (mTOR), are not abstract concepts confined to laboratories; they represent real, modifiable processes that influence how patients age, respond to disease, and maintain independence.
For clinicians, the message is straightforward: resistance training deserves the same precision in prescription as any drug—defined by intensity, frequency, progression, and patient context.
For patients, the message is equally important: building and preserving muscle is not about aesthetics. It is about metabolic health, resilience, and longevity.
The growing body of evidence supporting resistance training as a cornerstone therapy in conditions such as type 2 diabetes, sarcopenia, and metabolic dysfunction is compelling—and it continues to strengthen. As this field evolves, so too must our approach to care.
If this article shifts even a small part of that perspective—from viewing exercise as optional to recognizing it as essential—then it has served its purpose.
Medical Disclaimer
The information in this article, including the research findings, is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Before starting a resistance exercise program, you must consult with a qualified healthcare professional, especially if you have existing health conditions (such as cardiovascular disease, uncontrolled hypertension, or advanced metabolic disease). Exercise carries inherent risks, and you assume full responsibility for your actions. This article does not establish a doctor-patient relationship.
Related Articles
How Exercise Reprograms Your Hormones to Burn Fat, Lower Cortisol & Boost Metabolism | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
No Time to Train? Science-Backed Workouts That Deliver | DR T S DIDWAL
References
Behringer, M., Heinrich, C., & Franz, A. (2025). Anabolic signals and muscle hypertrophy: Significance for strength training in sports medicine. Sports Orthopaedics and Traumatology, 41(1), 9–18. https://doi.org/10.1016/j.orthtr.2025.01.002
Chen, W. (2025). Nutritional interventions in muscle hypertrophy research: A scientometric analysis within the context of resistance training (1992–2025). Journal of Health, Population and Nutrition, 44, 272. https://doi.org/10.1186/s41043-025-01031-w
Govindasamy, K., Rao, C. R., Chandrasekaran, B., Parpa, K., & Granacher, U. (2025). Effects of resistance training on sarcopenia risk among healthy older adults: A scoping review of physiological mechanisms. Life, 15(5), 688. https://doi.org/10.3390/life15050688
Jerez-Martínez, A., & Romero-Arenas, S. (2026). Impact of Hypertrophy-Focused Resistance Training on Mitochondrial Capacity: A New Perspective Through Near-Infrared Spectroscopy. Research Quarterly for Exercise and Sport, 97(1), 60–67. https://doi.org/10.1080/02701367.2025.2542816
Mingzheng, X., & You, W. (2025). AMPK/mTOR balance during exercise: Implications for insulin resistance in aging muscle. Molecular and Cellular Biochemistry, 480, 5941–5953. https://doi.org/10.1007/s11010-025-05362-4
Sharma, S., Sharma, M., Tripathi, D., et al. (2025). Impact of resistance exercise variants on sarcopenia: A scoping review. Discover Public Health, 22, 474. https://doi.org/10.1186/s12982-025-00866-2
Zhao, Y.-C. (2025). Dual roles of mTOR in skeletal muscle adaptation: Coordinating hypertrophic and mitochondrial biogenesis pathways for exercise-induced chronic disease management. Frontiers in Medicine, 12, 1635219. https://doi.org/10.3389/fmed.2025.1635219