Think Insulin Controls Weight? The Liver Is the Real Metabolic Powerhouse
Learn why your liver controls blood sugar, fat storage & heart risk. Discover how selective insulin resistance drives diabetes & fatty liver — plus science-backed fixes.
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/9/202629 min read
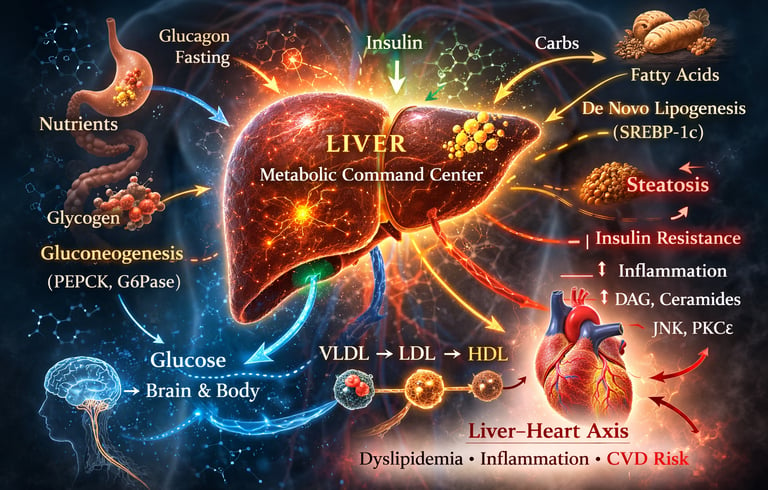
The liver is your body's metabolic control center. It decides how much sugar to release into your blood, whether to store or burn fat, and how to package cholesterol. When the liver becomes insulin resistant, it overproduces both glucose and fat — driving high blood sugar, fatty liver, and heart disease.
Key Takeaways for Your Liver Health
1. Your liver runs your metabolism, not your pancreas.
Before food even reaches your muscles or brain, your liver decides if those calories become energy, stored sugar, or fat. When the liver gets overwhelmed, blood sugar and weight problems start — often years before you notice.
2. High fasting blood sugar is usually a liver problem.
If you wake up with high glucose even when you eat well, your liver is likely making extra sugar overnight. This is called “hepatic glucose overproduction” and it’s one of the earliest signs of insulin resistance.
3. You can have high blood sugar and a fatty liver at the same time.
In a sick liver, insulin stops turning off sugar production but keeps turning on fat production. Doctors call this “selective insulin resistance.” It explains why type 2 diabetes, high triglycerides, and fatty liver often show up together.
4. Fatty liver disease has zero symptoms — until it’s serious.
Your liver has no pain nerves. Most people with MASLD (fatty liver) feel fine, even with early scarring. The only way to catch it early is with blood tests like FIB-4 or a FibroScan. Don’t wait for symptoms.
5. Your liver health is heart health.
A fatty, inflamed liver sends out proteins and fats that directly damage your arteries and heart muscle. MASLD raises your risk of heart attack, heart failure, and stroke — even if your cholesterol looks “okay.”
6. Exercise helps your liver even if you don’t lose weight.
Just 150 minutes of brisk walking per week cuts liver fat and calms inflammation. Resistance training helps too. Your liver responds to movement in weeks, long before the scale moves. This is one of the fastest ways to improve insulin sensitivity.
7. Normal liver enzymes don’t guarantee a healthy liver.
ALT and AST can be normal even with significant liver fat or early fibrosis. If you have diabetes, belly fat, or high triglycerides, ask your doctor about a FIB-4 score or liver imaging. Standard blood work misses a lot.
8. You can reverse fatty liver in early stages.
Simple fat buildup and even mild inflammation are often reversible with Mediterranean-style eating, cutting sugary drinks, reducing alcohol, and daily activity. The key is catching it before scarring becomes advanced. Your liver can heal if you give it the chance.
Bottom line: Think of your liver as the CEO of your metabolism. When the CEO is stressed, the whole company struggles — blood sugar, weight, cholesterol, and heart risk all go up. The good news? Small, consistent changes protect the CEO and improve everything downstream.Introduction
Most people blame their pancreas when blood sugar goes haywire, or their willpower when the scale won't budge. But cutting-edge research is pointing somewhere else entirely: your liver.
Long before insulin even reaches your muscles or your brain processes hunger signals, your liver has already decided what to do with every calorie you consume. It stores. It burns. It builds fat. It releases sugar. It talks to your heart. And when it breaks down — often silently, with zero symptoms — it can trigger a cascade of metabolic disease that looks like a dozen different problems but traces back to one source.
In this article, you'll learn:
How your liver controls blood sugar, body fat, and energy — moment to moment
What "selective insulin resistance" means and why it causes both high blood sugar and a fatty liver at the same time
The science-backed link between liver disease and heart disease (the liver–heart axis)
How to detect early liver dysfunction without a biopsy
Evidence-based strategies to protect and restore liver metabolic function
What Your Liver Actually Does Every Day
Your liver is the largest solid organ in your body and by far the most metabolically active. Weighing roughly 1.5 kg in adults, it performs over 500 distinct functions, but its role as a metabolic command center is what most people overlook.
Every single time you eat, fast, exercise, or experience stress, your liver responds in real time. It processes nutrients arriving from your digestive system through the portal circulation — a direct pipeline from gut to liver — before they reach any other organ. Glucose, fatty acids, amino acids, and hormones all pass through this gateway first.
What does the liver decide?
How much blood glucose to release or absorb
Whether to store fat or export it
How to partition amino acids between protein synthesis and fuel
Which hormones and signaling proteins to secrete back into the bloodstream
As Zhang and colleagues described in a 2019 review in Frontiers in Endocrinology, the liver integrates insulin, glucagon, cortisol, inflammatory mediators, and neural signals simultaneously — adjusting its output within minutes, not hours.
This is not a passive processing plant. It is an active, decision-making organ. And understanding how those decisions go wrong is the key to understanding modern metabolic disease.
How the Liver Controls Blood Sugar
Blood glucose regulation is one of the liver's most critical jobs. The brain runs almost entirely on glucose and cannot tolerate significant swings in supply, so the liver acts as a buffer, constantly adjusting output based on feeding and fasting signals.
Glycogenolysis: The First-Line Glucose Reserve
When you stop eating — whether for a few hours of fasting or overnight sleep — blood glucose begins to fall. The liver's first response is glycogenolysis: the rapid breakdown of stored glycogen (a branched polymer of glucose) back into free glucose, which is released into the bloodstream.
The liver can store roughly 100 grams of glycogen, enough to supply glucose for approximately 6–12 hours of fasting. After that, the reserve is depleted, the liver switches to a more energy-intensive backup system.
Gluconeogenesis: Manufacturing Glucose From Scratch
Gluconeogenesis is the liver's "night shift factory" — the synthesis of entirely new glucose molecules from non-carbohydrate precursors:
Lactate (from muscle activity)
Alanine and other amino acids (from muscle protein)
Glycerol (from fat breakdown)
This process is controlled by a network of transcription factors and enzymes, including FOXO1, PGC-1α, PEPCK, and G6Pase. Under normal conditions, insulin suppresses gluconeogenesis by excluding FOXO1 from the cell nucleus — essentially turning off the glucose factory when you've just eaten and blood sugar is already elevated.
The Clinical Problem: In type 2 diabetes and insulin resistance, this suppression fails. The liver continues manufacturing glucose even when blood sugar is already high — a primary driver of fasting hyperglycemia. Many people wake up with elevated blood glucose not because they ate poorly the night before, but because their liver overproduced sugar while they slept.
Why is my fasting blood sugar high even when I eat well? Elevated fasting glucose is often driven by hepatic gluconeogenesis. When the liver is insulin-resistant, it continues producing sugar overnight despite elevated blood glucose levels. This is called "hepatic glucose overproduction" and is a core feature of type 2 diabetes — independent of dietary carbohydrate intake.
The Liver as a Fat Factory: De Novo Lipogenesis
When you eat more carbohydrates than your body can immediately use or store as glycogen, the liver converts the excess into fat. This process is called de novo lipogenesis (DNL) — literally, "new fat creation."
The fat produced through DNL is either:
Stored in the liver → leading to hepatic steatosis (fatty liver)
Packaged into VLDL particles → exported into the bloodstream
In a metabolically healthy person, this system acts as a safety valve — preventing dangerous spikes in blood sugar by converting excess glucose into a storable form.
When the Safety Valve Breaks
In insulin-resistant states, the liver loses its ability to properly regulate VLDL secretion and LDL receptor activity. According to a 2026 review by Winterfeldt and Siddiqi in the journal Livers, this breakdown produces what is called the atherogenic lipid triad:
High triglycerides (VLDL overproduction)
Low HDL cholesterol (impaired reverse cholesterol transport)
Small, dense LDL particles (more dangerous than large, fluffy LDL)
This lipid profile dramatically increases cardiovascular risk — not because of dietary fat intake, but because of a liver that has lost its metabolic regulation.
Key proteins in this process include ApoB-100 (the structural backbone of VLDL and LDL) and PCSK9 (which controls LDL receptor availability). Both are now recognized as major therapeutic targets in cardiometabolic disease.
Selective Insulin Resistance: The Paradox That Explains Everything
Here is one of the most important — and counterintuitive — concepts in modern metabolic medicine:
In a diseased liver, insulin resistance is selective, not total.
You might expect that if the liver "ignores" insulin, everything would shut down. But the reality is more complicated and more dangerous. Research by Truong and Lee published in the Diabetes & Metabolism Journal in 2025 revealed that in metabolic liver disease, insulin signaling breaks down in one branch while remaining active in another:
Pathway Function Status in Diseased Liver AKT → FOXO1 Suppresses gluconeogenesis Impaired — liver keeps making glucose SREBP-1c Activates fat synthesis (lipogenesis) Preserved — liver keeps making fat
The result is a metabolic "short circuit" that produces both problems simultaneously:
The glucose-suppression signal is broken → fasting hyperglycemia
The fat-production signal is intact → hepatic steatosis and dyslipidemia
This is why patients with type 2 diabetes and fatty liver disease so often have elevated fasting glucose and elevated triglycerides and liver fat — all at the same time. Treating only one without the other rarely succeeds.
What Causes This Short Circuit?
Truong and Lee identify two primary molecular culprits:
Lipotoxicity: Excess accumulation of diacylglycerols (DAGs) and ceramides — toxic fat metabolites — inside liver cells. These molecules directly interfere with the insulin signaling cascade.
ER Stress: When the liver is overwhelmed with fat, the endoplasmic reticulum (the cell's protein-processing machinery) becomes overloaded, triggering stress responses that further impair insulin signaling.
Why this matters for treatment: This dual-pathway dysfunction explains why GLP-1 receptor agonists (like semaglutide) and SGLT2 inhibitors have shown such promise in MASLD — they address the molecular loop driving both fat accumulation and glucose overproduction simultaneously.
MASLD: The Evolving Science of Fatty Liver Disease
The medical community recently renamed Non-Alcoholic Fatty Liver Disease (NAFLD) to Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). This isn't just semantics — it reflects a deeper understanding that fatty liver is a systemic metabolic disorder, not simply a consequence of weight or alcohol.
Who Gets MASLD?
MASLD is now the most common chronic liver disease worldwide, affecting an estimated 25–38% of the global population. Risk factors include:
Obesity, especially visceral (abdominal) fat accumulation
Type 2 diabetes and insulin resistance
Metabolic syndrome (elevated glucose, triglycerides, blood pressure; low HDL)
High intake of refined carbohydrates and ultra-processed foods
Physical inactivity
Genetic variants, particularly in the PNPLA3 and TM6SF2 genes
Gut microbiome dysbiosis
Sleep-disordered breathing (sleep apnea)
Critically, MASLD can occur in people with normal BMI — particularly those with high visceral fat or genetic predisposition. BMI alone is an inadequate screening tool.
A 2026 review in Nature Medicine by Rinella, Sanyal, Loomba, and colleagues emphasized that MASLD management in the context of obesity must include liver risk stratification — not just weight-focused treatment targets.
How MASLD Progresses
MASLD progresses through a spectrum:
Stage 1: Simple Steatosis — Fat accumulates in liver cells. Often silent, reversible with lifestyle change.
Stage 2: MASH (Metabolic Dysfunction-Associated Steatohepatitis) — Inflammation and hepatocyte injury develop, driven by oxidative stress, lipid peroxidation, mitochondrial dysfunction, and inflammatory cytokine release (from Kupffer cells and adipose-derived macrophages).
Stage 3: Fibrosis — Stellate cell activation triggers scar tissue formation. Progressive and potentially irreversible.
Stage 4: Cirrhosis — Extensive scarring and liver architectural distortion. The risk of liver failure and hepatocellular carcinoma increases dramatically.
The critical clinical point: It is fibrosis stage — not the amount of fat present — that most strongly predicts liver-related and all-cause mortality. Simple fat accumulation is dangerous mainly because of where it can lead.
Can you feel a fatty liver? No. The liver has no pain-sensing nerve fibers. Most people with MASLD, including those with significant fibrosis, have no symptoms. This is why proactive screening with blood tests and imaging is essential — the window of reversibility closes silently.
The Liver's Energy Crisis: Mitochondrial Dysfunction in MASLD
Modern MASLD research increasingly recognizes mitochondria as central players in disease progression. As liver fat accumulates, hepatocyte mitochondria become overloaded with fatty acids, disrupting normal energy production and metabolic regulation.
Mitochondrial Dysfunction: Excess lipid accumulation impairs mitochondrial efficiency, reducing ATP production and compromising the liver's ability to maintain metabolic homeostasis.
Reactive Oxygen Species (ROS) Generation: Overloaded mitochondria produce excessive ROS, which damage cellular proteins, lipids, and DNA. This oxidative stress promotes inflammation and hepatocyte injury.
Impaired β-Oxidation: Normally, mitochondria burn fatty acids through β-oxidation. In MASLD, this process becomes inefficient, causing further lipid accumulation and worsening hepatic steatosis.
Mitophagy Failure: Mitophagy is the cellular quality-control process that removes damaged mitochondria. Impaired mitophagy allows dysfunctional mitochondria to accumulate, amplifying oxidative stress and metabolic dysfunction.
Together, mitochondrial dysfunction, oxidative stress, impaired fat oxidation, and defective mitophagy create a vicious cycle that drives progression from simple steatosis to MASH, fibrosis, and eventually cirrhosis. Recent evidence suggests that restoring mitochondrial health may become a major therapeutic target in future MASLD treatments.
The Liver–Heart Axis: Why Liver Health Is Heart Health
Perhaps the most important paradigm shift in cardiometabolic medicine over the past decade is the recognition that the liver and heart are in constant, bidirectional communication — and that a diseased liver actively damages the heart.
A landmark 2025 review by Capone and colleagues published in Circulation Research — one of the most respected cardiovascular journals — confirmed that MASLD is an independent risk factor for:
Coronary artery disease
Heart failure
Atrial fibrillation
Cardiac arrhythmias
"Independent" here means beyond what is explained by the associated conditions (obesity, diabetes, hypertension). The liver-heart connection operates through distinct, direct mechanisms.
Mechanism 1: Hepatokine Dysregulation
Hepatokines are proteins secreted by the liver that exert hormone-like effects on distant organs. In a healthy liver, the hepatokine profile supports metabolic balance. In MASLD, it shifts toward a pro-inflammatory, pro-atherogenic pattern.
Key hepatokines in the liver–heart axis:
Hepatokine Healthy Function Effect in MASLD FGF21 (Fibroblast Growth Factor 21) Improves insulin sensitivity; cardioprotective Secretion impaired; sensitivity lost Fetuin-A Minor regulatory role Over-secreted; causes myocardial insulin resistance and lipotoxicity Selenoprotein P Antioxidant transport Over-secreted; impairs insulin action in multiple tissues ANGPTLs Regulate triglyceride clearance Dysregulated; impairs lipoprotein lipase activity
Mechanism 2: Pro-Atherogenic Dyslipidemia
As described in Section 3, the diseased liver floods the bloodstream with VLDL particles, generating high triglycerides, low HDL, and small, dense LDL — a lipid profile that accelerates atherosclerotic plaque formation in the coronary arteries.
Mechanism 3: Systemic Inflammation
A fatty, inflamed liver releases cytokines including TNF-α, IL-6, and IL-1β into systemic circulation. These inflammatory mediators accelerate endothelial dysfunction and plaque instability — directly contributing to heart attack and stroke risk.
Mechanism 4: RAAS Dysregulation
Liver stress activates the renin-angiotensin-aldosterone system (RAAS), contributing to hypertension and adverse cardiac remodeling.
Clinical takeaway: Cardiologists, endocrinologists, and hepatologists must increasingly collaborate. Treating a heart patient without assessing liver metabolic function — and vice versa — means missing a major piece of the pathological puzzle.
The Gut–Liver Axis: A Hidden Driver of MASLD
The liver and gut are connected through the portal vein, creating a continuous communication network known as the gut–liver axis. Growing evidence suggests that disturbances in gut health can directly contribute to MASLD development and progression.
Increased Intestinal Permeability ("Leaky Gut"): Damage to the intestinal barrier allows bacterial products to enter the bloodstream and reach the liver.
Endotoxin (LPS) Exposure: Lipopolysaccharide (LPS), a component of Gram-negative bacteria, activates liver immune cells (Kupffer cells), triggering inflammation and promoting progression from steatosis to MASH.
Bile Acid Signaling: Beyond digestion, bile acids act as signaling molecules that regulate glucose, lipid, and energy metabolism.
FXR (Farnesoid X Receptor): A key bile acid receptor that suppresses hepatic fat synthesis, improves insulin sensitivity, and reduces inflammation. Impaired FXR signaling is linked to MASLD progression.
TGR5 (Takeda G Protein-Coupled Receptor 5): Another bile acid receptor that enhances energy expenditure, glucose regulation, and anti-inflammatory pathways.
Microbial Metabolites: Gut bacteria produce metabolites such as short-chain fatty acids, secondary bile acids, and trimethylamine (TMA), which can either protect or harm liver metabolism depending on microbial composition.
Together, intestinal permeability, microbial toxins, altered bile acid signaling, and dysbiosis create a pro-inflammatory environment that accelerates liver fat accumulation, insulin resistance, and fibrosis. The gut–liver axis is now considered one of the most promising therapeutic targets in MASLD research.
How Liver Dysfunction Drives Weight Gain
Weight gain is not simply a matter of "calories in, calories out" — not when the liver is metabolically dysregulated.
When hepatic metabolism breaks down, the following shifts occur:
More nutrients converted to fat. Impaired glycogen storage capacity means more dietary carbohydrate is funneled into de novo lipogenesis.
Impaired fat oxidation. Mitochondrial dysfunction in the diseased liver reduces its ability to burn fatty acids — leading to greater fat retention.
Altered appetite signaling. The liver plays a role in the peripheral metabolism of leptin and insulin — two key appetite hormones. Hepatic insulin resistance blunts satiety signaling.
VLDL overproduction. Excess triglycerides exported from the liver are deposited in adipose tissue and muscle, contributing to visceral fat accumulation.
A 2023 review in Obesity Reviews by Demir and colleagues confirmed that liver fat content is a strong predictor of cardiometabolic risk across populations — independent of total body fat mass.
This creates a vicious cycle: liver dysfunction promotes fat accumulation, and fat accumulation worsens liver dysfunction. Breaking this cycle requires targeting liver metabolic health directly — not just overall calorie restriction.
Early Detection: How to Assess Liver Metabolic Health Without a Biopsy
Liver biopsies have historically been the gold standard for diagnosing and staging liver disease. But they are invasive, expensive, and impractical for population screening. The good news: non-invasive tools are now remarkably accurate.
Blood-Based Biomarker Scores
FIB-4 Index (most widely validated):
Formula: Age × AST / (Platelet count × √ALT)
Score < 1.30 → Low probability of advanced fibrosis
Score > 2.67 → High probability of advanced fibrosis
Requires only routine blood work; widely available
NAFLD Fibrosis Score (NFS): Uses age, BMI, glucose, ALT/AST ratio, albumin, and platelet count. Well-validated for ruling out advanced fibrosis in clinical practice.
ELF Panel (Enhanced Liver Fibrosis): Measures hyaluronic acid, PIIINP, and TIMP-1 — direct markers of fibrotic activity. More sensitive than FIB-4 for detecting intermediate fibrosis.
Imaging Tools
Liver Ultrasound: Detects moderate-to-severe steatosis (>30% fat content). Widely available, inexpensive, but operator-dependent and less sensitive for mild steatosis.
FibroScan (Transient Elastography with CAP): Measures liver stiffness (fibrosis) and controlled attenuation parameter (steatosis) simultaneously. Non-invasive, reproducible, and validated across all fibrosis stages.
MRI-PDFF (Proton Density Fat Fraction): The most accurate non-invasive measure of hepatic fat content. Gold standard in research settings; increasingly available clinically.
Machine Learning–Assisted Prediction
A 2026 study by Liang and Ren in Frontiers in Physiology validated a high-performance clinical predictive model for early MASLD detection using routine metabolic variables:
BMI and waist circumference
Fasting blood glucose
ALT and AST (liver enzymes)
Triglycerides and HDL cholesterol
This machine learning model achieved strong discriminatory accuracy, offering a practical, low-cost screening tool for primary care settings — enabling early identification before irreversible fibrosis develops.
A separate 2022 genome-wide association study published in Communications Biology by van der Meer and colleagues used MRI-derived body composition measures to demonstrate clear genetic links between liver fat and cardiometabolic disease risk — highlighting the importance of genetic factors in liver health stratification.
The Molecular Mechanisms of MASLD, Insulin Resistance, and Cardiovascular Risk: A 2026 Literature Review
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) has evolved from being viewed as a localized liver condition to a recognized systemic metabolic crisis. At the center of this pathology is a destructive feedback loop between hepatic (liver) insulin resistance, lipid dysregulation, and accelerated cardiovascular disease (CVD).
This comprehensive, study-by-study scientific review breaks down the latest landmark discoveries from 2019 through 2026, mapping out the exact cellular pathways driving these diseases and how clinical medicine is adapting.
1. The Cellular "Off Switch": The AKT-FOXO1 Pathway
The Key Discovery: This study successfully mapped the AKT-FOXO1 signaling pathway, which serves as the body’s primary molecular "off switch" for gluconeogenesis (the liver's production of glucose). In a healthy state, insulin activates the enzyme AKT, which suppresses FOXO1, halting glucose output when blood sugar is already high. When this pathway fails due to insulin resistance, the switch gets stuck "on."
Clinical Relevance: This precise molecular failure explains the root cause of chronic fasting hyperglycemia (high blood sugar) seen in patients with prediabetes and Type 2 diabetes.
2. Lipotoxicity and Selective Hepatic Insulin Resistance
Study: Truong & Lee — Diabetes & Metabolism Journal (2025)
The Key Discovery: This research deeply characterized the phenomenon of selective hepatic insulin resistance. They identified that the liver can paradoxically become resistant to insulin's signals to stop making glucose, while remaining highly sensitive to insulin's signals to synthesize more fat. The team isolated three distinct molecular triggers driving this cellular chaos:
Diacylglycerols (DAGs): Toxic lipid intermediates that disrupt insulin receptor signaling.
Ceramides: Sphingolipids that accumulate in cell membranes and arrest downstream metabolism.
Endoplasmic Reticulum (ER) Stress: Intracellular structural strain caused by processing an overload of nutrients.
Clinical Relevance: This explains why insulin-resistant patients suffer from a double-whammy of simultaneous high blood sugar and skyrocketing liver fat synthesis.
3. The Atherogenic Lipid Triad, ApoB-100, and PCSK9
Study: Winterfeldt & Siddiqi — Livers (2026)
The Key Discovery: This paper defined the precise mechanics of the atherogenic lipid triad (the lethal combination of high triglycerides, low HDL, and an abundance of small, dense LDL particles) born from insulin resistance. The researchers highlighted Apolipoprotein B-100 (ApoB-100)—the structural protein found on all plaque-causing cholesterol particles—and PCSK9 (a protein that regulates LDL receptors) as the absolute premier therapeutic targets for treating lipid disorders stemming from liver dysfunction.
Clinical Relevance: It shifts the clinical focus away from merely tracking standard LDL cholesterol numbers toward tracking total ApoB particle counts, providing a far more accurate metric for cardiovascular danger in metabolic patients.
4. The Hepatokine-Mediated Liver-Heart Axis
The Key Discovery: This study confirmed that MASLD is an independent risk factor for cardiovascular disease, meaning liver fat increases heart attack risk even if cholesterol and blood pressure are kept stable. The mechanics are driven by the liver-heart axis: an inflamed, fatty liver secretes pathogenic proteins called hepatokines directly into circulation, which triggers systemic endothelial (blood vessel) inflammation and accelerates arterial plaque buildup.
Clinical Relevance: Managing MASLD is no longer just about protecting liver function; it is a critical, front-line intervention for preventing major adverse cardiovascular events (MACE).
5. Liver Fat vs. Total Body Fat: The True Driver of Risk
Genetics & Imaging Basis: van der Meer et al. — Communications Biology (2022)
Systemic Review Basis: Demir et al. — Obesity Reviews (2023)
The Key Discovery: Working in tandem, these two major publications fundamentally changed how we view body composition. van der Meer utilized large-scale Genome-Wide Association Studies (GWAS) and MRI imaging to prove a direct genetic link between localized liver fat and cardiometabolic disease. Following this, Demir et al. published a massive review confirming that ectopic liver fat is an independent predictor of cardiometabolic risk far beyond total body fat or BMI.
Clinical Relevance: An individual can have a "normal" BMI but possess high levels of hidden liver fat (often called TOFI: Thin on the Outside, Fat on the Inside), leaving them at identical cardiometabolic risk to someone living with severe obesity.
6. Machine Learning for Early MASLD Detection
The Key Discovery: Recognizing that specialized liver scans (like FibroScan or MRI-PDFF) are expensive and inaccessible to the general public, this study validated a highly accurate Machine Learning (ML) predictive model. The algorithm detects early-stage MASLD utilizing nothing more than cheap, routine biomarkers commonly found on standard annual blood panels.
Clinical Relevance: This opens the door for widespread, automated clinical screening, allowing primary care physicians to catch and reverse fatty liver disease years before advanced scarring or metabolic failure takes place.
7. A New Paradigm: Mandatory Liver Risk Stratification
Clinical Guideline: Rinella et al. — Nature Medicine (2026)
Pathophysiology Review: Romanos et al. — Diabetes, Obesity and Metabolism (2026)
The New Paradigm: Together, these 2026 publications mark a massive shift in metabolic medicine. Rinella et al. aggressively argue that due to the sheer scale of the metabolic epidemic, mandatory liver risk stratification must be implemented for all patients presenting with obesity or metabolic syndrome. Concurrently, Romanos et al. provided a master blueprint tying together these complex cellular pathologies with emerging targeted pharmaceutical treatments (such as GLP-1/GIP receptor agonists and THR-beta agonists).
Clinical Relevance: Treating obesity is no longer just about weight loss on a scale. Comprehensive care now requires clinicians to actively stage, track, and treat the underlying liver disease to ensure true cardiovascular and metabolic longevity.
The Liver-Heart Axis: How Metabolic Stress Impacts Your Cardiovascular Health
Think of your liver as your body’s metabolic control tower. When your metabolism is placed under chronic stress, a silent domino effect begins at the cellular level:
The Insulin Switch Fails: The liver becomes resistant to insulin's signals. It forgets to turn off glucose production, causing your fasting blood sugar to rise, while simultaneously accelerating the production of toxic cellular fats (diacylglycerols and ceramides).
The Rise of Dangerous Lipids: This cellular fat overload forces the liver to secrete a highly destructive lipid triad into your bloodstream: high triglycerides, low protective "good" (HDL) cholesterol, and an abundance of sticky, plaque-causing proteins (ApoB-100).
Ectopic Fat and Vascular Inflammation: This hidden fat builds up directly inside your liver tissue (steatosis). Science now shows that this localized liver fat drives heart disease far more aggressively than general body weight or BMI. As the liver becomes inflamed, it releases stress proteins (hepatokines) that travel straight to your cardiovascular system, irritating blood vessels and accelerating plaque buildup.
The Modern Medical Approach
Because this metabolic shift happens silently, modern medicine is evolving. Clinicians are now using machine learning algorithms to scan routine, everyday blood tests to catch early liver stress years before it advances. If you are managing metabolic or weight challenges, proactive liver screening is one of the most powerful steps you can take to safeguard your long-term cardiovascular health
Practical Steps to Protect Your Liver Metabolic Health
The following strategies have the strongest evidence for improving liver metabolic function. Always discuss with your healthcare provider before making significant changes, particularly if you have a diagnosed liver condition, diabetes, or cardiovascular disease.
Nutrition
Reduce ultra-processed foods and refined carbohydrates. Fructose, in particular, drives de novo lipogenesis more strongly than glucose. Sugary beverages and ultra-processed snacks are the most direct dietary triggers of hepatic fat accumulation.
Adopt a Mediterranean-style dietary pattern. Consistent evidence supports the Mediterranean diet for reducing liver fat, improving insulin sensitivity, and reducing cardiovascular risk — the three interrelated targets in liver-heart axis disease.
Prioritize whole food protein. Adequate dietary protein (1.2–1.6 g/kg body weight) supports liver repair, preserves muscle mass (which improves whole-body insulin sensitivity), and reduces lipogenic substrate availability.
Minimize alcohol. Even moderate alcohol intake can accelerate fibrosis progression in MASLD.
Consider omega-3 fatty acids. EPA and DHA (from fatty fish or supplements) have shown consistent benefits for reducing hepatic triglycerides and inflammation in multiple trials.
Physical Activity
Aerobic exercise reduces liver fat directly. Studies consistently show that moderate-intensity aerobic exercise (150+ minutes per week) reduces hepatic fat content — independent of weight loss. The liver responds to exercise signals rapidly, often within weeks.
Resistance training improves insulin sensitivity. Skeletal muscle is the body's largest glucose sink. Building and maintaining muscle mass reduces the metabolic burden on the liver by increasing peripheral glucose uptake. Aim for 2–3 sessions per week.
Avoid prolonged sedentary periods. Even brief walking breaks (5 minutes every hour) during sedentary work have been shown to blunt postprandial glucose and fat excursions — reducing the metabolic load the liver must handle.
Metabolic Health Monitoring
Evaluating cardiovascular, metabolic, and hepatic (liver) longevity requires looking closely at key blood biomarkers and physical metrics. When these markers drift outside of optimal zones, they signal systemic metabolic dysfunction, insulin resistance, and silent liver stress.
Below is an in-depth breakdown of the primary metabolic and liver biomarkers, their clinical targets, and the exact physiology behind why they matter to your long-term health.
1. Fasting Glucose
Optimal Target: Less than 100 mg/dL
Why It Matters (The Physiology): Fasting blood glucose is a primary window into your hepatic glucose output. When you sleep or fast, your liver is responsible for releasing a steady supply of glucose to keep your brain and body fueled. However, if the liver becomes insulin resistant, it ignores the signals to slow down and continues pumping out unnecessary sugar.
Clinical Significance: Chronically elevated fasting glucose is a strong warning sign of early-stage insulin resistance, prediabetes, and metabolic strain on the pancreas.
2. Triglycerides
Optimal Target: Less than 150 mg/dL
Why It Matters (The Physiology): Triglycerides are a direct reflection of Very Low-Density Lipoprotein (VLDL) overproduction by the liver. When the liver is overwhelmed by excess dietary sugars (especially fructose) and refined carbohydrates, it converts that surplus energy into fat via a process called de novo lipogenesis (creating new fat).
Clinical Significance: High triglycerides are a classic hallmark of poor metabolic health and a leading indicator of fat accumulation inside the liver tissue, a condition closely tied to fatty liver disease.
3. Alanine Aminotransferase (ALT)
Optimal Target:
Women: Less than 35 U/L
Men: Less than 45 U/L
Why It Matters (The Physiology): ALT is an enzyme found primarily inside liver cells (hepatocytes). It acts as a sensitive hepatocyte stress marker. When liver cells are damaged, inflamed, or dying due to toxic overload, fat accumulation, or alcohol strain, their cell membranes rupture, leaking ALT directly into the bloodstream.
Clinical Significance: Rising ALT levels are one of the earliest and clearest laboratory indicators of liver inflammation, cellular injury, and potential metabolic fatty liver progression.
4. HDL Cholesterol
Optimal Target:
Women: Greater than 50 mg/dL
Men: Greater than 40 mg/dL
Why It Matters (The Physiology): High-Density Lipoprotein (HDL) is a cornerstone of liver-heart axis health. Known as "good cholesterol," HDL acts as a molecular vacuum cleaner. Through a process called reverse cholesterol transport, HDL picks up excess cholesterol from your blood vessels and peripheral tissues and hauls it back to the liver to be safely broken down and excreted.
Clinical Significance: Low HDL levels undermine this protective pathway, significantly raising the risk of plaque buildup in the arteries (atherosclerosis) and worsening overall cardiovascular and metabolic profiles.
5. FIB-4 Score (Fibrosis-4 Index)
Optimal Target: Less than 1.30
Why It Matters (The Physiology): The FIB-4 score is a non-invasive, validated screening tool calculated using a patient's age, platelet count, and liver enzymes (AST and ALT). It is specifically designed to assess advanced liver fibrosis risk—the scarring of liver tissue that occurs after prolonged inflammation.
Clinical Significance: A FIB-4 score below 1.30 is highly reliable for ruling out advanced scarring. Keeping this score low confirms that while the liver may experience metabolic stress, it has not yet progressed to advanced, structural tissue damage or cirrhosis.
6. Waist Circumference
Optimal Target:
Women: Less than 88 cm (less than 35 inches)
Men: Less than 102 cm (less than 40 inches)
Why It Matters (The Physiology): While BMI measures total body mass, waist circumference specifically targets visceral fat—the dangerous adipose tissue packed tightly around internal organs like the liver, pancreas, and intestines. Visceral fat is not just inert storage; it is an active endocrine organ that pumps out inflammatory molecules (cytokines) directly into the portal vein leading straight to the liver.
Clinical Significance: Excess visceral fat is the ultimate key driver of systemic insulin resistance, metabolic syndrome, and lipid abnormalities. Managing this physical metric is often the most powerful lever an individual has for improving all the blood biomarkers listed above.
Summary for Context: These six markers do not exist in isolation. High visceral fat (waist circumference) triggers insulin resistance, causing the liver to overproduce sugar (glucose) and fat (triglycerides), leading to dropping protective lipids (HDL), inflamed liver cells (ALT), and potential long-term tissue scarring (FIB-4).
Request these tests at your annual physical if you have risk factors for MASLD. Early identification opens the largest window for lifestyle-based reversal.
Pharmacological Considerations (Discuss With Your Doctor)
Emerging therapies with liver-specific benefit include:
GLP-1 receptor agonists (e.g., semaglutide): Reduce liver fat, improve insulin sensitivity, and promote weight loss — addressing the core metabolic loop
SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin): Reduce hepatic glucose output and liver inflammation
Resmetirom (Rezdiffra): The first FDA-approved treatment specifically for MASH with liver fibrosis (approved 2024)
Vitamin E: Shown to reduce liver inflammation in non-diabetic MASH; discuss risks and benefits with your doctor
Emerging Therapies for MASLD: The Next Frontier
The treatment landscape for MASLD is evolving rapidly, with several promising therapies targeting the underlying drivers of liver fat accumulation, inflammation, and fibrosis.
FGF21 Analogues: Synthetic versions of fibroblast growth factor 21 designed to improve insulin sensitivity, increase fat oxidation, reduce liver fat, and suppress inflammation.
Dual GLP-1/GIP Agonists (Tirzepatide): Activate both GLP-1 and GIP receptors, producing substantial weight loss, improved glycemic control, and significant reductions in hepatic fat content.
Triple Agonists: Experimental drugs that simultaneously target GLP-1, GIP, and glucagon receptors, aiming to maximize weight loss, energy expenditure, and liver fat reduction.
ACC Inhibitors (Acetyl-CoA Carboxylase Inhibitors): Block a key enzyme involved in de novo lipogenesis, reducing the liver's ability to synthesize new fat.
FXR Agonists: Activate the farnesoid X receptor, improving bile acid metabolism, reducing hepatic fat accumulation, suppressing inflammation, and potentially slowing fibrosis progression.
THR-β Agonists Beyond Resmetirom: Selectively stimulate thyroid hormone receptor-beta in the liver, enhancing fatty acid oxidation, reducing liver fat, and improving lipid metabolism while minimizing systemic thyroid effects.
Collectively, these therapies represent a shift from treating symptoms toward directly targeting the metabolic, inflammatory, and fibrotic pathways that drive MASLD progression. Several are currently in late-stage clinical trials and may significantly expand treatment options in the coming years.
Common Myths About the Liver and Metabolism
Myth 1: "Fatty liver only happens in people who drink heavily"
False. MASLD (formerly NAFLD) is defined as fatty liver disease occurring in the absence of significant alcohol consumption. It is driven by metabolic factors — insulin resistance, poor diet, inactivity, and genetics — not alcohol. It is now the leading cause of liver disease in many countries.
Myth 2: "If my liver enzymes are normal, my liver is healthy"
Misleading. ALT and AST can be normal even in the presence of significant fibrosis. A normal liver panel does not exclude MASLD or advanced fibrosis. If you have metabolic risk factors, ask about a FIB-4 score or liver imaging.
Myth 3: "You can feel liver damage"
False. The liver contains no pain receptors. Significant fibrosis — and even early cirrhosis — can develop without any symptoms. By the time symptoms appear (fatigue, abdominal discomfort, jaundice), disease is often advanced. Silent progression is what makes early screening so valuable.
Myth 4: "Dietary fat causes fatty liver"
Oversimplified. The primary dietary driver of hepatic fat accumulation is excess carbohydrate intake — particularly fructose — which stimulates de novo lipogenesis. Dietary fat types matter, but the strongest evidence implicates sugar and refined carbohydrates, not total fat intake, in MASLD development.
Myth 5: "Liver supplements like milk thistle can cure fatty liver"
Unsupported. While silymarin (from milk thistle) has modest anti-inflammatory properties in cell studies, there is no high-quality clinical evidence that any supplement reverses MASLD, reduces fibrosis, or prevents disease progression. Lifestyle modification and, where appropriate, prescription therapy remain the foundation of treatment.
Myth 6: "Weight loss is the only treatment for MASLD"
Incomplete. While a 7–10% reduction in body weight consistently reduces liver fat and inflammation, exercise reduces liver fat independent of weight loss, and metabolic improvements (particularly in insulin sensitivity) occur even before significant weight change. The target is metabolic health, not a number on the scale.
Frequently Asked Questions
Q: What is the difference between glycogenolysis and gluconeogenesis?
Glycogenolysis breaks down already-stored glycogen in the liver — it's the rapid first-line response to falling blood sugar, active in the first 6–12 hours of fasting. Gluconeogenesis synthesizes entirely new glucose from non-carbohydrate precursors (lactate, amino acids, glycerol) — it dominates during prolonged fasting or in chronic insulin resistance. Both are regulated by glucagon, insulin, and cortisol, but through distinct enzymatic pathways. In type 2 diabetes, gluconeogenesis is often overactive, driving elevated fasting glucose independent of carbohydrate intake.
Q: What is selective hepatic insulin resistance and why does it matter?
In the insulin-resistant liver, the AKT-FOXO1 pathway — which normally suppresses glucose production — becomes impaired, while the SREBP-1c pathway — which drives fat synthesis — remains sensitive. The result is the liver simultaneously overproduces both glucose and fat: fasting hyperglycemia and hepatic steatosis together. This paradox explains why treating glucose alone in type 2 diabetes, without addressing liver fat and insulin resistance at the root, is often insufficient.
Q: Can fatty liver disease be reversed?
Yes — in its early stages. Simple steatosis (fat accumulation without significant inflammation or fibrosis) is largely reversible with sustained lifestyle change. Even early fibrosis can stabilize or partially regress. However, cirrhosis is generally considered irreversible, though further progression can be halted. The critical window for reversal is before significant fibrosis develops — which is why early detection matters enormously.
Q: Why do I have high fasting blood sugar even though I eat well?
High fasting glucose is typically driven by hepatic gluconeogenesis overnight. When the liver is insulin resistant, it continues manufacturing glucose from amino acids and lactate while you sleep — regardless of what you ate the night before. This "morning phenomenon" is a liver problem, not primarily a dietary one. Addressing liver insulin resistance (through exercise, dietary changes, or medication) is more effective than simply restricting carbohydrates.
Q: What tests should I ask my doctor about for liver health?
Start with a basic metabolic panel (glucose, ALT, AST, albumin) and a lipid panel (triglycerides, HDL, LDL). Ask your doctor to calculate your FIB-4 score from these values. If results are borderline, request a FibroScan or liver ultrasound. If you have type 2 diabetes, metabolic syndrome, or significant visceral obesity, proactive liver screening is warranted even without symptoms.
Q: How does liver health affect my cholesterol?
Your liver produces roughly 80% of your body's cholesterol and manages all aspects of lipoprotein metabolism — VLDL assembly, LDL receptor activity, and HDL recycling. In MASLD, these processes become dysregulated, producing the atherogenic triad: high triglycerides, low HDL, and small dense LDL. Improving liver metabolic health often improves lipid profiles significantly — sometimes more than statins alone.
Q: What medications are approved for fatty liver disease?
As of 2024, resmetirom (Rezdiffra) is the first FDA-approved medication specifically for MASH (metabolic dysfunction-associated steatohepatitis) with liver fibrosis. Additionally, GLP-1 receptor agonists (like semaglutide) and SGLT2 inhibitors are showing significant benefit in clinical trials for MASLD and are increasingly used off-label or for their metabolic co-benefits. Speak with a hepatologist or endocrinologist about which options are appropriate for your situation.
Q: Is MASLD genetic? Can I inherit it?
Genetics play a meaningful role. Variants in the PNPLA3 gene (particularly the I148M variant) and TM6SF2 gene significantly increase susceptibility to hepatic fat accumulation and more rapid fibrosis progression. However, genetics are not destiny — lifestyle factors powerfully modify genetic risk. If you have a family history of fatty liver disease or liver-related complications, earlier and more aggressive metabolic screening is warranted.
Q: How does exercise help the liver specifically?
Aerobic exercise reduces liver fat through multiple mechanisms: it increases hepatic fat oxidation, reduces de novo lipogenesis, improves whole-body insulin sensitivity (reducing the metabolic burden on the liver), and decreases visceral fat (a major source of free fatty acids flowing to the liver). The liver responds to exercise training relatively quickly — studies show measurable reductions in hepatic fat content within 6–8 weeks of consistent moderate exercise, even without significant weight loss.
Q: What is the liver–heart axis?
The liver–heart axis refers to the bidirectional communication between the liver and cardiovascular system through hepatokines, lipoproteins, inflammatory cytokines, and hormonal signals. A metabolically dysfunctional liver actively damages the heart by producing pro-atherogenic lipoproteins, releasing inflammatory proteins (like Fetuin-A), reducing cardioprotective factors (like FGF21), and disrupting hormonal balance (via RAAS activation). MASLD is now an independent cardiovascular risk factor — meaning it damages the heart beyond what is explained by accompanying conditions like obesity or diabetes.
Q: How does liver health affect aging and longevity?
Emerging research suggests that liver dysfunction may accelerate biological aging. Fatty liver disease is associated with inflammaging (chronic low-grade inflammation), cellular senescence (accumulation of dysfunctional aging cells), NAD+ depletion (reduced cellular energy production), and mitochondrial aging. Together, these processes impair metabolic flexibility, increase oxidative stress, and raise the risk of diabetes, cardiovascular disease, frailty, and age-related decline. Protecting liver health may therefore be an important strategy for promoting healthy aging and longevity.
Q: What are autophagy and lipophagy, and why do they matter for liver health?
Autophagy is the body's cellular recycling system that removes damaged proteins and organelles. In the liver, a specialized form called lipophagy breaks down excess fat stored within liver cells. When autophagy becomes impaired, fat accumulation, inflammation, and cellular stress increase, contributing to MASLD progression. Research suggests that exercise, calorie restriction, and intermittent fasting may stimulate autophagy pathways, helping maintain liver metabolic health and reducing the risk of fatty liver disease.
Q: Can you develop fatty liver disease even if you are not overweight?
Yes. This condition is known as Lean MASLD. Some individuals develop significant liver fat despite having a normal body mass index (BMI). Factors that contribute include increased visceral fat, insulin resistance, genetic variants such as PNPLA3 and TM6SF2, poor diet quality, physical inactivity, and altered gut microbiota. Because lean individuals are often considered "low risk," diagnosis may be delayed. A normal BMI does not guarantee a healthy liver, making metabolic screening important even in people who appear lean.
Conclusion and Action Steps
Your liver is not a passive processing organ. It is your body's metabolic decision-maker — determining, moment by moment, whether the nutrients you consume become energy, storage, or the building blocks of disease.
When hepatic metabolism becomes dysregulated — through insulin resistance, fat accumulation, and inflammatory signaling — the consequences extend far beyond the liver itself. Blood sugar rises. Cholesterol profiles worsen. Heart disease risk escalates. Weight becomes harder to manage. And all of it happens silently, without pain, often without any abnormal lab values until the disease is advanced.
The science is increasingly clear: protecting your liver metabolic health is one of the highest-leverage interventions available for preventing type 2 diabetes, cardiovascular disease, and premature aging.
Your Action Steps
This week:
Request a liver panel (ALT, AST) and a full lipid panel at your next blood draw
Ask your doctor to calculate your FIB-4 score
Identify your primary dietary source of refined carbohydrates or sugar and begin reducing it
This month:
Aim for 150+ minutes of moderate aerobic activity per week
Add 2 sessions of resistance training
Adopt one Mediterranean-style dietary habit (e.g., replace processed snacks with nuts, fish, or vegetables)
Ongoing:
Monitor waist circumference alongside weight
If you have type 2 diabetes, metabolic syndrome, or a family history of liver disease: ask about FibroScan
Treat your liver health as inseparable from your heart health
⚕️ Important: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making changes to your diet, exercise routine, or medication regimen — especially if you have a diagnosed medical condition.
Disclaimer: This article is for educational and informational purposes only and should not be considered medical advice. Always consult with qualified healthcare professionals before making changes to your health regimen or treatment plan. The information presented reflects current research as of February 2026 and may be subject to change as new evidence emerges.
Related Articles
Obesity and Biological Aging: The Hidden Cellular Damage Shortening Your Healthspan
References
Zhang, X., Yang, S., Chen, J., & Su, Z. (2019). Unraveling the regulation of hepatic gluconeogenesis. Frontiers in Endocrinology, 9, Article 802. https://doi.org/10.3389/fendo.2018.00802
Truong, X. T., & Lee, D. H. (2025). Hepatic insulin resistance and steatosis in metabolic dysfunction-associated steatotic liver disease: New insights into mechanisms and clinical implications. Diabetes & Metabolism Journal, 49(5), 964–986. https://doi.org/10.4093/dmj.2025.0644
Winterfeldt, K., & Siddiqi, S. A. (2026). The liver at the crossroads: Orchestrating lipoprotein dynamics and lipid homeostasis. Livers, 6(1), Article 6. https://doi.org/10.3390/livers6010006
Capone, F., Vacca, A., Bidault, G., Sarver, D., Kaminska, D., Strocchi, S., Vidal-Puig, A., Greco, C. M., Lusis, A. J., & Schiattarella, G. G. (2025). Decoding the liver-heart axis in cardiometabolic diseases. Circulation Research, 136(11), 1335–1362. https://doi.org/10.1161/CIRCRESAHA.125.325492
Liang, T., & Ren, J. (2026). Development and validation of a high-performance clinical predictive model for early identification of non-alcoholic fatty liver disease. Frontiers in Physiology, 17, Article 1689882. https://doi.org/10.3389/fphys.2026.1689882
van der Meer, D., Gurholt, T. P., Sønderby, I. E., et al. (2022). The link between liver fat and cardiometabolic diseases is highlighted by genome-wide association study of MRI-derived measures of body composition. Communications Biology, 5, Article 1271. https://doi.org/10.1038/s42003-022-04237-4
Demir, M., Bornstein, S. R., Mantzoros, C. S., & Perakakis, N. (2023). Liver fat as risk factor of hepatic and cardiometabolic diseases. Obesity Reviews, 24(10), e13612. https://doi.org/10.1111/obr.13612
Rinella, M. E., Sanyal, A. J., Loomba, R., et al. (2026). MASLD as a complication of obesity must include liver risk stratification. Nature Medicine, 32, 18–19. https://doi.org/10.1038/s41591-025-04130-7
Romanos, M., Garcia Cordova, J. M., Villamarin, J., Pazmino Zurita, J. D., & Acosta, A. (2026). Obesity and metabolic dysfunction-associated steatotic liver disease (MASLD): A literature review on pathophysiology and treatment. Diabetes, Obesity and Metabolism, 28(Suppl. 2), 19–30. https://doi.org/10.1111/dom.70659
European Association for the Study of the Liver. (2023). EASL clinical practice guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. Journal of Hepatology, 79(3), 696–777.
Lazarus, J. V., Mark, H. E., Anstee, Q. M., et al. (2022). Advancing the global public health agenda for NAFLD: A consensus statement. Nature Reviews Gastroenterology & Hepatology, 19(1), 60–78.
Younossi, Z. M., Koenig, A. B., Abdelatif, D., Fazel, Y., Henry, L., & Wymer, M. (2016). Global epidemiology of nonalcoholic fatty liver disease: Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology, 64(1), 73–84.
Petersen, K. F., Dufour, S., Befroy, D., Lehrke, M., Hendler, R. E., & Shulman, G. I. (2005). Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes. Diabetes, 54(3), 603–608.
Hallsworth, K., Fattakhova, G., Hollingsworth, K. G., Thoma, C., Moore, S., Taylor, R., Day, C. P., & Trenell, M. I. (2011). Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut, 60(9), 1278–1283. https://doi.org/10.1136/gut.2011.242073
Harrison, S. A., Bedossa, P., Guy, C. D., et al. (2024). A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. New England Journal of Medicine, 390(6), 497–509. https://doi.org/10.1056/NEJMoa2309000