Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health
Dive into the latest 2025 research on adipokines. Discover how fat cells act as an endocrine organ and how lifestyle changes can optimize leptin sensitivity and boost protective adiponectin.
METABOLISMOBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/13/202611 min read
For decades, body fat was viewed as little more than passive energy storage — a biological warehouse where excess calories accumulated until they were burned away through diet or exercise. Modern metabolic science has completely overturned that simplistic idea. Researchers now recognize adipose tissue as one of the body’s most dynamic endocrine organs, constantly releasing biochemical signals that regulate appetite, inflammation, insulin sensitivity, vascular health, immune function, and even aging itself (Tilg et al., 2025).
In other words, your body fat is not silent. It is communicating every second.
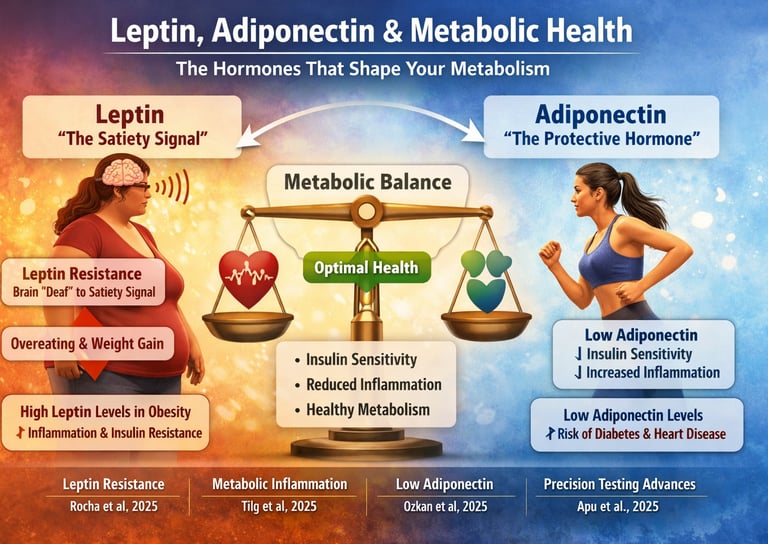
Among the most influential of these metabolic messengers are two adipokines — leptin and adiponectin. These hormones function like metabolic traffic controllers, determining whether the body maintains metabolic flexibility and energy balance or progresses toward insulin resistance, chronic inflammation, obesity, fatty liver disease, and cardiovascular dysfunction.
Leptin acts as the body’s satiety hormone, informing the brain that adequate energy has been stored. Under healthy conditions, rising leptin levels suppress hunger and increase energy expenditure. Yet in obesity, this communication system often breaks down. Instead of restoring balance, chronically elevated leptin contributes to leptin resistance — a state in which the brain becomes biologically “deaf” to satiety signals, promoting persistent hunger and metabolic dysfunction (Rocha et al., 2025).
Adiponectin performs almost the opposite role. It enhances insulin sensitivity, protects blood vessels, reduces oxidative stress, and dampens inflammatory signaling. Ironically, adiponectin levels decline precisely when visceral fat accumulation increases — at the exact moment the body requires its protective effects most urgently (Ozkan et al., 2025).
This hormonal imbalance represents far more than an academic curiosity. Emerging evidence suggests that adipokine dysfunction may predict future metabolic disease more accurately than Body Mass Index (BMI) alone. Two individuals with identical BMI values may possess dramatically different adipokine profiles — and profoundly different long-term risks for Type 2 diabetes, metabolic syndrome, nonalcoholic fatty liver disease, and atherosclerotic cardiovascular disease.
The implications are transformative. Obesity is increasingly understood not merely as excess body weight, but as a disorder of endocrine signaling and chronic low-grade inflammation. This shift is redefining modern preventive medicine.
Fat Tissue: The Endocrine Organ Hidden in Plain Sight
Adipose tissue was once considered metabolically inert. Today, scientists recognize it as an active endocrine and immunologic organ that secretes dozens of biologically active compounds known as adipokines. These signaling molecules influence nearly every major physiological system, including glucose metabolism, appetite regulation, immune activation, vascular function, and mitochondrial energy production.
When adipose tissue expands beyond healthy limits — especially visceral fat surrounding abdominal organs — its biological behavior changes dramatically. Healthy adipocytes begin to enlarge, oxygen delivery becomes impaired, immune cells infiltrate fat tissue, and inflammatory pathways activate. The result is a persistent state of metabolic inflammation sometimes referred to as “meta-inflammation” (Tilg et al., 2025).
This inflammatory environment disrupts normal adipokine signaling, particularly the balance between leptin and adiponectin.
The consequences extend far beyond weight gain alone:
Impaired insulin signaling
Increased hepatic fat accumulation
Elevated cardiovascular risk
Endothelial dysfunction
Chronic systemic inflammation
Altered appetite regulation
Reduced mitochondrial efficiency
Accelerated biological aging
In essence, dysfunctional fat tissue becomes a biochemical amplifier of chronic disease.
Leptin: The Satiety Hormone That Stops Working
Discovered in the 1990s, leptin rapidly transformed obesity science. Produced primarily by adipocytes, leptin travels through the bloodstream to the hypothalamus, where it signals that sufficient energy reserves are available.
Under normal physiological conditions, leptin helps regulate:
Hunger and satiety
Energy expenditure
Reproductive function
Thyroid signaling
Immune activity
Neuroendocrine balance
As fat stores increase, leptin production rises. In theory, this should reduce food intake and prevent excessive weight gain.
Yet obesity research revealed a paradox: individuals with obesity often have extremely high leptin concentrations but continue to experience increased appetite and reduced metabolic flexibility. This phenomenon became known as leptin resistance.
The Biology of Leptin Resistance
Leptin resistance occurs when the brain no longer responds appropriately to leptin’s satiety signals. The hormone is present in abundance, but the signaling pathway becomes impaired.
Several mechanisms appear responsible:
Chronic inflammation within the hypothalamus
Impaired leptin transport across the blood-brain barrier
Endoplasmic reticulum stress
Insulin resistance
Sleep deprivation
Excessive ultra-processed food intake
Oxidative stress
The result resembles insulin resistance. Just as high insulin no longer effectively lowers blood glucose, high leptin no longer effectively suppresses appetite.
This creates a vicious metabolic cycle:
Increased body fat raises leptin levels
Chronic exposure induces leptin resistance
Satiety signaling weakens
Hunger persists despite adequate energy stores
Further fat accumulation develops
Inflammation intensifies
Research by Rocha and colleagues (2025) demonstrated strong correlations between elevated leptin concentrations and increased body fat percentage in adolescents, suggesting that adipokine dysfunction begins early in life and may predict future metabolic disease trajectories.
Importantly, leptin is also pro-inflammatory. Elevated leptin signaling stimulates cytokine production and immune activation, linking obesity to chronic systemic inflammation and cardiometabolic disease.
Adiponectin: The Protective Hormone Modern Metabolism Depends On
If leptin represents metabolic overload, adiponectin represents metabolic protection.
Unlike most adipokines, adiponectin levels decrease as body fat increases — particularly visceral adiposity. This inverse relationship is one of the most important discoveries in metabolic endocrinology.
Adiponectin improves metabolic health through multiple mechanisms:
Enhances insulin sensitivity
Increases fatty acid oxidation
Reduces hepatic glucose production
Suppresses inflammatory signaling
Improves endothelial function
Protects mitochondria
Reduces oxidative stress
Higher adiponectin levels are consistently associated with:
Lower Type 2 diabetes risk
Better glucose control
Reduced cardiovascular disease
Improved metabolic flexibility
Lower systemic inflammation
Healthier lipid metabolism
Ozkan et al. (2025), analyzing data from the ARIC study, found that favorable adiponectin profiles strongly predicted long-term maintenance of metabolic health independent of BMI and traditional cardiometabolic risk factors.
This finding is critical because it demonstrates that adiponectin is not simply a passive marker of health — it is an active biological determinant of metabolic resilience.
Why Visceral Fat Matters More Than Weight Alone
Not all fat behaves equally.
Subcutaneous fat, located beneath the skin, is metabolically less harmful than visceral fat stored around internal organs. Visceral adiposity is particularly dangerous because it is highly inflammatory and strongly associated with low adiponectin production.
This helps explain why some individuals with “normal weight obesity” develop metabolic syndrome despite appearing lean, while others with higher BMI remain metabolically healthier.
The difference often lies in adipokine biology.
Obesity Is an Inflammatory Disease
One of the most important conceptual shifts in modern metabolic medicine is the recognition that obesity-related disease is fundamentally inflammatory.
Tilg and colleagues (2025) described adipokines as the “masterminds” of metabolic inflammation, orchestrating immune responses that connect obesity to insulin resistance, cardiovascular disease, and fatty liver disease.
In obesity:
Enlarged adipocytes release inflammatory cytokines
Macrophages infiltrate fat tissue
Oxidative stress rises
Leptin signaling increases
Adiponectin declines
Chronic low-grade inflammation persists
This persistent inflammatory state disrupts nearly every metabolic pathway.
The implications are enormous. Weight loss alone may not fully restore metabolic health if adipokine dysfunction and inflammation persist. Future therapies may increasingly focus on improving adipose tissue quality and endocrine signaling rather than simply reducing body mass.
Beyond BMI: The Rise of Adipokine Biomarkers
For decades, BMI has dominated obesity assessment despite its major limitations.
BMI cannot distinguish between:
Muscle and fat mass
Visceral and subcutaneous fat
Metabolically healthy versus unhealthy obesity
Inflammatory status
Hormonal dysfunction
Adipokine profiling may offer a far more biologically meaningful assessment.
The Leptin/Adiponectin Ratio (LAR)
One of the most promising emerging biomarkers is the leptin/adiponectin ratio (LAR), which reflects the balance between pro-inflammatory and protective adipokine signaling.
A pilot study by Balestra et al(2026). evaluated LAR in obese adults with liver steatosis undergoing Very-Low Energy Ketogenic Therapy (VLEKT).
Researchers observed significant improvements in:
Body weight
Insulin resistance
Liver stiffness
Triglycerides
Hepatic steatosis
Fasting glucose
LDL cholesterol
Importantly, reductions in LAR correlated with broader improvements in adipose tissue endocrine function, inflammatory balance, renal markers, and hepatic health.
The study suggests that LAR may serve as a multidimensional biomarker capable of monitoring systemic metabolic recovery more comprehensively than HOMA-IR alone.
The Adiponectin/Leptin Ratio and Metabolic Syndrome
Additional evidence supporting adipokine profiling emerged from Abdulateef et al. (2026), who evaluated adiponectin, leptin, Galectin-1, and the adiponectin/leptin ratio in patients with metabolic syndrome.
The findings were striking:
Adiponectin levels were significantly lower in metabolic syndrome
The adiponectin/leptin ratio was markedly reduced
The ratio independently predicted metabolic syndrome risk
Higher ratios were associated with better metabolic health
Even after adjusting for age and BMI, adipokine balance remained highly predictive.
This reinforces a crucial principle: metabolic disease is not simply about body size — it is about endocrine and inflammatory signaling.
Can Lifestyle Change Adipokines?
One of the most encouraging discoveries in adipokine research is that these hormones are highly modifiable.
Biology is not destiny.
Exercise and Adipokine Function
Regular exercise remains one of the most effective strategies for improving adipokine balance.
Aerobic exercise:
Increases adiponectin
Improves insulin sensitivity
Reduces visceral fat
Lowers inflammatory cytokines
Resistance training:
Enhances glucose uptake
Improves leptin sensitivity
Preserves lean muscle mass
Supports mitochondrial function
Even modest weight reduction — approximately 5–10% of body weight — can meaningfully improve adiponectin concentrations.
Sleep and Leptin Signaling
Sleep deprivation profoundly disrupts appetite-regulating hormones.
Poor sleep:
Reduces leptin sensitivity
Increases hunger hormones like ghrelin
Worsens insulin resistance
Promotes visceral fat accumulation
Chronic circadian disruption may therefore contribute directly to obesity and metabolic syndrome through adipokine dysregulation.
Nutrition and Metabolic Inflammation
Anti-inflammatory nutrition patterns appear particularly beneficial for adipokine optimization.
Evidence supports diets emphasizing:
Polyphenol-rich vegetables and fruits
Omega-3 fatty acids
High-fiber foods
Mediterranean dietary patterns
Low glycemic load carbohydrates
Minimally processed foods
These approaches reduce inflammatory signaling while improving insulin sensitivity and adiponectin production.
Could Natural Compounds Improve Adipokines?
Emerging research is exploring whether certain bioactive compounds can beneficially influence adipokine biology.
A systematic review by Mahdavi et a l(2026) evaluated propolis and its effects on leptin, resistin, and adiponectin.
Preclinical findings suggested:
Reduced leptin expression
Lower inflammatory signaling
Increased adiponectin levels
Improved antioxidant defense
Potential mechanisms included:
PPAR-γ activation
NF-κB inhibition
Reduced oxidative stress
Human evidence remains inconsistent, but these findings highlight growing interest in nutritional modulation of adipokine pathways.
Precision Medicine and the Future of Metabolic Care
The future of obesity medicine may rely heavily on personalized adipokine profiling.
Apu et al. (2025) developed advanced multiplex assays capable of simultaneously measuring leptin, adiponectin, and resistin with remarkable precision using targeted mass spectrometry.
This technology could eventually enable clinicians to:
Detect early metabolic dysfunction
Predict disease trajectories
Personalize nutrition interventions
Monitor therapeutic response
Assess inflammatory risk
Such advances represent a transition from crude anthropometric assessment toward precision metabolic medicine.
Clinical Pearls: What Modern Research Teaches Us
1. Adipokines as Predictive Biomarkers (Beyond BMI)
Leptin and adiponectin profiles are better predictors of future metabolic health transitions than BMI alone. Two individuals with the same Body Mass Index (BMI) can have dramatically different metabolic risks. Favorable adiponectin levels (the protective hormone) predict sustained metabolic health, while unfavorable profiles (high leptin, likely resistance) predict metabolic deterioration, independent of traditional risk factors.
Pearl: Don't rely solely on BMI; consider adipokine profiling to capture the actual biological status and predict future disease trajectory.
2. The Central Role of Leptin Resistance
In obesity, high leptin levels do not mean the body has enough satiety signaling; it indicates leptin resistance. The brain is effectively "deaf" to the high signal. This is the core metabolic dysfunction driving continued overeating and weight gain.
Pearl: The therapeutic goal for high leptin isn't to lower leptin, but to restore leptin sensitivity through interventions that improve insulin signaling (exercise, quality sleep, stress management).
3. Adiponectin is Your Metabolic Protector
Adiponectin is the "good guy" hormone that promotes insulin sensitivity and reduces chronic inflammation. Paradoxically, levels decrease as visceral fat increases, meaning the people who need its protection the most have the least of it.
Pearl: Prioritize strategies specifically known to boost adiponectin, such as aerobic exercise and anti-inflammatory nutrition. Even modest weight loss (5-10%) can yield a meaningful increase.
4. Metabolic obesity
is an Inflammatory Condition
Obesity-related disease is fundamentally a systemic inflammatory condition driven by dysfunctional adipokine signaling. Adipose tissue acts as an endocrine organ, and its dysregulation (particularly unbalanced leptin/adiponectin) orchestrates chronic low-grade inflammation.
Pearl: Interventions must address the immunometabolic link. Treatments shouldn't just target caloric restriction but should aim to restore healthy adipokine function to resolve the underlying inflammation.
5. Adipokine Levels are Modifiable
Despite genetic influences, lifestyle factors have a substantial impact on adipokine levels, demonstrating that biology is not destiny. Measurable improvements can occur relatively quickly.
Pearl: Patients can achieve measurable improvements in adiponectin within 4-12 weeks of consistent exercise and diet changes. This provides a strong, objective target and a positive feedback mechanism for encouraging sustained lifestyle adherence.
The New Definition of Metabolic Health
Modern science is redefining obesity and metabolic disease.
The traditional model focused primarily on calories and body weight. The emerging model recognizes a far more complex biological reality involving:
Endocrine signaling
Inflammation
Immune activation
Hormonal resistance
Mitochondrial dysfunction
Adipose tissue biology
Leptin and adiponectin sit at the center of this metabolic network.
Understanding these hormones changes how we think about:
Hunger
Weight gain
Insulin resistance
Cardiovascular disease
Fatty liver disease
Longevity
Most importantly, it shifts the conversation away from blame and toward biology.
Your fat tissue is not passive. It is biologically active, hormonally intelligent, and metabolically influential. Whether those signals protect your health or undermine it depends largely on the quality and function of adipose tissue itself.
The future of metabolic medicine will likely move beyond simplistic weight-centered approaches toward restoring healthy adipokine signaling, reducing metabolic inflammation, and improving endocrine resilience.
In that future, leptin and adiponectin may become as clinically important as cholesterol and blood pressure are today.
Key Takeaways
Adipose tissue functions as a major endocrine organ, not merely energy storage
Leptin regulates satiety, but obesity commonly induces leptin resistance
Adiponectin enhances insulin sensitivity and suppresses inflammation
Visceral fat disrupts adipokine balance and promotes chronic disease
Adipokines predict metabolic health more accurately than BMI alone
Chronic metabolic inflammation links obesity to cardiometabolic disease
The leptin/adiponectin ratio is emerging as a powerful biomarker
Exercise, sleep, and anti-inflammatory nutrition significantly improve adipokine function
Precision adipokine testing may shape the future of personalized metabolic medicine
Frequently Asked Questions
Q: Can I lower my leptin levels if they're too high?
A: High leptin levels usually indicate leptin resistance rather than true leptin excess. The goal is restoring leptin signaling through improved insulin sensitivity, regular exercise, and quality sleep rather than lowering leptin itself.
Q: How quickly can I improve my adiponectin levels?
A: Studies show measurable improvements in adiponectin concentrations within 4-12 weeks of consistent exercise and modest weight loss. Even without weight loss, regular aerobic activity can increase adiponectin levels.
Q: Is adiponectin more important than leptin?
A: They work complementarily. Leptin signals energy availability, while adiponectin promotes metabolic protection. Both matter, but from a metabolic disease prevention perspective, maintaining adequate adiponectin may be slightly more critical.
Q: Do genetics determine my adipokine levels?
A: Genetics influence baseline adipokine production, but lifestyle factors have enormous impact. Even people genetically predisposed to lower adiponectin can improve through exercise and diet.
Q: Can supplements improve my adipokine profile?
A: Some research suggests certain supplements (curcumin, resveratrol, omega-3s) may modestly improve adiponectin levels, but lifestyle changes provide far more substantial effects.
Author’s Note
As a clinician and academic deeply engaged in metabolic medicine, my goal in writing this article is to bridge the gap between cutting-edge scientific research and practical, patient-centered understanding. Leptin and adiponectin are often discussed only in advanced endocrinology or research settings, yet their influence on everyday metabolic health is profound. By translating complex hormonal pathways into accessible explanations, I hope to empower both healthcare professionals and the public with knowledge that drives early detection, prevention, and more personalized intervention strategies.
The studies highlighted here—from adolescent adipokine correlations to advanced biomarker measurement technologies—represent a major shift in how we understand metabolic disease. Rather than treating obesity as a simple imbalance of calories, the emerging science underscores the intricate biology of inflammation, hormonal resistance, and endocrine signaling within adipose tissue.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
PCOS Is Being Renamed in 2026: What the New Science Means for Women
How Exercise Reverses Leptin Resistance and Restores Metabolic Health | DR T S DIDWAL
Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health | DR T S DIDWAL
hsCRP Explained: What Inflammation Means for Your Heart | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
5 Steps to Reverse Metabolic Syndrome: Diet, Habit, & Lifestyle Plan | DR T S DIDWAL
The Role of Cholesterol in Health and Disease: Beyond the "Bad" Label | DR T S DIDWAL
Lowering Cholesterol with Food: 4 Phases of Dietary Dyslipidemia Treatment | DR T S DIDWAL
The Best Dietary Fat Balance for Insulin Sensitivity, Inflammation, and Longevity | DR T S DIDWAL
References
Apu, J., Yang, X., Lin, T. T., Fillmore, T. L., Gritsenko, M. A., Kelly, S. S., Swensen, A. C., Shi, T., Master, S. R., DeLany, J. P., Goodpaster, B. H., Qian, W. J., & Qu, J. (2025). A multiplex assay of leptin, resistin, and adiponectin by immunoaffinity enrichment and targeted mass spectrometry. Journal of Mass Spectrometry and Advances in the Clinical Lab, 36, 11–18. https://doi.org/10.1016/j.jmsacl.2025.01.003
Malek Mahdavi, A., Javadivala, Z., Ilkay, H.O. et al. Mechanistic insights into propolis in targeting adipokines including leptin, resistin, and adiponectin: A systematic review. J Diabetes Metab Disord 25, 31 (2026). https://doi.org/10.1007/s40200-026-01855-1
Ozkan, B., Zhang, S., Echouffo-Tcheugui, J. B., Florido, R., Nambi, V., Michos, E. D., Abushamat, L. A., Matsushita, K., Gerstenblith, G., Blumenthal, R. S., Hoogeveen, R., Ballantyne, C. M., Coresh, J., Selvin, E., & Ndumele, C. E. (2025). Adipokines and transitions in metabolic health over time: The Atherosclerosis Risk In Communities (ARIC) Study. The Journal of Clinical Endocrinology and Metabolism, 110(9), e2939–e2945. https://doi.org/10.1210/clinem/dgae916
Rocha, A. R. F., de Morais, N. S., Azevedo, F. M., Morais, D. C., Pereira, P. F., Peluzio, M. D. C. G., Franceschini, S. D. C. C., & Priore, S. E. (2025). Leptin, CRP, and adiponectin correlate with body fat percentage in adolescents: Systematic review and meta-analysis. Frontiers in Nutrition, 12, 1560080. https://doi.org/10.3389/fnut.2025.1560080
Abdulateef, Darya Saeed, Mahmood, Trifa Abdalla, Arkawazi, Lizan Ismail, Galectin-1, Adiponectin, Leptin, and the Adiponectin to Leptin Ratio as Predictors of Metabolic Syndrome: Influence of Age and Body Mass Index, BioMed Research International, 2026, 1789457, 9 pages, 2026. https://doi.org/10.1155/bmri/1789457
Tilg, H., Ianiro, G., Gasbarrini, A., & colleagues. (2025). Adipokines: Masterminds of metabolic inflammation. Nature Reviews Immunology, 25, 250–265. https://doi.org/10.1038/s41577-024-01103-8
Balestra, F., Donghia, R., De Luca, M., Stabile, D., Coletta, S., Panzetta, G., Palieri, R., Di Chito, M., De Pergola, G., Giannelli, G., Pesole, P. L., & Scavo, M. P. (2026). Leptin/Adiponectin ratio as a new multidimensional biomarker in obese patients with liver steatosis undergoing VLEKT: Results from a pilot study. Frontiers in Nutrition, 13, Article 1754299. https://doi.org/10.3389/fnut.2026.1754299