Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health
Is your body fat an endocrine organ? Learn how "sick fat" triggers metabolic inflammation and heart disease, and discover emerging biomarkers for early cardiovascular detection.
OBESITYHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/30/202613 min read
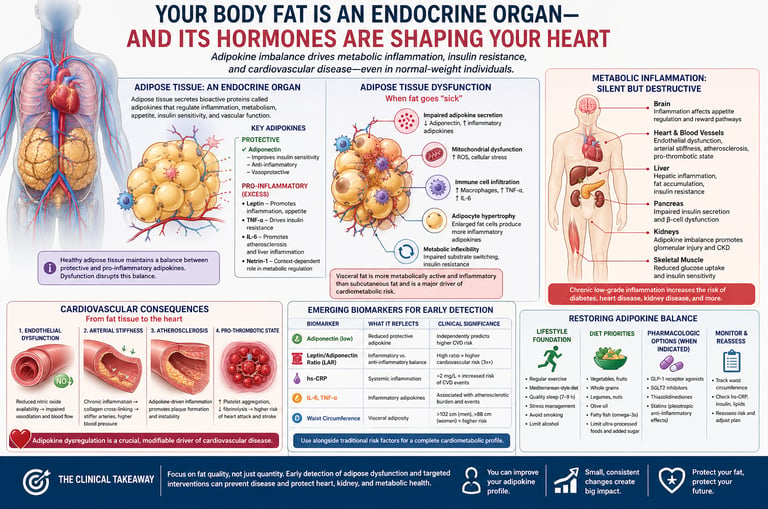
Adipose tissue is an endocrine organ that releases adipokines—hormones that regulate inflammation, metabolism, and cardiovascular health. When fat becomes dysfunctional, it promotes chronic inflammation, insulin resistance, and atherosclerosis, increasing heart disease risk even in people with normal weight.
Best ways to improve adipokine balance
Exercise: Raises adiponectin within 6–12 weeks
Diet: Mediterranean-style eating reduces inflammation
Sleep & stress control: Normalize hormonal signaling
Medications (if needed): GLP-1 agonists, SGLT2 inhibitors
Most useful early biomarkers
hs-CRP (>2 mg/L = higher risk)
Leptin/adiponectin ratio (LAR)
Fasting insulin / HOMA-IR
Waist circumference (visceral fat marker)
Clinicians' Perspective
1. Paradigm Shift in Adipose Biology
Historically, adipose tissue was considered a passive energy storage site (triglyceride reservoir).
Modern research now defines it as a metabolically active endocrine organ.
It continuously secretes adipokines, which regulate key physiological processes (Tilg et al., 2025).
2. What Are Adipokines?
Adipokines = bioactive signaling proteins released by:
Adipocytes (fat cells)
Immune cells within adipose tissue
They regulate:
Appetite control
Insulin sensitivity
Vascular tone
Immune and inflammatory responses
3. Role in Healthy Adipose Tissue
Maintain metabolic homeostasis through balanced signaling:
↑ Anti-inflammatory adipokines
↓ Pro-inflammatory adipokines
Key benefits:
Improved insulin sensitivity
Reduced systemic inflammation
Preserved vascular flexibility
4. Adipose Tissue Dysfunction
Occurs due to:
Adipocyte enlargement (hypertrophy)
Hypoxia within fat tissue
Lipid overload
Leads to:
Disrupted adipokine balance
Shift toward pro-inflammatory state
Results in systemic metabolic consequences (Bou Matar et al., 2025)
5. Dual Role of Adipokines
In health:
Maintain metabolic harmony
In disease:
Drive chronic inflammation and metabolic disorders
Described as:
“Masterminds of metabolic inflammation” (Tilg et al., 2025)
6. Key Adipokines and Their Functions
Adiponectin
Source: Adipocytes
Function:
↑ Insulin sensitivity
Anti-inflammatory
Dysfunction: Reduced levels
Classification: Protective
Leptin
Source: Adipocytes
Function: Appetite regulation
Dysfunction: Elevated → promotes vascular inflammation
Classification: Pro-inflammatory (in excess)
TNF-α
Source: Macrophages in adipose tissue
Function: Acute immune activation
Dysfunction: Chronic elevation → insulin resistance
Classification: Pro-inflammatory
IL-6
Source: Adipocytes and immune cells
Function: Acute-phase signaling
Dysfunction: Promotes atherosclerosis and liver inflammation
Classification: Pro-inflammatory
Netrin-1
Source: Adipocytes
Function: Neuronal guidance; emerging metabolic roles
Dysfunction: Context-dependent effects
Classification: Complex / Emerging
7. Emerging Insight: Netrin-1 vs Adiponectin
Recent evidence shows:
Adiponectin → consistently protective
Netrin-1 → context-dependent, sometimes opposing effects
Highlights:
Metabolic disease is not driven by a single molecule
Instead, it reflects disruption of the entire adipokine network (Ramos-Zavala et al., 2025)
Key Clinical Insight
Cardiometabolic disease is best understood as a result of adipokine imbalance, not simply excess fat mass.
Focus should shift toward adipose tissue function and signaling, rather than weight alone.40%Of normal-weight adults may harbor occult adipose dysfunction
3×Higher cardiovascular risk with elevated leptin-to-adiponectin ratio
8 weeks Time to measurable adiponectin improvement with sustained exercise
60%Of metabolic inflammation cases are clinically silent and symptom-free
Adipose Tissue Dysfunction: When Fat Goes "Sick"
The term "adipose tissue dysfunction" refers to a fundamental breakdown in fat tissue's capacity to regulate its own secretory and metabolic functions. This is not simply a matter of having "too much fat"—it is about the quality and behavior of fat cells, regardless of their quantity. A person with a body mass index in the normal range can have profoundly dysfunctional adipose tissue, while some individuals with elevated BMI retain relatively healthy fat cell function (Bou Matar et al., 2025).
Bou Matar et al. (2025), publishing in Frontiers in Endocrinology, conducted a landmark investigation into the mechanisms by which adipose dysfunction disrupts metabolic homeostasis. Their work identified five interlocking pathological processes:
Impaired Adipokine Secretion
Dysfunctional fat tissue fails to suppress inflammatory adipokines and simultaneously reduces output of protective molecules like adiponectin, creating a persistent pro-inflammatory state.
Mitochondrial Dysfunction
Energy production within fat cells becomes inefficient, leading to excess reactive oxygen species (ROS) and cellular stress that further impairs adipokine balance.
Immune Cell Infiltration
Macrophages and other immune cells invade dysfunctional adipose tissue, releasing additional waves of TNF-α and IL-6 that amplify local and systemic inflammation.
Adipocyte Hypertrophy
Enlarged fat cells shift toward a pro-inflammatory secretory profile. Gao et al. (2025) demonstrated in Adipocyte that hypertrophied cells produce dramatically more TNF-α and IL-6, creating a vicious amplifying cycle.
Metabolic Inflexibility
Fat tissue loses the capacity to shift between different metabolic substrates, contributing to whole-body insulin resistance and impaired glucose disposal.
Clinical Pearl: Location Is Everything
Visceral adipose tissue—the fat that surrounds internal organs in the abdomen—is far more metabolically active and inflammatory than subcutaneous fat stored under the skin. A normal-appearing waist can harbor dangerous visceral fat. This is why waist circumference (≥88 cm in women, ≥102 cm in men) is a more sensitive cardiometabolic risk marker than BMI alone. Lin & Tandar (2026) confirmed global patterns of visceral adiposity as a leading driver of cardiometabolic disease across diverse populations.
Metabolic Inflammation: The Silent Force Behind Chronic Disease
Metabolic inflammation is perhaps the most insidious concept in modern medicine. Unlike the inflammation you experience after a sprained ankle—red, swollen, and unmistakably painful—metabolic inflammation is chronic, systemic, and entirely symptom-free. You cannot feel it, yet it is silently scratching the lining of your arteries, impairing the function of your pancreas, and priming your liver for disease.
He et al. (2026), publishing in Pathology Research and Practice, provided a comprehensive mechanistic framework for how adipokines mediate crosstalk between metabolic dysregulation and inflammatory pathways. Their research revealed that adipokines are not passive responders—they are active coordinators of immune-metabolic communication. Key mechanisms include:
Pattern Recognition Activation: Inflammatory adipokines activate pattern recognition receptors (including Toll-like receptors) on immune cells, priming the entire innate immune system for a heightened inflammatory response—even in the absence of infection.
Feedforward Amplification: Once triggered, adipokine-driven inflammation creates self-sustaining feedback loops. TNF-α produced by macrophages stimulates adipocytes to produce more inflammatory adipokines, which recruit more macrophages. This cycle is difficult to interrupt without deliberate intervention.
Organ-Specific Crosstalk: Adipokines communicate differently with the liver, skeletal muscle, pancreas, and kidneys. In the liver, inflammatory adipokines promote hepatic insulin resistance and fat accumulation. In the pancreas, they impair insulin secretion. In skeletal muscle, they reduce glucose uptake. The consequence is a system-wide metabolic implosion.
Key Research Finding
A major study by Yang et al. (2026) in Lipids in Health and Disease found that adiponectin deficiency directly contributes to diabetic kidney disease progression, with inflammatory adipokines activating kidney-resident immune cells and promoting glomerular injury. This confirms that adipokine dysfunction reaches far beyond the cardiovascular system—it is a whole-body phenomenon.
One particularly important consequence of metabolic inflammation is its effect on the kidneys. Yang et al. (2026) demonstrated that adipokine dysregulation activates lipotoxic pathways within renal tissue, damaging the delicate filtering structures called glomeruli. This creates a mechanistic link between adipose dysfunction and the development and progression of diabetic kidney disease—a condition affecting hundreds of millions of people worldwide.
Cardiovascular Consequences: From Fat Tissue to the Heart
The cardiovascular consequences of adipokine dysregulation are perhaps the most clinically urgent dimension of this story. The American College of Cardiology (2025) released findings indicating that changes in the biology of internal fat may represent a leading cause of heart failure—a statement that would have seemed remarkable just a decade ago, when fat was considered a bystander rather than a biological actor in cardiac disease.
Kishimoto and Higashi (2025/2026), writing in Hypertension Research, provided a comprehensive update on adipokine-mediated vascular pathology. Their synthesis identifies four distinct vascular disease mechanisms directly attributable to adipokine dysfunction:
Endothelial Dysfunction
Inflammatory adipokines impair the ability of the endothelium—the single-cell lining of blood vessels—to produce nitric oxide, the molecule responsible for maintaining vascular flexibility and regulating blood flow. The result is stiffened, poorly responsive arteries
Arterial Stiffness
Chronic exposure to TNF-α and IL-6 promotes cross-linking of collagen and elastin in arterial walls. Arteries lose their youthful compliance, blood pressure rises, and the heart must work harder with every beat—accelerating cardiac aging.
Atherosclerotic Plaque Formation
Adipokine-driven inflammation promotes the infiltration of oxidized LDL and macrophages into arterial walls, creating the lipid-laden plaques that can rupture and trigger heart attacks. Early atherosclerosis may be detectable in people in their 30s and 40s with metabolic inflammation.
Increased Thrombotic Risk
Adipokine dysregulation alters the coagulation system—promoting platelet aggregation and impairing fibrinolysis. This creates a "prothrombotic" state in which blood clots more readily, substantially raising the risk of heart attack and stroke.
The special issue published by Mannino (2025) in the International Journal of Molecular Sciences synthesised recent advances in adipose tissue metabolic function and dysfunction, confirming that the mechanistic links between dysfunctional adipose tissue and cardiovascular outcomes are now backed by robust, multi-dimensional evidence spanning molecular biology, epidemiology, and clinical observation.
Emerging Biomarkers for Early Cardiovascular Detection
One of the most exciting developments in cardiometabolic medicine is the emergence of adipokine-based biomarkers that can identify cardiovascular risk before clinical events occur. Traditional risk scores rely on cholesterol, blood pressure, and age. Adipokine profiling adds a new biological layer that captures inflammatory and metabolic dysfunction not reflected in standard panels.
Netala et al. (2025), publishing in the International Journal of Molecular Sciences, reviewed cardiovascular biomarkers as precision diagnostic tools. Their analysis highlights several adipokine-related markers that improve risk prediction:
Adipokine Biomarker Toolkit
Adiponectin (low levels): Independently predicts elevated cardiovascular risk, even after controlling for traditional risk factors. Consider testing in patients with metabolic syndrome or unexplained insulin resistance.
Leptin/Adiponectin Ratio (LAR): A high ratio reflects simultaneous over-activation of the inflammatory "accelerator" (leptin) and failure of the anti-inflammatory "brake" (adiponectin). LAR outperforms either marker alone for cardiovascular risk stratification.
High-sensitivity C-reactive protein (hs-CRP): A downstream marker of adipokine-driven inflammation; levels above 2 mg/L significantly increase cardiovascular event risk. Koo et al. (2025) confirmed it among the strongest predictors of future cardiovascular disease.
IL-6 and TNF-α: Direct products of dysfunctional adipose tissue; both correlate with atherosclerotic burden and incident cardiovascular events.
Nazir et al. (2025), in a comprehensive literature review in Health Science Reports, documented how modern laboratory technologies now enable adipokine profiling that was technically impossible just five years ago. Clinical applications include screening asymptomatic individuals with metabolic risk factors, monitoring disease progression, assessing treatment response, and identifying patients who require more aggressive intervention.
Therapeutic Strategies: Restoring Adipokine Balance
Understanding that adipokine dysregulation—not simply body weight—is the driver of cardiometabolic disease opens powerful new therapeutic avenues. The goal is not merely weight reduction but the restoration of adipose tissue function and a healthy adipokine profile.
Lifestyle Modification: The Most Potent Intervention
Sustained physical activity remains the single most effective intervention for normalizing adipokine profiles. Exercise directly stimulates adiponectin production and suppresses inflammatory adipokines. Research consistently demonstrates measurable improvements in adiponectin and hs-CRP within 6–12 weeks of a regular exercise program—even without significant weight loss. This is a profound finding: you can begin to "reprogram" your fat cells before the scale reflects any change.
Dietary quality matters independently of caloric balance. Diets rich in fiber, whole grains, polyphenols, and omega-3 fatty acids promote healthy adipokine profiles. Ultra-processed foods, excess added sugar, and refined carbohydrates accelerate adipose dysfunction and worsen inflammatory markers.
Pharmacological Approaches
Several existing drug classes act—at least in part—by improving adipokine profiles. GLP-1 receptor agonists (semaglutide, liraglutide) reduce adipose inflammation and improve adiponectin levels. SGLT-2 inhibitors (empagliflozin, dapagliflozin) protect against metabolic inflammation through mechanisms independent of weight loss. Thiazolidinediones directly improve adipose tissue insulin sensitivity, increasing adiponectin production substantially.
Emerging Frontier
Research on direct adiponectin supplementation and Netrin-1 pathway modulation is in preclinical and early clinical stages. Given that Ramos-Zavala et al. (2025) identified the opposing roles of Netrin-1 and adiponectin in metabolic inflammation, future therapies may aim to simultaneously boost protective adipokines while suppressing inflammatory ones—rather than targeting a single molecule.
Monitoring and Early Detection
For individuals with metabolic risk factors, a comprehensive cardiometabolic evaluation should now include more than standard lipid panels. Requesting hs-CRP, fasting insulin, waist circumference measurement, and (where available) adiponectin levels can provide a much richer picture of true metabolic risk than cholesterol alone. Nazir et al. (2025) advocate for this broader biomarker approach as a path to genuinely personalized cardiovascular prevention.
Practical Applications for Daily Life
Translating cutting-edge adipokine research into actionable daily habits is both possible and impactful. Here are evidence-grounded practices you can begin implementing toda
Move daily—even in short bursts
As little as 30 minutes of moderate aerobic activity daily raises adiponectin and reduces inflammatory adipokines. Walking, cycling, and swimming are all effective. Consistency matters more than intensity.
Eat an adipokine-friendly diet
Emphasize vegetables, legumes, whole grains, olive oil, and fatty fish. Limit ultra-processed foods and added sugars. The Mediterranean dietary pattern has the strongest evidence for improving adipokine balance
Track waist circumference
Measure at the level of your navel monthly. Reducing waist circumference below 88 cm (women) or 102 cm (men) is one of the most powerful steps you can take to reduce visceral adiposity and normalize adipokine secretion.
Ask for hs-CRP testing
At your next check-up, request a high-sensitivity C-reactive protein test. Levels above 2 mg/L signal elevated cardiovascular risk driven by metabolic inflammation—even if all other markers appear normal.
Prioritize sleep quality
Sleep deprivation directly disrupts adipokine secretion and raises inflammatory markers. Aim for 7–9 hours of quality sleep per night. Treating sleep apnea, if present, can substantially improve metabolic profiles
Manage chronic stress
Chronic psychological stress elevates cortisol, which promotes visceral fat accumulation and worsens adipokine balance. Mind-body practices—yoga, meditation, deep breathing—have measurable anti-inflammatory effects.
Frequently Asked Questions
Q: Can I have normal weight but still have adipose tissue dysfunction? A: Yes. Metabolically obese normal-weight (MONW) individuals can have dysfunctional adipose tissue. What matters is the metabolic quality of fat tissue, not just quantity.
Q: How quickly can adipokine profiles improve with lifestyle changes? A: Adiponectin levels and inflammatory markers can improve within weeks to months of sustained physical activity and dietary improvement, though complete restoration takes longer.
Q: Are adipokine biomarkers currently available in clinical practice? A: Some adipokines (particularly adiponectin and inflammatory cytokines) are measurable in specialized labs. However, comprehensive adipokine profiling isn't yet standard clinical practice but is emerging in research settings.
Q: Is adipose tissue dysfunction reversible? A: In most cases, yes—particularly in earlier stages. Restoration of normal adipokine patterns can occur with sustained lifestyle modification or appropriate pharmacotherapy.
Q: What's the connection between adipokines and insulin resistance? A: Dysfunctional adipose tissue produces fewer protective molecules (adiponectin) while increasing inflammatory adipokines. These changes directly impair insulin signaling in liver, muscle, and adipose tissue.
Q: Can diet influence adipokine production? A: Absolutely. Diets rich in whole grains, fiber, and unsaturated fats promote healthy adipokine profiles, while ultra-processed foods and excess sugar worsen adipose dysfunction.
Clinical pearls
1. The "Quality over Quantity" Rule
In the world of fat tissue, function matters more than volume. You can be at a "normal" weight but still have "sick" fat (adipose tissue dysfunction) that secretes inflammatory markers. Conversely, healthy fat cells that are small and insulin-sensitive act as a protective endocrine organ.
The Pearl: Don't just chase a number on the scale; focus on metabolic markers like blood sugar and waist circumference, which are better indicators of how your fat is "behaving."
2. Adiponectin: Your Internal "Fire Extinguisher"
Think of Adiponectin as your body’s natural anti-inflammatory. In healthy states, levels are high, keeping your arteries flexible and your insulin working well. As fat cells enlarge (hypertrophy), they "turn off" the production of this protector.
The Pearl: Exercise is one of the most potent ways to boost Adiponectin. It’s essentially a way to "re-program" your fat cells to start producing protective signals again.
3. The "Silent" Nature of Metabolic Inflammation
Unlike a swollen ankle or a sore throat, metabolic inflammation (driven by TNF-α and IL-6) is low-grade and invisible. It doesn't cause pain, but it acts like "sand in the gears" of your cardiovascular system, slowly scratching the lining of your arteries (endothelial dysfunction).
The Pearl: Because you can’t "feel" metabolic inflammation, regular screening of high-sensitivity C-reactive protein (hs-CRP) can provide a "weather report" for your internal inflammatory climate.
4. Adipocyte Hypertrophy and "Crosstalk"
When fat cells get too large, they become stressed and begin to leak inflammatory signals. These signals don't stay in the fat; they travel through the blood to talk to your heart, liver, and kidneys, telling them to become resistant to insulin and more prone to scarring.
The Pearl: Weight distribution is a key clue. Fat stored around the midsection (visceral fat) is much more likely to be "loud" and inflammatory than fat stored under the skin on the hips or legs.
5. The "Ratios" are the Future of Risk
Modern medicine is moving away from looking at just one number (like total cholesterol). We now look at the Leptin-to-Adiponectin ratio. Leptin signals "fullness" but can become inflammatory when too high, while Adiponectin protects.
The Pearl: A high ratio means your metabolic "brakes" (Adiponectin) are failing while your "gas pedal" for inflammation (Leptin) is stuck to the floor. Future heart health is about restoring that balance.
Author’s Note
This article reflects an evolving shift in clinical medicine—from viewing adipose tissue as a passive storage depot to recognizing it as a dynamic endocrine organ central to cardiometabolic health. The concept of adipokine imbalance provides a unifying framework linking insulin resistance, chronic inflammation, and cardiovascular disease across diverse patient populations, including those with normal body weight.
For clinicians, the key implication is a move beyond weight-centric assessment toward functional evaluation of adipose tissue. Traditional markers such as BMI and LDL cholesterol, while useful, may fail to capture early metabolic dysfunction. Incorporating measures like waist circumference, hs-CRP, fasting insulin, and—where feasible—adipokine profiling can enhance early detection and risk stratification.
Equally important is the recognition that adipose dysfunction is modifiable. Lifestyle interventions—particularly structured exercise, dietary quality, sleep optimization, and stress regulation—remain first-line therapies with robust evidence for improving adipokine balance and reducing systemic inflammation. Pharmacological agents such as GLP-1 receptor agonists and SGLT2 inhibitors further expand our ability to target underlying metabolic pathways, not merely symptoms.
This synthesis is grounded in current peer-reviewed literature; however, adipokine biology remains a rapidly advancing field. Emerging biomarkers and therapeutic targets—such as adiponectin modulation and Netrin-1 signaling—hold promise but require further validation before routine clinical integration.
Clinical takeaway: Prioritize adipose tissue health, not just body weight. Early identification and targeted intervention can meaningfully alter the trajectory of cardiometabolic disease.
Medical Disclaimer: This article is written for educational and informational purposes only. It does not constitute medical advice and should not be used to replace consultation with a qualified healthcare provider. Individual health circumstances vary. Always discuss diagnostic testing, treatment decisions, and lifestyle changes with your physician or care team.
Related Articles
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health | DR T S DIDWAL
Lower Blood Pressure Naturally: Evidence-Based Exercise Guide for Metabolic Syndrome | DR T S DIDWAL
Movement Snacks: How VILPA Delivers Max Health Benefits in Minutes | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
How Insulin Resistance Accelerates Cardiovascular Aging | DR T S DIDWAL
References
American College of Cardiology. (2025, August 31). Changes in biology of internal fat may be the leading cause of heart failure. ACC Press Releases. https://www.acc.org/About-ACC/Press-Releases/2025/08/28/17/46/Changes-in-Biology-of-Internal-Fat
Bou Matar, D., Zhra, M., Nassar, W. K., Altemyatt, H., Naureen, A., Abotouk, N., Elahi, M. A., & Aljada, A. (2025). Adipose tissue dysfunction disrupts metabolic homeostasis: Mechanisms linking fat dysregulation to disease. Frontiers in Endocrinology, 16, 1592683. https://doi.org/10.3389/fendo.2025.1592683
Gao, D., Bing, C., & Griffiths, H. R. (2025). Disrupted adipokine secretion and inflammatory responses in human adipocyte hypertrophy. Adipocyte, 14(1). https://doi.org/10.1080/21623945.2025.2485927
He, Z., Zhao, L., Liu, J., Zheng, W., Gong, C., Guo, L., & Liang, T. (2026). Adipokine-mediated crosstalk between metabolic dysregulation and inflammatory pathways. Pathology Research and Practice, 278, 156312. https://doi.org/10.1016/j.prp.2025.156312
Kishimoto, S., & Higashi, Y. (2025/2026). Recent advances and emerging perspectives in vascular and cardiovascular research: A 2025 update. Hypertension Research, 49, 1–12. https://doi.org/10.1038/s41440-025-02540-1
Koo, T. H., Leong, X. B., & Mohamed, M. (2025). Systematic review of advanced inflammatory markers as predictors of cardiovascular diseases. Research in Cardiovascular Medicine, 14(1), 8–14. https://doi.org/10.4103/rcm.rcm_35_24
Lin, J. C., & Tandar, C. E. (2026). Global patterns of visceral adiposity and cardiometabolic disease. Nature Reviews Endocrinology, 22, 8. https://doi.org/10.1038/s41574-025-01191-z
Mannino, F. (2025). Special issue "New insights into adipose tissue metabolic function and dysfunction, 3rd edition." International Journal of Molecular Sciences, 26(16), 7831. https://doi.org/10.3390/ijms26167831
Nazir, A., Nazir, A., Afzaal, U., Aman, S., Sadiq, S. U. R., Akah, O. Z., Jamal, M. S. W., & Hassan, S. Z. (2025). Advancements in biomarkers for early detection and risk stratification of cardiovascular diseases—A literature review. Health Science Reports, 8(5), e70878. https://doi.org/10.1002/hsr2.70878
Netala, V. R., Hou, T., Wang, Y., Zhang, Z., & Teertam, S. K. (2025). Cardiovascular biomarkers: Tools for precision diagnosis and prognosis. International Journal of Molecular Sciences, 26(7), 3218. https://doi.org/10.3390/ijms26073218
Ramos-Zavala, M. G., García-Galindo, J. J., Beltrán-Ramírez, A., Balleza-Alejandri, L. R., Peña-Durán, E., Huerta-Huerta, A., Rubio-Arellano, E. D., López-Murillo, L. D., Pascoe-Gonzalez, S., Campos-Bayardo, T. I., & Suárez-Rico, D. O. (2025). Opposing profiles of Netrin-1 and adiponectin in metabolic inflammation and insulin resistance. Frontiers in Pharmacology, 16, 1632956. https://doi.org/10.3389/fphar.2025.1632956
Tilg, H., Ianiro, G., Gasbarrini, A., & Adolph, T. E. (2025). Adipokines: Masterminds of metabolic inflammation. Nature Reviews Immunology, 25(4), 250–265. https://doi.org/10.1038/s41577-024-01103-8
Yang, K., Fang, Y., He, J., et al. (2026). Adipokine networks in diabetic kidney disease: Mechanistic insights and therapeutic implications. Lipids in Health and Disease. https://doi.org/10.1186/s12944-025-02851-9