hsCRP Explained: What Inflammation Means for Your Heart
Discover what hsCRP really means for heart disease and inflammation. Learn normal ranges, hidden risks, and proven ways to lower hsCRP naturally.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/24/202622 min read
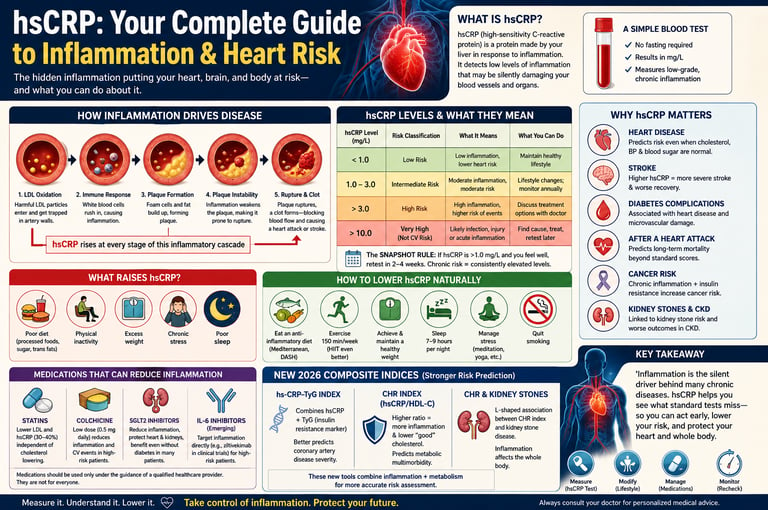
hsCRP (high-sensitivity C-reactive protein) is a blood marker that detects low-grade chronic inflammation linked to heart disease, stroke, diabetes, and metabolic dysfunction. Unlike standard cholesterol tests, hsCRP helps identify hidden cardiovascular risk even in people with normal LDL, blood pressure, and blood sugar. According to modern cardiology research, elevated hsCRP is now considered an independent predictor of heart attack and vascular disease risk.
What Does hsCRP Measure?
hsCRP measures low-grade inflammation associated with:
Heart disease and plaque instability
Stroke severity and recovery outcomes
Type 2 diabetes complications
Insulin resistance and metabolic syndrome
Chronic systemic inflammation
Residual cardiovascular risk despite normal cholesterol
Clinical Pearls: hsCRP, Inflammation & Heart Health
1. hsCRP reveals a hidden risk that cholesterol numbers often miss.
Even with normal cholesterol, blood pressure, and blood sugar, an hsCRP level above 2.0 mg/L signals ongoing vascular inflammation that can silently destabilize plaques and raise heart attack risk. The 2025 ACC Scientific Statement now recognizes this “residual inflammatory risk” as a key target in modern prevention.
2. One hsCRP test is only a snapshot — confirmation matters.
Because hsCRP can rise temporarily due to infections, intense exercise, or stress, a single elevated result should be repeated in 2–4 weeks. Consistently elevated levels (especially 1.0–3.0 mg/L or higher) indicate chronic inflammation worth addressing.
3. Women without classic risk factors still need hsCRP screening.
Approximately 5–10% of women have no smoking history, no hypertension, no diabetes, and normal cholesterol — yet elevated hsCRP. These “SMuRF-less but inflamed” women carry significantly higher heart attack and stroke risk that standard calculators miss. hsCRP is currently the best practical tool to identify them.
4. In diabetes, controlling inflammation is as important as controlling blood sugar.
Two patients with identical HbA1c and lipid profiles can have very different outcomes based on their hsCRP. Elevated hsCRP strongly predicts microvascular complications (eyes, kidneys, nerves) and macrovascular events, showing that inflammation drives diabetic damage beyond glucose alone.
5. Lifestyle changes meaningfully lower hsCRP — and the benefits are broad.
A Mediterranean-style diet, regular aerobic exercise (especially HIIT), 7–9 hours of quality sleep, stress reduction, and weight loss of just 5–10% can reduce hsCRP by 20–40% in many people. These same steps also improve metabolic health, lower cancer risk signals, and support overall longevity.
6. Statins do double duty — and sometimes more help is needed.
Statins lower both LDL cholesterol and hsCRP (by ~30–40%). However, if hsCRP remains elevated despite good cholesterol control, residual inflammatory risk persists. In high-risk patients, low-dose colchicine or other targeted therapies may be added after discussion with your cardiologist.
hsCRP: Your Complete Guide to Inflammation & Heart Risk
Imagine passing every standard heart health test with flying colors — normal cholesterol, healthy blood pressure, stable blood sugar — and still suffering a heart attack. This isn't a rare tragedy. It happens to millions of people every year, and a growing mountain of science now tells us why: chronic inflammation, measured by a blood marker called high-sensitivity C-reactive protein (hsCRP), is silently driving cardiovascular disease in people traditional screenings completely miss.
In 2025, the American College of Cardiology released a landmark scientific statement declaring inflammation an independent, central driver of heart disease — not a side effect, not a bystander, but a core mechanism (Mensah et al., 2025). By 2026, researchers had gone further, linking hsCRP to coronary artery disease severity, stroke outcomes, post-heart-attack survival, and even kidney stone formation through groundbreaking composite indices.
This guide gives you everything you need to understand hsCRP: what it measures, how to interpret your results, what the newest research reveals, and exactly what you can do to bring inflammation under control. Whether you're a patient reviewing a lab report or a clinician looking for the latest evidence, you'll find it here.
What you'll learn:
What hsCRP is and why it matters more than most doctors discuss
How to interpret your results (with a clear reference table)
Who is most at risk — including people traditional tests miss entirely
The 2025–2026 research that's reshaping cardiovascular prevention
Proven strategies to lower hsCRP through lifestyle and medicine
Answers to the questions people actually search for
1. What is ishsCRP? The Science Made Simple
C-reactive protein (CRP) is a protein your liver releases into the bloodstream whenever your immune system detects a threat — an infection, tissue injury, or ongoing irritation inside blood vessel walls. Think of it as a flare your body fires when something is wrong beneath the surface.
High-sensitivity CRP (hsCRP) is a more refined laboratory version of the standard CRP test. It detects extremely low concentrations of CRP — levels too small for the older test to catch — which is precisely what makes it useful for cardiovascular risk assessment. The inflammation that quietly damages arteries over years produces only modest CRP elevations. The standard CRP test misses them; hsCRP does not.
Why Inflammation Drives Heart Disease
Atherosclerosis — the gradual buildup of plaques inside artery walls — is not simply a plumbing problem caused by excess cholesterol. It is a biological immune response. When LDL cholesterol particles become oxidized and lodge in artery walls, the immune system mounts an inflammatory response: white blood cells infiltrate the vessel wall, foam cells accumulate, and inflammatory cytokines keep the process going. Over time, inflammation makes plaques unstable and prone to rupture. A ruptured plaque triggers a clot, and a clot in a coronary artery causes a heart attack.
hsCRP reflects this entire inflammatory cascade. Elevated levels signal that this process is active — even when cholesterol numbers look acceptable.
2. How hsCRP Is Measured and What Your Results Mean
hsCRP is measured through a simple blood test. Fasting is generally not required, though avoiding vigorous exercise and illness in the 24 hours before testing improves accuracy.
hsCRP Reference Ranges for Cardiovascular Risk
Low Cardiovascular Risk: hs-CRP Less than 1.0 mg/L
Clinical Status: Optimal baseline; minimal systemic vascular inflammation detected.
Recommended Action: Maintain current heart-healthy lifestyle habits, balanced nutrition, and regular physical activity.
Intermediate (Moderate) Cardiovascular Risk: hs-CRP 1.0 to 3.0 mg/L
Clinical Status: Moderate systemic inflammation; early endothelial signaling or subclinical metabolic stress.
Recommended Action: Implement targeted lifestyle modifications (dietary adjustments, visceral fat reduction, stress management) and monitor levels annually.
High Cardiovascular Risk: hs-CRP Greater than 3.0 mg/L
Clinical Status: Advanced systemic vascular inflammation; heightened risk of atherogenesis (plaque buildup) and cardiovascular events.
Recommended Action: Discuss targeted cardioprotective interventions, advanced lipid testing, and metabolic optimization strategies with your doctor.
Acute Phase / Non-Specific Inflammation: hs-CRP Greater than 10.0 mg/L
Clinical Status: Massive inflammatory spike; highly indicative of an active acute infection, recent physical trauma, or systemic autoimmune flare-up rather than purely cardiovascular risk.
Recommended Action: Investigate underlying non-cardiac causes first; allow the acute event to resolve completely, and schedule a retest in 2 to 4 weeks to establish a true vascular baseline.
(Source: American Heart Association / ACC guidelines)
The "Snapshot" Rule — Why One Test Isn't Enough
hsCRP is highly sensitive, which is both its strength and its limitation. A single elevated reading could reflect a recent cold, intense exercise, poor sleep, or stress. Chronic cardiovascular inflammation, by contrast, produces a sustained, low-grade elevation — not a spike.
Best practice: If your hsCRP is above 1.0 mg/L and you feel well, retest in 2–4 weeks. Two consistently elevated readings confirm a chronic inflammatory state worth addressing.
3. hsCRP and Heart Disease: The 2025 ACC Scientific Statement
The most authoritative document shaping clinical practice right now is the 2025 ACC Scientific Statement on Inflammation and Cardiovascular Disease by Mensah and colleagues. This statement consolidates decades of research into a clear clinical directive: inflammation is not an optional consideration in cardiovascular prevention — it is central to it.
Key Conclusions of the 2025 ACC Statement
Inflammation is an independent driver of cardiovascular disease, separate from cholesterol, blood pressure, and blood sugar
hsCRP testing offers measurable clinical value for risk stratification beyond traditional scores like the Framingham Risk Score or Pooled Cohort Equations
Healthcare providers should integrate hsCRP into treatment decisions for at-risk populations
Addressing residual inflammatory risk — the elevated hsCRP that persists even after optimal LDL control — is now considered a priority in preventive cardiology
What "Residual Inflammatory Risk" Means for You
Achieving your LDL target with a statin is important. But if your hsCRP remains above 2.0 mg/L despite good cholesterol control, research shows your risk for a future cardiac event remains substantially elevated. This is the concept of residual inflammatory risk — and it explains why some statin-treated patients still have heart attacks.
Addressing residual risk requires a dual-pathway approach: lowering both lipids and inflammation simultaneously.
4. Women Without Risk Factors: The "SMuRF-Less but Inflamed" Paradox
One of the most clinically important findings of 2025 comes from a study by Ridker and colleagues in the European Heart Journal. The research examined women with no standard modifiable risk factors (SMuRFs) — no high cholesterol, no hypertension, no diabetes, no smoking history — who nonetheless showed elevated hsCRP.
What the Research Found
Approximately 5–10% of women have no conventional cardiovascular risk factors but carry elevated hsCRP
These women face significantly higher rates of heart attack and stroke compared to women with low CRP and no risk factors
Standard risk calculators give these women a falsely reassuring "low risk" score, completely missing their true danger
hsCRP testing is the only practical tool currently available to identify this hidden high-risk group
Clinical Meaning
This research dismantles the assumption that a clean lipid panel equals a healthy cardiovascular system. For women in particular — who already face a historical under-diagnosis gap in heart disease — this finding has immediate practical consequences: every woman should be considered for hsCRP testing, especially those who feel healthy by conventional standards.
5. hsCRP in Type 2 Diabetes: Beyond Blood Sugar Control
Type 2 diabetes doubles cardiovascular risk independent of cholesterol. But what's driving that excess risk? A 2025 study by Basil and colleagues, along with a comprehensive mechanistic review by Stanimirovic et al. (2022), points clearly to chronic systemic inflammation as the connecting thread.
The Diabetes-Inflammation Connection
Patients with type 2 diabetes have systematically higher hsCRP levels than non-diabetic populations
Elevated hsCRP in diabetics predicts cardiovascular events even after controlling for HbA1c and lipid levels — meaning inflammation adds independent risk information that blood sugar markers don't capture
Type 2 diabetes is itself a state of chronic low-grade inflammation: insulin resistance promotes inflammatory cytokine release, and those cytokines worsen insulin resistance, creating a destructive cycle
In a 2025 study by Dhadwad and Yadav, elevated hsCRP strongly associated with microvascular complications — diabetic retinopathy, nephropathy, and neuropathy — suggesting inflammation harms small vessels long before standard lab values signal a problem
The Practical Implication
Two patients with identical HbA1c values and identical lipid profiles can have very different cardiovascular risk profiles based solely on their hsCRP levels. Glycemic control is necessary but not sufficient. Inflammatory status is an equally important target in diabetes management.
6. New 2026 Research: Composite Indices That Predict Risk Better
The field of inflammatory biomarkers moved significantly in 2026, with researchers developing and validating composite indices that combine hsCRP with other metabolic markers for superior risk prediction.
The hs-CRP/TyG Index: Coronary Artery Disease Severity
A 2026 retrospective study by Yang and colleagues published in Frontiers in Endocrinology examined the hs-CRP-TyG index — a novel combination of hsCRP and the Triglyceride-Glucose (TyG) index, itself a surrogate marker for insulin resistance.
Key findings:
The hs-CRP-TyG index predicted not just the presence of coronary artery disease but its angiographic severity — how many vessels were involved and how badly they were obstructed
The combined index outperformed the TyG index alone, demonstrating that layering inflammation data onto metabolic data produces meaningfully better risk discrimination
This index may eventually help clinicians decide which patients need earlier or more aggressive coronary intervention
The hs-CRP/HDL-C Ratio (CHR Index): Cardiovascular Metabolic Multimorbidity
Chen and colleagues (2026) published a large cross-sectional study in Scientific Reports examining the hs-CRP/HDL-C ratio, also called the CHR index. This ratio captures a dual burden: rising inflammation (hsCRP up) combined with falling cardioprotective HDL (HDL-C down).
Key findings:
Higher CHR index values were significantly associated with cardiovascular metabolic multimorbidity — the simultaneous presence of multiple conditions including heart disease, diabetes, and metabolic syndrome
The relationship was dose-dependent: as the CHR index rose, the number of concurrent cardiometabolic conditions increased
CHR may prove more useful than either hsCRP or HDL-C alone for identifying patients with complex, overlapping metabolic disease
The CHR Index and Kidney Stone Disease
A surprising 2026 finding from Shi and colleagues, published in The Aging Male, revealed an L-shaped association between the CHR index and kidney stone disease in U.S. adults. Below a threshold CHR value, rising inflammation and declining HDL correlated with increased kidney stone risk. Above that threshold, the association plateaued.
This finding illustrates the systemic reach of the inflammatory state: the same metabolic-inflammatory imbalance that damages coronary arteries also contributes to urological disease — underscoring why addressing hsCRP has benefits that extend well beyond cardiovascular prevention.
7. hsCRP and Stroke: What the Newest Data Shows
Beyond coronary artery disease, a 2026 retrospective cohort study by Bhatt and colleagues, published in BMC Neurology, investigated how hsCRP and D-Dimer levels at hospital admission relate to stroke severity and early functional outcomes in ischemic stroke patients.
Key Findings
Higher admission hsCRP levels correlated with greater stroke severity (measured by NIHSS scores) on arrival
Elevated hsCRP independently predicted worse early functional outcomes, including greater disability at discharge
The association was particularly pronounced in older age groups, suggesting age-related inflammatory baseline elevation compounds stroke injury
Combined hsCRP and D-Dimer assessment provided additive prognostic information — together, they created a clearer picture of acute inflammatory burden than either marker alone
What This Means
hsCRP is not just a risk marker you measure before disease occurs. In the acute setting, it reflects the severity of the inflammatory response to vascular injury — and that response determines how much brain tissue survives. This research adds another dimension to the case for keeping baseline inflammation low: lower pre-stroke hsCRP may translate to less severe strokes and better recovery.
8. hsCRP After a Heart Attack: Mortality Prediction Beyond GRACE
The GRACE score (Global Registry of Acute Coronary Events) is the standard tool for predicting long-term mortality in patients who have had a heart attack and undergone percutaneous coronary intervention (PCI). But according to a 2026 study presented at the American College of Cardiology Scientific Sessions by Hyun, Chang, and Lee, hsCRP significantly improves long-term mortality prediction beyond what GRACE alone provides.
Key Findings
In a landmark 1-year landmark analysis of PCI-treated myocardial infarction survivors, high hsCRP at 1 year post-MI independently predicted long-term mortality
Adding hsCRP to the GRACE score produced statistically significant improvement in mortality discrimination — meaning clinicians could better identify which survivors were at highest risk for a second fatal event
This positions hsCRP as a valuable post-MI surveillance tool, not just a pre-event screening marker
Clinical Implication
For patients recovering from a heart attack, periodic hsCRP testing alongside standard follow-up may identify those with persistent residual inflammatory risk — the patients who most need intensification of anti-inflammatory therapy rather than routine maintenance care.
9. Microvascular Damage, Cancer Risk, and the Systemic Reach of Inflammation
Elevated hsCRP doesn't threaten only the heart and brain. A growing body of research reveals its implications across multiple organ systems.
Microvascular Complications in Diabetes
Dhadwad and Yadav (2025) demonstrated that among diabetic patients, hsCRP levels above 3 mg/L were strongly associated with established microvascular complications — damage to the tiny blood vessels supplying the eyes, kidneys, and nerves. Crucially, hsCRP predicted these complications even in patients whose glucose levels appeared controlled, confirming that inflammation — not hyperglycemia alone — is a primary driver of diabetic tissue injury.
The Cancer Connection
A 2025 longitudinal cohort study by Zheng and colleagues published in BMC Public Health traced the temporal relationship between chronic inflammation, insulin resistance, and cancer risk. Their findings were striking:
The combination of elevated hsCRP and insulin resistance increased cancer risk beyond what either factor predicted independently
Chronic inflammation and insulin resistance appear to reinforce each other over time, creating a vicious cycle that eventually raises cancer susceptibility
This suggests that anti-inflammatory interventions targeting hsCRP may contribute to multi-disease prevention — reducing cardiovascular risk and cancer risk simultaneously
Systemic Inflammation in U.S. Patients with Atherosclerosis
The PLUTUS study (Lv et al., 2025) provided a critical reality check: despite widespread use of statins and other cardiovascular medications, a substantial proportion of U.S. patients with established atherosclerotic disease still carry test-confirmed systemic inflammation (hsCRP > 2.0 mg/L). The burden was highest among patients who also had chronic kidney disease — a combination that creates a synergistic inflammatory environment, dramatically elevating cardiovascular event risk. Standard therapy, in other words, is not enough for a large share of real-world patients.
10. How to Lower Your hsCRP: Evidence-Based Strategies
The good news: inflammation is modifiable. Multiple lifestyle interventions have demonstrated meaningful, measurable reductions in hsCRP.
Diet: The Anti-Inflammatory Plate
Mediterranean Diet Consistently the best-studied dietary pattern for reducing hsCRP. Emphasizes olive oil, fatty fish, vegetables, legumes, whole grains, nuts, and limited red meat. Meta-analyses show adherence to the Mediterranean diet reduces hsCRP by an average of 20–30%.
DASH Diet Originally designed for blood pressure, DASH (Dietary Approaches to Stop Hypertension) also reduces inflammatory markers through its emphasis on fruits, vegetables, low-fat dairy, and whole grains with restricted sodium and saturated fat.
Foods to Emphasize:
Fatty fish (salmon, sardines, mackerel): rich in omega-3 fatty acids, which directly suppress inflammatory cytokines
Berries, leafy greens, and cruciferous vegetables: high antioxidant polyphenol content
Extra virgin olive oil: oleocanthal has ibuprofen-like anti-inflammatory activity
Nuts (especially walnuts): omega-3 and polyphenol content
Turmeric/curcumin: inhibits NF-κB, a master inflammatory regulator
Foods to Minimise:
Ultra-processed foods and refined carbohydrates
Sugary beverages (including fruit juices)
Trans fats and excessive saturated fat
Excessive alcohol
Exercise
Regular aerobic exercise is one of the most reliable non-pharmacological ways to reduce hsCRP. Research supports the following:
150 minutes per week of moderate aerobic activity (brisk walking, cycling, swimming) reduces hsCRP significantly over 8–12 weeks
High-Intensity Interval Training (HIIT) appears particularly effective for CRP reduction, with some studies showing 30–40% decreases
Resistance training also contributes, especially for patients with metabolic syndrome or obesity
Sedentary behaviour independently raises CRP — breaking up prolonged sitting matters even on days you exercise
Weight Management
Adipose tissue — especially visceral fat around abdominal organs — is metabolically active, constantly secreting inflammatory cytokines including IL-6, which drives CRP production. Even 5–10% weight loss produces measurable reductions in hsCRP, independent of diet composition.
Sleep
Chronic sleep deprivation (under 6 hours nightly) elevates inflammatory markers. 7–9 hours per night supports healthy immune regulation and is associated with lower baseline CRP. Treating obstructive sleep apnea — a powerful driver of nocturnal hypoxia-induced inflammation — can meaningfully reduce hsCRP.
Stress Management
Chronic psychological stress activates the hypothalamic-pituitary-adrenal axis and sympathetic nervous system, both of which promote inflammatory signaling. Mindfulness-based stress reduction (MBSR), meditation, yoga, and cognitive behavioral therapy have each demonstrated CRP-lowering effects in clinical trials.
Smoking Cessation
Smoking is a direct, potent driver of systemic inflammation. Cessation reduces hsCRP within weeks and continues to decline for years afterwards.
11. Medications That Reduce Inflammation
When lifestyle measures are insufficient, several pharmacological options target inflammation directly or have anti-inflammatory effects as a secondary benefit.
Statins
Statins (atorvastatin, rosuvastatin, etc.) lower LDL cholesterol but also have pleiotropic anti-inflammatory effects. They reduce hsCRP by approximately 30–40% independent of their lipid-lowering action. The JUPITER trial demonstrated that rosuvastatin dramatically reduced cardiovascular events specifically in people with normal LDL but elevated hsCRP — one of the most powerful validations of the hsCRP concept in clinical medicine.
Low-Dose Colchicine
Originally used for gout, colchicine at low doses (0.5 mg daily) has emerged as a targeted anti-inflammatory cardiovascular agent. The COLCOT and LoDoCo2 trials demonstrated significant reductions in cardiovascular events in patients with recent MI or stable coronary artery disease.
Important cautions: Colchicine should be used with caution or avoided in patients with significant kidney or liver impairment, or those taking strong CYP3A4 or P-glycoprotein inhibitors. It is not appropriate for low-risk individuals or as a standalone preventive measure.
SGLT2 Inhibitors
Originally diabetes medications (empagliflozin, dapagliflozin, canagliflozin), SGLT2 inhibitors reduce systemic inflammation through multiple mechanisms, including reduced oxidative stress and favorable metabolic effects. They are now approved for heart failure and CKD regardless of diabetic status, and consistently reduce inflammatory markers in trial data.
Emerging: IL-6 Inhibitors
Agents targeting the IL-6 inflammatory pathway — particularly ziltivekimab — are in late-stage clinical trials for high-risk cardiovascular patients with chronic kidney disease and elevated hsCRP. Early results are promising, offering potent CRP reduction in a population where current therapies leave substantial residual inflammatory risk.
12. Recent Clinical Trials & Evidence:
1 .hs-CRP in Cardiovascular and Metabolic Risk (2025–2026)
Mensah et al. (American College of Cardiology, 2025)
Study Focus: General & Clinical Guidance Update.
Key Finding: Confirmed that chronic inflammation acts as a central, fully independent driver of cardiovascular disease (CVD).
Clinical Relevance: Establishes the medical foundation for using high-sensitivity C-reactive protein (hs-CRP) as a primary risk stratification biomarker in standard practice.
Study Focus: Apparently healthy women without standard cardiovascular risk factors.
Key Finding: Roughly 5% to 10% of seemingly "low-risk" women exhibit significantly elevated hs-CRP levels alongside high cardiovascular risk.
Clinical Relevance: Demonstrates that routine hs-CRP screening is essential for women, as traditional lipid panels miss a critical window of inflammatory risk.
Study Focus: General Population Cohort.
Key Finding: Chronic system inflammation combined with insulin resistance multiplicatively accelerates and raises long-term cancer risks.
Clinical Relevance: Proves that aggressive anti-inflammatory management offers multi-disease preventative benefits extending far beyond cardiology.
2. Diabetes, Insulin Resistance, and Microvascular Complications
Study Focus: Patients diagnosed with Type 2 Diabetes (T2D).
Key Finding: Elevated hs-CRP accurately predicts future adverse cardiovascular events even when blood sugar ($HbA1c$) and lipid panels are perfectly controlled.
Clinical Relevance: Highlights the need to add baseline hs-CRP testing to routine diabetic cardiovascular assessments.
Study Focus: Diabetic Patient Cohort.
Key Finding: High hs-CRP levels directly correlate with the onset and progression of diabetic microvascular complications (organ damage).
Clinical Relevance: Confirms that systemic inflammation drives diabetic end-organ damage independently of ambient blood glucose levels.
3. Atherosclerosis, Real-World Treatment Gaps, & Post-MI Care
Lv et al. (PLUTUS Trial, 2025)
Study Focus: United States Atherosclerosis Patients.
Key Finding: A massive subset of patients undergoing standard guideline-directed medical therapy still exhibit persistently elevated hs-CRP.
Clinical Relevance: Highlights a major residual inflammatory treatment gap in real-world clinical cardiology care.
Study Focus: Myocardial Infarction (Heart Attack) Survivors treated with PCI (stenting).
Key Finding: Evaluating hs-CRP levels 1 year post-infarction significantly improves long-term mortality tracking compared to using the traditional GRACE score alone.
Clinical Relevance: Validates hs-CRP as a critical monitoring biomarker during long-term post-MI follow-up appointments.
4. Advanced Composite Biomarkers and Novel Risk Indices
Study Focus: Coronary Angiography Patients.
Key Finding: The hs-CRP-TyG index (combining inflammation with the Triglyceride-Glucose index) predicts the true severity of coronary artery disease (CAD) far better than the TyG index alone.
Clinical Relevance: Introduces a powerful, accessible composite index for highly accurate advanced coronary risk stratification.
Study Focus: Large Cross-Sectional Cohort.
Key Finding: The CHR ratio (C-reactive protein to High-Density Lipoprotein Cholesterol ratio) effectively predicts the onset of cardiometabolic multimorbidity.
Clinical Relevance: Provides clinicians with a single, highly efficient calculation to capture dual metabolic and inflammatory burdens simultaneously.
Study Focus: U.S. Adult Population.
Key Finding: Identified a distinct L-shaped association between the CHR ratio and the incidence of kidney stones.
Clinical Relevance: Demonstrates that systemic vascular inflammation directly influences broader urological and metabolic health.
5. Acute Neurovascular Events
Study Focus: Ischemic Stroke Patients.
Key Finding: High hs-CRP measurements upon hospital admission accurately predict increased stroke severity and poorer functional outcomes.
Clinical Relevance: Suggests that keeping pre-stroke baseline inflammation low directly preserves neurological recovery potential.
13. Common Myths and Mistakes About hsCRP
Myth 1: "My cholesterol is normal, so I don't need to worry about inflammation."
False. The JUPITER trial and the 2025 ACC statement both confirm that normal LDL with elevated hsCRP still confers substantial cardiovascular risk. These two pathways are independent.
Myth 2: "A high hsCRP always means heart disease."
Not necessarily. Levels above 10 mg/L usually indicate an acute infection, injury, or autoimmune flare — not chronic cardiovascular inflammation. Cardiovascular risk is assessed in the 1–3 mg/L range, and only after excluding acute illness.
Myth 3: "If I lower my cholesterol with a statin, my inflammation will take care of itself."
Partially true, but not reliably. Statins reduce hsCRP in many patients, but not all. Some patients achieve excellent LDL control while maintaining elevated hsCRP — their residual inflammatory risk remains high and may require additional intervention.
Myth 4: "hsCRP testing is only for sick people."
Incorrect. The strongest case for hsCRP testing is precisely in people who appear healthy by conventional standards — particularly women with no traditional risk factors and people in the intermediate-risk category where testing tips the decision on whether to begin preventive therapy.
Myth 5: "One hsCRP test tells me everything I need to know."
A single elevated reading is a starting point, not a conclusion. hsCRP fluctuates with minor infections, exercise, and stress. Confirm chronic elevation with a second test 2–4 weeks later.
Myth 6: "I can ignore inflammation if I eat well."
Diet is important, but for some individuals — particularly those with genetic predispositions to inflammation, autoimmune conditions, or established disease — lifestyle changes alone may not normalize hsCRP. Medical evaluation is essential.
14. FAQs
Q: Should everyone get an hsCRP test?
The 2025 ACC statement recommends hsCRP testing for people with borderline cardiovascular risk, those with established risk factors, and women without conventional risk markers. It is not universally recommended for all adults, but the bar for testing is lower than many clinicians currently apply — especially given the evidence on inflamed-but-otherwise-healthy individuals. Ask your doctor whether it's appropriate for you.
Q: What is a good hsCRP level?
Below 1.0 mg/L is considered low cardiovascular risk. The ideal target — particularly if you have known risk factors — is below 2.0 mg/L. Some anti-inflammatory interventions (colchicine, statins in high-risk patients) aim to bring levels below 1.0 mg/L.
Q: Can I lower my hsCRP without medication?
Yes. A Mediterranean or DASH diet, regular aerobic exercise (especially HIIT), adequate sleep (7–9 hours), stress management, weight loss, and smoking cessation each independently reduce hsCRP. Many people achieve significant reductions through lifestyle changes alone, particularly if baseline elevation is modest.
Q: Does hsCRP go up with exercise?
Acutely, yes. Intense or prolonged exercise temporarily elevates CRP for 24–48 hours as part of normal muscle repair. Chronically, however, regular moderate exercise consistently lowers baseline hsCRP. This is why you should avoid strenuous exercise before your hsCRP blood draw.
Q: What is the hs-CRP/HDL-C ratio (CHR index) and should I ask for it?
The CHR index, studied in 2026 by Chen et al., divides your hsCRP level by your HDL cholesterol level. A higher ratio reflects both greater inflammation and lower cardioprotective cholesterol — a double disadvantage. While it's not yet standard of care, it may provide additional insight if your doctor is evaluating cardiometabolic risk. You can calculate it yourself if you have both values from a standard lipid panel and hsCRP test.
Q: Is elevated hsCRP dangerous during pregnancy?
Mildly elevated CRP is common during normal pregnancy due to physiological immune changes. However, significantly elevated hsCRP has been associated with increased risk of complications, including preeclampsia and preterm birth. Discuss any elevated results with your obstetrician.
Q: How does hsCRP differ from the standard CRP test?
Both measure the same protein, but hsCRP uses a more sensitive assay capable of detecting concentrations below 3–5 mg/L — the range relevant to cardiovascular risk. The standard CRP test was designed to detect acute infection and inflammation (typically >10 mg/L), and it cannot see the low-grade elevations relevant to heart disease.
Q: Does colchicine actually work for heart disease?
Yes. The COLCOT trial (2019) and LoDoCo2 trial (2020) both demonstrated statistically significant reductions in major adverse cardiovascular events with 0.5 mg daily colchicine in post-MI and stable CAD patients, respectively. It is now incorporated into several cardiovascular guidelines as an option for high-risk patients with residual inflammatory risk. It is not appropriate for everyone — discuss with your cardiologist.
Q: How often should I retest hsCRP?
There is no universal standard. For people on interventions (lifestyle changes, statins, or anti-inflammatory therapy), retesting at 3–6 months assesses response. For monitoring in stable, at-risk individuals not yet on specific therapy, annual testing is reasonable. Your doctor should guide the frequency based on your clinical situation.
Q: Can hsCRP predict stroke risk?
Yes. Research has consistently shown that elevated hsCRP predicts first ischemic stroke independent of traditional vascular risk factors. The 2026 study by Bhatt and colleagues added a further layer: in patients who have already had a stroke, higher admission hsCRP is associated with worse neurological severity and poorer early functional recovery. This strengthens the case for maintaining low baseline hsCRP as a neuroprotective strategy.
Q: What's the connection between hsCRP and the TyG index?
The TyG (Triglyceride-Glucose) index is a well-validated surrogate marker for insulin resistance — calculated from fasting triglyceride and glucose values. Combining it with hsCRP into the hs-CRP-TyG index (Yang et al., 2026) creates a composite that captures both insulin resistance and systemic inflammation simultaneously. In a coronary angiography study, this combined index predicted the severity of coronary artery disease more accurately than either marker alone, suggesting that the metabolic-inflammatory intersection is especially dangerous.
Q: Are anti-inflammatory diets safe for everyone?
Generally, yes. A Mediterranean or plant-rich anti-inflammatory diet is safe and beneficial for the vast majority of adults. However, people on certain medications (e.g., warfarin, where high vitamin K foods require consistent intake) should consult their doctor before making large dietary shifts. Specific supplements like high-dose fish oil or turmeric may interact with blood thinners.
15. Conclusion and Action Steps
The science is unambiguous: hsCRP is a window into your true cardiovascular health that no standard blood panel currently opens. It reveals inflammation that persists despite normal cholesterol, drives heart attacks in "healthy" women, accelerates diabetic complications, worsens stroke outcomes, predicts post-MI mortality, and connects to cancer risk — all through the same fundamental mechanism of chronic systemic inflammation.
The 2025 ACC statement legitimized hsCRP as a mainstream clinical tool. The 2026 research — on composite indices like the hs-CRP-TyG and CHR, post-MI surveillance, and stroke outcomes — is expanding its utility further. If you are not yet having this conversation with your doctor, now is the time to start.
Your Action Plan
Talk to your doctor about whether hsCRP testing is appropriate for your situation — especially if you are a woman without obvious risk factors, have type 2 diabetes, have a family history of early heart disease, or fall into the "intermediate risk" category on standard risk scores.
If elevated, retest in 2–4 weeks after excluding acute illness or recent intense exercise. Chronic elevation warrants a management plan.
Prioritize anti-inflammatory lifestyle changes — Mediterranean diet, regular aerobic exercise, 7–9 hours of sleep, stress management, healthy weight, and no smoking. These lower hsCRP measurably and have zero side effects.
Ask about your full cardiometabolic picture — request a lipid panel including HDL-C alongside hsCRP so your doctor can calculate the CHR index if appropriate.
Don't settle for cholesterol control alone — if you are on a statin and have risk factors, ask specifically whether your hsCRP has been measured. Residual inflammatory risk is a treatable problem, not an inevitability.
Post-heart attack or stroke patients: Ask your cardiologist or neurologist about incorporating hsCRP into your follow-up surveillance. New evidence from 2026 shows it adds predictive information beyond standard scoring tools.
Inflammation is not fate. It is measurable, modifiable, and manageable. Start the conversation today.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Beyond Cholesterol: Life-Saving Latest Blood Tests to Prevent Heart Attacks | DR T S DIDWAL
References
Basil, B., Mohammed, J. A., Mba, I. N., et al. (2025). High-sensitivity c-reactive protein and cardiovascular disease risk assessment in a population of type 2 diabetes mellitus patients. BMC Cardiovascular Disorders, 25, Article 498. https://doi.org/10.1186/s12872-025-04975-3
Bhatt, S. P., Chang, H., Joshi, P. K., et al. (2026). Associations of hs-CRP and D-Dimer with stroke severity and early functional outcomes in ischemic stroke: A retrospective age-stratified cohort study. BMC Neurology, 26, Article 254. https://doi.org/10.1186/s12883-026-04797-6
Chen, B., Han, L., Meng, T., et al. (2026). Associations of the hs-CRP/HDL-C ratio with cardiovascular metabolic multimorbidity: A large cross-sectional study. Scientific Reports, 16, Article 13371. https://doi.org/10.1038/s41598-026-43849-2
Dhadwad, J., & Yadav, P. (2025). Association of hsCRP levels with microvascular complications in diabetic patients. Journal of Clinical and Diagnostic Research, 19(9), OC15–OC18. https://doi.org/10.7860/JCDR/2025/79982/21517
Hyun, S., Chang, K., & Lee, K. (2026). HS-CRP improves long-term mortality prediction beyond GRACE in PCI-treated MI survivors: A 1-year landmark analysis. Journal of the American College of Cardiology, 87(13_Supplement), A794. https://doi.org/10.1016/j.jacc.2026.02.2050
Libby, P., Ridker, P. M., & Maseri, A. (2002). Inflammation and atherosclerosis. Circulation, 105(9), 1135–1143. https://doi.org/10.1161/hc0902.104353
Lv, L., Rajpura, J., Liu, M., Strum, M., Chastek, B., Johnson, J., & Gluckman, T. J. (2025). Prevalence and clinical characteristics of patients with hsCRP testing and test-confirmed systemic inflammation among individuals with atherosclerotic cardiovascular disease with or without chronic kidney disease in the United States (PLUTUS). American Journal of Preventive Cardiology, 21, Article 100950. https://doi.org/10.1016/j.ajpc.2025.100950
Mensah, G. A., Arnold, N., Prabhu, S. D., Ridker, P. M., & Welty, F. K. (2025). Inflammation and cardiovascular disease: 2025 ACC scientific statement. Journal of the American College of Cardiology. Advance online publication. https://doi.org/10.1016/j.jacc.2025.08.047
Nidorf, S. M., Fiolet, A. T. L., Mosterd, A., et al. (2020). Colchicine in patients with chronic coronary disease (LoDoCo2). New England Journal of Medicine, 383(19), 1838–1847. https://doi.org/10.1056/NEJMoa2021372
Pearson, T. A., Mensah, G. A., Alexander, R. W., et al. (2003). Markers of inflammation and cardiovascular disease: Application to clinical and public health practice. Circulation, 107(3), 499–511. https://doi.org/10.1161/01.CIR.0000052939.59093.45
Ridker, P. M., Danielson, E., Fonseca, F. A. H., et al. (2008). Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein (JUPITER). New England Journal of Medicine, 359(21), 2195–2207. https://doi.org/10.1056/NEJMoa0807646
Ridker, P. M., Figtree, G. A., Moorthy, M. V., Mora, S., & Buring, J. E. (2025). C-reactive protein and cardiovascular risk among women with no standard modifiable risk factors: Evaluating the 'SMuRF-less but inflamed'. European Heart Journal, Article ehaf658. https://doi.org/10.1093/eurheartj/ehaf658
Shi, B., Yuan, W., Liu, S., Dai, Y., Sun, X., & Jia, Y. (2026). An L-shaped curve relating Hs-CRP/HDL-C (CHR) index to kidney stone disease (KSD) in US adult participants: A cross-sectional study. The Aging Male, 29(1), Article 2650010. https://doi.org/10.1080/13685538.2026.2650010
Stanimirovic, J., Radovanovic, J., Banjac, K., Obradovic, M., Essack, M., Zafirovic, S., Gluvic, Z., Gojobori, T., & Isenovic, E. R. (2022). Role of C-reactive protein in diabetic inflammation. Mediators of Inflammation, 2022, Article 3706508. https://doi.org/10.1155/2022/3706508
Tardif, J. C., Kouz, S., Waters, D. D., et al. (2019). Efficacy and safety of low-dose colchicine after myocardial infarction (COLCOT). New England Journal of Medicine, 381(26), 2497–2505. https://doi.org/10.1056/NEJMoa1912388
Yang, M., Hu, L., Liu, T., Yi, Y., & Xu, Y. (2026). Association of the hs-CRP-TyG index with coronary artery disease risk and angiographic severity: A retrospective comparative study with the TyG index. Frontiers in Endocrinology, 17, Article 1836149. https://doi.org/10.3389/fendo.2026.1836149
Zheng, X., Wang, Y., Chen, Y., et al. (2025). Temporal relationship between chronic inflammation and insulin resistance and their combined cumulative effect on cancer risk: A longitudinal cohort study. BMC Public Health, 25, Article 1501. https://doi.org/10.1186/s12889-025-22632-4