Cardiovascular Inflammaging: Understanding How Chronic Inflammation Ages Your Heart
Chronic inflammation (inflammaging) is an independent heart disease risk. Discover how senescent cells and immunosenescence age your heart and the best anti-inflammatory strategies.
HEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/7/202614 min read
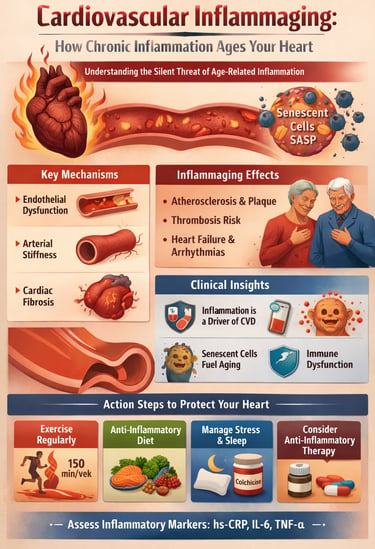
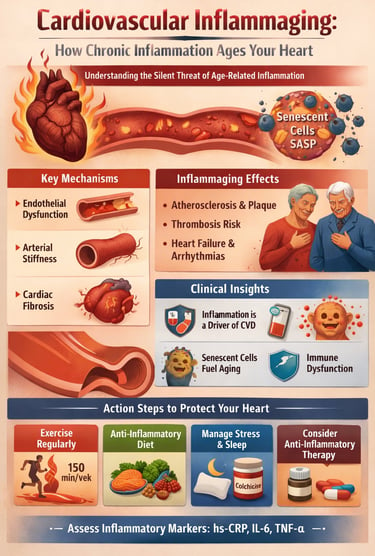
Cardiovascular inflammaging refers to the chronic, low-grade inflammation that develops with aging and silently damages the heart and blood vessels over time. Unlike acute inflammation, this persistent immune activation accelerates atherosclerosis, arterial stiffness, and cardiac dysfunction—even in people with normal cholesterol and blood pressure.
What Causes Inflammaging in the Heart?
Immune system aging (immunosenescence): Reduced immune precision leads to continuous inflammatory signaling
Senescent (“zombie”) cells: Release harmful inflammatory factors (SASP) that damage tissues
Gut microbiome imbalance: Promotes systemic inflammation via immune and metabolic pathways
Chronic stress, poor sleep, and inactivity: Amplify inflammatory cytokines like IL-6 and CRP
How Inflammation Damages the Cardiovascular System
Inflammaging contributes to multiple silent but progressive changes:
Endothelial dysfunction: Reduced nitric oxide → impaired blood flow
Arterial stiffness: Loss of elasticity → increased blood pressure
Atherosclerosis: Faster plaque buildup and instability
Cardiac fibrosis: Stiff heart muscle → diastolic dysfunction
Increased clot risk: Prothrombotic state
Autonomic imbalance: Reduced heart rate variability
Why Normal Cholesterol Doesn’t Mean Low Risk
Research shows that inflammatory markers like high-sensitivity C-reactive protein (hs-CRP) predict heart attacks and strokes independently of traditional risk factors.A person with normal LDL but elevated hs-CRP may have higher cardiovascular risk than someone with mildly elevated cholesterol but low inflammation.
Key Biomarkers to Check
hs-CRP:
<1 mg/L → Low risk
1–3 mg/L → Moderate risk
3 mg/L → High inflammatory risk
IL-6 and TNF-α (advanced testing)
Lipoprotein(a) [Lp(a)]
Homocysteine
Key Takeaways
Inflammaging is a major hidden driver of heart disease
It acts independently of cholesterol and blood pressure
hs-CRP is a critical but underused risk marker
Lifestyle interventions remain the most powerful treatment
Future therapies will target aging biology itself, not just symptoms
Imagine your heart is a house. Traditional cardiology focuses on the obvious threats — burst pipes (plaque rupture), faulty wiring (arrhythmias), and structural collapse (heart failure). But what if the real danger is a slow, silent termite infestation eating away at the foundations for decades before anyone notices the damage?
That is precisely what cardiovascular inflammaging does.
The Six Ways Inflammation Ages Your Heart
A landmark mechanistic review by Spray et al. (2025), published in Cell Reports Medicine, and a comprehensive analysis by Zeng et al. (2025) in Ageing and Disease have mapped the precise cardiovascular pathways through which inflammaging operates. Here is what happens inside your body:
1. Endothelial Dysfunction: Your Vascular Lining Breaks Down
The endothelium — a single cell-thick lining of your blood vessels — is far more than passive wallpaper. It regulates blood flow, prevents clotting, and controls vessel tone. Pro-inflammatory cytokines compromise this lining, reducing nitric oxide production (the molecule that keeps vessels relaxed and dilated) and increasing oxidative stress. The result is the very first, invisible step toward atherosclerosis (Zeng et al., 2025).
2. Arterial Stiffening: Your Vessels Lose Their Bounce
Chronic inflammation accelerates collagen deposition in arterial walls, making them progressively less elastic. Your arteries lose the compliant, spring-like quality that normally buffers blood pressure surges. This arterial stiffening forces your heart to pump harder against greater resistance — contributing to systolic hypertension and, over time, heart failure (Spray et al., 2025).
3. Cardiac Fibrosis and Diastolic Dysfunction
Inflammatory cytokines overstimulate cardiac fibroblasts — cells responsible for maintaining the heart's connective tissue framework — triggering excessive collagen production. This stiffens the heart muscle itself, impairing its ability to relax and fill with blood between beats. This condition, called diastolic dysfunction, often develops silently years before any overt heart failure symptoms emerge (Zeng et al., 2025).
4. Accelerated Atherosclerosis
Chronic inflammation is not merely associated with plaque — it actively drives plaque formation and destabilization. Inflammatory macrophages infiltrate arterial walls, oxidize LDL cholesterol, and create the unstable plaques most likely to rupture and cause a heart attack or stroke (Bartoli-Leonard et al., 2025).
5. Prothrombotic State: Blood That Clots Too Easily
Inflammaging tilts the blood toward clotting. Inflammatory mediators activate platelets, impair natural anticoagulant mechanisms, and prime the coagulation cascade — explaining why aging itself, independent of cholesterol or blood pressure, increases clot risk (Spray et al., 2025).
6. Autonomic Dysfunction: Heart Rate Regulation Falters
The autonomic nervous system — which fine-tunes heart rate, blood pressure, and blood vessel tone on a moment-to-moment basis — loses regulatory precision with age and inflammation. Reduced heart rate variability and increased susceptibility to arrhythmias are measurable consequences (Ajoolabady et al., 2024).
The Zombie Cell Problem: Cellular Senescence and SASP
Perhaps the most dramatic chapter in the inflammaging story involves senescent cells — cells that have stopped dividing but, critically, have also refused to die.
A major 2026 review by Zanders, Arifaj, Wagner, and Dimmeler in Immunological Reviews provides compelling evidence that the accumulation of these senescent cells is a central driver of cardiovascular inflammaging. These cellular "zombies" are not merely inactive bystanders. They actively secrete a toxic cocktail of pro-inflammatory cytokines, growth factors, and tissue-degrading enzymes collectively known as the Senescence-Associated Secretory Phenotype (SASP) (Zanders et al., 2026).
Within the cardiovascular system, SASP:
Promotes endothelial dysfunction in blood vessel walls
Accelerates smooth muscle cell aging and arterial stiffening
Fuels macrophage-mediated plaque inflammation in atherosclerosis
Drives fibrosis in cardiac tissue
Creates a self-perpetuating inflammatory cycle that spreads senescence to neighboring healthy cells
What makes this especially clinically important is that senescent cells accumulate with age in proportion to inflammatory burden — meaning the longer unhealthy lifestyle habits persist, the greater the senescent cell load, and the more severe the cardiovascular consequences. Conversely, this also means that interventions targeting senescent cells — a rapidly advancing field called senolytic therapy — hold genuine promise for cardiovascular rejuvenation (Zanders et al., 2026).
Why "Normal" Lab Values Don't Tell the Whole Story
This is one of the most practically important insights from modern cardiovascular research: millions of people with normal cholesterol, controlled blood pressure, and healthy body weight still suffer heart attacks and strokes.
The reason? Traditional cardiovascular risk assessment was never designed to capture inflammatory burden.
Research by Bartoli-Leonard et al. (2025), published in the Journal of the American Heart Association, demonstrates that elevated inflammatory biomarkers — particularly high-sensitivity CRP (hs-CRP), IL-6, and TNF-α — independently predict cardiovascular events even after fully accounting for all conventional risk factors. This means inflammation adds a layer of risk completely invisible to a standard lipid panel.
The clinical implication is profound: A 55-year-old with LDL of 90 mg/dL, blood pressure of 118/75 mmHg, and hs-CRP of 4.5 mg/L may carry substantially higher cardiovascular risk than a 60-year-old with LDL of 130 mg/dL and hs-CRP of 0.4 mg/L. Current standard screening would identify the younger person as lower risk. Inflammaging-aware assessment would correctly identify them as higher risk.
The Gut Microbiota Connection: A Hidden Regulator of Heart Inflammation
One of the most exciting emerging dimensions of cardiovascular inflammaging involves the gut microbiome. Research by Zhang and Li (2025) in Rejuvenation Research highlights that the gut microbiota does not merely influence digestive health — it actively modulates systemic immune aging through multiple mechanisms, including regulation of IgG antibody biology.
As we age, gut microbial diversity declines (dysbiosis). This dysbiosis:
Promotes leakage of bacterial products (lipopolysaccharides) into the bloodstream, directly stimulating systemic inflammation
Alters IgG glycosylation patterns in ways that amplify pro-inflammatory signaling
Reduces production of short-chain fatty acids (SCFAs) that normally suppress inflammatory pathways
Impairs the gut's ability to regulate immune tolerance
This gut-immune-heart axis explains why dietary interventions rich in fiber, fermented foods, and polyphenols exert such powerful anti-inflammatory and cardiovascular effects — they work, in part, by reshaping the gut microbiome toward a more youthful, anti-inflammatory configuration (Zhang & Li, 2025).
Clonal Hematopoiesis (CHIP): A Newly Recognized Driver of Cardiovascular Inflammaging
One of the most important recent discoveries in cardiovascular aging biology is Clonal Hematopoiesis of Indeterminate Potential (CHIP) — an age-related condition in which blood stem cells acquire somatic mutations that allow certain inflammatory immune cell clones to expand disproportionately over time.
CHIP becomes increasingly common with aging, affecting approximately 10–20% of adults over age 70. While originally studied in hematology because of its association with leukemia risk, research over the last decade has revealed that CHIP is also a powerful and independent cardiovascular risk factor. Individuals with CHIP have significantly higher risks of atherosclerotic cardiovascular disease, myocardial infarction, stroke, heart failure, and cardiovascular mortality — even in the absence of traditional risk factors.
Mechanistically, CHIP-associated mutations (particularly in genes such as TET2, DNMT3A, ASXL1, and JAK2) drive exaggerated inflammatory signaling in monocytes and macrophages. These mutated immune cells overproduce inflammatory cytokines including IL-1β, IL-6, and TNF-α, amplifying endothelial dysfunction, plaque instability, and vascular remodeling. Experimental studies suggest that CHIP may accelerate atherosclerosis through chronic activation of the NLRP3 inflammasome, linking clonal hematopoiesis directly to the biology of inflammaging.
Importantly, CHIP helps explain why some older adults experience aggressive cardiovascular disease despite apparently normal cholesterol levels and otherwise favorable metabolic profiles. It reinforces the emerging concept that cardiovascular disease is not solely a lipid-storage disorder, but also a disorder of immune dysregulation and inflammatory aging.
As genomic testing becomes more accessible, CHIP screening may eventually become part of advanced cardiovascular risk stratification — particularly in older adults with unexplained inflammatory burden or premature cardiovascular disease. Therapeutic strategies targeting inflammasome signaling and IL-1β pathways are now being actively investigated in CHIP-associated cardiovascular disease.
Practical Applications: Your Anti-Inflammaging Action Plan
Science is most valuable when it translates into actionable steps. Based on the current evidence base, here is a comprehensive strategy to reduce cardiovascular inflammaging:
1. Exercise: The Most Potent Anti-Inflammatory Drug
Regular physical activity reduces circulating IL-6, TNF-α, and CRP while simultaneously improving endothelial function and arterial compliance. The evidence supports a combined approach:
Zone 2 aerobic exercise (brisk walking, cycling at a conversational pace): 150 minutes per week minimum
Resistance training: 2–3 sessions per week, targeting all major muscle groups
High-Intensity Interval Training (HIIT): 1–2 sessions per week for additional cardiovascular benefit
Even modest increases in physical activity from a sedentary baseline produce measurable reductions in inflammatory markers (Spray et al., 2025).
2. Mediterranean-Style Diet: Eat Against Inflammation
The Mediterranean dietary pattern — rich in extra virgin olive oil, oily fish, colorful vegetables, legumes, whole grains, nuts, and berries — consistently demonstrates the most robust anti-inflammatory cardiovascular evidence:
Polyphenols (from berries, olive oil, green tea) suppress NF-κB, a master inflammatory switch
Omega-3 fatty acids (from fatty fish, flaxseed, walnuts) reduce IL-6 and TNF-α production
Dietary fiber promotes gut microbial diversity, reducing systemic inflammatory burden
Limit: Ultra-processed foods, refined sugars, industrial seed oils, and red processed meats — all of which amplify inflammaging
3. Prioritize Sleep: Inflammation's Overnight Amplifier
Sleep deprivation and poor sleep quality are potent drivers of inflammaging. During sleep, the body clears metabolic waste, regulates cortisol, and performs critical immune housekeeping. Target 7–9 hours of quality sleep nightly. Address sleep apnea aggressively — untreated obstructive sleep apnea is one of the most underrecognized drivers of cardiovascular inflammaging.
4. Stress Management: The Cortisol-Inflammation Link
Chronic psychological stress chronically elevates cortisol, which paradoxically promotes inflammatory gene expression over time. Regular mindfulness meditation, yoga, time in nature, and community connection all demonstrably reduce inflammatory marker levels and cardiovascular risk.
5. Optimize Gut Health
Consume 30+ different plant foods per week (diversity drives microbiome diversity)
Include fermented foods daily (yogurt, kefir, kimchi, sauerkraut, kombucha)
Minimize antibiotic use to essential clinical indications
Consider probiotic supplementation if clinically indicated
6. Know Your Inflammatory Numbers
Ask your doctor to check:
High-sensitivity CRP (hs-CRP): Target below 1.0 mg/L; above 3.0 mg/L indicates high inflammatory cardiovascular risk
IL-6 and TNF-α: Emerging but increasingly available in specialist settings
Lipoprotein(a) [Lp(a)]: A pro-inflammatory, genetically determined cardiovascular risk factor
Homocysteine: Elevated levels are both a marker and mediator of vascular inflammation
7. Discuss Pharmacological Options With Your Doctor
For selected patients, anti-inflammatory pharmacotherapy may be warranted:
Colchicine (low-dose): The COLCOT and LoDoCo2 trials demonstrated significant cardiovascular event reduction through inflammasome inhibition. Now approved for secondary prevention in many countries.
Statins: Beyond LDL lowering, statins have meaningful anti-inflammatory pleiotropic effects.
Senolytic agents: Clinical trials ongoing — watch this space in 2026–2027.
Biological agents targeting IL-6 and TNF-α: Currently primarily used in inflammatory arthritis; cardiovascular applications under active investigation
.
Frequently Asked Questions (FAQs)
Q1: Can I have cardiovascular inflammaging without any symptoms? Yes — and this is precisely what makes it dangerous. Inflammaging operates entirely silently for years to decades. There are no chest pains, no breathlessness, no warning signals. The first detectable evidence is typically on laboratory testing (elevated hs-CRP, IL-6) or imaging (early endothelial dysfunction, arterial stiffening). This is why proactive inflammatory biomarker testing is so important, particularly after age 40 or in those with a family history of premature heart disease.
Q2: Is cardiovascular inflammaging reversible? Partial reversal is achievable and well-documented, particularly through sustained lifestyle intervention. Studies show that regular aerobic exercise, Mediterranean-style eating, and adequate sleep can meaningfully reduce hs-CRP, IL-6, and other inflammatory markers within weeks to months. Complete reversal of accumulated structural damage (fibrosis, arterial stiffening) is harder to achieve, but slowing and partially reversing the process of inflammaging is absolutely within reach for most people.
Q3: My cholesterol is normal. Do I still need to worry about inflammation? Yes. This is one of the most important messages from current cardiovascular research. Normal LDL cholesterol does not protect you from inflammation-driven cardiovascular disease. Bartoli-Leonard et al. (2025) clearly demonstrate that inflammatory burden predicts cardiovascular events independently of lipid levels. If you have cardiovascular risk factors, a family history of heart disease, or simply want comprehensive assessment, ask your doctor about adding hs-CRP to your standard cardiac risk panel.
Q4: What is the connection between gut health and heart disease through inflammation? The gut microbiome regulates systemic immune function through multiple mechanisms, including modulation of IgG antibody biology, production of anti-inflammatory short-chain fatty acids, and control of bacterial product leakage into the bloodstream (Zhang & Li, 2025). Age-related gut dysbiosis amplifies systemic inflammaging and therefore cardiovascular risk. A high-fiber, plant-diverse, fermented-food-rich diet is one of the most powerful tools for simultaneously improving gut health and reducing cardiovascular inflammaging.
Q5: What are senolytic drugs, and should I be taking them? Senolytics are drugs designed to selectively eliminate senescent "zombie" cells that drive SASP-mediated inflammaging (Zanders et al., 2026). The most studied compounds currently are dasatinib + quercetin (D+Q) and fisetin. While promising preclinical and early clinical data exist, senolytics are NOT yet approved or recommended for routine clinical use. They remain under active investigation in clinical trials. Quercetin (a polyphenol) is available as a supplement and shows mild senolytic properties, but should not be viewed as equivalent to pharmaceutical senolytics. Discuss with your physician before considering any senolytic approach.
Q6: Does sex affect cardiovascular inflammaging risk? Yes, significantly. Estrogen has potent anti-inflammatory properties, which explains why premenopausal women have substantially lower rates of cardiovascular disease compared to age-matched men. After menopause, this protective effect diminishes, and women's cardiovascular disease risk rises sharply — partly due to accelerating inflammaging without estrogen's buffering effect (Ajoolabady et al., 2024). Men tend to accumulate inflammatory cardiovascular burden earlier. By older age, both sexes face substantial inflammaging-related risk, but the trajectory and timing differ, which has implications for sex-specific screening and prevention strategies.
Q7: At what age should I start taking inflammaging seriously? Now — regardless of your current age. The inflammatory processes that cause cardiovascular disease in later life begin accumulating in young adulthood. A 30-year-old who starts exercising regularly, eating a Mediterranean diet, managing stress, and sleeping 8 hours nightly is making cardiovascular investments that compound over decades. Prevention is exponentially easier than reversal. That said, even individuals in their 60s, 70s, and beyond show measurable cardiovascular benefit from anti-inflammatory lifestyle changes — it is never too late to begin.
Clinical pearls
1 Inflammation is an Independent Cardiovascular Risk Driver: Chronic, low-grade systemic inflammation, often referred to as inflammaging, is not just a secondary marker but an independent, primary driver of cardiovascular disease (CVD), even in individuals with optimal traditional risk factors
Inflammation is the "Hidden Fire": Even if your cholesterol is normal, chronic inflammation can act like a slow-burning fire in your arteries. Testing for markers like CRP can show if you have a "hidden risk" that standard tests miss.
2 Senescent Cell Burden & SASP: The accumulation of non-dividing "zombie" cells drives vascular aging. These cells secrete the Senescence-Associated Secretory Phenotype (SASP), a cocktail of cytokines that directly induces endothelial dysfunction and cardiac fibrosis.
As we age, some cells stop working but don't leave. These "zombie cells" release toxins that stiffen your heart and blood vessels. New science is looking for ways to clear these out to keep your heart young.
3 Vascular Wall Autonomy: Arterial stiffening is an active biochemical process. Endothelial and smooth muscle cells are not passive victims; they actively amplify the inflammatory cycle, making the vascular wall itself a key therapeutic target.
Your blood vessels are alive and constantly reacting. They don't just wear out like old pipes; they actively participate in your health. Keeping them "calm" through good habits prevents them from becoming stiff and brittle.
4 Multi-Modal Lifestyle Intervention: Evidence-based lifestyle changes (Mediterranean diet, zone-2 and resistance exercise) remain the most potent "epigenetic" tools to downregulate systemic inflammatory signaling across multiple pathways.
Exercise and a plant-rich diet aren't just for weight loss; they act like a "clean-up crew" for your blood vessels, lowering the chemicals that cause inflammation and aging.
5 The Immunosenescence Paradox: Aging creates a dual-threat state of hyperinflammation and immunodeficiency. Management requires immune modulation to restore homeostatic balance rather than broad immunosuppression.
As we get older, our immune system gets confused—it’s too weak to fight off germs but too "cranky," causing constant internal irritation. We want to help it find its balance so it protects you instead of attacking your heart.
The Emerging Frontier: What's Coming in Inflammaging Therapy
The next five years in cardiology are likely to be defined by anti-inflammaging therapeutics. Several promising avenues are advancing toward clinical reality:
Senolytic clinical trials targeting cardiovascular endpoints are underway, with preliminary results expected in 2026–2027. The combination of dasatinib + quercetin and the flavonoid fisetin is the most advanced candidate (Zanders et al., 2026).
Gut microbiome modulation through precision probiotics, dietary fibre interventions, and even fecal microbiota transplantation for cardiometabolic indications is an active research area, driven in part by the IgG-gut connection described by Zhang and Li (2025).
CAR-T cell therapies adapted to target and clear senescent cells represent the most ambitious — and potentially most powerful — approach on the horizon, though clinical application remains years away.
Complement cascade inhibition is entering cardiovascular clinical trials, as hyperactivation of this ancient immune pathway has been identified as a significant driver of age-related vascular inflammation (Spray et al., 2025).
Author’s Note
Cardiovascular disease is often framed as a consequence of dyslipidemia, hypertension, and lifestyle excesses. While these factors remain important, contemporary research increasingly demonstrates that they do not fully explain cardiovascular risk—particularly in aging populations. This article was written to highlight cardiovascular inflammaging as a central, biologically driven mechanism that bridges aging, immune dysregulation, and cardiovascular pathology.
The concept of inflammaging reframes cardiovascular disease not merely as a disorder of vessels and lipids, but as a chronic, immune-mediated condition shaped by lifelong inflammatory exposure. By integrating recent advances in immunosenescence, senescent cell biology, endothelial dysfunction, and vascular remodeling, this article aims to translate complex mechanistic science into clinically meaningful insight.
Particular emphasis was placed on evidence from 2024–2025 literature to ensure relevance to current practice. While emerging therapies such as senolytics, immune modulation, and targeted anti-inflammatory pharmacotherapy show promise, this work deliberately underscores the enduring importance of lifestyle interventions—exercise, nutrition, sleep, stress management, and social connection—as foundational anti-inflammaging strategies with the strongest real-world evidence.
This article is intended for clinicians, researchers, and scientifically engaged readers seeking a deeper understanding of why cardiovascular risk rises with age even in the absence of traditional risk factors. It also serves as a call to broaden cardiovascular prevention beyond cholesterol and blood pressure, toward a more integrative model that addresses immune aging and chronic inflammation as modifiable drivers of disease.
Ongoing research will undoubtedly refine biomarkers, clarify patient selection for anti-inflammatory therapies, and determine the long-term safety of novel interventions. Until then, recognizing and addressing inflammaging represents one of the most promising frontiers in preventive cardiology and healthy aging.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
The Cholesterol Paradox: When Lower Numbers Don’t Mean Lower Heart Risk | DR T S DIDWAL
hsCRP in Cardiovascular Disease: Should It Be Measured for Risk Assessment in 2026? | DR T S DIDWAL
Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health | DR T S DIDWAL
hsCRP Explained: What Inflammation Means for Your Heart | DR T S DIDWAL
References
Ajoolabady, A., Pratico, D., Tang, D., Zhou, S., Franceschi, C., & Ren, J. (2024). Immunosenescence and inflammaging: Mechanisms and role in diseases. Ageing Research Reviews, 101, Article 102540. https://doi.org/10.1016/j.arr.2024.102540
Bartoli-Leonard, F., Clark, D. E., Singhal, N. S., & Nguyen, P. K. (2025). Unmasking the hidden burden: Inflammation and cardiovascular disease JAHA spotlight on the role of the immune system in cardiovascular health and disease. Journal of the American Heart Association, e047298. https://doi.org/10.1161/JAHA.125.047298
Spray, L., Richardson, G., Haendeler, J., Altschmied, J., Rumampouw, V., Wallis, S. B., Georgiopoulos, G., White, S., Unsworth, A., Stellos, K., Tual-Chalot, S., & Spyridopoulos, I. (2025). Cardiovascular inflammaging: Mechanisms, consequences, and therapeutic perspectives. Cell Reports Medicine, 6(9), Article 102264. https://doi.org/10.1016/j.xcrm.2025.102264
Zanders, L., Arifaj, D., Wagner, J. U. G., & Dimmeler, S. (2026). Cellular senescence, inflammaging and cardiovascular disease. Immunological Reviews, 337(1), Article e70084. https://doi.org/10.1111/imr.70084
Zeng, Y., Buonfiglio, F., Li, J., Pfeiffer, N., & Gericke, A. (2025). Mechanisms underlying vascular inflammaging: Current insights and potential treatment approaches. Aging and Disease, 16(4), 1889. https://doi.org/10.14336/ad.2024.0922
Zhang, X.-Y., & Li, D.-G. (2025). Immunoglobulin G and aging: Biological functions and its crosstalk with the gut microbiota. Rejuvenation Research, 29(2). https://doi.org/10.1177/15491684251396176