What Causes Visceral Fat? Hormones, Lifestyle, and Metabolic Risk Explained
Explore the science behind visceral fat formation, including cortisol, insulin resistance, and diet. Clinician-backed strategies to reduce belly fat safely.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/16/202618 min read
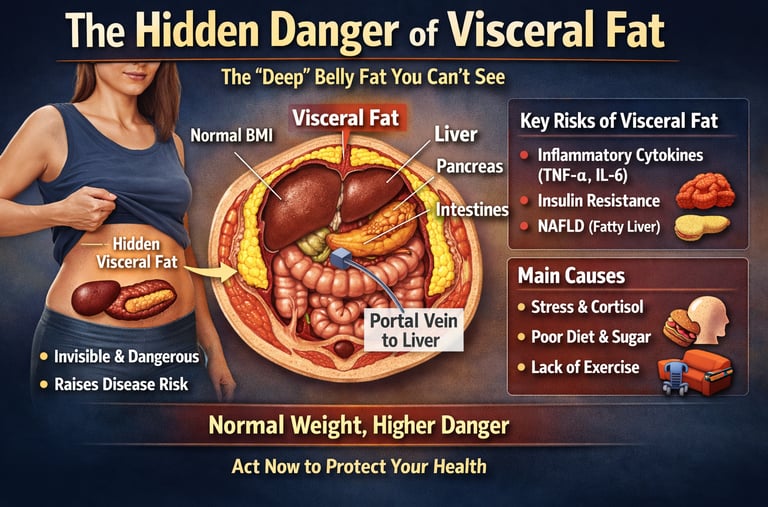
Visceral fat silently surrounds your vital organs, driving heart disease, diabetes, and liver damage — often in people who appear perfectly healthy by every standard measure. A patient with a normal BMI but increased waist circumference may already be on the path toward insulin resistance, fatty liver disease, or cardiovascular complications.
For decades, most people believed body weight alone determined metabolic health. If the number on the scale looked normal — and Body Mass Index (BMI) fell within the “healthy” range — the assumption was that the body was metabolically safe. But modern obesity and cardiometabolic research is overturning that idea. Scientists now understand that one of the most dangerous forms of fat is often the one you cannot see: visceral fat, the deep abdominal fat that surrounds vital organs, including the liver, pancreas, heart, and intestines (Lin & Tandar, 2026).
Unlike the soft subcutaneous fat beneath the skin, visceral adipose tissue behaves like an active endocrine organ. It releases inflammatory cytokines such as TNF-α and IL-6, disrupts insulin signalling, increases triglyceride production, and accelerates the development of insulin resistance, fatty liver disease, metabolic syndrome, and cardiovascular disease (Cesaro et al., 2023; Dhokte & Czaja, 2024). Even more concerning, this hidden abdominal fat can accumulate silently in people who appear lean by conventional standards — particularly in South Asian populations, where dangerous visceral adiposity often develops at lower BMI thresholds (Lin & Tandar, 2026).
Emerging imaging studies now suggest visceral fat may impair heart function years before symptoms appear, linking excess abdominal fat to early myocardial dysfunction and subclinical cardiovascular disease (Vicardi et al., 2026). In other words, your waist circumference may reveal far more about your long-term health than your body weight alone. The good news is that visceral fat is also highly responsive to evidence-based lifestyle interventions.
Key Takeaways
Visceral fat surrounds internal organs and drives inflammation
Dangerous visceral fat can exist even at normal BMI
Waist-to-height ratio predicts risk better than BMI
Sleep, stress, and sugar intake strongly influence visceral fat
Visceral fat can improve rapidly with lifestyle intervention
What Exactly Is Visceral Fat?
Visceral fat is the fat stored deep within the abdominal cavity — not the soft flesh you can pinch beneath your skin (that is subcutaneous fat), but a dense, biologically active tissue nestled around your internal organs. Its two primary anatomical locations — the omental and mesenteric fat depots — sit in dangerous proximity to the portal circulation: the blood supply that drains directly into the liver (Khawaja et al., 2024).
This proximity is precisely what makes visceral fat so metabolically toxic. Every inflammatory molecule, every excess free fatty acid released from visceral tissue travels straight to the liver via the portal vein — causing direct, measurable damage to one of your body's most vital organs.
Crucially, visceral fat is not passive storage. It functions as a metabolically active endocrine organ, secreting a range of biologically active molecules including tumour necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and C-reactive protein — all potent drivers of systemic inflammation — while simultaneously suppressing adiponectin, a protective anti-inflammatory adipokine (Gugliucci, 2022). This imbalance creates a state of chronic low-grade inflammation that quietly corrodes metabolic health over the years.
How Visceral Fat Is Measured: Beyond the Bathroom Scale
CT scanning and MRI remain the gold standard for quantifying visceral fat with precision. In everyday clinical practice, however, simpler tools carry considerable predictive power:
Women — Waist Circumference≥ 88 cm, 35 inches or above signals elevated cardiometabolic risk
Men — Waist Circumference≥ 102 cm, 40 inches or above signals elevated cardiometabolic risk
Waist-to-Height Ratio> 0.5. Divide waist by height. Above 0.5 is a red flag regardless of BMI
The limitations of Body Mass Index deserve emphasis. BMI does not distinguish between fat mass and muscle mass, nor does it reveal fat distribution. An individual with a "normal" BMI can carry clinically significant visceral fat — a condition increasingly described as normal-weight obesity or metabolically obese normal weight (Luo et al., 2025). This is not an edge case; it is a widespread clinical reality, and one that screening focused exclusively on BMI will systematically miss.
Clinical insight: South Asian individuals — including those of Indian, Pakistani, Bangladeshi, and Sri Lankan origin — accumulate dangerous levels of visceral fat at BMI thresholds 3–5 points lower than European population averages. If you are of South Asian heritage, your metabolic risk may begin well below 25 kg/m². Waist circumference and waist-to-height ratio are particularly important screening tools for this population (Lin & Tandar, 2026).
Why Visceral Fat Is So Dangerous: The Biology Explained
The Inflammatory Cascade
Visceral adipose tissue releases elevated concentrations of TNF-α and IL-6, creating a state of chronic low-grade systemic inflammation. This inflammatory signalling progressively disrupts insulin receptor function, accelerates atherosclerotic plaque formation, and drives multi-organ metabolic dysfunction. Equally damaging is the simultaneous suppression of adiponectin — the very hormone that would normally protect against insulin resistance and cardiovascular disease (Cesaro et al., 2023; Gugliucci, 2022).
The Portal Mechanism: Direct Liver Damage
Because visceral fat drains via the portal vein into the liver, excess free fatty acids arrive at the hepatic tissue in high concentrations. The liver responds by developing hepatic insulin resistance (it stops responding to insulin's signal to suppress glucose production), increasing gluconeogenesis, and accumulating surplus fat — a condition known as non-alcoholic fatty liver disease (NAFLD), now the most common liver condition globally (Khawaja et al., 2024; Dhokte & Czaja, 2024).
Cardiac Risk: A New Imaging Frontier
A 2026 review in Nutrients by Vicardi and colleagues introduced a significant new dimension to our understanding of visceral fat's cardiac impact. Examining epicardial and visceral adipose tissue through cardiac imaging, the study found associations between fat burden and global longitudinal strain — a sensitive echocardiographic marker of subclinical myocardial dysfunction that predicts adverse cardiac events before any clinical symptoms emerge (Vicardi et al., 2026). In other words, visceral fat may be silently weakening your heart muscle long before you ever feel breathless or experience chest discomfort. Emerging evidence also suggests that visceral adiposity is strongly associated with elevated ApoB-containing lipoprotein particles, even when LDL cholesterol appears “normal.” This ApoB–LDL discordance is increasingly recognised in insulin-resistant states and may partly explain why some individuals develop cardiovascular disease despite apparently acceptable conventional lipid profiles.
The Triglyceride-Glucose Index: A Powerful Predictive Tool
A 2026 study in the European Journal of Medical Research by Yin and colleagues demonstrated that combining the visceral adiposity index with the triglyceride-glucose index produces a significantly more accurate predictor of cardiovascular disease incidence in middle-aged and older adults than either marker alone (Yin et al., 2026). This composite index — simple enough to calculate from a standard lipid panel and fasting glucose — may become a routine risk stratification tool in clinical practice within the decade.
Ectopic Fat Spillover
When visceral adipose tissue reaches storage capacity, fat begins to accumulate in organs not designed to hold it — the liver, skeletal muscle, and pancreas. This ectopic fat deposition impairs pancreatic beta-cell function (reducing insulin secretion), decreases muscle insulin sensitivity, and perpetuates a vicious cycle of metabolic deterioration (Luo et al., 2025).
The Hormonal Architecture of Visceral Fat
Understanding visceral fat without understanding hormones is like understanding a fire without oxygen. Your hormonal environment is not merely associated with visceral fat accumulation — it actively governs it.
Cortisol: The Stress Hormone That Builds Belly Fat
Visceral adipocytes carry a higher density of cortisol receptors than subcutaneous fat cells. When cortisol is chronically elevated — through sustained psychological stress, poor sleep, or shift work — it activates lipoprotein lipase specifically in visceral depots, directing fat storage around your organs rather than beneath your skin. Cortisol simultaneously increases appetite for calorie-dense foods and drives gluconeogenesis, compounding metabolic harm.
Clinical Pearl — The Midnight Cortisol Storm
Sleep restriction of fewer than six hours per night creates a neuroendocrine "perfect storm": ghrelin (hunger hormone) rises sharply, leptin (satiety hormone) falls, and cortisol levels remain abnormally elevated into the evening — precisely when they should be lowest. This combination increases caloric intake while simultaneously directing fat specifically toward visceral depots. Sleep is not optional; it is metabolic medicine.
Insulin and Hyperinsulinemia: The One-Way Fat Valve
Chronically elevated insulin — a hallmark of diets heavy in refined carbohydrates and sugar — inhibits hormone-sensitive lipase, the enzyme responsible for releasing stored fat for energy. This effectively locks fat inside visceral cells. Simultaneously, insulin activates de novo lipogenesis, converting dietary carbohydrate into new fat. Raheem et al. (2022) confirmed that visceral adiposity is directly associated with metabolic profiles predictive of both type 2 diabetes and myocardial infarction, with hyperinsulinemia as a central mechanistic driver.
Fructose: The Liver's Hidden Burden
Unlike glucose, fructose is metabolised almost exclusively in the liver. Excess fructose intake — particularly from sugar-sweetened beverages and ultra-processed foods — overwhelms the liver's metabolic capacity and triggers a "shortcut" to visceral and hepatic fat via direct stimulation of de novo lipogenesis (Dhokte & Czaja, 2024). Critically, this process can occur even in the absence of an overall caloric surplus. Liquid sugars and high-fructose corn syrup may be among the most potent dietary drivers of visceral fat accumulation.
Sex Hormones and the Menopausal Shift
Oestrogen, at premenopausal concentrations, actively directs fat storage toward the gluteofemoral region — hips and thighs — a metabolically safer depot. This represents a genuine hormonal shield against visceral accumulation. Agrawal et al. (2022) confirmed through large-scale genomic analysis that gluteofemoral and visceral fat have distinct genetic architectures, reflecting their different metabolic roles. When oestrogen declines at menopause, this protective signalling is lost and fat rapidly redistributes toward the visceral compartment — explaining the sharply increased cardiometabolic risk observed in postmenopausal women.
In men, low testosterone is independently associated with visceral fat accumulation and metabolic syndrome, making hormonal assessment a relevant component of cardiometabolic risk evaluation.
Visceral Fat vs. Subcutaneous Fat: A Critical Distinction
Visceral Fat
Stored deep inside the abdominal cavity, surrounding organs such as the liver, pancreas, and intestines
Metabolically highly active and functions as an endocrine organ
Releases large amounts of inflammatory cytokines including TNF-α, IL-6, and CRP
Associated with suppressed adiponectin levels, reducing metabolic protection
Strongly linked to insulin resistance, fatty liver disease, type 2 diabetes, and cardiovascular disease
Commonly assessed using waist circumference, waist-to-height ratio, CT scan, MRI, or DEXA imaging
Responds rapidly to lifestyle interventions and often decreases faster with exercise and dietary improvement
Subcutaneous Fat
Located beneath the skin and can usually be pinched
Metabolically less active and relatively less inflammatory
Produces lower levels of inflammatory cytokines
Adiponectin levels are relatively preserved
Gluteofemoral subcutaneous fat (hips and thighs) may provide metabolic and cardiovascular protection
Typically measured using skinfold calipers or body composition analysis
Mobilises more slowly during weight loss and exercise interventions
Why Body Fat Distribution Matters
“Apple-shaped” fat distribution reflects central visceral fat accumulation and is associated with substantially higher cardiometabolic risk
“Pear-shaped” fat distribution reflects greater gluteofemoral fat storage and is generally considered metabolically safer
The "apple versus pear" body shape distinction is not merely cosmetic. It is a reflection of this fundamental metabolic difference. Apple-shaped fat distribution — characterised by central visceral accumulation — carries substantially greater cardiometabolic risk than pear-shaped gluteofemoral distribution (Agrawal et al., 2022; Shetty et al., 2025).
The Disease Burden: What Visceral Fat Does to Your Body
Visceral fat does not operate in isolation. It sits at the convergence of multiple pathological processes, accelerating or directly causing some of the most prevalent chronic diseases of our time:
Cardiovascular disease: Cesaro et al. (2023) established that visceral adipose tissue contributes substantially to residual cardiovascular risk — the risk that persists even after treating conventional risk factors such as LDL cholesterol. Visceral fat promotes atherosclerosis through inflammatory cytokines, dyslipidaemia, and endothelial dysfunction. Yin et al. (2026) further refined this picture by demonstrating that combined visceral adiposity and triglyceride-glucose index scores predict cardiovascular events with high accuracy in middle-aged and older adults.
Subclinical cardiac dysfunction: The 2026 cardiac imaging data from Vicardi et al. revealed that epicardial and visceral fat accumulation correlate with impaired global longitudinal strain — a measure of how efficiently the heart muscle contracts. This establishes a direct imaging-confirmed link between visceral adiposity and preclinical heart muscle dysfunction, opening a new avenue for early detection.
Type 2 diabetes: Dhokte and Czaja (2024) provide a comprehensive mechanistic account of how visceral fat drives type 2 diabetes through the combined forces of portal lipotoxicity, adipokine imbalance, systemic inflammation, and hepatic insulin resistance. Visceral fat does not merely correlate with diabetes — it is a primary causal driver.
NAFLD and liver disease: The portal delivery of excess free fatty acids from visceral depots directly promotes hepatic fat accumulation. NAFLD now affects an estimated 25–30% of adults globally and is the leading cause of liver transplantation in many high-income countries.
Metabolic syndrome: Visceral fat is the central pathological feature of metabolic syndrome — the clustering of central obesity, elevated triglycerides, low HDL, hypertension, and impaired glucose metabolism that dramatically amplifies cardiovascular and diabetic risk.
Practical Applications: Six Evidence-Based Steps to Reduce Visceral Fat
Here is the genuinely hopeful part of this story: visceral fat is highly and rapidly responsive to lifestyle intervention — often more so than subcutaneous fat. Measurable reductions in visceral fat have been documented within six to twelve weeks of consistent lifestyle change, frequently before significant body weight changes occur (Luo et al., 2025).
Prioritise Zone 2 Aerobic Exercise (150–300 min/week)
Moderate-intensity steady-state cardio — the pace at which you can hold a conversation — is among the most evidence-based visceral fat interventions. This intensity maximises fat oxidation, improves mitochondrial function, and reduces visceral fat independent of total weight loss. Brisk walking, cycling, swimming, and jogging all qualify. Consistency trumps intensity
Eliminate Sugar-Sweetened Beverages and Ultra-Processed Foods
No single dietary change delivers more visceral fat benefit than removing liquid sugar and ultra-processed foods. Fructose-rich beverages bypass normal satiety signals and overflow directly into hepatic and visceral fat production. Replace with water, herbal teas, and whole foods rich in fibre, lean protein, and healthy fats. You do not need a perfect diet — you need a substantially better one.
Protect 7–9 Hours of Quality Sleep — Every Night
Even partial sleep restriction of two to three nights raises ghrelin, suppresses leptin, elevates evening cortisol, and impairs insulin sensitivity. Sleep is not passive recovery — it is active hormonal regulation. Turn off screens one hour before bed, keep bedroom temperature cool, and treat consistent sleep as the metabolic intervention it truly is.
Build Lean Muscle with Twice-Weekly Resistance Training
Skeletal muscle is your body's primary glucose disposal organ — responsible for up to 80% of insulin-mediated glucose uptake. Inadequate muscle mass forces excess blood sugar into visceral storage. Even two sessions of resistance training per week meaningfully improve insulin sensitivity, increase resting metabolic rate, and shift the hormonal environment away from fat storage. You do not need to lift heavy — bodyweight exercises, resistance bands, and moderate weights all work.
Implement Active Stress Management Daily
Chronic psychological stress is not a lifestyle inconvenience — it is a direct driver of cortisol-mediated visceral fat deposition. Evidence-based strategies include structured breathing exercises (four counts in, six counts out), mindfulness practice, time in natural environments, and therapeutic support when needed. Even ten to fifteen minutes of intentional stress reduction daily produces measurable hormonal benefits over weeks.
Measure What Actually Matters — Ask for a Waist Circumference
At your next health check, request a waist circumference measurement alongside your blood pressure and cholesterol. Calculate your waist-to-height ratio (waist ÷ height; target below 0.5). Ask about fasting triglycerides, fasting insulin, HDL cholesterol, CRP, and liver enzymes — these blood markers collectively paint a picture of visceral fat-related metabolic dysfunction that BMI alone will miss entirely (Shetty et al., 2025).
Frequently Asked Questions
Q1 Can I have dangerous visceral fat even with a normal BMI?
Absolutely — and this is one of the most important clinical insights of the past decade. A person with a BMI in the "healthy" range can carry significant visceral fat if their lifestyle, hormonal profile, or genetic predisposition favours central fat deposition. This condition is called normal-weight obesity or metabolically obese normal weight. Lin and Tandar (2026) confirmed this in their global review, noting that conventional BMI-based screening systematically fails to detect visceral adiposity in a significant portion of the population. Waist circumference and waist-to-height ratio are far more informative than BMI alone for assessing true metabolic risk.
Q2 How quickly can visceral fat be reduced with lifestyle changes?
This is where the good news is genuinely encouraging. Visceral fat is highly responsive to lifestyle intervention — often more so than subcutaneous fat. Studies consistently show measurable reductions in visceral fat within six to twelve weeks of regular aerobic exercise and dietary improvement, frequently before significant changes in body weight appear on the scale. Your waist circumference may decrease, and blood markers like triglycerides and fasting insulin may improve, while the number on the scale remains largely unchanged. This is normal and represents real, meaningful metabolic progress (Luo et al., 2025).
Q3 Is stress genuinely a cause of visceral fat, or is it just a contributing factor?
Stress is a direct, mechanistic cause of visceral fat accumulation — not merely an aggravating factor. Cortisol, the primary stress hormone, has a preferential affinity for visceral adipocytes, which carry a higher density of cortisol receptors than subcutaneous fat cells. Chronically elevated cortisol activates lipoprotein lipase in visceral depots, directly promoting fat storage around your organs. Cortisol also increases appetite for calorie-dense foods and drives glucose production, compounding metabolic harm. Managing stress is not a "wellness nice-to-have" — it is a core cardiometabolic intervention.
Q4 Why do women gain visceral fat so rapidly after menopause?
Oestrogen at premenopausal concentrations acts as an active metabolic shield, directing fat storage toward the gluteofemoral region — hips and thighs — where it is metabolically far safer. This protective mechanism is tied to oestrogen's activation of alpha-adrenergic receptors in gluteofemoral depots. When oestrogen declines at menopause, this signalling is lost and fat redistribution toward the visceral compartment accelerates sharply. This is a primary driver of the increased cardiovascular and diabetic risk observed in postmenopausal women — and a key reason why lifestyle habits effective in a woman's thirties may need deliberate upgrading in her fifties, particularly with regard to strength training and dietary quality (Agrawal et al., 2022).
Q5 What blood tests should I ask for to assess visceral fat-related risk?
While there is no single blood test for visceral fat, several markers in a standard panel collectively illuminate metabolic risk: elevated fasting triglycerides, low HDL cholesterol, elevated fasting insulin (hyperinsulinemia), elevated high-sensitivity CRP (a marker of systemic inflammation), elevated liver enzymes (ALT and AST, suggesting hepatic fat), and elevated fasting glucose or HbA1c. Shetty et al. (2025) recommend integrating these markers with physical measurements — particularly waist circumference and waist-to-height ratio — for a comprehensive cardiometabolic risk assessment. The triglyceride-glucose index, derived from fasting triglycerides and fasting glucose, is emerging as a particularly powerful composite risk marker (Yin et al., 2026).
Q6 Does alcohol contribute to visceral fat accumulation?
Yes, through multiple overlapping mechanisms. Alcohol itself provides seven kilocalories per gram — nearly double the caloric density of carbohydrate or protein — and its primary metabolite, acetate, is preferentially taken up by the liver and converted into fat, directly accelerating hepatic and visceral fat accumulation. Alcohol also disrupts sleep architecture, raising overnight cortisol and impairing the hormonal environment that governs fat metabolism. Heavy and regular drinking is associated with the characteristic "alcoholic belly" that reflects precisely this pattern. Even moderate reduction in alcohol consumption produces measurable improvements in liver fat and abdominal fat distribution within weeks.
Q7 Can visceral fat affect heart function before heart disease is diagnosed?
Yes — and this represents one of the most important recent developments in this field. The 2026 cardiac imaging study by Vicardi and colleagues found that both epicardial and visceral fat accumulation correlate with impaired global longitudinal strain, a sensitive measure of subtle heart muscle dysfunction that can be detected by echocardiography before any clinical symptoms emerge (Vicardi et al., 2026). This means visceral fat may be quietly impairing myocardial function years before a diagnosis of heart failure or coronary disease is considered. Early assessment of visceral adiposity is not just about preventing diabetes — it is about protecting the heart from damage that begins long before it becomes visible on standard tests.
Clinical pearls
1. The Fallacy of "Healthy" BMI
Scientific Perspective: Body Mass Index (BMI) is an aggregate metric that fails to differentiate between lean mass, subcutaneous fat, and visceral adipose tissue (VAT). Phenotypic variations like "normal-weight obesity" or metabolically obese normal weight (MONW) present significant cardiometabolic risks that BMI-centric screening systematically misses. Furthermore, South Asian populations exhibit metabolic vulnerability and visceral accumulation at much lower BMI thresholds BMI < 25 than European cohorts.
The scale doesn't tell the whole story. You can look completely healthy on the outside and have a "normal" weight, but still carry dangerous fat hidden deep around your internal organs. This is especially true for people of South Asian descent, who tend to store this dangerous belly fat even at lower weights.
2. The Portal Vein Direct Pathway
Scientific Perspective: Visceral fat depots (omental and mesenteric) drain directly into the hepatic portal circulation. This anatomical positioning exposes the liver to high concentrations of non-esterified free fatty acids (NEFAs) and pro-inflammatory cytokines (TNF-alpha, IL-6). This direct influx triggers hepatic insulin resistance, upregulates gluconeogenesis, and drives the pathogenesis of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD/NAFLD).
Belly fat has a direct hotline to your liver. Because of how your blood flows, every toxic chemical and excess fat molecule released by hidden belly fat goes straight into your liver first. This quickly overwhelms the liver, forcing it to become fatty and sluggish, which eventually leads to type 2 diabetes.
3. Subclinical Myocardial Dysfunction
Scientific Perspective: Advanced cardiac imaging reveals that visceral and epicardial adiposity are independently associated with a reduction in Global Longitudinal Strain (GLS). GLS is a highly sensitive echocardiographic marker of subclinical myocardial dysfunction, proving that ectopic fat burden induces mechanical and metabolic stress on the myocardium long before changes in left ventricular ejection fraction (LVEF) or overt clinical symptoms manifest.
Hidden fat weakens your heart muscle before you ever feel it. New heart-imaging technology shows that deep body fat silently impairs how well your heart muscle contracts. This means it could be reducing your heart's pumping efficiency years before you ever experience warning signs like breathlessness or chest pain.
4. The Sleep-Cortisol Neuroendocrine Loop
Scientific Perspective: Sleep restriction (< 6 hours/night) induces a neuroendocrine cascade characterized by the upregulation of ghrelin, downregulation of leptin, and a disruption of the diurnal cortisol rhythm (evening cortisol elevation). Visceral adipocytes possess a high density of glucocorticoid receptors; chronically elevated cortisol selectively activates lipoprotein lipase (LPL) in these tissues, preferentially shunting lipid storage into visceral rather than subcutaneous depots.
Poor sleep acts as a magnet for belly fat. When you get less than 6 hours of sleep, your brain triggers a hormonal storm. Your hunger hormones spike, your fullness hormones drop, and your stress hormone (cortisol) stays dangerously high at night. Because deep belly fat cells are highly sensitive to stress hormones, your body is chemically directed to store fat around your organs instead of under your skin.
5. Fructose-Induced De Novo Lipogenesis
Scientific Perspective: Fructose metabolism is uniquely hepatic and escapes the rate-limiting phosphofructokinase step that regulates glycolysis. When consumed in excess—particularly via liquid mediums—fructose overwhelms hepatic processing pathways, directly stimulating de novo lipogenesis (DNL) and driving ectopic fat accumulation in the liver and visceral cavities. This pathological fat accumulation can occur independently of an overall caloric surplus.
Liquid sugar is a shortcut to organ fat. Unlike regular sugar, which your whole body uses for energy, the sugar found in sodas, juices, and ultra-processed foods (fructose) can only be broken down by your liver. When you drink or eat too much of it, your liver gets overwhelmed and immediately turns that sugar straight into deep belly fat—even if you aren't eating too many total calories.
6. The Menopausal Oestrogen Shield Loss
Scientific Perspective: Premenopausal oestrogen concentrations promote a safe, gluteofemoral (subcutaneous) adipocyte distribution by modulating alpha-adrenergic and lipoprotein lipase activity. At menopause, the cessation of ovarian oestrogen production removes this protective metabolic shield. This results in a distinct genomic shift, rapidly redistributing adipose deposition from the lower body to the visceral compartment and sharply accelerating postmenopausal cardiometabolic risk.
Menopause changes where your body stores fat. Before menopause, the hormone oestrogen acts like a protective shield, directing fat to be stored safely in the hips and thighs. When oestrogen drops during menopause, that shield disappears, and the body suddenly shifts its fat storage to the deep belly area. This explains why women's risk for heart disease and diabetes rises after menopause, making strength training and diet quality more important than ever in your 50s.
Clinician’s Perspective
As physicians, we are increasingly encountering patients who appear “healthy” by conventional measures yet already show early signs of metabolic dysfunction beneath the surface. A normal Body Mass Index does not necessarily mean metabolic safety. In clinical practice, we frequently see individuals with normal body weight but elevated waist circumference, fatty liver disease, insulin resistance, elevated triglycerides, hypertension, or prediabetes — all driven in part by excess visceral adiposity.
What makes visceral fat particularly concerning is its biological activity. This is not passive energy storage. Visceral adipose tissue functions as an inflammatory endocrine organ that directly influences insulin signalling, vascular health, liver metabolism, and cardiovascular risk. In many patients, visceral fat accumulation begins years before overt disease becomes clinically apparent. By the time type 2 diabetes, coronary artery disease, or metabolic syndrome is diagnosed, the underlying inflammatory process has often been progressing silently for decades.
The encouraging reality is that visceral fat is highly modifiable. Even modest improvements in physical activity, sleep quality, nutrition, stress management, and muscle mass can produce measurable metabolic benefits within weeks. From a preventive medicine perspective, early recognition of visceral adiposity may represent one of the most powerful opportunities we have to reduce the future burden of diabetes, fatty liver disease, stroke, and cardiovascular disease worldwide.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Beyond BMI: Why Waist-to-Height Ratio (WHtR) is the New Clinical Gold Standard
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Researc
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Agrawal, S., Wang, M., Klarqvist, M. D. R., Smith, K., Shin, J., Dashti, H., Diamant, N., Choi, S. H., Jurgens, S. J., Ellinor, P. T., Philippakis, A., Claussnitzer, M., Ng, K., Udler, M. S., Batra, P., & Khera, A. V. (2022). Inherited basis of visceral, abdominal subcutaneous and gluteofemoral fat depots. Nature Communications, 13(1), 3771. https://doi.org/10.1038/s41467-022-30931-2
Cesaro, A., De Michele, G., Fimiani, F., Acerbo, V., Scherillo, G., Signore, G., Rotolo, F. P., Scialla, F., Raucci, G., Panico, D., Gragnano, F., Moscarella, E., Scudiero, O., Mennitti, C., & Calabrò, P. (2023). Visceral adipose tissue and residual cardiovascular risk: A pathological link and new therapeutic options. Frontiers in Cardiovascular Medicine, 10, 1187735. https://doi.org/10.3389/fcvm.2023.1187735
Dhokte, S., & Czaja, K. (2024). Visceral adipose tissue: The hidden culprit for type 2 diabetes. Nutrients, 16(7), 1015. https://doi.org/10.3390/nu16071015
Gugliucci, A. (2022). Biomarkers of dysfunctional visceral fat. In Advances in Clinical Chemistry (Vol. 108). Elsevier. https://doi.org/10.1016/bs.acc.2022.08.002
Khawaja, T., Nied, M., Wilgor, A., et al. (2024). Impact of visceral and hepatic fat on cardiometabolic health. Current Cardiology Reports, 26, 1297–1307. https://doi.org/10.1007/s11886-024-02127-1
Lin, J. C., & Tandar, C. E. (2026). Global patterns of visceral adiposity and cardiometabolic disease. Nature Reviews Endocrinology, 22, 8. https://doi.org/10.1038/s41574-025-01191-z
Luo, J., Wang, Y., Mao, J., et al. (2025). Features, functions, and associated diseases of visceral and ectopic fat: A comprehensive review. Obesity, 33(5), 825–838. https://doi.org/10.1002/oby.24239
Raheem, J., Sliz, E., Shin, J., et al. (2022). Visceral adiposity is associated with metabolic profiles predictive of type 2 diabetes and myocardial infarction. Communications Medicine, 2, 81. https://doi.org/10.1038/s43856-022-00140-5
Shetty, S., Suvarna, R., Bhattacharya, S., & Seetharaman, K. (2025). Visceral adiposity and cardiometabolic risk: Clinical insights and assessment. Cardiology in Review. https://doi.org/10.1097/CRD.0000000000000984
Vicardi, M., Farzaneh-Far, A., Fava, C., Dalle Carbonare, L., & Romano, S. (2026). Epicardial and visceral adipose tissue and global longitudinal strain: A review of cardiac imaging insights in subclinical myocardial dysfunction. Nutrients, 18(6), 1009. https://doi.org/10.3390/nu18061009
Yin, Y., Zhang, J., Liu, X., et al. (2026). The combination of visceral adiposity and triglyceride-glucose indices as predictors of cardiovascular disease incidence in middle-aged and older adults. European Journal of Medical Research, 31, 332. https://doi.org/10.1186/s40001-026-03907-x