Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
Visceral fat increases heart disease risk—even in normal-weight individuals. Learn how hidden belly fat drives inflammation, cholesterol damage, and atherosclerosis.
HEARTOBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/12/202622 min read
How does visceral fat cause heart disease?
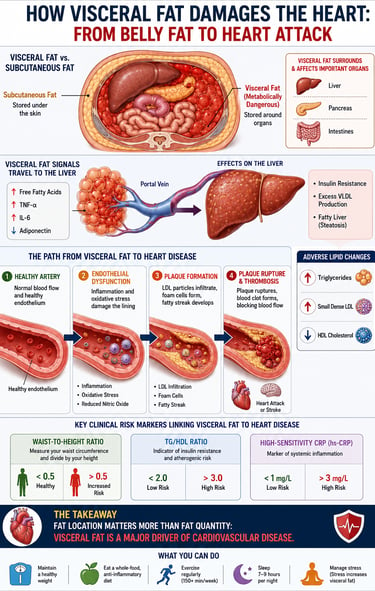
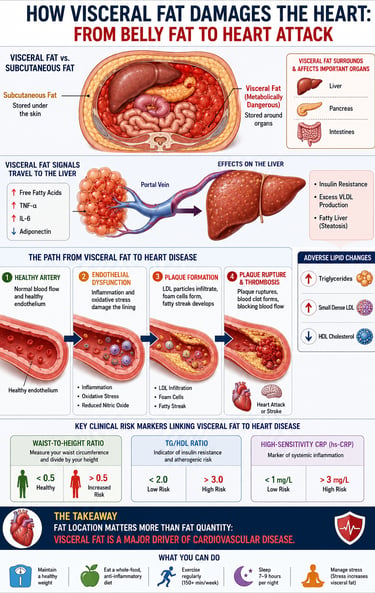
Visceral fat is deep abdominal fat that acts like a toxic organ. It releases inflammatory cytokines and free fatty acids directly into the liver through the portal vein. This triggers insulin resistance, atherogenic dyslipidemia with small dense LDL, endothelial dysfunction, and chronic inflammation. Together, these accelerate atherosclerosis and raise heart attack and stroke risk, even at a normal BMI. BMI
Visceral fat and heart disease: 3 core mechanisms
1. Inflammation: Secretes TNF-α and IL-6 that damage artery linings and destabilize plaque.
2. Atherogenic dyslipidemia: Raises triglycerides and small dense LDL, lowers protective HDL.
3. Insulin resistance: Overloads the liver with fatty acids, driving VLDL production and high blood pressure.
How to check your visceral fat risk at home
- Waist-to-height ratio: Keep it under 0.5.
- TG/HDL ratio: Aim for below 2.0. Above 3.0 signals high risk.
- Waist circumference: Men under 94 cm, women under 80 cm for most populations.
Visceral Fat and Heart Disease: Key Takeaways
1. Location beats quantity for heart risk
Visceral fat wrapped around your liver and intestines is the main driver of cardiovascular disease, not total body fat or BMI. You can have a normal BMI and still be high risk if visceral fat is elevated.
2. BMI misses the real danger
The TOFI phenotype, Thin Outside Fat Inside, proves BMI can't detect visceral fat. Waist circumference, waist-to-height ratio > 0.5, and TG/HDL ratio > 3.0 are better predictors of cardiometabolic risk.
3. Visceral fat acts like a toxic organ
It pumps inflammatory cytokines like TNF-α and IL-6, free fatty acids, and low adiponectin directly into your portal vein. That overloads your liver and triggers a cascade of insulin resistance, VLDL overproduction, and systemic inflammation.
4. It creates the worst lipid profile
Visceral fat drives atherogenic dyslipidemia: small, dense LDL that penetrates artery walls easily, high triglycerides, and low HDL. Your standard LDL-C can look fine while sdLDL is silently damaging arteries.
5. Atherosclerosis gets accelerated at every stage
Cytokines from visceral fat cause endothelial dysfunction, promote LDL oxidation, fuel foam cell formation, and make plaque caps unstable. This is the pathway to a heart attack and stroke.
6. Insulin resistance and visceral fat feed each other
Portal fatty acids and inflammation cause hepatic and muscle insulin resistance. High insulin then promotes more visceral fat storage, sodium retention, and vascular thickening. That is metabolic syndrome in action.
7. 2024 to 2026 research confirms causality, not just correlation
Multiple prospective cohorts show visceral fat volume and its trajectory independently predict carotid atherosclerosis, arterial stiffness, and CVD across all CKM stages. Risk rises with cumulative exposure, even after adjusting for traditional factors.
8. It is reversible with targeted changes
Visceral fat responds faster than subcutaneous fat to resistance training, HIIT, Zone 2 cardio, cutting refined carbs and sugary drinks, and Mediterranean-style eating. Metabolic markers like triglycerides and insulin sensitivity improve in 2 to 4 weeks, before the scale moves. GLP-1 and SGLT2 medications also reduce it when needed.
Visceral Fat and Heart Disease: Why Hidden Belly Fat Is Your Heart's #1 Hidden Enemy
You step on the scale. Normal. Your BMI looks fine. So why is your cardiologist worried?
Because the most dangerous fat in your body is invisible — it doesn't jiggle, it doesn't show up in your BMI, and it won't appear until it has already spent years quietly damaging your heart.
Visceral fat — the deep abdominal fat wrapped around your liver, pancreas, and intestines — is now recognized as a causal driver of cardiovascular disease, not merely a bystander. It functions less like storage tissue and more like a malfunctioning endocrine organ, flooding your bloodstream and liver with inflammatory chemicals 24 hours a day.
A growing body of research from 2025–2026 confirms what clinicians have long suspected: fat location, not fat quantity, is the dominant determinant of cardiometabolic risk. You can have a perfectly normal weight and still be silently developing atherosclerosis, insulin resistance, and atherogenic dyslipidemia — driven entirely by excess visceral fat.
In this article, you'll learn exactly how visceral fat attacks your cardiovascular system at the molecular level, how to assess your own risk using simple tools, and what interventions the evidence actually supports.
1. What Is Visceral Fat — And Why Is It Different?
Body fat is not one uniform substance. There are two fundamentally distinct types:
Subcutaneous fat sits just beneath your skin — the fat you can pinch on your belly, thighs, and arms. While excess subcutaneous fat isn't ideal, it is metabolically relatively benign.
Visceral fat is stored deep inside the abdominal cavity, surrounding your internal organs. This is the fat you cannot pinch. And this is the fat that kills.
The key difference lies in biology. Visceral adipose tissue (VAT) is an active endocrine organ that continuously secretes:
Pro-inflammatory cytokines — TNF-α, IL-6, MCP-1
Free fatty acids — released directly into the portal vein feeding your liver
Adipokines — including excess leptin and critically low adiponectin
Subcutaneous fat drains into the systemic circulation. Visceral fat drains directly into the portal circulation — the blood supply that flows straight to your liver. This means your liver receives the full, concentrated cytokine payload from visceral fat before any dilution occurs. The resulting cascade of hepatic insulin resistance, VLDL overproduction, and systemic inflammation is the opening act in cardiovascular disease.
2. The TOFI Problem: Why BMI Lies to Your Doctor
BMI — Body Mass Index — calculates your weight relative to your height. It was designed as a population-level screening tool in the 19th century. It was never intended to measure metabolic health, fat distribution, or cardiovascular risk.
Its central flaw: BMI cannot distinguish between muscle, subcutaneous fat, and visceral fat.
This gave rise to the TOFI phenotype: Thin Outside, Fat Inside. Sometimes called "metabolically obese normal weight" (MONW), TOFI individuals appear lean by conventional measures yet harbour dangerous quantities of visceral fat invisible to their BMI.
A landmark 2025 study published in the European Journal of Preventive Cardiology (Makhmudova et al.) directly tested this. Researchers measured visceral adipose tissue, aortic distensibility, and atherosclerotic cardiovascular risk across every BMI category. The finding was unambiguous: high visceral fat predicted impaired aortic distensibility and elevated atherosclerotic risk even in individuals with completely normal BMI. Fat location — not fat quantity — was the decisive cardiovascular variable.
This has critical implications for South Asian populations, where visceral fat accumulation occurs at substantially lower body weights than in Western populations. Standard BMI thresholds systematically underestimate cardiometabolic risk in these groups.
The clinical bottom line: BMI is not a cardiovascular risk tool. Waist circumference and waist-to-height ratio are.
3. How Visceral Fat Attacks Your Heart: The Biology
Understanding why visceral fat is so dangerous requires understanding what happens when it malfunctions.
The Dysregulated Endocrine Organ
Loss of Cardioprotection: Healthy fat tissue produces adiponectin—a hormone that protects arteries and improves insulin sensitivity. As visceral fat grows, its adiponectin production drops sharply.
The Cellular "Flip": According to a landmark 2022 BMC Medicine study, visceral fat eventually switches its immune cells from a helpful, anti-inflammatory state (M2 macrophages) to a hostile, pro-inflammatory state (M1 macrophages).
Inflammatory Molecule Factory: This cellular flip turns visceral fat into a factory that continuously pumps out destructive molecules directly into your system:
TNF-α: Drives insulin resistance and damages blood vessel linings.
IL-6: Forces the liver to mass-produce C-Reactive Protein (CRP), fueling body-wide inflammation.
MCP-1: Pulls aggressive immune cells straight into artery walls to form plaque.
Excess Leptin: Overstimulates the nervous system and encourages blood clotting.
PAI-1: Blocks the body’s natural ability to dissolve blood clots, heavily increasing heart attack risk.
Excess VLDL: Floods the bloodstream with the exact lipid particles that build arterial plaque.
The "Portal Pipeline"
Lethal Anatomy: Unlike the fat under your skin, visceral fat is uniquely dangerous because it drains directly into the portal vein—the highway straight to your liver.
The Liver Toxic Dump: This direct pipeline overloads the liver with three highly damaging compounds:
Fatty Acids (NEFA): Forces the liver to package and export massive amounts of dangerous, artery-clogging VLDL.
Cytokines (IL-6, TNF-α): Triggers severe liver insulin resistance, which accelerates VLDL production even further.
Endocannabinoids: Chemical signals that trap the liver in a loop of storing fat inside itself (causing fatty liver disease).
The Bottom Line: This continuous overload of the portal vein is the exact biochemical engine behind atherogenic dyslipidemia—the specific, aggressive cholesterol profile that drives rapid artery clogging, plaque instability, and heart attacks.
4. The Atherosclerosis Cascade: Step by Step
Atherosclerosis — the progressive hardening, narrowing, and eventual blockage of arteries — is the underlying process behind most heart attacks and strokes. Visceral fat accelerates every stage.
Stage 1: Endothelial Dysfunction
The endothelium is the single-cell-thick inner lining of every blood vessel. It is exquisitely sensitive to inflammatory cytokines. TNF-α and IL-6 from visceral fat reduce nitric oxide (NO) production — the molecule that keeps vessels relaxed and protected — while generating reactive oxygen species (ROS) that damage the arterial wall. Endothelial dysfunction is the very first step in atherosclerosis, preceding visible plaque by years or decades.
Stage 2: LDL Retention and Oxidation
Damaged endothelium allows ApoB-containing lipoproteins — particularly small dense LDL (sdLDL) particles — to penetrate and become trapped within the arterial wall. Trapped in an inflammatory environment, LDL undergoes oxidation into oxidized LDL (oxLDL): one of the most potent drivers of plaque formation known.
Stage 3: Foam Cell Formation and Fatty Streaks
Macrophages (immune cells) are recruited to the site of oxidized LDL accumulation. They engulf the oxLDL particles, becoming bloated "foam cells." These foam cells accumulate into fatty streaks — the earliest visible lesion of atherosclerosis — which then progressively develop into complex fibrous plaques.
Stage 4: Plaque Instability and Rupture
Chronic inflammation — maintained continuously by visceral fat's cytokine output — progressively thins the fibrous cap protecting atherosclerotic plaques. When an unstable plaque ruptures, it triggers acute thrombus (blood clot) formation. If this clot occludes a coronary artery: myocardial infarction. If it occludes a cerebral artery: stroke.
A 2025 study in Communications Medicine (de Souza et al.) provided direct imaging evidence for this entire pathway: both visceral adipose tissue volume and hepatic fat content were independent determinants of carotid artery atherosclerosis — a validated surrogate for coronary artery disease — after adjusting for all conventional cardiovascular risk factors.
5. Atherogenic Dyslipidemia: The Lipid Fingerprint of Visceral Fat
Visceral fat doesn't simply raise LDL cholesterol. It generates a specific, highly dangerous lipid pattern called atherogenic dyslipidemia, characterized by three simultaneous abnormalities.
Small Dense LDL (sdLDL): The Most Dangerous Cholesterol Particle
Standard LDL cholesterol tests measure total LDL mass. They do not distinguish between large, fluffy LDL particles (relatively benign) and small, dense LDL (sdLDL) — particles that are categorically more dangerous:
Small enough to penetrate deeply into the arterial wall
Longer half-life in circulation
Stronger binding affinity for arterial proteoglycans
Far more susceptible to oxidation into the highly inflammatory oxLDL
A comprehensive 2022 review by Jin et al. in Frontiers in Cardiovascular Medicine detailed the full mechanism: visceral fat stimulates hepatic VLDL overproduction → excess VLDL undergoes remodeling via cholesteryl ester transfer protein (CETP) and hepatic lipase → sdLDL particles are produced.
Your standard lipid panel will likely not reveal this. You can appear to have "acceptable" LDL-C while your arteries are being aggressively damaged by sdLDL.
Elevated Triglycerides
Visceral fat has exceptionally high lipolytic activity — it continuously releases fatty acids into the portal circulation. The liver responds by packaging these excess fatty acids into triglyceride-rich VLDL particles and secreting them into the bloodstream. Chronically elevated triglycerides are an independent cardiovascular risk factor and are the direct substrate for sdLDL production.
Low HDL Cholesterol
HDL performs reverse cholesterol transport: it collects cholesterol from peripheral tissues and arterial walls and returns it to the liver for disposal. In visceral obesity, HDL levels fall and HDL quality deteriorates. The net result is impaired removal of cholesterol from developing atherosclerotic plaques, accelerating their growth.
The TG/HDL Ratio: A Powerful Bedside Tool
TG/HDL Ratio (mg/dL) Clinical Interpretation < 2.0 Low risk; favorable lipid pattern 2.0 – 3.0 Borderline; monitor closely > 3.0 High risk; likely sdLDL predominance, probable insulin resistance > 5.0 Very high risk; strong indicator of metabolic syndrome
The TG/HDL ratio requires no special testing — it is calculable from any standard fasting lipid panel. Despite its simplicity, it serves as a highly specific surrogate marker for insulin resistance and sdLDL particle predominance, providing actionable cardiovascular risk information that standard cholesterol testing alone cannot offer.
6. Chronic Inflammation: The Slow Fire That Burns Your Arteries
If atherogenic dyslipidemia is the fuel of cardiovascular disease, chronic low-grade inflammation is the spark that ignites it — and visceral fat keeps that spark burning indefinitely.
The inflammatory profile of visceral obesity is not the acute inflammation you feel during an infection. It is a para-inflammatory state — below the threshold of obvious symptoms, but persistent enough to progressively damage endothelium, destabilize plaques, and drive a pro-thrombotic environment.
Key inflammatory biomarkers elevated in visceral obesity:
hs-CRP — the most clinically available marker of vascular inflammation; levels above 3.0 mg/L signal high cardiovascular risk
IL-6 — the primary driver of hepatic CRP production; an independent cardiovascular risk predictor
TNF-α — simultaneously promotes insulin resistance and endothelial dysfunction
MCP-1 — facilitates monocyte recruitment into arterial walls, directly accelerating plaque formation
Fibrinogen and PAI-1 — create a pro-thrombotic state that makes arterial clot formation more likely if a plaque ruptures
A 2022 review in the Journal of Obesity (Guerreiro et al.) systematically documented the role of macrophage infiltration in visceral fat — specifically the shift from anti-inflammatory M2 to pro-inflammatory M1 macrophage polarization — as the cellular mechanism that transitions visceral fat from metabolically manageable to actively pathological.
7. Visceral Fat and Insulin Resistance: A Vicious Cycle
Visceral fat and insulin resistance are locked in a mutually reinforcing loop — each making the other worse, and together dramatically amplifying cardiovascular risk.
How visceral fat causes insulin resistance:
Portal free fatty acid overload → hepatic insulin resistance → impaired glucose regulation and amplified VLDL secretion
Pro-inflammatory cytokines (TNF-α, IL-6) → skeletal muscle insulin resistance → impaired peripheral glucose disposal
Adiponectin deficiency → loss of a critical insulin-sensitising signal
Ectopic fat deposition in the liver and muscle → direct intracellular insulin signaling impairment
How insulin resistance worsens cardiovascular disease:
Chronically elevated insulin (hyperinsulinemia) is not metabolically neutral:
Increases renal sodium retention → raises blood pressure
Amplifies sympathetic nervous system activity → further elevates blood pressure and heart rate
Promotes vascular smooth muscle cell proliferation → directly contributes to arterial wall thickening
This is why visceral fat sits at the mechanistic center of metabolic syndrome — the cluster of hypertension, dysglycemia, atherogenic dyslipidemia, and abdominal obesity that multiplies cardiovascular risk far beyond the sum of its parts.
8. What the Latest Research Says (2024–2026)
The evidence base linking visceral fat to cardiovascular outcomes has expanded substantially in recent years, with large prospective cohort studies providing compelling data.
He et al. (2024) — Nutrition, Metabolism and Cardiovascular Diseases Following a prospective cohort over time, this study found that visceral adiposity was associated not just with the incidence of cardiometabolic disease but with its developmental trajectory — meaning higher visceral fat actively accelerated disease progression, not merely its onset. This has profound implications for the timing of intervention.
Wang et al. (2026) — BMC Cardiovascular Disorders This prospective cohort study examined associations between visceral fat accumulation and cardiovascular disease across cardiovascular-kidney-metabolic (CKM) syndrome stages 0–3. A critical finding was that arterial stiffness mediated a significant portion of visceral fat's cardiovascular effect — identifying arterial stiffness as an important intermediate target for intervention.
Xu & Sun (2026) — The Aging Male Drawing on two independent prospective cohorts, this study demonstrated that dynamic trajectories of visceral fat — not just its baseline level — were critical determinants of cardiovascular disease onset. Individuals whose visceral fat consistently increased over time faced substantially higher cardiovascular risk than those with stable or declining visceral fat, even after controlling for baseline levels.
Chen & Fang (2026) — BMC Cardiovascular Disorders Using the CHARLS database (one of the most comprehensive longitudinal datasets of middle-aged and older Chinese adults), this study demonstrated a graded, dose-dependent relationship between cumulative visceral fat exposure and cardiovascular disease risk across all stages of CKM syndrome — an association that persisted after adjustment for all traditional risk factors.
Li et al. (2026) — Frontiers in Endocrinology Extending the evidence beyond coronary artery disease, this prospective cohort study in hypertensive patients demonstrated that elevated metabolic scores for visceral fat were significantly and independently associated with peripheral arterial disease — confirming that visceral fat's vascular damage is systemic, not limited to the heart.
Bielinski, St. Sauver & Borlaug (2026) — Progress in Cardiovascular Diseases This editorial argued specifically that visceral adipose tissue should be formally incorporated as a biomarker in cardiovascular disease risk assessment, noting its superior predictive capacity relative to BMI in metabolically ambiguous patients.
9. Who Is Most at Risk? Special Clinical Scenarios
The TOFI Patient: Normal Weight, Hidden Danger
The TOFI phenotype deserves particular clinical attention because these individuals are most likely to be falsely reassured by conventional risk assessment. Normal BMI, no overt obesity, possibly even normal total cholesterol — yet they harbour visceral fat volumes that confer significantly elevated atherosclerotic risk. The Makhmudova et al. (2025) study explicitly confirmed this across BMI categories.
Red flags for TOFI in clinical practice:
TG/HDL ratio > 3.0 with normal or borderline BMI
Waist-to-height ratio > 0.5 despite apparent leanness
Fasting glucose trending above 5.6 mmol/L
Fatty liver on ultrasound in a patient with normal weight
Sarcopenic Obesity
This increasingly common phenotype combines low skeletal muscle mass with elevated visceral fat. Reduced muscle mass severely limits glucose disposal capacity — dramatically amplifying insulin resistance already driven by visceral fat. The cardiovascular risk in sarcopenic obesity exceeds that of either condition alone.
Visceral Fat and Aging
Aging drives a progressive redistribution of body fat toward visceral depots — even without any change in total body weight. Declining testosterone, estrogen, growth hormone, and shifts in cortisol metabolism all promote visceral accumulation with age. A landmark 2026 review in Nature Aging (Maeyens et al.) comprehensively documented how visceral adiposity interacts with aging biology to amplify cardiovascular and metabolic disease risk — establishing visceral fat monitoring as essential in healthy aging strategies.
South Asian Populations
South Asian individuals accumulate visceral fat and develop cardiometabolic complications at lower BMI thresholds than populations of European descent. Standard BMI and waist circumference cutoffs significantly underestimate risk in this group. A waist circumference above 90 cm in men and 80 cm in women warrants clinical attention in South Asian adults — thresholds lower than those recommended by current Western guidelines.
10. How to Assess Your Visceral Fat Risk Right Now
You do not need a CT scanner or MRI to meaningfully assess visceral fat risk. The following evidence-based tools are available at home or in any clinic.
Step 1: Waist Circumference
Measure at the level of your navel, after exhaling normally:
Population Men (elevated risk) Women (elevated risk) European/Western > 94 cm (37 in) > 80 cm (31.5 in) South Asian > 90 cm (35.5 in) > 80 cm (31.5 in) High risk threshold > 102 cm (40 in) > 88 cm (34.6 in)
Step 2: Waist-to-Height Ratio (WtHR)
Divide your waist circumference by your height (same units).
WtHR > 0.5 = elevated cardiometabolic risk in most adult populations
WtHR > 0.6 = high risk
Example: 5'10" (178 cm) tall? Your waist should be under 89 cm.
This single ratio performs better than BMI across ethnic groups for predicting cardiovascular and metabolic risk.
Step 3: TG/HDL Ratio
From a fasting lipid panel: Triglycerides (mg/dL) ÷ HDL (mg/dL)
< 2.0: Low risk
2.0–3.0: Monitor
> 3.0: High risk — likely sdLDL predominance and insulin resistance
Step 4: Additional Biomarkers
Fasting glucose / HbA1c — early insulin resistance and prediabetes detection
hs-CRP — quantifies systemic vascular inflammation; > 3.0 mg/L = high cardiovascular risk
ApoB — most precise measure of atherogenic particle burden when available
Fasting insulin — direct measurement of insulin resistance
When to Consider Advanced Imaging
If simple measures raise concern, clinicians may proceed to:
DEXA — precise body composition, visceral fat estimation
Abdominal CT or MRI — gold standard for VAT quantification
Liver ultrasound — assessment of hepatic steatosis (fatty liver), a marker of visceral fat burden
11. Evidence-Based Strategies to Reduce Visceral Fat
Nutrition: The Dietary Framework That Works
What the evidence supports:
Reduce refined carbohydrates and added sugars — this directly suppresses hepatic VLDL production and visceral fat deposition. Sugar-sweetened beverages are particularly potent drivers of visceral fat accumulation and should be eliminated.
Mediterranean dietary pattern — consistently shown in clinical trials to reduce visceral fat and cardiovascular risk. Key elements: olive oil, fatty fish, legumes, vegetables, whole grains, nuts.
Adequate dietary protein — increases satiety, preserves muscle mass during weight loss, and improves insulin sensitivity.
Avoid ultra-processed foods — independently associated with visceral fat accumulation and cardiovascular disease, beyond their caloric contribution.
Practical dietary checklist:
[ ] Eliminate all sugar-sweetened beverages (including fruit juice)
[ ] Reduce refined grains (white bread, white rice, pasta) to < 1 serving/day
[ ] Add 2+ servings of fatty fish per week (salmon, sardines, mackerel)
[ ] Use olive oil as primary cooking fat
[ ] Include legumes (lentils, chickpeas, beans) 4–5 times per week
[ ] Eat vegetables at every meal
Exercise: The Most Targeted Tool for Visceral Fat
Exercise reduces visceral fat through mechanisms beyond simple calorie burning — and crucially, it reduces visceral fat even without significant total body weight loss. This is one of the most clinically important facts in this entire article.
Resistance training is the most insulin-sensitizing form of exercise. Building muscle mass directly improves glucose disposal capacity, reducing the metabolic burden that drives visceral fat accumulation. Myokines — signalling molecules released by contracting muscle — specifically promote visceral fat lipolysis.
High-Intensity Interval Training (HIIT) has the strongest evidence for preferential visceral fat reduction. Even short HIIT sessions (15–20 minutes, 2–3 times per week) consistently outperform moderate-intensity steady-state cardio for visceral fat loss in head-to-head trials.
Zone 2 aerobic training (sustained moderate intensity — you can hold a conversation but are clearly working) enhances mitochondrial fat oxidation capacity and supports long-term visceral fat management. Aim for 150+ minutes per week.
Practical exercise template (evidence-based minimum):
Monday: Resistance training (40–50 min)
Tuesday: Zone 2 cardio like a brisk walk or cycling (30–45 min)
Wednesday: Rest or gentle, low-impact movement
Thursday: Resistance training (40–50 min)
Friday: HIIT session (20 min)
Saturday: Zone 2 cardio (45–60 min)
Sunday: Rest
Sleep and Stress: The Underestimated Drivers
Short sleep duration (< 6 hours/night) independently promotes visceral fat accumulation via cortisol dysregulation and appetite-regulating hormone disruption. Prioritizing 7–9 hours of quality sleep is a genuine visceral fat intervention.
Chronic psychological stress elevates cortisol, which directly promotes visceral fat deposition. Structured stress reduction (mindfulness, cognitive behavioral techniques, social support) has measurable cardiometabolic benefits.
Pharmacological Options
When lifestyle interventions are insufficient or when cardiovascular risk is high:
GLP-1 receptor agonists (semaglutide, liraglutide) — demonstrated significant visceral fat reduction in clinical trials alongside major cardiovascular outcome benefits in high-risk populations
SGLT2 inhibitors (empagliflozin, dapagliflozin) — cardiometabolic protection through multiple mechanisms including visceral fat reduction, blood pressure lowering, and direct cardiac benefits
Statins — reduce LDL-C and stabilize atherosclerotic plaques; address downstream cardiovascular risk even when visceral fat remains elevated
Always discuss pharmacological options with your physician. These medications carry specific indications, contraindications, and require medical supervision.
12. Visceral Fat Reduction Timeline: What to Expect
What Changes, and When?
2–4 Weeks: Improved Metabolic Function – Enhanced insulin sensitivity and a reduction in post-meal blood glucose spikes.
4–8 Weeks: Lipid & Energy Shifts – Lower fasting triglycerides, alongside noticeable improvements in daily energy and mood.
2–3 Months: Systemic Inflammation Drops – Measurable reductions in triglycerides, increases in "good" HDL cholesterol, and a decrease in hs-CRP (a key inflammation marker).
3–6 Months: Physical Shifts – Visible reduction in waist circumference and a highly improved TG/HDL ratio.
6–12 Months: Internal Structural Changes – Measurable reduction in actual visceral fat volume, verifiable through medical imaging.
1–3 Years: Cardiovascular Repair – Stabilization of arterial plaque and potential partial regression of early-stage atherosclerosis.
The Bottom Line
Metabolic health improves long before the scale moves. Do not let a slow-moving scale discourage you. Your internal biology, liver health, and blood vessels are actively healing and changing well before your waistline noticeably shifts. Trust the process—the internal victory comes first.
13. Common Myths and Mistakes
Myth 1: "My BMI is normal, so my heart risk is low." False. The TOFI phenotype (Thin Outside, Fat Inside) establishes unequivocally that normal BMI does not rule out high visceral fat or elevated cardiovascular risk. Waist circumference and waist-to-height ratio are essential additional assessments.
Myth 2: "I just need to lose weight — any fat loss is the same." Not so. Visceral fat and subcutaneous fat respond differently to different interventions. Exercise specifically preferentially reduces visceral fat even in the absence of total weight loss — a phenomenon documented in multiple controlled trials. The location of fat loss matters more than the amount.
Myth 3: "Cardio is the best exercise for heart health." Moderate steady-state cardio has benefits, but resistance training and HIIT are superior for visceral fat reduction and insulin sensitivity improvement. A complete program includes all three modalities.
Myth 4: "My cholesterol levels are fine, so I'm not at risk." Standard LDL cholesterol testing does not detect sdLDL predominance or atherogenic dyslipidemia. A "normal" LDL-C with a TG/HDL ratio above 3.0 indicates significant hidden cardiovascular risk.
Myth 5: "Visceral fat only matters if you're obese." Visceral fat is dangerous across all BMI categories. Some individuals of normal BMI have high-risk visceral fat levels. Conversely, some individuals with elevated BMI have metabolically favorable fat distribution. BMI and visceral fat risk are not the same thing.
Mistake: Ignoring the TG/HDL ratio on your lipid panel. This simple calculation is one of the most informative cardiovascular risk markers available from a routine blood test. If your triglycerides are above 150 mg/dL and HDL is below 50 mg/dL — calculate the ratio and discuss it with your doctor.
14. Frequently Asked Questions
Q: Does visceral fat directly cause heart disease, or is it just a marker?
Visceral fat is now considered a causal driver of cardiovascular disease, not merely an associated marker. Through chronic inflammation, atherogenic dyslipidemia, endothelial dysfunction, and insulin resistance, visceral fat actively initiates and accelerates the atherosclerotic processes that underlie most heart attacks and strokes. The causal mechanisms are well-characterized at the molecular level.
Q: Can I have significant heart disease risk with a normal BMI?
Yes — and this is one of the most important clinical facts in modern cardiovascular medicine. The TOFI phenotype demonstrates clearly that individuals with completely normal BMI can carry dangerous levels of visceral fat and face disproportionately elevated cardiovascular risk. Makhmudova et al. (2025) confirmed elevated atherosclerotic risk associated with high visceral fat even in the normal BMI category. This is precisely why waist circumference and waist-to-height ratio must be assessed alongside BMI.
Q: What is small dense LDL and why is it more dangerous than regular LDL?
sdLDL is a subtype of LDL cholesterol characterized by smaller particle size and higher density. These properties make it significantly more atherogenic: sdLDL particles more readily penetrate arterial walls, bind more tightly to arterial proteoglycans, remain in circulation longer, and are more susceptible to oxidation into the highly inflammatory oxLDL. Visceral fat specifically promotes sdLDL production via hepatic VLDL overproduction and CETP-mediated remodeling. Standard LDL cholesterol testing cannot detect sdLDL predominance.
Q: What TG/HDL ratio should I be aiming for?
Aim for a TG/HDL ratio below 2.0 (measured in mg/dL). A ratio between 2.0 and 3.0 warrants monitoring and lifestyle attention. A ratio above 3.0 strongly suggests insulin resistance, sdLDL predominance, and elevated cardiometabolic risk requiring active intervention and clinical review.
Q: How long does it take to reduce visceral fat?
Metabolic improvements (insulin sensitivity, triglycerides, inflammation) begin within 2–4 weeks of consistent lifestyle change. Measurable reductions in waist circumference typically emerge within 3–6 months. Significant visceral fat volume reduction on imaging generally requires 6–12 months of sustained intervention. Importantly, metabolic benefits precede visible changes — do not use the scale as your primary progress marker.
Q: Does exercise reduce visceral fat even without weight loss?
Yes — this is one of the most clinically important facts in exercise medicine. Multiple controlled trials demonstrate that both resistance training and HIIT reduce visceral fat independently of total body weight loss. The mechanisms include myokine signaling that specifically promotes visceral fat lipolysis, improved insulin sensitivity that reduces visceral fat deposition, and the browning effect on white adipose tissue. You can be getting metabolically healthier long before the scale moves.
Q: Is visceral fat reversible?
Yes, visceral fat is highly responsive to lifestyle intervention — more so than subcutaneous fat. A combination of dietary carbohydrate reduction, resistance training, and HIIT produces consistent, measurable visceral fat reduction in clinical trials. This reversibility is one of the most encouraging aspects of visceral fat biology: meaningful cardiovascular risk reduction is achievable through targeted lifestyle change.
Q: How does aging affect visceral fat?
Aging drives progressive visceral fat accumulation even without weight gain, driven by declining sex hormones (estrogen, testosterone), growth hormone, and shifts in cortisol metabolism. A comprehensive 2026 review in Nature Aging (Maeyens et al.) documented this interaction in detail. The practical implication: active lifestyle strategies become progressively more important — not less — as you age. Monitoring waist circumference and TG/HDL ratio should be part of routine health assessment from middle age onward.
Q: Should I ask my doctor for advanced lipid testing?
If your TG/HDL ratio is above 3.0, waist-to-height ratio is above 0.5, or you have other risk factors — yes. ApoB measurement provides the most precise assessment of total atherogenic particle burden. ApoB is superior to LDL-C for cardiovascular risk prediction in patients with metabolically discordant lipid profiles and is increasingly available in routine clinical chemistry panels.
Q: Can medications reduce visceral fat?
GLP-1 receptor agonists (semaglutide, liraglutide) have demonstrated significant visceral fat reduction in randomized controlled trials alongside major cardiovascular outcome benefits. SGLT2 inhibitors also provide cardiometabolic protection through mechanisms that include visceral fat reduction. These options are appropriate in higher-risk patients when lifestyle changes are insufficient — always in consultation with a physician.
15. Your Action Plan: Start Protecting Your Heart This Week
This Week
[ ] Measure your waist circumference
[ ] Calculate your waist-to-height ratio (should be < 0.5)
[ ] Request a fasting lipid panel and calculate your TG/HDL ratio
[ ] Eliminate all sugar-sweetened beverages and ultra-processed snacks
[ ] Begin walking 30 minutes daily
This Month
[ ] Begin resistance training 2–3 times per week
[ ] Add 2 HIIT sessions per week (20 minutes each)
[ ] Shift your diet toward a Mediterranean-style pattern
[ ] Prioritize 7–9 hours of sleep per night
This Quarter
[ ] Book a cardiovascular risk review with your doctor
[ ] Share your waist circumference and TG/HDL ratio at that visit
[ ] If hs-CRP is elevated, discuss further cardiovascular assessment
[ ] Consider ApoB testing if TG/HDL > 3.0
Long-Term (6–18 months)
[ ] Reassess waist circumference and TG/HDL ratio every 3 months
[ ] Consider DEXA body composition analysis if risk factors persist
[ ] Discuss pharmacological options with your physician if lifestyle changes prove insufficient
Important: This article is for informational and educational purposes only. It does not constitute medical advice. Always consult a qualified healthcare professional before making significant changes to your diet, exercise program, or medications — especially if you have existing health conditions.
Conclusion
Visceral fat is not a passive storage depot. It is a biologically active, metabolically aggressive tissue that works against your cardiovascular health every hour of every day — through chronic inflammation, atherogenic dyslipidemia, insulin resistance, and endothelial dysfunction.
The most important shift in cardiovascular medicine over the past decade is the recognition that fat location matters far more than fat quantity. Your BMI can be perfectly normal while visceral fat silently accelerates atherosclerosis, impairs your metabolism, and elevates your risk of a heart attack or stroke.
But here is the genuinely good news: visceral fat is one of the most modifiable cardiovascular risk factors we have. It responds to targeted lifestyle intervention within weeks. Metabolic improvements begin before the scale moves. And the evidence from 2024–2026 is unambiguous: reducing visceral fat reduces cardiovascular risk in a graded, dose-dependent fashion.
Measure. Assess. Act.
Your heart cannot see your scale. But it registers every metabolic change you make.
This article is intended for educational purposes and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment decisions.
Related Articles
High BCAA Levels Could Signal Dangerous Visceral Fat—Here's What New Research Shows
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Bielinski, S. J., St. Sauver, J. L., & Borlaug, B. A. (2026). Visceral adiposity tissue: A promising biomarker to improve cardiovascular disease risk assessment. Progress in Cardiovascular Diseases, 94, 63–64. https://doi.org/10.1016/j.pcad.2026.01.003
Chen, Q., & Fang, H. (2026). Association between cumulative metabolic score for visceral fat and cardiovascular disease risk in cardiovascular-kidney-metabolic syndrome stage 0–3 patients: A prospective cohort analysis based on CHARLS database. BMC Cardiovascular Disorders. https://doi.org/10.1186/s12872-026-05801-0
de Souza, R. J., Pigeyre, M. E., Schulze, K. M., et al. (2025). Visceral adipose tissue and hepatic fat as determinants of carotid atherosclerosis. Communications Medicine, 5, 424. https://doi.org/10.1038/s43856-025-01123-y
Guerreiro, V. A., Carvalho, D., & Freitas, P. (2022). Obesity, adipose tissue, and inflammation answered in questions. Journal of Obesity, 2022, 2252516. https://doi.org/10.1155/2022/2252516
He, Q., Wang, Y., Feng, Z., et al. (2024). Visceral adiposity associated with incidence and development trajectory of cardiometabolic diseases: A prospective cohort study. Nutrition, Metabolism and Cardiovascular Diseases, 34(5), 1235–1244. https://doi.org/10.1016/j.numecd.2023.11.006
Jin, X., Yang, S., Lu, J., & Wu, M. (2022). Small, dense low-density lipoprotein-cholesterol and atherosclerosis: Relationship and therapeutic strategies. Frontiers in Cardiovascular Medicine, 8, 804214. https://doi.org/10.3389/fcvm.2021.804214
Kolb, H. (2022). Obese visceral fat tissue inflammation: From protective to detrimental? BMC Medicine, 20, 494. https://doi.org/10.1186/s12916-022-02672-y
Li, S., Yan, C., Wu, M., et al. (2026). The metabolic score for visceral fat and risk of peripheral arterial disease in hypertension patients: A prospective cohort study. Frontiers in Endocrinology, 17, 1764481. https://doi.org/10.3389/fendo.2026.1764481
Maeyens, L. T., Nelson, J. F., & Zhao, S. (2026). Visceral adiposity, metabolic health and aging. Nature Aging, 6, 506–519. https://doi.org/10.1038/s43587-026-01076-4
Makhmudova, U., Wild, B., Williamson, A., et al. (2025). Visceral adipose tissue, aortic distensibility and atherosclerotic cardiovascular risk across body mass index categories. European Journal of Preventive Cardiology, zwaf447. https://doi.org/10.1093/eurjpc/zwaf447
Nath, K. (2026). Obesity, visceral adiposity, and cardiometabolic complications: Limelight, February 2026. Mayo Clinic Proceedings, 101, 205–207.
Wang, K., Luo, X., Wan, D., et al. (2026). Associations of visceral fat accumulation with cardiovascular disease across cardiovascular-kidney-metabolic syndrome stages 0–3: Mediation effects of arterial stiffness in a prospective cohort study. BMC Cardiovascular Disorders, 26, 387. https://doi.org/10.1186/s12872-026-05775-z
Xu, L., & Sun, M. (2026). Correlations between the cumulative metabolic score for visceral fat and its dynamic trajectories with the onset of cardiovascular disease in middle-aged and older adults: Findings from two prospective cohorts. The Aging Male, 29(1). https://doi.org/10.1080/13685538.2026.2650602
American Heart Association. Extra belly weight, not BMI, was a stronger predictor of heart failure risk and inflammation. https://newsroom.heart.org/news/extra-belly-weight-not-bmi-was-a-stronger-predictor-of-heart-failure-risk-inflammation