Visceral Fat vs Subcutaneous Fat: The Hidden Belly Fat Driving Diabetes and Heart Disease
Visceral fat is the most dangerous fat in your body. Learn how it causes insulin resistance, fatty liver, and heart disease—and how to measure and reduce it effectively.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/1/202616 min read
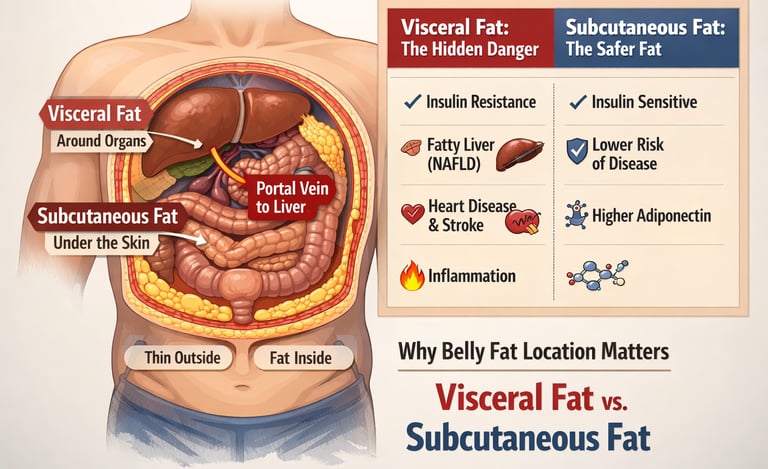
Why Belly Fat Is More Dangerous Than Other Fat
Belly fat is dangerous because it often includes visceral fat, which drains directly into the liver via the portal vein. This increases liver fat, insulin resistance, and triglycerides, making abdominal obesity a major driver of metabolic syndrome and heart disease.
Visceral fat directly damages the liver through the portal circulation.
How Visceral Fat Causes Insulin Resistance
This mechanism explains why visceral fat is uniquely harmful.
Free fatty acids flow directly to the liver
Hepatic insulin resistance develops
Glucose production increases
Triglycerides rise
This leads to fatty liver (NAFLD), hyperglycemia, and dyslipidemia.
Clinical pearls
1. The Portal Drainage Phenomenon
Scientific Perspective: Visceral Adipose Tissue (VAT) is uniquely positioned to drain directly into the portal vein. This subjects the liver to high concentrations of non-esterified fatty acids (NEFAs) and pro-inflammatory cytokines (IL-6, TNF-α), bypassing peripheral circulation and directly inducing hepatic insulin resistance and dyslipidemia.
Think of visceral fat as a "leaky pipe" that drains toxins directly into your liver. Unlike the fat under your skin, this deep belly fat sends fat and inflammation straight to your liver first, which is why it causes so much damage to your blood sugar and cholesterol.
2. The "TOFI" Paradox (Metabolic Obesity)
Scientific Perspective: BMI lacks the specificity to distinguish between fat compartments. Individuals with the "Thin-Outside-Fat-Inside" phenotype may have a normal BMI but possess a high Visceral-to-Subcutaneous Ratio (VSR), leading to a cardiometabolic risk profile identical to that of an individual with overt obesity.
You can’t judge a book by its cover, and you can’t judge your health solely by the scale. You can be "thin" but still have dangerous levels of hidden fat wrapped around your organs. Your waist size is often a much better health indicator than your total weight.
3. Ethnicity-Specific Risk Thresholds
Scientific Perspective: Adipose tissue storage capacity and distribution patterns vary significantly by ethnicity. South Asian populations exhibit lower thresholds for metabolic dysfunction, necessitating the use of lower waist circumference cut-offs (e.g., 90 cm for men) to accurately screen for Type 2 Diabetes and CVD risk.
One size does not fit all when it comes to health standards. For many people of South Asian or Southeast Asian descent, the body begins to struggle with belly fat much sooner than it does for Europeans. Don't wait for "standard" BMI charts to tell you there is a problem.
4. Preferential Mobilization of VAT
Scientific Perspective: Due to its higher density of beta-adrenergic receptors and higher blood flow, visceral fat is more metabolically active and sensitive to lipolysis than subcutaneous fat. Consequently, negative energy balance and exercise result in a disproportionately greater percentage loss of VAT compared to total body fat.
The "bad" fat is actually the easiest to lose. When you start exercising and eating better, your body prioritizes burning that dangerous internal fat first. Even if you only lose 5% of your total weight, you might be getting rid of up to 30% of the dangerous fat around your organs.
5. Adipose Tissue as an Endocrine Organ
Scientific Perspective: VAT is not an inert energy storage depot; it is an active endocrine organ. It secretes adipokines like adiponectin and resistin. In a state of visceral adiposity, the ratio shifts toward pro-inflammatory secretions, creating a state of chronic, low-grade systemic inflammation.
Your belly fat isn't just sitting there; it’s acting like a factory that produces hormones. When you have too much visceral fat, that factory starts pumping out "stress signals" that keep your whole body in a state of constant, low-level inflammation, which wears out your heart and blood vessels.
6. The Superiority of Waist-to-Height Ratio (WHtR)
Scientific Perspective: WHtR is a more robust predictor of cardiometabolic risk than BMI or waist circumference alone because it normalizes abdominal girth to body size. A ratio $> 0.5$ serves as a universal proxy for elevated visceral adiposity across different sexes and ethnicities.
Patient Perspective: There is one simple rule to remember for your health: Keep your waist below half your height. This is one of the most accurate ways to check your risk at home without needing a fancy scan or a complicated calculator.
The Hidden Fat Driving Modern Metabolic Disease
What if the most dangerous fat in your body isn’t the fat you can see—but the fat silently surrounding your organs?
For decades, obesity has been defined by body weight and body mass index (BMI). But emerging evidence in cardiometabolic medicine reveals a more critical truth: fat distribution matters far more than total fat mass. Two individuals with the same BMI can have vastly different risks of insulin resistance, Type 2 diabetes, fatty liver disease (NAFLD), and cardiovascular disease, depending on where their fat is stored (Després, 2012).
At the center of this paradigm shift is visceral fat—the metabolically active fat stored deep within the abdominal cavity. Unlike subcutaneous fat, which acts as a relatively safe energy reservoir, visceral fat functions as a pathogenic endocrine organ, releasing free fatty acids, inflammatory cytokines, and adipokines that directly impair metabolic health (Lee & Kim, 2024). Through the portal theory of insulin resistance, these substances are delivered straight to the liver via the portal vein, driving hepatic insulin resistance, increased gluconeogenesis, and dyslipidaemia—key mechanisms underlying metabolic syndrome (Shulman, 2014).
This explains a critical clinical paradox: individuals with a normal BMI may still carry excess abdominal fat and remain at high risk—a phenotype often described as “thin outside, fat inside” (TOFI). Conversely, some individuals with higher body weight but predominantly subcutaneous fat may have a more favorable metabolic profile.
Measures such as waist circumference, waist-to-height ratio, and visceral fat assessment are now recognized as superior predictors of cardiometabolic risk compared to BMI alone (Fox et al., 2007). In fact, elevated visceral adiposity is strongly linked to atherosclerosis, systemic inflammation, and premature mortality.
Understanding the difference between visceral fat vs subcutaneous fat is no longer academic—it is central to preventing and reversing modern metabolic disease.
Two Types of Fat: Not All Fat Is Created Equal
Subcutaneous Adipose Tissue (SAT): The "Safer" Fat
Subcutaneous fat sits just beneath the skin and is the fat you can pinch. It accumulates around the hips, thighs, buttocks, and the outer abdomen. While no fat is entirely without consequence, this type is generally considered metabolically protective — at least compared to its deeper counterpart.
Here's why:
It releases relatively low amounts of fatty acids into the bloodstream
It remains sensitive to insulin (meaning it responds normally to blood sugar signals)
It secretes higher amounts of adiponectin, a hormone that improves insulin sensitivity and has anti-inflammatory properties
Think of subcutaneous fat as a metabolic buffer — it absorbs excess energy and keeps it somewhat safely stored away from your vital organs. People with a predominantly "pear-shaped" body (fat stored in the hips and thighs) tend to have better metabolic profiles than those with an "apple-shaped" body, where fat is concentrated in the abdomen.
Visceral Adipose Tissue (VAT): The Hidden Danger
Visceral fat is stored inside the abdominal cavity — nestled around the liver, intestines, pancreas, and other organs. It includes omental fat (draped over intestines), mesenteric fat (surrounding intestinal blood vessels), and retroperitoneal fat (behind the abdominal organs).
Unlike subcutaneous fat, visceral fat is metabolically hyperactive. It:
Releases large amounts of free fatty acids (FFAs) directly into circulation
Secretes pro-inflammatory signals, including TNF-α, IL-6, and resistin
Produces significantly less adiponectin, disrupting normal insulin signalling
Is densely packed with immune cells — particularly inflammatory M1 macrophages — that sustain chronic low-grade inflammation
A landmark 2024 review by Lee and Kim in Biochemical Pharmacology described visceral adipose tissue as a pathogenic endocrine organ that drives systemic metabolic dysregulation through both inflammatory and hormonal pathways (Lee & Kim, 2024). Their analysis underscores that it's not simply the presence of fat, but its metabolic behaviour, that triggers disease.
The Portal Theory: How Belly Fat Attacks Your Liver
One of the most important mechanisms linking visceral fat to disease is the portal hypothesis.
Here's the key anatomical fact: visceral fat drains directly into the portal vein — the blood vessel that carries blood straight to the liver before it enters general circulation. This means that every fatty acid and inflammatory molecule released by visceral fat goes directly to the liver first, in highly concentrated amounts.
The consequences are significant:
Hepatic insulin resistance: Free fatty acids impair the liver's ability to respond to insulin by disrupting the IRS-1/PI3K signalling pathway. The liver starts producing glucose even when blood sugar is already high — a hallmark of Type 2 diabetes.
Increased gluconeogenesis: Key liver enzymes (PEPCK and G6Pase) that manufacture new glucose from non-sugar sources become overactivated, raising fasting blood sugar.
Fat accumulation in the liver: When the liver is overwhelmed by incoming fatty acids, it begins storing fat within its own cells — the beginning of Non-Alcoholic Fatty Liver Disease (NAFLD), which can progress to inflammation (NASH) and cirrhosis.
Elevated VLDL production: The liver begins overproducing VLDL particles, raising triglyceride levels and contributing to dyslipidaemia — a core feature of metabolic syndrome.
A recent 2025 cross-sectional study by Chagas and colleagues in Frontiers in Nutrition confirmed that different metabolic, dietary, and lifestyle factors independently modulate visceral and subcutaneous fat accumulation — reinforcing that these two fat compartments behave very differently and require distinct therapeutic approaches (Chagas et al., 2025).
Cardiovascular Risk: Why Visceral Fat Is Your Heart's Enemy
The link between visceral fat and cardiovascular disease is robust, consistent, and independent of total body weight.
A 2024 systematic review published in BMC Public Health by Emamat and colleagues examined the association between the visceral-to-subcutaneous abdominal fat ratio (VSR) and cardiovascular disease risk. Their findings were striking: a higher VSR was consistently associated with increased risk of coronary artery disease, stroke, and cardiovascular mortality — even after adjusting for BMI and overall body fat (Emamat et al., 2024). This means that two people with identical BMIs but different fat distributions face meaningfully different cardiac risk levels.
The mechanisms driving this cardiovascular toxicity include:
Small dense LDL particles: Visceral fat-driven dyslipidaemia shifts LDL towards smaller, denser particles that penetrate arterial walls more easily
Endothelial dysfunction: Chronic inflammation suppresses nitric oxide production, impairing the ability of blood vessels to relax and dilate
Prothrombotic state: Elevated PAI-1 (plasminogen activator inhibitor-1) from visceral fat impairs the breakdown of blood clots, increasing thrombosis risk
A comprehensive 2025 review in Obesity by Luo and colleagues examined the full spectrum of visceral and ectopic fat features, confirming that visceral adiposity drives cardiometabolic risk through inflammatory, hormonal, and lipotoxic pathways that extend well beyond simple caloric excess (Luo et al., 2025).
What About Ethnicity and Sex?
Cardiovascular risk from visceral fat is not uniform across all populations. South Asians, for example, accumulate significantly more visceral fat at lower BMI values than European populations — meaning standard BMI thresholds may dramatically underestimate metabolic risk in South Asian individuals. This has major implications for clinical practice in South Asia, Southeast Asia, and among diaspora communities globally.
In women, menopause triggers a significant redistribution of fat from subcutaneous depots (hips, thighs) towards visceral depots — partly explaining the spike in cardiovascular risk after menopause despite sometimes modest weight gain.
A 2026 analysis in Nature Reviews Endocrinology by Lin and Tandar reviewed global patterns of visceral adiposity, confirming that ethnicity-specific thresholds for waist circumference and VAT measurement are essential for accurate cardiovascular risk stratification across diverse populations (Lin & Tandar, 2026).
Visceral Fat's Reach: Organ by Organ
Visceral fat doesn't just affect the liver and heart. Its inflammatory and hormonal signals reach virtually every major organ:
Skeletal muscle: Visceral fat-driven insulin resistance reduces glucose uptake in muscles, accelerating progression toward Type 2 diabetes.
Pancreas: Ectopic fat deposits in and around the pancreas impair beta-cell function, reducing insulin secretion capacity over time.
Brain: Inflammatory signals crossing the blood-brain barrier trigger hypothalamic inflammation, disrupting appetite regulation and leptin signalling — contributing to a vicious cycle of further weight gain.
Kidneys: Growing evidence links visceral adiposity with chronic kidney disease and albuminuria, partly mediated through hypertension and inflammation.
A 2024 commentary in the Journal of Clinical Endocrinology & Metabolism by Kubota and Yabe highlighted the concept of visceral adipose tissue "quality" — not just quantity — as a determinant of metabolic health. Their analysis suggested that even modest amounts of metabolically dysfunctional visceral fat can drive significant metabolic harm, particularly in individuals who appear lean by traditional measures (Kubota & Yabe, 2024).
Measuring What Matters: Imaging vs. Anthropometric Tools
The Gold Standard: CT and MRI
Computed Tomography (CT) can precisely quantify visceral fat area at the L4-L5 vertebral level. A visceral fat area greater than 100 cm² is widely used as a clinical threshold for elevated metabolic risk, though ethnicity-specific cutoffs differ. MRI provides comparable accuracy without radiation exposure and is the preferred research standard.
A 2026 study by Liu and colleagues in Abdominal Radiology demonstrated that the visceral-to-subcutaneous fat area ratio derived from AI-automated CT analysis significantly improved long-term mortality prediction compared to either measure alone — suggesting that the ratio of fat compartments may be more informative than absolute volumes (Liu et al., 2026).
Similarly, a 2025 paper in The American Journal of Clinical Nutrition by Tinsley examined the comparative utility of visceral adipose tissue measurements versus waist-based anthropometry in assessing metabolic risk, confirming that while CT-based VAT measurement offers superior precision, anthropometric proxies remain clinically useful and highly accessible in routine practice (Tinsley, 2025).
Practical Tools for Everyday Clinical Use
You don't need a CT scanner to assess visceral fat risk. These tools are validated, accessible, and underused:
Waist circumference is arguably the most important vital sign in metabolic medicine that most healthcare providers still don't routinely measure. Cutoffs vary by ethnicity:
Men: >94 cm (European), >90 cm (South/Southeast Asian)
Women: >80 cm (European), >80 cm (South/Southeast Asian)
Waist-to-hip ratio (WHR): Values above 0.90 in men and 0.85 in women indicate central adiposity and elevated cardiovascular risk.
Waist-to-height ratio: A ratio above 0.5 — regardless of ethnicity or sex — is a simple, powerful predictor of cardiometabolic risk. A useful way to remember it: "keep your waist to less than half your height."
DEXA scanning can quantify regional fat distribution (including android vs gynoid fat mass) without CT-level radiation, making it a practical tool for body composition monitoring in clinical settings.
The Limitations of BMI
BMI measures weight relative to height — nothing more. It cannot distinguish fat from muscle, subcutaneous from visceral fat, or metabolically healthy from unhealthy fat distribution. This is why the "TOFI" phenotype (Thin Outside, Fat Inside) exists: individuals with a normal BMI but significant visceral fat accumulation who carry hidden cardiometabolic risk. Conversely, some individuals with elevated BMI have predominantly subcutaneous fat and remain metabolically healthy. BMI alone is an inadequate risk assessment tool.
Reducing Visceral Fat: What Actually Works
The good news is that visceral fat is metabolically active — which makes it responsive to intervention. Even modest reductions have outsized clinical benefits.
Exercise: The Most Potent VAT Reducer
Zone 2 cardio (comfortable aerobic pace, ~60–70% max heart rate): Builds mitochondrial capacity and enhances fat oxidation over time
Resistance training: Preserves and builds lean muscle mass while reducing visceral fat, improving insulin sensitivity beyond what cardio alone achieves
HIIT (High-Intensity Interval Training): Evidence suggests HIIT produces disproportionate reductions in visceral fat relative to total exercise volume — particularly effective for time-constrained individuals
A combination approach yields the best outcomes
Nutritional Strategies
Caloric deficit with high protein intake: Preserves muscle during weight loss while promoting fat mobilisation
Mediterranean dietary pattern: Consistently associated with reduced visceral fat, lower triglycerides, and improved cardiovascular outcomes
Low-carbohydrate diets: Show preferential reductions in visceral fat, particularly hepatic fat, in the short term
Time-restricted eating / intermittent fasting: Emerging evidence supports reductions in VAT through metabolic rhythm and caloric restriction mechanisms
Pharmacological Approaches
GLP-1 receptor agonists (e.g., semaglutide, liraglutide): Produce significant visceral fat reductions alongside total weight loss, with documented cardiovascular benefits in high-risk populations
SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin): Reduce visceral and ectopic fat, improve insulin sensitivity, and offer cardioprotective and nephroprotective benefits
Emerging therapies targeting adipose tissue inflammation and adipokine pathways are under active investigation
Key insight from the evidence: Even a 5–10% reduction in total body weight produces disproportionately large reductions in visceral fat — often 30–40% — due to its high metabolic activity and preferential mobilisation during energy deficit.
What This Means for You
Rethinking Obesity: The clinical paradigm is shifting from total body weight to fat distribution. BMI alone fails to capture cardiometabolic risk, particularly in populations with high visceral adiposity at lower body weights.
Visceral Fat as an Endocrine Organ: Visceral adipose tissue is biologically active, secreting pro-inflammatory cytokines (TNF-α, IL-6) and reducing protective adipokines like adiponectin. This creates a state of chronic low-grade inflammation central to metabolic disease.
Portal Theory and Hepatic Impact: Through direct drainage into the portal circulation, visceral fat delivers free fatty acids to the liver, driving hepatic insulin resistance, increased gluconeogenesis, and dyslipidaemia—core features of metabolic syndrome.
Beyond Diabetes—A Multisystem Threat: Visceral fat contributes to NAFLD, atherosclerosis, hypertension, and even cognitive dysfunction, reinforcing its role as a systemic disease driver rather than a localized fat depot.
Cardiovascular Risk Amplifier: Elevated visceral fat is strongly associated with small dense LDL particles, endothelial dysfunction, and a prothrombotic state, significantly increasing the risk of myocardial infarction and stroke—independent of BMI.
The Hidden High-Risk Phenotype: The “thin outside, fat inside” (TOFI) phenotype highlights the limitations of visual assessment. Normal-weight individuals may harbor significant visceral fat and remain undiagnosed without targeted screening.
Measurement Must Evolve: Waist circumference and waist-to-height ratio (>0.5) should be routine clinical tools. Imaging (CT/MRI) refines risk assessment but is not essential for initial screening.
Therapeutic Priority: Visceral fat is highly responsive to intervention. Resistance training, aerobic exercise (Zone 2), caloric control, and high-protein diets produce disproportionate reductions in VAT compared to subcutaneous fat.
Pharmacological Advances: Agents such as GLP-1 receptor agonists and SGLT2 inhibitors extend benefits beyond glycemic control, significantly reducing visceral and ectopic fat.
Clinical Imperative: The future of cardiometabolic care lies in targeting visceral adiposity, insulin resistance, and muscle health simultaneously—shifting from weight-centric to metabolism-centric medicine.
Summary Comparison: Visceral vs. Subcutaneous Fat
Here is the comparison between visceral and subcutaneous fat rewritten in a clear, point-by-point format for better readability.
1. Location and Physical Characteristics
Visceral Fat: Located deep within the abdominal cavity, nestled around vital organs like the liver, intestines, and pancreas. It is "hidden" fat and cannot be pinched.
Subcutaneous Fat: Situated just beneath the skin. This is the "pinchable" fat found on the arms, legs, and outer abdomen.
2. Metabolic Activity
Visceral Fat: Highly metabolically active. It behaves like an endocrine organ, constantly pumping out signals and chemicals into the body.
Subcutaneous Fat: Moderately active. It serves primarily as a passive energy storage depot and a thermal insulator.
3. Insulin Sensitivity and Blood Sugar
Visceral Fat: Characterized by low insulin sensitivity (high insulin resistance). It actively disrupts the body’s ability to manage blood sugar.
Subcutaneous Fat: Displays high insulin sensitivity. It generally responds well to insulin and helps buffer excess energy safely.
Shutterstock
4. Hormonal and Inflammatory Profile
Visceral Fat: Secretes high levels of pro-inflammatory cytokines (such as TNF-$\alpha$ and IL-6) and produces very low amounts of adiponectin (a protective hormone).
Subcutaneous Fat: Produces lower levels of inflammatory markers and secretes high amounts of adiponectin, which helps improve metabolism and reduce inflammation.
5. Fatty Acid Release and the Liver
Visceral Fat: High rate of free fatty acid release. Because of its location, these fats drain directly into the portal vein, hitting the liver with high concentrations of fat.
Subcutaneous Fat: Low rate of fatty acid release. When it does release fat, it goes into general circulation rather than directly to the liver.
6. Disease Risk and Protection
Visceral Fat: Highly associated with increased cardiovascular risk, Type 2 diabetes, and fatty liver disease.
Subcutaneous Fat: Generally considered neutral or even protective. Fat stored in the hips and thighs (subcutaneous) is associated with better metabolic health.
7. Response to Lifestyle Changes
Visceral Fat: Responds rapidly to exercise and dietary changes. Because it is so metabolically active, it is often the first fat the body "burns" during a caloric deficit.
Subcutaneous Fat: Responds moderately or slowly. It is often more stubborn and takes longer to mobilize compared to the deep internal fat.
Frequently Asked Questions
1. Can I have normal weight but dangerous levels of visceral fat? Yes — this is called the "TOFI" phenotype (Thin Outside, Fat Inside). People with a normal BMI can carry significant visceral fat, particularly if they are sedentary, consume a high-sugar or high-refined-carbohydrate diet, or have a genetic predisposition to central fat storage. Waist circumference and fasting metabolic markers are essential to detect this hidden risk.
2. How does visceral fat cause diabetes? Visceral fat drains free fatty acids and inflammatory molecules directly into the portal vein, reaching the liver in high concentrations. This impairs the liver's response to insulin and triggers excessive glucose production. Over time, the pancreas is forced to compensate by secreting more insulin until beta-cell capacity fails — resulting in Type 2 diabetes. This process is described by the portal hypothesis.
3. Is it possible to reduce visceral fat without losing overall weight? Yes, to a meaningful extent. Exercise — particularly resistance training and aerobic activity — can reduce visceral fat even without significant changes in total body weight, by improving metabolic efficiency, reducing inflammation, and shifting body composition from fat to lean mass.
4. Why is visceral fat more dangerous for South Asians? South Asian individuals accumulate more visceral fat relative to total body fat at lower BMI values compared to European populations. This means standard BMI-based risk thresholds underestimate cardiometabolic risk in South Asians. Lower waist circumference cutoffs (≥90 cm in men, ≥80 cm in women) are recommended for South Asian populations.
5. What blood tests can indicate high visceral fat? No single test directly measures visceral fat, but a cluster of markers suggests its presence: elevated fasting insulin, high HOMA-IR (insulin resistance index), elevated triglycerides, low HDL cholesterol, raised ALT/AST (liver enzymes), and elevated hs-CRP (inflammation marker). A high triglyceride/HDL ratio is one of the most accessible and informative surrogate markers.
6. How quickly does visceral fat respond to diet and exercise? Visceral fat is highly responsive to lifestyle change — often more so than subcutaneous fat. Studies show that 8–12 weeks of consistent exercise with modest caloric restriction can produce measurable VAT reductions on imaging. Even a 5–10% reduction in body weight can reduce visceral fat by up to 30–40%.
7. Do medications like semaglutide specifically target visceral fat? GLP-1 receptor agonists like semaglutide do not specifically "target" visceral fat, but clinical trials show they produce proportionally greater reductions in visceral and hepatic fat compared to subcutaneous fat. This partly explains their cardiovascular and metabolic benefits beyond simple weight reduction.
Take Action: Your Next Steps
Understanding visceral fat is the first step. The next is taking meaningful action — and you don't need to wait until a problem develops.
Your Immediate Action Checklist
✅ Measure your waist circumference today — at the level of your navel, relaxed, not sucked in
✅ Calculate your waist-to-height ratio (waist ÷ height should be below 0.5)
✅ Request a metabolic panel from your doctor: fasting insulin, HOMA-IR, lipid profile, liver enzymes, hs-CRP
✅ Start moving daily — even 30 minutes of brisk walking consistently reduces visceral fat over time
✅ Reduce ultra-processed foods and added sugars — the primary dietary drivers of visceral fat accumulation
Have a question? Drop it in the comments below — I respond to every question personally.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Beyond BMI: Why Waist-to-Height Ratio (WHtR) is the New Clinical Gold Standard
What Causes Visceral Fat? Hormones, Lifestyle, and Metabolic Risk Explained | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
Breakthrough Research: Leptin Reduction is Required for Sustained Weight Loss | DR T S DIDWAL
References
Chagas, C. L., da Silva, N. F., Rodrigues, I. G., Arcoverde, G. M. P. F., Ferraz, V. D., Sobral Filho, D. C., Diniz, A. D. S., Pinho, C. P. S., Cabral, P. C., & de Arruda, I. K. G. (2025). Different factors modulate visceral and subcutaneous fat accumulation in adults: A single-center study in Brazil. Frontiers in Nutrition, 12, 1524389. https://doi.org/10.3389/fnut.2025.1524389
Després, J.-P. (2012). Body fat distribution and risk of cardiovascular disease: An update. Circulation, 126(10), 1301–1313. https://doi.org/10.1161/CIRCULATIONAHA.111.067264
Emamat, H., Jamshidi, A., Farhadi, A., Ghalandari, H., Ghasemi, M., & Tangestani, H. (2024). The association between the visceral-to-subcutaneous abdominal fat ratio and the risk of cardiovascular diseases: A systematic review. BMC Public Health, 24(1), 1827. https://doi.org/10.1186/s12889-024-19358-0
Fox, C. S., Massaro, J. M., Hoffmann, U., Pou, K. M., Maurovich-Horvat, P., Liu, C.-Y., Vasan, R. S., Murabito, J. M., Meigs, J. B., Cupples, L. A., D’Agostino, R. B., & O’Donnell, C. J. (2007). Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation, 116(1), 39–48. https://doi.org/10.1161/CIRCULATIONAHA.106.675355
Kubota, S., & Yabe, D. (2024). Visceral adipose tissue quality and its impact on metabolic health. The Journal of Clinical Endocrinology & Metabolism, 109(8), e1665–e1666. https://doi.org/10.1210/clinem/dgae021
Lee, M.-J., & Kim, J. (2024). The pathophysiology of visceral adipose tissues in cardiometabolic diseases. Biochemical Pharmacology, 222, 116116. https://doi.org/10.1016/j.bcp.2024.116116
Lin, J. C., & Tandar, C. E. (2026). Global patterns of visceral adiposity and cardiometabolic disease. Nature Reviews Endocrinology, 22, 8. https://doi.org/10.1038/s41574-025-01191-z
Liu, D., Kuchnia, A., Blake, G., et al. (2026). Ratio of visceral-to-subcutaneous fat area improves long-term mortality prediction over either measure alone: Automated CT-based AI measures with longitudinal follow-up in a large adult cohort. Abdominal Radiology, 51, 1618–1627. https://doi.org/10.1007/s00261-025-05149-7
Luo, J., Wang, Y., Mao, J., et al. (2025). Features, functions, and associated diseases of visceral and ectopic fat: A comprehensive review. Obesity, 33(5), 825–838. https://doi.org/10.1002/oby.24239
Shulman, G. I. (2014). Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. Cell Metabolism, 19(6), 929–940. https://doi.org/10.1016/j.cmet.2014.03.014
Tinsley, G. M. (2025). Visceral adipose tissue compared with waist-based anthropometry in assessing metabolic risk. The American Journal of Clinical Nutrition, 122(5), 1145–1146. https://doi.org/10.1016/j.ajcnut.2025.08.011