Beyond BMI: Why Waist-to-Height Ratio (WHtR) Is the New Clinical Gold Standard
Is BMI a lie? Discover why waist circumference and the Waist-to-Height Ratio (WHtR) are superior clinical predictors of diabetes and heart disease.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/9/202617 min read
The Problem: BMI (Body Mass Index) measures your weight, but it cannot see your risk. It fails to distinguish between healthy muscle and life-threatening internal fat.
The Danger: The TOFI phenotype (Thin Outside, Fat Inside) means you can have a "normal" weight while your liver and heart are surrounded by toxic visceral fat.
The Solution: Clinical research now favors the Waist-to-Height Ratio (WHtR). It is a more accurate predictor of diabetes, heart disease, and longevity than the scale.
The Goal: Keep your waist circumference below half your height.
"Your scale tells you how much you weigh; your tape measure tells you how long you’ll live. In my practice, I treat waist circumference as a vital sign—just like blood pressure."
BMI measures quantity of mass. Waist circumference measures distribution of fat. They answer different clinical questions.
Visceral fat is the true disease driver — not total body weight.
WHtR ≥ 0.5 is the most universally applicable, ethnicity-independent risk threshold available today.
TOFI individuals — normal BMI, elevated visceral fat — represent a high-risk, underdiagnosed population that only waist-based measures can detect.
South Asians require lower cut-off thresholds and heightened vigilance.
The optimal clinical protocol uses BMI + waist circumference + WHtR together.
Waist circumference should be treated as a vital sign — measured at every clinical encounter.
Clinical pearls
1. The "Waist-to-Height" Golden Rule
Scientific Perspective: The Waist-to-Height Ratio (WHtR) is a more potent predictor of cardiovascular disease and mortality than BMI because it accounts for both frame size and central adiposity. A ratio of 0.5 indicates that the volume of visceral fat has likely exceeded the body's safe metabolic storage capacity.
Keep your waist circumference to less than half your height. It’s a simple "pass/fail" test that doesn't require a calculator or a doctor's scale to know if your internal organs are under pressure.
2. The South Asian "Metabolic Paradox"
Scientific Perspective: Phenotypic data shows South Asians have a lower "adipose expandability threshold." They accumulate visceral fat and develop insulin resistance at much lower BMIs (e.g., 23 kg/m²) compared to Europid populations. This necessitates the use of stricter, ethnicity-specific cut-offs (Men 90 cm, Women 80 cm).
For South Asians, being "lean" is no guarantee of safety. Because of genetics, your body stores fat "inside" the belly rather than "under" the skin. You must monitor your waistline even if your weight has stayed the same since college.
3. Sarcopenic Obesity: The Invisible Threat
Scientific Perspective: In aging, a "stable" weight often masks a dangerous cross-over: the loss of skeletal muscle (sarcopenia) replaced by an equal weight of visceral fat. This maintains a "normal" BMI while metabolic health plummets due to reduced glucose disposal in the muscle.
The scale can stay exactly the same while your body composition gets worse. If you are losing muscle and gaining a "potbelly," your risk for diabetes is rising, even if your total weight hasn't changed a pound.
4. Visceral Fat as a Gland, Not a Storage Tank
Scientific Perspective: Visceral adipose tissue (VAT) is not inert energy; it is an active endocrine organ. It secretes inflammatory cytokines such as IL-6 and TNF-α directly into the portal vein, which flows directly to the liver, triggering systemic inflammation and fatty liver (NAFLD).
Think of belly fat as a "leaky factory" inside you that pumps out inflammatory chemicals 24/7. This inflammation irritates your arteries and makes it harder for your body to manage blood sugar.
5. Exercise: Quality of Loss Over Quantity of Loss
Scientific Perspective: Aerobic and resistance training can significantly reduce visceral fat and liver fat even if total body weight remains unchanged. This "metabolic remodeling" improves insulin sensitivity and lipid profiles regardless of the number on the scale.
Don't get discouraged if the scale doesn't move after a month of exercise. Your body is likely burning the "dangerous" fat around your organs first. A looser belt is a much better sign of success than a lower number on the scale.
6. The "TOFI" Warning (Thin Outside, Fat Inside)
Scientific Perspective: The TOFI phenotype represents individuals with a healthy BMI but high ectopic fat (fat in the liver, pancreas, and muscle). These individuals often have "Normal" fasting glucose but elevated Triglyceride-to-HDL ratios, signaling early-stage metabolic dysfunction.
You can be "skinny" and still be pre-diabetic. If you have a slim frame but a protruding belly, you need the same blood work and lifestyle focus as someone who is clinically obese. Your health is determined by what’s under the hood, not just the paint job.
Waist Circumference vs BMI: Which Predicts Disease Better? A Metabolic Risk Perspective
You step on the scale. The number looks fine. Your Body Mass Index (BMI) falls neatly within the “normal” range. On paper, everything suggests you are metabolically healthy.
But beneath that reassuring number, a very different story may be unfolding.
Across the world, millions of individuals with a “healthy BMI” are silently developing insulin resistance, fatty liver disease, and early atherosclerosis—conditions driven not by how much fat they carry, but by where that fat is stored. This is the hidden danger of visceral fat, the metabolically active fat that accumulates deep within the abdomen, surrounding vital organs and driving chronic inflammation.
This disconnect between appearance and metabolic health has led to the recognition of the TOFI (Thin Outside, Fat Inside) phenotype, where individuals appear lean but carry disproportionately high levels of internal fat and cardiometabolic risk (Salmón-Gómez et al., 2023). At the same time, others classified as “overweight” by BMI may have relatively low visceral fat and remain metabolically healthy—highlighting the fundamental limitation of BMI as a standalone tool.
Emerging evidence consistently shows that waist circumference and waist-to-height ratio (WHtR) outperform BMI in predicting type 2 diabetes, cardiovascular disease, and even all-cause mortality (Ross et al., 2020; Suwała & Junik, 2024). Unlike BMI, these measures directly capture central obesity, the key driver of metabolic dysfunction through mechanisms such as lipotoxicity, adipose tissue inflammation, and hepatic insulin resistance.
Even more importantly, recent longitudinal data suggest that changes in waist circumference over time are stronger predictors of prediabetes than changes in BMI, reinforcing the concept that central fat accumulation is an early and dynamic marker of disease risk (Nuamah et al., 2026).
The message is clear: the scale measures weight, but your waist measures risk.
What Is BMI — And Why Did We Rely on It for So Long?
Body Mass Index was developed by Belgian mathematician Adolphe Quetelet in the 19th century as a population-level statistical tool — never as a clinical diagnostic instrument. Yet for over a century, medicine adopted it as the standard gateway measurement for obesity and metabolic risk.
The formula is simple:
BMI = Weight (kg) ÷ Height (m²)
BMI Range Classification < 18.5 Underweight 18.5 – 24.9 Normal weight 25.0 – 29.9 Overweight ≥ 30 Obese
(WHO classification)
Its appeal is obvious. It is fast, free, requires no equipment, and works at a population scale. Large epidemiological studies have used BMI to establish clear links between excess weight and conditions ranging from type 2 diabetes to certain cancers.
But here is the critical problem: BMI cannot distinguish between fat and muscle, and it cannot tell you where fat is stored in your body.
A professional athlete carrying 90 kg of muscle and a sedentary office worker carrying 90 kg of mixed fat and lean mass will have the same BMI, despite having vastly different metabolic risk profiles. Similarly, a person with a "normal" BMI of 23 but significant fat stored around their abdominal organs could be walking into a metabolic crisis while their chart looks clean.
A landmark analysis published in Nature Communications phenotyped large population-based cohorts by BMI category and found that metabolic risk varied enormously within each BMI tier — demonstrating that BMI alone fails to characterise cardiometabolic risk with sufficient precision (Beyene et al., 2023). A separate cross-sectional study published in the Journal of Clinical Medicine confirmed that BMI significantly underperformed waist circumference in predicting above-average cardiovascular risk when assessed using validated SCORE2 calculators — and proposed new optimal cut-off values to address this gap (Suwała & Junik, 2024).
The evidence is unambiguous: BMI is a useful screening tool at the population level, but a poor clinical predictor of individual metabolic disease.
Waist Circumference: Measuring What Actually Matters
Waist circumference is not simply a measure of how round your belly looks. It is a validated clinical surrogate for visceral adiposity — the fat that accumulates inside your abdominal cavity, wrapping around your liver, pancreas, intestines, and kidneys.
This distinction matters enormously because visceral fat is biologically active in ways that subcutaneous fat (the fat directly under your skin) is not. Visceral fat secretes pro-inflammatory molecules including tumour necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), drives hepatic insulin resistance through portal free fatty acid flux, and directly fuels the chronic low-grade inflammation underlying atherosclerosis, type 2 diabetes, and non-alcoholic fatty liver disease.
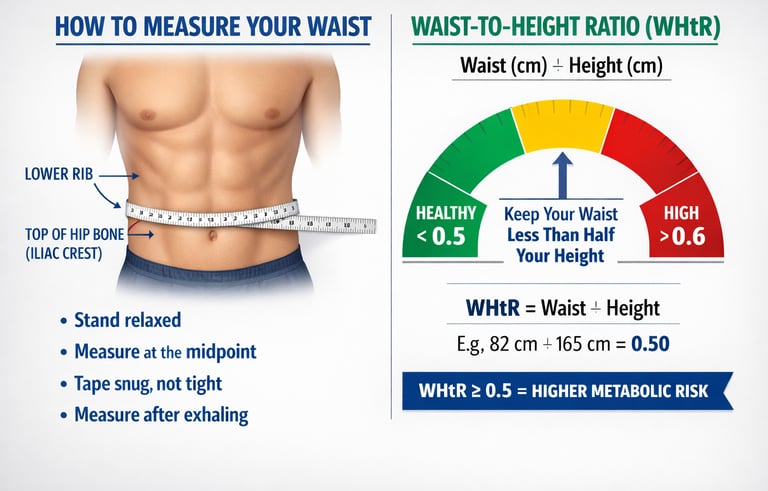
How to Measure Waist Circumference Correctly
Accurate measurement requires standardisation:
Stand upright and relax your abdomen naturally (do not suck in)
Place the tape measure at the midpoint between the lower rib margin and the iliac crest (the top of the hip bone)
Measure at the end of a gentle exhale
The tape should be snug but not compressing the skin
Clinical Cut-Off Values
For Europid (Caucasian) populations:
Men: ≥ 102 cm = increased metabolic risk
Women: ≥ 88 cm = increased metabolic risk
For South Asian populations (critically important):
Men: ≥ 90 cm = increased metabolic risk
Women: ≥ 80 cm = increased metabolic risk
South Asians develop visceral fat accumulation and its metabolic consequences at significantly lower absolute waist measurements — a biological reality that standard Europid cut-offs consistently miss, leading to widespread underdiagnosis of metabolic disease in this population.
A landmark Consensus Statement from the International Atherosclerosis Society (IAS) and the International Chair on Cardiometabolic Risk (ICCR) Working Group formally recommended that waist circumference be treated as a vital sign in clinical practice, analogous to blood pressure — measured routinely at every clinical encounter (Ross et al., 2020). This was not a minor academic suggestion. It was an international expert consensus calling for a fundamental shift in how we screen for metabolic disease.
The Waist-to-Height Ratio (WHtR): A Universal Risk Predictor
Waist circumference alone has one limitation: it doesn't account for height. A waist of 85 cm may carry different risk implications for a person who is 155 cm tall versus one who is 190 cm tall.
The Waist-to-Height Ratio (WHtR) corrects this by expressing waist circumference as a proportion of height:
WHtR = Waist Circumference (cm) ÷ Height (cm)
The critical threshold is elegantly simple:
WHtR ≥ 0.5 = increased cardiometabolic risk
Or, in patient-friendly language: keep your waist to less than half your height.
A comprehensive analysis published in BMC Public Health evaluated WHtR alongside waist-to-BMI ratio, a body shape index, and other anthropometric parameters using data from the NHANES III cohort, finding that WHtR demonstrated strong predictive capacity for cardiovascular disease mortality — and outperformed BMI across multiple subgroup analyses (Lee et al., 2025). Its advantages include applicability across ethnic groups, sexes, and age categories, making it arguably the most universally deployable single-number risk metric currently available.
This conclusion received powerful further support from a large-scale cohort study with independent replication published in medRxiv in 2025. Ho and colleagues directly pitted waist circumference and WHtR against BMI across risks for multiple diseases simultaneously, finding that waist-based measures consistently demonstrated superior predictive performance across a range of cardiometabolic outcomes — strengthening the evidence base for moving beyond BMI as a primary screening tool in clinical practice (Ho et al., 2025).
The TOFI Phenotype: Thin Outside, Fat Inside
Perhaps the most medically dangerous consequence of over-relying on BMI is the systematic failure to identify what researchers call the TOFI phenotype: Thin Outside, Fat Inside.
TOFI individuals have a normal or even lean BMI. They do not appear overweight. Standard clinical screening based on weight alone will completely miss them. Yet inside their bodies, visceral fat has accumulated around their abdominal organs, fat has infiltrated their liver, their pancreatic beta cells are under stress, and their skeletal muscle is laced with lipid deposits.
Why Does TOFI Develop?
The leading explanation is the impaired adipose expandability hypothesis. In healthy metabolic responders, subcutaneous fat tissue can expand to safely store excess dietary energy. In TOFI-susceptible individuals, this capacity is limited. When subcutaneous storage is exhausted, fat overflows into ectopic depots — the liver, pancreas, pericardium, and skeletal muscle — where it causes direct organ toxicity.
Metabolic Features of TOFI
Insulin resistance despite normal weight
Elevated triglycerides and low HDL cholesterol
Elevated inflammatory markers (hs-CRP, IL-6)
Non-alcoholic fatty liver disease (NAFLD) without obesity
Hypertension despite lean appearance
A systematic review of body composition phenotyping highlighted that TOFI and metabolically unhealthy lean phenotypes are frequently observed and carry substantial cardiometabolic risk — risk that is invisible to BMI-based screening (Salmón-Gómez et al., 2023).
TOFI is particularly prevalent among South Asians, who demonstrate a genetic and metabolic predisposition to visceral fat accumulation even at low BMI values. A South Asian man with a BMI of 23 and a waist circumference of 92 cm is already in high-risk territory by ethnicity-specific criteria — yet his BMI alone would classify him as perfectly healthy.
The clinical implication is unambiguous: waist circumference and WHtR must be measured in every patient, regardless of their BMI.
Visceral Fat and Disease: The Mechanistic Evidence
Understanding why waist circumference predicts disease better than BMI requires understanding what visceral fat actually does inside your body.
The Lipotoxicity Cascade
Visceral fat cells are metabolically hyperactive. They release free fatty acids directly into the portal circulation, flooding the liver with lipid substrate. The liver responds by producing excess triglycerides, developing insulin resistance, and accumulating intrahepatic fat — the hallmark of NAFLD. Left unchecked, this progresses to non-alcoholic steatohepatitis (NASH), fibrosis, and cirrhosis.
Chronic Inflammation
Visceral adipose tissue is infiltrated by activated macrophages that continuously secrete TNF-α, IL-6, and other pro-inflammatory cytokines. This creates a state of chronic low-grade systemic inflammation — the common molecular substrate of atherosclerosis, type 2 diabetes, hypertension, and several cancers.
Predicting Prediabetes: The Importance of Trajectory
It is not only where fat is stored today that matters — it is how your measurements change over time. A prospective cohort study from the Aichi Workers' Cohort Study followed working-age adults longitudinally and found that increases in waist circumference were stronger predictors of incident prediabetes than changes in BMI, even when both were measured in the same individuals over the same period (Nuamah et al., 2026). This finding carries an important practical message: someone whose BMI remains stable but whose waist circumference is gradually expanding is accumulating visceral fat and moving toward prediabetes — a trajectory that BMI tracking would completely miss. Serial waist measurements are therefore not just diagnostic tools but early warning systems for metabolic deterioration.
Cardiovascular Risk: Beyond Simple Correlation
Recent research has added important nuance to our understanding of how adiposity patterns interact with cardiac risk. A major study published in JACC: Asia demonstrated that the combination of BMI burden and waist circumference burden over time predicts risk of atrial fibrillation — one of the most common cardiac arrhythmias and a leading cause of stroke — with greater precision than either metric alone (Rhee et al., 2024). This underscores a key clinical principle: these measurements are complementary, not competing. The best approach uses both.
Anthropometric Tools: Key Differences
1. Body Mass Index (BMI)
What it measures: Total body mass relative to height
Best strength:
Simple, quick, and widely used
Effective for large-scale population screening
Key limitation:
Cannot distinguish between fat and muscle
Does not reflect fat distribution
Recommended use:
First-line screening tool in clinical and public health settings
2. Waist Circumference
What it measures: Central (visceral) adiposity
Best strength:
Strong predictor of cardiometabolic disease
Reflects visceral fat accumulation
Ethnicity-specific cut-offs improve accuracy
Key limitation:
Measurement technique can vary between observers
Recommended use:
Routine clinical assessment
Should be treated as a vital sign
3. Waist-to-Height Ratio (WHtR)
What it measures: Waist circumference relative to height
Best strength:
Applicable across sex, age, and ethnic groups
Strong predictor of cardiometabolic risk
Easy patient self-monitoring (“keep waist < half height”)
Key limitation:
Not yet widely adopted in routine clinical practice
Recommended use:
Risk stratification
Preventive health screening and patient education
4. Waist-to-Hip Ratio (WHR)
What it measures: Fat distribution pattern (central vs peripheral)
Best strength:
Good predictor of cardiovascular disease risk
Key limitation:
Less practical and less commonly used clinically
Recommended use:
Epidemiological research
Advanced risk assessment settings
Clinical Decision-Making: A Practical Framework
The 3-Step Metabolic Risk Screen
Step 1: Measure BMI
Provides a basic weight-for-height index
Identifies extremes (severe underweight or morbid obesity)
Step 2: Measure waist circumference
Apply ethnicity-specific cut-offs
Flags central obesity in individuals with normal BMI
Step 3: Calculate WHtR
Divide waist circumference by height
A result ≥ 0.5 signals elevated risk regardless of BMI category
Risk Stratification Matrix
BMI Status Waist Status Risk Profile Action Normal Normal Low risk Routine monitoring Normal Elevated High metabolic risk Full metabolic workup Elevated Normal Moderate risk Lifestyle assessment Elevated Elevated Very high risk Urgent intervention
The most clinically dangerous quadrant is Normal BMI + Elevated Waist — the silent TOFI zone where conventional screening fails.
Special Populations: Who Needs Extra Attention?
South Asians
This population carries a disproportionate burden of type 2 diabetes and cardiovascular disease at lower BMI and waist values than Europid populations. Ethnic-specific cut-offs (men ≥90 cm, women ≥80 cm) must be applied without exception. A South Asian patient with a "borderline" waist of 88 cm may already be carrying significant metabolic risk.
Older Adults and Sarcopenic Obesity
As we age, muscle mass declines and fat redistributes centrally even without weight gain — a condition called sarcopenic obesity. An elderly patient may have a normal or even low BMI driven by muscle loss, while simultaneously carrying dangerous quantities of visceral fat. BMI completely misses this. Waist circumference and WHtR remain informative even as body composition shifts with age.
A 2026 study published in Geriatrics specifically examined this population and found that the Cardiometabolic Index — a composite metric incorporating waist circumference — outperformed BMI alone in predicting cardiometabolic multimorbidity risk in older adults (Kunutsor & Laukkanen, 2026). Critically, waist circumference remained an independent predictor of multi-system metabolic disease in this age group even after adjustment for BMI, reinforcing that central adiposity assessments must not be abandoned in older patients simply because their weight appears acceptable. For elderly individuals, routine waist measurement may be among the most actionable and cost-effective tools available in preventive geriatric medicine.
Athletes and Muscular Individuals
High BMI in athletes typically reflects lean muscle mass rather than fat. However, even athletes can develop relative central adiposity if dietary habits shift or training volume decreases. Waist circumference and WHtR protect against misclassification in both directions — correctly identifying low-risk muscular individuals and flagging any emerging central fat accumulation.
Practical Applications: What You Can Do Today
For Patients — Your 5-Minute Home Assessment:
Measure your waist at the midpoint between your lower rib and hip bone, at the end of a natural exhale
Measure your height
Divide waist by height to get your WHtR
If your result is ≥ 0.5, discuss this with your doctor regardless of what your BMI says
Track changes every 3 months — trends matter as much as absolute values
For Clinicians — Integrating Into Practice:
Add waist circumference as a mandatory vital sign alongside blood pressure and heart rate
Apply ethnicity-specific cut-offs as standard (not optional) protocol
Calculate and document WHtR in all metabolic, cardiac, and diabetes clinic encounters
Flag Normal BMI + Elevated Waist patients for full metabolic panels (fasting glucose, HbA1c, lipids, liver enzymes)
Use WHtR ≥ 0.5 as an entry point for lifestyle intervention conversations
Common Myths — Corrected
Myth 1: "My BMI is normal, so I'm metabolically healthy." False. As the TOFI phenotype clearly demonstrates, normal BMI does not exclude insulin resistance, fatty liver, or cardiovascular risk. Waist circumference must be measured independently.
Myth 2: "Only overweight or obese people develop metabolic disease." False. Lean individuals with excess visceral fat carry substantial disease risk. Weight is not the determining factor — fat distribution is.
Myth 3: "If I lose weight, my metabolic risk disappears." Incomplete. Weight loss helps, but the pattern of fat loss matters. Visceral fat reduction — not total weight loss — drives metabolic improvement. Exercise, particularly aerobic activity, disproportionately reduces visceral fat even before significant weight changes occur.
Myth 4: "Waist measurements are inaccurate and subjective." Standardised technique significantly reduces variability. Following validated protocol (correct landmark, end-expiratory timing, appropriate tape tension) yields reproducible results comparable in reliability to blood pressure measurement.
Frequently Asked Questions
Q1: Is waist circumference always better than BMI for predicting disease? For predicting metabolic conditions like type 2 diabetes, cardiovascular disease, and fatty liver, waist circumference and WHtR consistently outperform BMI. However, BMI retains value at population level and for detecting extremes of underweight or severe obesity. The best clinical approach combines both metrics.
Q2: What is the ideal waist circumference for a healthy adult? For Caucasian/Europid adults: below 94 cm for men and below 80 cm for women represents low risk. For South Asian adults: below 90 cm for men and below 80 cm for women. However, WHtR below 0.5 is the most universally applicable target across all ethnic groups.
Q3: Can I be obese by BMI but metabolically healthy? Yes. This is called the Metabolically Healthy Obese (MHO) phenotype. Some individuals with high BMI have normal waist circumference, normal insulin sensitivity, normal blood pressure, and normal lipid profiles. However, long-term evidence suggests MHO is often a transitional state that can progress to metabolic disease over time, so monitoring remains important.
Q4: How often should I measure my waist circumference? Every 3 months if you are actively working on weight management or metabolic health. Annually as part of routine preventive health check-ups. After any significant dietary, lifestyle, or medication change that might affect body composition.
Q5: Does visceral fat reduction require weight loss? Not necessarily. Structured aerobic exercise — particularly 150+ minutes per week of moderate-intensity activity — significantly reduces visceral fat even in the absence of meaningful scale weight change. Dietary approaches (particularly reducing refined carbohydrates and ultra-processed foods) also reduce visceral fat independently of total caloric restriction.
Q6: Is WHtR the same for men and women? Yes — the universal cut-off of 0.5 applies across sexes, which is one of WHtR's major clinical advantages over waist circumference alone (which uses different thresholds for men and women).
Q7: Should children have their waist circumference measured? Yes. Childhood central obesity is a significant predictor of adult metabolic disease. Age- and sex-specific percentile charts exist for waist circumference in children, and WHtR ≥ 0.5 has been validated as a risk threshold in paediatric populations as well.
Call to Action: Know Your Real Risk Number
Your BMI is not your metabolic destiny. The number that truly matters is the one measured at your waist.
Here is what I want you to do right now:
✅ Grab a measuring tape and measure your waist using the technique described above
✅ Divide that number by your height to calculate your WHtR
✅ If your WHtR is ≥ 0.5, book an appointment with your doctor and specifically request a full metabolic panel — not just a standard weight check
✅ Share this article with someone you care about who may be getting false reassurance from a "normal" BMI
Author’s Note: A Clinician’s Perspective
As a practicing physician with over four decades of clinical experience, I have watched the "BMI Era" dominate medicine with a mix of utility and frustration. For years, we used Body Mass Index because it was easy—a quick calculation that allowed us to categorize patients in seconds. But in my clinic, I have seen the devastating gaps this metric leaves behind.
I have seen "normal weight" patients—individuals who look fit and healthy on the outside—present with the advanced metabolic markers of a 300-pound man: fatty liver, insulin resistance, and systemic inflammation. Conversely, I have seen "overweight" patients with incredible muscle mass and perfect blood work who were being unfairly stigmatized by a mathematical formula from the 1800s.
My clinical stance is this: Weight is a poor surrogate for health. Location is everything.
We are currently in a transition toward a more nuanced, "geroscience-informed" approach to longevity. We now understand that the fat living deep within your abdominal cavity—visceral fat—is not just stored energy; it is a toxic, inflammatory organ that directly poisons the liver and stresses the heart.
Why I advocate for the Waist-to-Height Ratio (WHtR):
It is the "Great Equalizer": It works for the 6'4" athlete and the 5'2" grandmother alike. It respects the biological reality that your frame size dictates how much central mass you can safely carry.
It catches the "TOFI" (Thin Outside, Fat Inside): By making waist circumference a "vital sign," we stop missing the millions of people who are metabolically "obese" despite being technically "lean."
It empowers the patient: You do not need a laboratory or a complex machine to track your metabolic destiny. A simple piece of string and a tape measure are more predictive of your lifespan than the most expensive digital scale.
In my own life and in my practice, I prioritise strength over mass and waistline over weight. As we age, our goal should not be to simply be "thin," but to be metabolically resilient. This starts by looking past the scale and measuring what actually drives disease.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
BMI vs Body Fat: Which Better Predicts Hidden Cardiometabolic Risk?
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Beyene, H. B., Giles, C., Huynh, K., et al. (2023). Metabolic phenotyping of BMI to characterize cardiometabolic risk: evidence from large population-based cohorts. Nature Communications, 14, 6280. https://doi.org/10.1038/s41467-023-41963-7
Ho, F., Pentti, J., Kivimäki, M., & Sattar, N. (2025). Waist, waist-height-ratio vs body mass index and the risks of multiple diseases: a cohort study with replication. medRxiv, 2025.10.16.25338152. https://doi.org/10.1101/2025.10.16.25338152
Kunutsor, S. K., & Laukkanen, J. A. (2026). Cardiometabolic Index, BMI, Waist Circumference, and Cardiometabolic Multimorbidity Risk in Older Adults. Geriatrics, 11(1), 4. https://doi.org/10.3390/geriatrics11010004
Lee, T. L., Lin, F. J., Yeh, C. F., et al. (2025). Evaluating the potential of waist-to-BMI ratio, a body shape index, and other anthropometric parameters in predicting cardiovascular disease mortality: evidence from NHANES III. BMC Public Health, 25, 1828. https://doi.org/10.1186/s12889-025-22944-5
Nuamah, H. G., Song, Z., Takada, M., et al. (2026). Changes in body mass index and waist circumference as predictors of incident prediabetes: the Aichi Workers' Cohort Study. Scientific Reports, 16, 10538. https://doi.org/10.1038/s41598-026-45909-z
Rhee, T.-M., Han, K.-D., Choi, E.-K., Kim, B.-S., Lee, K.-Y., Choi, J., Ahn, H.-J., Kwon, S., Lee, S.-R., Oh, S., & Lip, G. Y. H. (2025). Combination of body mass index and waist circumference burden determines the risk of atrial fibrillation. JACC: Asia, 5(1), 129–139. https://doi.org/10.1016/j.jacasi.2024.08.021
Ross, R., Neeland, I. J., Yamashita, S., Shai, I., Seidell, J., Magni, P., Santos, R. D., Arsenault, B., Cuevas, A., Hu, F. B., Griffin, B. A., Zambon, A., Barter, P., Fruchart, J. C., Eckel, R. H., Matsuzawa, Y., & Després, J. P. (2020). Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nature Reviews Endocrinology, 16(3), 177–189. https://doi.org/10.1038/s41574-019-0310-7
Salmón-Gómez, L., Catalán, V., Frühbeck, G., et al. (2023). Relevance of body composition in phenotyping the obesities. Reviews in Endocrine and Metabolic Disorders, 24, 809–823. https://doi.org/10.1007/s11154-023-09796-3
Suwała, S., & Junik, R. (2024). Body Mass Index and Waist Circumference as Predictors of Above-Average Increased Cardiovascular Risk Assessed by the SCORE2 and SCORE2-OP Calculators and the Proposition of New Optimal Cut-Off Values: Cross-Sectional Single-Center Study. Journal of Clinical Medicine, 13(7), 1931. https://doi.org/10.3390/jcm13071931