The #1 Diet Strategy to Reduce Visceral Fat (According to Latest Research)
Discover the best diet for visceral fat loss. Compare low-carb vs Mediterranean diets, learn what to eat, and use proven strategies to reduce dangerous belly fat fast.
OBESITYNUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/4/202613 min read
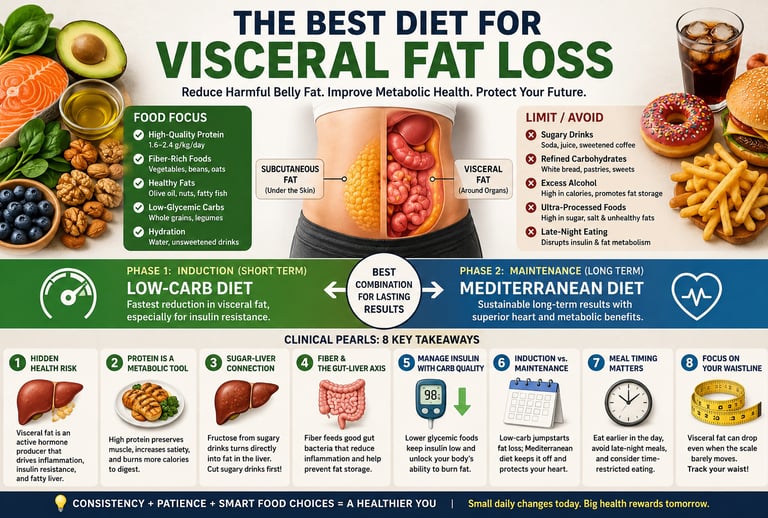
The best diet for visceral fat loss emphasizes high protein, fiber-rich whole foods, healthy fats, and fewer refined carbohydrates and sugary drinks. Research suggests low-carbohydrate diets produce the fastest short-term visceral fat loss, while the Mediterranean diet offers the best long-term heart health and sustainability. Combining both approaches often delivers the best results.
Key Takeaways
Not all belly fat is the same.
The most harmful fat is visceral fat, which surrounds your internal organs. It increases your risk of type 2 diabetes, heart disease, and fatty liver, even if you don't look overweight.Protein should be part of every meal.
Eating enough protein helps you stay full, protects your muscles as you lose weight, and makes it easier for your body to burn fat.Cut back on sugary drinks first.
Soft drinks, fruit juices, and sweetened beverages are one of the biggest contributors to harmful belly fat. Replacing them with water or unsweetened drinks can make a big difference.Choose better carbohydrates, not just fewer carbohydrates.
Swap white bread, white rice, and sugary snacks for whole grains, beans, vegetables, and fruits. These foods help keep blood sugar and insulin levels healthier.Healthy fats are good for you.
Foods like olive oil, nuts, seeds, avocados, and oily fish support heart health and may help reduce harmful abdominal fat when eaten in moderation.A low-carb diet can help you lose belly fat faster, but the Mediterranean diet is easier to maintain.
Many people benefit from starting with a lower-carb approach and then switching to a Mediterranean-style eating pattern for long-term success.Meal timing matters too.
Avoid late-night eating, include plenty of protein and fiber during the day, and try taking a 10-minute walk after meals to improve blood sugar control.Focus on your waistline—not just the scale.
Even if your weight changes slowly, a smaller waist circumference often means you're losing harmful visceral fat and improving your overall metabolic health.
Not all body fat is created equal. While subcutaneous fat—the layer resting just beneath your skin—may pose a cosmetic concern, visceral adipose tissue (VAT) represents a profound clinical threat. Shrouded deep within the abdominal cavity and wrapping around vital organs like the liver and pancreas, visceral fat functions not as a passive storage depot, but as an active, aggressive endocrine organ. It relentlessly secretes pro-inflammatory cytokines, including TNF-alpha and interleukin-6 (IL-6), which trigger systemic inflammation and disrupt delicate insulin signaling pathways (Nurkolis et al., 2025).
The most critical realization for any patient or practitioner is that exercise alone cannot outrun the metabolic consequences of a poor diet when visceral fat is the target. Because VAT is uniquely sensitive to hormonal fluctuations—particularly the "storage signal" of insulin—its accumulation is governed meal-by-meal by nutritional choices (Krittayaphong et al., 2024). Visceral fat depots drain directly into the liver through the portal vein, making them the primary recipients of high-fructose and high-glycemic loads that drive ectopic fat deposition and non-alcoholic fatty liver disease (NAFLD) (Vij et al., 2025).
However, this metabolic volatility is also a doorway to rapid recovery. Research confirms that visceral fat is more "labile" than subcutaneous fat; it is the first to be mobilized when insulin levels drop. A strategic nutritional intervention can reduce visceral fat by 5–10% within just 8 to 12 weeks, leading to immediate improvements in HbA1c, lipid profiles, and liver enzymes—even if the number on the scale barely moves (Krittayaphong et al., 2024). By prioritizing protein, managing carbohydrate quality, and leveraging the timing of nutrient intake, you can effectively "disarm" this internal inflammatory machine and reclaim your metabolic health (Akbari et al., 2024).
Why is diet the primary driver of visceral fat loss
Not all body fat is equal. The fat sitting beneath your skin — subcutaneous fat — is relatively harmless. Visceral adipose tissue (VAT), the fat that wraps around your internal organs, is a different story. It actively secretes inflammatory chemicals, disrupts insulin signalling, and increases your risk of type 2 diabetes, heart disease, and fatty liver — all before the scale shows anything alarming.
Here is the most important thing to understand: exercise alone cannot outrun a poor diet when visceral fat is the target. VAT is metabolically driven. Its accumulation is governed primarily by hormonal signals — especially insulin — that are controlled, meal by meal, by what you eat.
Key clinical takeaway: A reduction of just 5–10% of visceral fat — achievable through diet in 8–12 weeks — meaningfully improves insulin sensitivity, reduces liver fat, and lowers inflammatory markers, even if your weight barely changes (Krittayaphong et al.2024).
How diet changes your fat biology
To make smart food choices for visceral fat, it helps to understand why certain foods store fat around your organs in the first place.
Insulin: the master regulator
Every time you eat carbohydrates or — to a lesser extent — protein, your pancreas releases insulin. In healthy amounts, insulin is essential. But when chronically elevated, insulin acts as a one-way door: it promotes fat storage inside fat cells and prevents the release of stored fat for energy. Visceral fat depots are especially sensitive to this effect because they drain directly into the liver through the portal vein, making them prime recipients of the hormonal signals that drive ectopic fat deposition.
Inflammation and adipokines
Visceral fat is not inert. It produces pro-inflammatory molecules — including TNF-α and IL-6 — and suppresses adiponectin, a hormone that would otherwise improve insulin sensitivity. A diet high in refined carbohydrates and poor-quality fats drives diet-induced endotoxemia, a condition where gut bacteria leak into circulation and amplify this inflammation further.(Nurkolis et al.2025)
The good news: dietary change reverses these processes faster than almost any other intervention.
Protein — The Most Powerful Macronutrient for Visceral Fat Loss
Strongest evidence-backed dietary lever
High-protein intake (1.6–2.4 g/kg/day) consistently outperforms standard protein diets for visceral fat reduction
Thermic Effect of Food (TEF)
Protein has the highest thermic effect among all macronutrients
~20–30% of calories are expended during digestion and metabolism
Leads to higher energy expenditure without increasing physical activity
Appetite Regulation & Hormonal Effects
Stimulates key satiety hormones:
GLP-1 (glucagon-like peptide-1)
PYY (peptide YY)
CCK (cholecystokinin)
Results in:
Reduced hunger
Lower caloric intake
Improved postprandial glucose control
Lean Mass Preservation
Prevents loss of skeletal muscle during calorie restriction
Maintains resting metabolic rate (RMR)
Enhances nutrient partitioning toward muscle rather than fat
Metabolic Advantages
Reduces postprandial insulin spikes compared to high-carbohydrate meals
Improves insulin sensitivity
Supports fat oxidation, particularly when combined with energy deficit
Practical Implementation
Target 25–40 g protein per meal
Distribute evenly across 3–4 meals/day
Prioritize leucine-rich sources to maximize muscle protein synthesis
Best Protein Sources for Visceral Fat Loss
Animal-based:
Eggs
Greek yogurt
Whey protein
Lean meats
Fatty fish
Plant-based:
Lentils
Edamame
Legumes (combined for amino acid completeness)
Synergy with Resistance Training
Combining high-protein intake with resistance training:
Maximizes visceral fat reduction
Preserves or increases lean muscle mass
Lowers insulin area-under-the-curve (AUC)
Clinical Takeaway
Protein is not just a macronutrient—it is a metabolic regulator
Adequate intake is essential for targeting visceral fat, not just overall weight loss
Carbohydrates and visceral fat: quality matters more than quantity
The low-carb versus moderate-carb debate often misses the more important point: carbohydrate quality is the primary dietary driver of visceral fat accumulation in most people.
The fructose-liver connection
Fructose — found in table sugar, high-fructose corn syrup, fruit juices, and many "healthy" sauces — is processed almost exclusively by the liver. Unlike glucose, it bypasses normal appetite regulation and is preferentially shunted toward de novo lipogenesis (making new fat), directly contributing to NAFLD and visceral fat accumulation.
Fibre is protective
Dietary fibre slows glucose absorption, feeds beneficial gut bacteria that produce short-chain fatty acids (SCFAs), and improves insulin sensitivity through the gut-liver axis. A 2025 systematic review confirmed that predominantly plant-based dietary patterns — rich in fibre from legumes, vegetables, and whole grains — significantly reduce visceral adipose tissue compared with control diets. (Vij et al.2025)
✓Eliminate sugar-sweetened beverages — the single highest-impact change for most patients
✓Replace refined grains with intact whole grains (oats, barley, brown rice)
✓Include at least two servings of legumes weekly
✗Avoid fruit juices even if "100% natural" — the fibre is gone, the fructose stays
✗Don't confuse "low-fat" processed foods with healthy options — they often substitute fat with sugar
Dietary fat: friend or foe?
Dietary Fat and Visceral Fat: Quality Over Quantity
Dietary fat does not directly translate into visceral fat accumulation
The type of fat consumed plays a far more critical role than total fat intake
Monounsaturated Fatty Acids (MUFAs)
Found in:
Olive oil
Avocados
Nuts
Consistently associated with:
Lower visceral fat levels
Improved insulin sensitivity
Mechanism:
Enhances lipid metabolism
Reduces inflammatory signaling
Omega-3 Fatty Acids (EPA & DHA)
Sources:
Fatty fish (salmon, sardines, mackerel)
Flaxseeds (ALA precursor)
Mechanisms:
Activate PPAR (peroxisome proliferator-activated receptors)
Increase fat oxidation
Suppress hepatic lipid synthesis
Clinical effect:
Reduction in visceral adiposity
Improvement in metabolic health markers
⚠️ Saturated Fat: Context Matters
Evidence remains mixed in isolation
Becomes harmful when combined with:
Refined carbohydrates
High glycemic load diets
This combination:
Worsens insulin resistance
Promotes visceral fat accumulation
❌ Trans Fats
Consistently harmful across all studies
Effects:
Increase inflammation
Impair insulin sensitivity
Promote visceral fat deposition
Recommendation:
Eliminate completely from the diet
Best Fat Sources for Reducing Visceral Fat
Extra virgin olive oil
Salmon and sardines
Mackerel
Walnuts and almonds
Avocado
Flaxseeds
Clinical Takeaway
Focus on fat quality, not just quantity
Prioritize MUFAs and omega-3s while avoiding trans fats and minimizing harmful dietary patterns involving refined carbohydrates
Mediterranean vs Low-Carb vs Low-Fat: What the Network Meta-Analysis Shows
One of the most common clinical questions is: Which diet works best for visceral fat and weight loss?
The most robust comparative evidence comes from the Akbari et al. 2024 network meta-analysis
This analysis:
Included 7 randomized controlled trials (9 trial arms)
Total 1,004 participants
Used PRISMA-compliant frequentist random-effects methodology
Simultaneously ranked low-carb, Mediterranean, and low-fat diets
Key Results
Low-carb vs Mediterranean
Additional weight loss: −2.70 kg
95% CI: −4.65 to −0.75
P-score Rankings (Weight Loss)
Low-carb: 0.90 (Rank #1)
Low-fat: 0.52
Mediterranean: 0.28
P-score Rankings (Body Fat Reduction)
Low-carb: 0.71 (Rank #1)
Across all diets
All three produced significant weight loss vs baseline
Which Diet Performs Best?
Best for Short-Term Weight Loss: Low-Carbohydrate Diet
Ranked #1 for both total weight and body fat reduction
Produced significantly greater weight loss than the Mediterranean diet
Mechanism:
Rapid insulin reduction
Increased lipolysis and visceral fat mobilization
Particularly effective in:
Insulin-resistant individuals
Type 2 diabetes patients
Best for Long-Term Sustainability: Mediterranean Diet
Ranked lowest for short-term weight loss in the analysis
However, offers:
Strong cardiovascular protection
Anti-inflammatory effects
Superior long-term adherence
Remains a gold standard for overall metabolic health
Low-Fat Diet: Moderate Performance
Intermediate ranking between low-carb and Mediterranean
Effective for weight loss, but less potent for visceral fat reduction
Clinical Interpretation
The network meta-analysis confirms:
Low-carb diets are superior for short-term fat and weight loss
However, important limitations remain:
Outcomes vary based on:
Age
Sex
Genetics
Lifestyle factors
Long-term sustainability and safety require further study
Practical Clinical Strategy
For many patients, the most effective approach is:
Phase 1 (8–12 weeks): Low-carbohydrate diet
Rapid visceral fat reduction
Improved insulin sensitivity
Phase 2: Mediterranean-style maintenance
Long-term adherence
Cardiometabolic protection
Key Takeaway
No single diet is universally superior
Low-carb excels in the short term, especially for insulin resistance
Mediterranean diet dominates long-term outcomes
The optimal strategy is sequential and personalized, not dogmatic
Personalised approach
✓Insulin-resistant or type 2 diabetic phenotype → begin with low-carb (<100g carbs/day) for maximal early VAT reduction
✓General population without metabolic disease → Mediterranean diet is the most sustainable first-line approach
✓Weight loss plateaus → consider cycling to a low-carb phase for 4–8 weeks to break stagnation
✓Monitor: HbA1c, triglycerides, waist circumference, and ALT at baseline and 3 months
Intermittent fasting and time-restricted eating
Intermittent fasting (IF) — particularly the 16:8 time-restricted feeding model — has accumulated substantial clinical interest as a tool for visceral fat reduction. Its primary mechanism is straightforward: extending the overnight fasting window lowers insulin exposure for a larger portion of the day, allowing adipose tissue to mobilise stored fat more freely.
Emerging mechanistic research published in 2024 found that intermittent fasting improves insulin resistance not only through calorie reduction but through direct modulation of the gut microbiota and bile acid metabolism — two pathways that regulate hepatic fat processing and systemic inflammation.(Lei et al, 2024)
When total caloric intake is matched, IF produces visceral fat loss comparable to continuous calorie restriction, but with reported improvements in adherence for certain populations — particularly those who find meal tracking difficult.
IF works best when combined with a high-protein eating window. Without adequate protein during eating periods, muscle loss — not just fat loss — can occur, which is counterproductive for long-term metabolic health.
Plant-based diets and visceral fat: what the latest evidence says
A 2025 systematic review and meta-analysis evaluated the effect of predominantly plant-based dietary patterns on visceral fat across multiple randomised controlled trials. The findings were clinically meaningful: plant-based diets significantly reduced visceral adipose tissue compared with control diets, primarily through higher fibre intake, SCFA production, reduced dietary acid load, and gut microbiome remodelling.
Importantly, "plant-based" did not require strict veganism. Even flexitarian patterns — reducing animal products without eliminating them — showed measurable reductions in VAT when centred on whole plant foods. The key driver was fibre density and the displacement of refined carbohydrates and processed meats, not the complete absence of animal products.
Practical Diet Protocols: What to Actually Eat
These templates are designed as flexible macronutrient frameworks, tailored to different metabolic phenotypes. They are not rigid meal plans—food quality, adherence, and metabolic context remain paramount.
Template 1 — High-Protein Fat Loss (General Population)
Protein: 30–35%
Carbohydrates: 35–40%
Fat: 25–30%
Key Focus:
Emphasize lean protein at every meal
Choose low-glycemic index (GI) carbohydrates
Use extra virgin olive oil as the primary fat source
Best suited for:
General fat loss
Patients without significant insulin resistance
Template 2 — Low-Carbohydrate (Insulin-Resistance Phenotype)
Protein: 30–35%
Carbohydrates: <100 g/day
Fat: 40–45%
Key Focus:
Prioritize monounsaturated fats (MUFA) and omega-3 fatty acids
Include non-starchy vegetables liberally
Minimize refined carbohydrates and sugars
Monitoring:
Assess HbA1c and triglycerides at ~3 months
Clinical Insight:
Supported by evidence from the Akbari et al. 2024 network meta-analysis
Represents the most effective short-term strategy for visceral fat reduction
Template 3 — Mediterranean Anti-Inflammatory Pattern
Protein: 20–25%
Carbohydrates: 40–45%
Fat: 30–35%
Key Focus:
High intake of fiber-rich whole grains and legumes
Fatty fish 2–3 times per week
Olive oil as the primary fat source
Limit red meat to ≤1 serving/week
Best suited for:
Long-term maintenance
Cardiometabolic risk reduction
Clinical Strategy:
Ideal as a maintenance phase following an initial low-carb intervention
Meal Timing Principles
✓ Prioritize protein and fiber first within meals
→ Blunts postprandial glucose excursions✓ Post-meal activity matters
→ A 10-minute walk can reduce post-meal glucose by up to ~20%✓ Front-load calories earlier in the day
→ Late-night eating is associated with increased visceral fat deposition✓ Time-restricted eating (if used)
→ Prefer an eating window that ends before 7–8 pm
Common Mistakes That Stall Visceral Fat Loss
✗ Overconsumption of “healthy” calorie-dense foods
→ Nuts and olive oil are beneficial but energy-dense and easy to overeat✗ Liquid calories
→ Smoothies, fruit juices, specialty coffees, and alcohol bypass satiety mechanisms✗ Insufficient protein intake
→ <1.2 g/kg leads to muscle loss and reduced metabolic rate✗ Extreme calorie restriction
→ <1,200 kcal/day can trigger metabolic adaptation and muscle catabolism✗ Neglecting sleep
→ Even short-term sleep deprivation elevates cortisol and promotes visceral fat storage✗ Relying solely on body weight
→ Waist circumference is a more accurate proxy for visceral fat changes
Clinical Takeaway
Effective visceral fat reduction requires:
Right macronutrient distribution
Meal timing optimization
Avoidance of common behavioral pitfalls
The most successful strategy is structured, personalized, and sustainable—not extreme or short-lived interventions
Get my free meal plan ↗Track my progress ↗
Frequently asked questions
How long does it take to lose visceral fat with diet?
Most well-designed dietary interventions show measurable reductions in VAT within 8–12 weeks when a moderate caloric deficit (300–500 kcal/day) is combined with adequate protein and reduced refined carbohydrates. Imaging studies confirm changes in liver and visceral fat even before body weight drops significantly.
Is intermittent fasting better than daily calorie restriction for belly fat?
When total calories are matched, both approaches produce comparable visceral fat loss. Intermittent fasting may offer additional benefits through gut microbiome modulation and bile acid metabolism — independent of calorie reduction alone — making it a useful option for patients who struggle with constant tracking.
Does a plant-based diet reduce visceral fat?
Yes. A 2025 systematic review and meta-analysis confirmed that predominantly plant-based diets significantly reduce visceral adipose tissue, driven primarily by higher dietary fibre, SCFA production, and gut microbiome improvements. You do not need to go fully vegan — a flexitarian approach centred on whole plant foods is effective.
Which diet is best for visceral fat — Mediterranean, low-carb, or low-fat?
A 2024 network meta-analysis directly comparing all three found the low-carbohydrate diet ranked highest for both weight loss (P-score 0.90) and body fat reduction (P-score 0.71), producing significantly greater weight loss than the Mediterranean diet (−2.70 kg, 95% CI: −4.65 to −0.75). However, the Mediterranean diet outperforms in the long term for cardiovascular health and sustainability. The best clinical strategy is often a low-carb induction phase followed by a Mediterranean maintenance pattern.
How does insulin affect visceral fat specifically?
Chronically elevated insulin drives fat storage and inhibits fat mobilisation in adipocytes. Visceral fat deposits are metabolically active and insulin-sensitive, making them especially responsive to dietary strategies that lower postprandial insulin — such as reducing refined carbohydrates, increasing fibre, and distributing protein throughout the day.
Can I lose visceral fat without losing weight overall?
Yes — particularly early in a dietary intervention. VAT is more metabolically active than subcutaneous fat and responds faster to insulin and dietary changes. It is clinically common to see reductions in waist circumference and hepatic fat on imaging before overall weight significantly changes, especially with structured dietary and exercise interventions.
What is the single most important dietary change for visceral fat?
Eliminating sugar-sweetened beverages and added fructose delivers the largest return for a single dietary change, followed closely by increasing daily protein intake. These two modifications directly reduce postprandial insulin, lower hepatic de novo lipogenesis, and improve satiety — addressing the three central drivers of VAT accumulation simultaneously.
Author’s Note (Clinician’s Perspective)
As a clinician managing patients with obesity, insulin resistance, and type 2 diabetes daily, I have come to recognize a critical truth: not all weight loss is metabolically equal. The reduction of visceral adipose tissue—rather than total body weight alone—is what consistently translates into meaningful improvements in glycemic control, hepatic health, and cardiovascular risk. This distinction is often underappreciated in both clinical practice and public discourse.
In real-world settings, patients frequently present with frustration after attempting multiple dietary approaches—low-fat, calorie-restricted, or even “healthy eating”—with limited success in improving metabolic markers. What is often missing is a targeted strategy that addresses the underlying drivers of visceral fat accumulation, particularly chronic hyperinsulinemia, poor nutrient partitioning, and low-grade inflammation. From this perspective, diet is not merely a tool for calorie reduction, but a metabolic intervention.
The inclusion of high-quality comparative evidence, such as the Akbari et al. 2024 network meta-analysis, reinforces an important clinical insight: while multiple dietary patterns can reduce visceral fat, their effectiveness varies depending on the patient’s metabolic phenotype, degree of insulin resistance, and long-term adherence. In my practice, low-carbohydrate approaches often yield rapid improvements in patients with significant insulin resistance, whereas Mediterranean-style diets provide a more sustainable framework for long-term cardiometabolic health.
Importantly, no single dietary model is universally superior. The art of clinical nutrition lies in individualization—aligning evidence-based strategies with patient preferences, cultural context, and metabolic goals. Sustainable visceral fat reduction requires not just the right diet, but the right diet for the right patient.
This chapter is therefore designed not as a prescriptive guideline, but as a clinically grounded framework to help practitioners and informed patients make more precise, physiology-driven decisions.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
One Diet Lowers Triglycerides. Another May Lower LDL. Here's What New Research Reveals.
Beyond the Scale: Low-Carb vs Low-Fat Diets for Visceral Fat Loss and Muscle Preservation
Visceral Fat Treatment: GLP-1, Semaglutide, and SGLT2 Explained
How to Lose Visceral Fat Fast: The Science of HIIT, Zone 2, and Strength Training
Is Your Muscle Insulin Resistant? 2026 Update | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Vij, V., Deshmukh, K., Vijayageetha, M., Goyal, C., Gumashta, J., & Gandhi, A. P. (2025). Effect of predominantly plant-based diets on visceral fat: A systematic review and meta-analysis. Journal of Human Nutrition and Dietetics, 38(2), e70055. https://doi.org/10.1111/jhn.70055
Nurkolis, F., Harbuwono, D. S., Taslim, N. A., et al. (2025). New insight on dietary strategies to increase insulin sensitivity and reduce diabetes prevalence: An expert perspective and recommendation. Discover Food, 5, 136. https://doi.org/10.1007/s44187-025-00422-6
Krittayaphong, R., Treesuwan, W., Pramyothin, P., Songsangjinda, T., Kaolawanich, Y., Srivanichakorn, W., Jangtawee, P., Yindeengam, A., Tanapibunpon, P., & Vanavichit, A. (2024). Impact of diet intervention on visceral adipose tissue and hepatic fat in patients with obesity or type 2 diabetes: A randomized trial. Scientific Reports, 14(1), 21388. https://doi.org/10.1038/s41598-024-72246-w
Lei, S., Liu, G., Wang, S., Zong, G., Zhang, X., Pan, L., & Han, J. (2024). Intermittent fasting improves insulin resistance by modulating the gut microbiota and bile acid metabolism in diet-induced obesity. Molecular Nutrition & Food Research, 68, 2400451. https://doi.org/10.1002/mnfr.202400451
Akbari, M., Vali, M., Rezaei, S., Bazmi, S., Tabrizi, R., & Lankarani, K. B. (2024). Comparison of weight loss effects among overweight/obese adults: A network meta-analysis of Mediterranean, low carbohydrate, and low-fat diets. Clinical Nutrition ESPEN, 64, 7–15. https://doi.org/10.1016/j.clnesp.2024.08.023