The Silent Window of Cardiometabolic Disease: How to Detect Insulin Resistance Before Glucose Rises
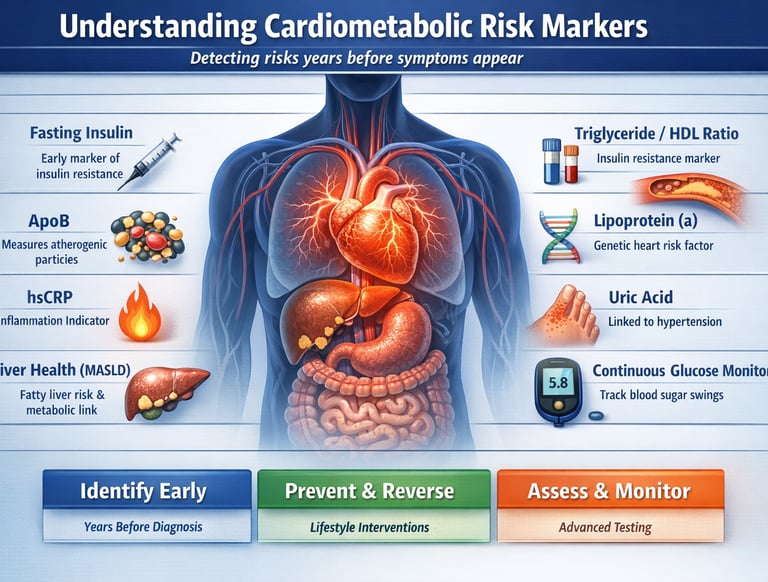
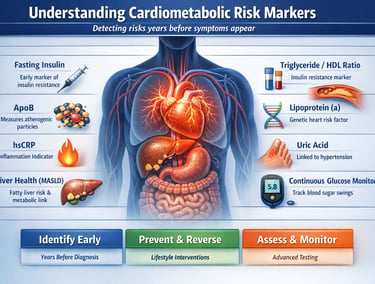
Discover the hidden biomarkers of insulin resistance, inflammation, and heart disease years before diabetes develops. Learn how fasting insulin, ApoB, hsCRP, and advanced cardiometabolic testing can identify risk early and help prevent cardiovascular disease.
DIABETESMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/2/202617 min read
What if your annual blood tests are normal—but your risk of diabetes, heart disease, and fatty liver is already increasing?
For millions of people, this is exactly what happens.
Most cardiovascular disease and type 2 diabetes do not begin when glucose rises above a diagnostic threshold or when cholesterol becomes abnormal. The biological processes that drive these conditions often start 10 to 15 years earlier, silently progressing beneath the surface while standard laboratory tests remain reassuringly normal.
This hidden phase of disease is increasingly recognized as the most important window in preventive medicine.
During this period, insulin levels begin to rise as the body struggles to maintain normal blood sugar. The liver starts producing excess triglycerides. Small changes appear in inflammatory markers. Atherogenic lipoprotein particles accumulate within the arterial wall. Endothelial dysfunction develops long before a plaque becomes visible on a scan.
Yet none of these changes may be detected by routine fasting glucose measurements alone.
Modern cardiometabolic science has transformed our understanding of disease progression. Researchers now recognize that fasting insulin, Apolipoprotein B (ApoB), high-sensitivity C-reactive protein (hsCRP), liver fat accumulation, and other emerging biomarkers can identify metabolic dysfunction years before traditional diagnostic criteria are met.
This shift represents a fundamental change in medicine. Instead of waiting for disease to appear, clinicians can increasingly detect risk during its earliest and most reversible stages.
In this comprehensive guide, you will learn:
Why normal glucose does not always mean normal metabolic health
How insulin resistance develops years before diabetes
The most important cardiometabolic biomarkers available today
Why ApoB often predicts cardiovascular risk better than LDL cholesterol
How inflammation, fatty liver, and visceral fat accelerate disease progression
Which laboratory tests provide the greatest preventive value
Practical strategies for interpreting and improving your results
The Silent Decade Before Diabetes and Heart Disease
Stage 1 (Years 0–5)
Rising fasting insulin
Normal glucose
Increasing visceral fat
Early hepatic insulin resistance
Stage 2 (Years 5–10)
Elevated triglycerides
Lower HDL
Fatty liver development
Rising ApoB
Stage 3 (Years 10–15)
Prediabetes
Elevated HbA1c
Chronic inflammation
Endothelial dysfunction
Stage 4
Type 2 diabetes
Coronary artery disease
Stroke
Heart failure
Disease is usually diagnosed at Stage 4, but prevention is most effective during Stages 1 and 2.
Why Single Markers Are No Longer Enough
The old model of cardiovascular risk assessment was simple: check LDL cholesterol, keep it under a threshold, and prescribe a statin if it was high. Clean and convenient — but dangerously incomplete.
Cardiometabolic disease is not driven by a single defect. It is a cascade — a chain reaction in which each link feeds the next:
Insulin resistance develops silently in muscle and liver tissue, forcing the pancreas to overcompensate with higher insulin output
Hyperglycemia follows as the pancreas eventually exhausts its ability to keep blood sugar in check
Dyslipidemia — specifically high triglycerides, small dense LDL particles, and low HDL — emerges as a downstream consequence of metabolic dysregulation
Chronic low-grade inflammation (metaflammation) amplifies every step of the process, damaging arterial walls and impairing glucose uptake
Endothelial dysfunction — damage to the lining of blood vessels — is the final common pathway toward atherosclerosis, heart attack, and stroke
A 2026 landmark study on global cardiovascular risk factors projects that the burden of modifiable cardiovascular risk will continue rising through 2050 unless detection and intervention strategies are fundamentally modernised (Chong et al., 2025). That modernisation begins with better biomarkers.
Clinical Insight
Disease does not begin on the day of diagnosis. It begins years earlier, silently, in biomarker shifts that standard panels miss. The goal of advanced cardiometabolic profiling is to close that gap.
Tier 1 — Core Clinical Markers: The Essentials You Already Know
Glycemic Markers
These are the first-line indicators of how your body handles sugar — and they are the most widely used, though far from the most sensitive.
Fasting glucose — Measures blood sugar after an overnight fast. Normal is below 100 mg/dL. Prediabetes begins at 100–125 mg/dL. Critically, glucose can remain "normal" even while insulin resistance is already severe, because the pancreas is compensating by producing more insulin
HbA1c (glycated haemoglobin) — Reflects average blood glucose over the past 2–3 months. The prediabetes range is 5.7–6.4%. A useful, accessible marker, but it misses early insulin resistance and can be artificially skewed by conditions such as anaemia or haemoglobin variants
Lipid Profile
LDL-C (low-density lipoprotein cholesterol) — The traditional "bad cholesterol." Often reliable, but it can be falsely reassuring in patients with metabolic syndrome, where LDL particle number is more dangerous than LDL concentration
HDL-C (high-density lipoprotein cholesterol) — Generally protective, though its role is increasingly understood to be context-dependent. Very high HDL in the setting of inflammation can lose its protective properties
Triglycerides — A direct reflection of carbohydrate and caloric overload. Elevated triglycerides are one of the earliest detectable signs of insulin resistance. When combined with low HDL, they form a classic metabolic syndrome pattern
Blood Pressure
One of the strongest individual predictors of cardiovascular disease. Chronically elevated blood pressure stiffens arteries, damages the kidneys, and strains the heart. It is also a consequence — and driver — of insulin resistance itself
Tier 2 — Insulin Resistance Markers: The Early Warning System
This is where standard clinical care often fails patients. Insulin resistance can persist for a decade before glucose rises — yet it is driving silent damage throughout the body the entire time.
Fasting Insulin
Measures how much insulin the pancreas needs to keep blood sugar stable. When insulin is chronically elevated, even in the fasting state, it signals that cells have become resistant, and the pancreas is overworking to compensate
Optimal fasting insulin is generally considered to be below 5–8 µIU/mL, though reference ranges vary by lab. Many people with "normal" glucose already have fasting insulin levels of 15–25 µIU/mL — a major red flag
This marker is inexpensive, widely available, and vastly underused in primary care settings
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance)
A simple calculated score using fasting glucose and fasting insulin together. It provides a standardised estimate of insulin resistance severity
A score above 2.0–2.5 is generally considered to indicate insulin resistance. This marker is particularly useful for monitoring trends over time as patients implement lifestyle changes
Waist Circumference
A low-tech but powerful proxy for visceral (belly) fat — the metabolically active fat that surrounds internal organs and drives inflammation and insulin resistance
Risk thresholds: above 88 cm (35 inches) for women; above 102 cm (40 inches) for men. This single measurement independently predicts cardiometabolic risk, even in people with a normal BMI
Key Principle
Insulin resistance often precedes the onset of type 2 diabetes by 10 to 15 years. Testing for it early is one of the most powerful preventive actions a clinician can take (Rizo-Roca et al., 2025).
Tier 3 — Advanced Lipid Markers: Beyond LDL Cholesterol
Modern lipidology has moved well beyond the simple LDL number. The key question is not just how much cholesterol is in the blood, but how many atherogenic particles are there, and how dangerous are they?
Apolipoprotein B (ApoB)
Every single atherogenic lipoprotein particle — including LDL, VLDL, IDL, and Lp(a) — carries exactly one ApoB protein. This means ApoB directly counts the total number of dangerous particles
A person can have a "normal" LDL-C but a high ApoB if their particles are small and dense (which is far more dangerous for arteries). This is especially common in metabolic syndrome
Multiple major guidelines and recent lipid research now identify ApoB as the superior predictor of atherosclerotic cardiovascular disease compared to LDL-C alone (Yang, 2025)
Optimal ApoB is generally considered to be below 70–80 mg/dL for high-risk individuals
Lipoprotein(a) [Lp(a)]
A genetically determined lipoprotein that is largely unresponsive to lifestyle changes. It is an independent risk factor for early heart disease and aortic stenosis
Elevated Lp(a) — generally above 50 mg/dL or 125 nmol/L — is found in approximately 20% of the global population and dramatically increases cardiovascular risk, particularly when combined with other risk factors
It should be measured at least once in every adult's lifetime, especially those with a family history of premature cardiovascular disease
Non-HDL Cholesterol
Calculated simply by subtracting HDL-C from total cholesterol, non-HDL cholesterol captures the full atherogenic cholesterol burden — including remnant particles that standard LDL testing misses
A practical and underused alternative to ApoB when the latter is unavailable
Tier 4 — Inflammatory Markers: The Hidden Fire
Chronic low-grade inflammation — sometimes called "metaflammation" — is not the dramatic inflammation you feel when you twist an ankle. It is quieter, slower, and far more damaging over time. It corrodes arterial walls, blocks insulin signalling, and promotes the growth of atherosclerotic plaques.
High-Sensitivity CRP (hsCRP)
The most widely available inflammatory marker in clinical practice. The hsCRP test is significantly more sensitive than standard CRP and can detect low-level inflammation that standard tests miss
Risk interpretation: below 1 mg/L = low cardiovascular risk; 1–3 mg/L = moderate risk; above 3 mg/L = high risk (in the absence of acute infection or injury)
Elevated hsCRP predicts future cardiovascular events independently of cholesterol levels. The landmark JUPITER trial demonstrated that treating elevated hsCRP — even in patients with normal LDL — significantly reduced heart attack risk
Interleukin-6 (IL-6)
An upstream signalling cytokine that triggers CRP production in the liver. Elevated IL-6 is linked to visceral fat, insulin resistance, and accelerated atherosclerosis
Currently used more in research and specialised clinical settings, but increasingly accessible and valuable for understanding the inflammatory burden
Tumour Necrosis Factor-alpha (TNF-α)
A key driver of insulin resistance at the cellular level. Secreted by adipose tissue, TNF-α interferes with insulin receptor signalling and promotes systemic inflammation
An emerging marker in precision metabolic medicine, particularly relevant in patients with significant visceral adipositythe
Tier 5 — Vascular and Endothelial Markers: The Artery's Health Report
The endothelium — the single-cell lining of every blood vessel in the body — is not just structural scaffolding. It is a dynamic, hormonally active organ that regulates blood flow, prevents clotting, controls inflammation, and maintains vascular tone. Its dysfunction precedes visible plaque by years.
Flow-Mediated Dilation (FMD) — A non-invasive ultrasound test measuring the ability of the brachial artery to dilate in response to increased blood flow. Reduced FMD is an early and sensitive marker of endothelial dysfunction, detectable before any clinical symptoms
ICAM-1 and VCAM-1 (adhesion molecules) — These molecules are expressed on the surface of damaged endothelial cells, allowing white blood cells and cholesterol particles to adhere and begin the process of plaque formation. Elevated levels indicate early atherosclerotic activity
Pulse Wave Velocity (PWV) — A gold-standard measurement of arterial stiffness. Stiffer arteries indicate more advanced vascular ageing and are independently associated with heart attack, stroke, and kidney disease. PWV increases with age, hypertension, diabetes, and smoking
Recent advances in digital phenotyping — including wearable-based vascular assessments — are making these markers increasingly accessible outside of specialised cardiology centres (Tan et al., 2026).
Tier 6 — Liver Markers: The Metabolic Engine Room
The liver sits at the metabolic crossroads of the entire body — processing glucose, synthesising lipoproteins, clearing toxins, and managing energy storage. In cardiometabolic disease, the liver is almost always involved early.
ALT and AST (liver enzymes) — Elevated levels signal hepatocellular stress. Metabolic dysfunction-associated steatotic liver disease (MASLD, formerly known as NAFLD) affects approximately 25–30% of adults globally and is strongly linked to insulin resistance, type 2 diabetes, and cardiovascular mortality. Crucially, liver enzyme elevation in the context of metabolic syndrome is not "just a liver problem" — it is a whole-body alarm signal
GGT (gamma-glutamyl transferase) — A sensitive marker of oxidative stress and liver cell damage. Elevated GGT is an independent predictor of insulin resistance, type 2 diabetes, and cardiovascular events — often before ALT becomes abnormal
Liver fat quantification (imaging) — Hepatic steatosis (fatty liver), measured by ultrasound or MRI-based techniques, is one of the most powerful predictors of future cardiometabolic disease. Even modest degrees of liver fat excess accelerate both atherosclerosis and insulin resistance
Clinical Insight
A fatty liver is not merely a liver condition. It is one of the earliest and most reliable indicators of cardiometabolic risk — present in many patients years before diabetes or heart disease is diagnosed.
Tier 7 — Emerging and Functional Markers: The Frontier of Precision Medicine
The newest generation of cardiometabolic biomarkers is moving from research laboratories into clinical practice, driven by advances in metabolomics, digital health technology, and personalised medicine (Macvanin & Klisic, 2026).
Adiponectin and Leptin
Adiponectin — An anti-inflammatory hormone secreted by healthy fat cells. Low adiponectin levels are associated with insulin resistance, inflammation, and cardiovascular disease. Adiponectin falls as visceral fat accumulates — making it a useful early marker of metabolic deterioration
Leptin — The satiety hormone. When fat cells multiply, they produce more leptin — but the brain eventually stops responding to its signal (leptin resistance), leading to perpetual hunger and energy dysregulation. High leptin levels, combined with obesity, indicate leptin resistance and a high-risk metabolic phenotype
Uric Acid
Once considered relevant only for gout, uric acid is now recognised as an independent marker of insulin resistance, hypertension, and cardiovascular risk. Elevated uric acid inhibits nitric oxide production in the endothelium, directly impairing vascular function
Optimal levels are generally below 5.5 mg/dL for men and 4.5 mg/dL for women
Continuous Glucose Monitoring (CGM) Metrics
Glycemic variability — Large swings in blood glucose throughout the day, even within the "normal" range, are associated with increased oxidative stress, endothelial damage, and long-term cardiometabolic risk
Time in range (TIR) — The percentage of time blood glucose stays within a target range (typically 70–140 mg/dL). CGM is now being explored as a screening tool even in non-diabetic individuals with metabolic risk factors
Digital phenotyping approaches — including CGM integrated with wearable activity and heart rate data — represent the most advanced frontier of individualised risk profiling (Tan et al., 2026)
Breakdown of the cardiometabolic scorecard
Tier 1: The "Early Warning" Markers (Very Early / Excellent Value)
Fasting Insulin: Detects insulin resistance at a very early stage. It offers excellent clinical value for catching metabolic changes before they alter blood sugar levels.
HOMA-IR (Homeostatic Model Assessment for Insulin Resistance): Identifies metabolic dysfunction very early, providing excellent insight into how hard your body is working to manage blood sugar.
Tier 2: Pre-Symptomatic Screeners (Early / Excellent Value)
TG/HDL Ratio (Triglyceride-to-HDL Ratio): Spots metabolic syndrome early with excellent predictive value for cardiovascular and insulin issues.
ApoB (Apolipoprotein B): Measures total atherogenic (plaque-forming) particles early, providing excellent assessment of true heart disease risk compared to standard cholesterol panels.
hsCRP (High-Sensitivity C-Reactive Protein): Detects systemic inflammation early with excellent clinical value for predicting cardiovascular events
.
Tier 3: Targeted Organ & Genetic Risk (Early / High Value)
Lp(a) (Lipoprotein(a)): Identifies genetic cardiovascular risk. Because it is genetically determined, it offers lifelong detection and high clinical value from a single lifetime test.
ALT / GGT (Liver Enzymes): Detect fatty liver disease and liver stress early, offering high clinical utility for metabolic screening.
Tier 4: Traditional Screeners (Late / Moderate Value)
HbA1c (Glycated Haemoglobin): Detects prediabetes and diabetes. However, it alters late in the metabolic disease process, giving it moderate value for early prevention.
Fasting Glucose: Detects active diabetes. Like HbA1c, glucose spikes late after years of underlying insulin resistance, offering moderate value for early intervention.
Putting It Together: Risk Profiles in Plain Language
Understanding your individual biomarker picture requires integrating multiple signals — not reacting to a single number in isolation.
Low Risk Profile
Fasting glucose below 90 mg/dL and fasting insulin below 7 µIU/mL
Normal HbA1c (below 5.4%), ApoB below 80 mg/dL
hsCRP below 1 mg/L, normal liver enzymes, healthy waist circumference
Good endothelial function on vascular assessment
Early Risk Profile (Act Now)
Fasting insulin elevated (above 10 µIU/mL) despite normal glucose — the pancreas is compensating, but the window for lifestyle reversal is still wide open
Triglyceride-to-HDL ratio above 3.0 — a strong surrogate for insulin resistance and small dense LDL
hsCRP in the 1–3 mg/L range, mild elevation in GGT, or incidental fatty liver on ultrasound
Waist circumference approaching or exceeding threshold values
Advanced Risk Profile (Urgent Attention)
HbA1c in prediabetic or diabetic range, HOMA-IR above 3.0
Elevated ApoB with high triglycerides — indicating a large burden of atherogenic particles
hsCRP consistently above 3 mg/L, significant liver steatosis, or impaired endothelial function
Elevated Lp(a) compounding all other risk factors
Practical Panels: What to Ask Your Doctor For
Minimal Panel — Suitable for Primary Care / Annual Check-ups
HbA1c and fasting glucose
Full lipid panel (LDL, HDL, triglycerides, non-HDL)
Blood pressure measurement
Waist circumference (inexpensive and highly informative)
ALT and AST liver enzymes
Expanded Panel — For Anyone with Metabolic Risk Factors
Everything in the minimal panel, plus:
Fasting insulin and HOMA-IR calculation
ApoB and non-HDL cholesterol
hsCRP (high-sensitivity)
GGT and uric acid
Liver ultrasound if enzymes are elevated
Advanced Panel — Precision Medicine Approach
Everything in the expanded panel, plus:
Lp(a) — at least once in lifetime; more often if elevated
IL-6 and adiponectin
Pulse wave velocity or flow-mediated dilation (specialist referral)
CGM-based metabolomics in research or specialised clinical settings
Full metabolomic profiling where available (Rizo-Roca et al., 2025)
Common Mistakes Clinicians and Patients Both Make
Over-relying on LDL-C alone — A "normal" LDL does not mean your arteries are safe, particularly in patients with metabolic syndrome or elevated ApoB
Ignoring fasting insulin — This is the most consequential test that most people have never had. It should be standard in every metabolic workup
Treating numbers instead of mechanisms — Lowering a single marker without addressing the underlying insulin resistance, inflammation, or dyslipidemia driving it rarely changes long-term outcomes
Dismissing borderline results — "Borderline" HbA1c, mildly elevated hsCRP, and slightly high insulin are not minor findings. They are early signals demanding investigation and intervention
Evaluating markers in isolation — One marker in isolation almost always tells an incomplete story. True risk assessment demands a systems-level view of all available data
From Detection to Action: A Three-Step Clinical Strategy
Step 1 — Identify Early Risk
Use fasting insulin and the triglyceride-to-HDL ratio as your first screen for insulin resistance
Add ApoB and hsCRP to characterise atherogenic particle burden and inflammatory status
Do not wait for glucose or HbA1c to become abnormal — by then, significant metabolic damage has already occurred
Step 2 — Address Root Causes
Visceral fat reduction — Even a 5–10% reduction in body weight substantially improves insulin sensitivity, triglycerides, liver fat, and hsCRP
Resistance training and muscle preservation — Skeletal muscle is the body's primary glucose disposal organ. Building and maintaining muscle mass is one of the most powerful anti-diabetic and anti-inflammatory interventions available
Dietary pattern modification — Reducing refined carbohydrate and fructose intake directly targets insulin resistance and triglyceride elevation. A whole-food, minimally processed dietary approach consistently improves the full cardiometabolic panel
Sleep and stress management — Chronic sleep deprivation and cortisol excess independently drive insulin resistance, inflammation, and cardiovascular risk factors that are rarely addressed in standard clinical encounters
Step 3 — Monitor Response Over Time
Track biomarkers at 3–6 month intervals when implementing lifestyle changes, and at 12-month intervals for maintenance monitoring
Use HOMA-IR, fasting insulin, and hsCRP as your primary response markers — they tend to improve faster than HbA1c and LDL-C and give earlier feedback on whether interventions are working
Celebrate directional improvement, not just crossing arbitrary thresholds — a HOMA-IR falling from 4.2 to 2.8 is meaningful progress even if it has not yet reached the "optimal" range
Bottom line: Cardiometabolic disease is largely preventable. The science is clear — early, integrated biomarker profiling combined with targeted lifestyle and, where necessary, pharmacological intervention can halt and even reverse the cardiometabolic cascade (Tahir & Gerszten, 2023).
Frequently Asked Questions
1. What are the most important cardiometabolic risk markers to test?
The most clinically relevant markers include HbA1c, fasting glucose, fasting insulin, triglycerides, HDL-C, Apolipoprotein B (ApoB), and hsCRP. Together, they assess glycemic control, insulin resistance, lipid particle burden, and inflammation—key drivers of cardiometabolic disease.
2. Why is fasting insulin a better early marker than glucose?
Fasting insulin rises years before glucose becomes abnormal, reflecting early insulin resistance. Normal glucose with elevated insulin indicates compensated metabolic dysfunction, where the pancreas is overworking to maintain glycemic control.
3. What is a normal fasting insulin level?
Optimal fasting insulin is generally:
<5–8 µIU/mL → Insulin sensitive
8–15 µIU/mL → Early resistance
>15 µIU/mL → Significant insulin resistance
Interpretation should always be contextualized with glucose and HOMA-IR.
4. What is HOMA-IR and how is it interpreted?
HOMA-IR estimates insulin resistance using fasting glucose and insulin.
<1.0 → Optimal
1.0–2.0 → Acceptable
>2.0–2.5 → Insulin resistance
>3.0 → Advanced dysfunction
It is best used for trend monitoring over time.
5. What is ApoB and why is it superior to LDL cholesterol?
ApoB measures the number of atherogenic lipoprotein particles, making it a more accurate predictor of cardiovascular risk than LDL-C, which measures only cholesterol content. It is increasingly endorsed by the American Heart Association for risk stratification.
6. What is a normal ApoB level?
<80 mg/dL → Optimal (high-risk individuals)
80–100 mg/dL → Moderate risk
>100 mg/dL → Elevated risk
Lower targets are recommended for patients with diabetes or established cardiovascular disease.
7. What does hsCRP indicate about heart disease risk?
hsCRP reflects chronic low-grade inflammation, a key contributor to atherosclerosis.
<1 mg/L → Low risk
1–3 mg/L → Moderate risk
>3 mg/L → High risk
It predicts cardiovascular events independently of cholesterol levels.
8. What is the triglyceride-to-HDL ratio and why is it important?
The triglyceride-to-HDL ratio is a simple surrogate marker of insulin resistance:
<2.0 → Insulin sensitive
2–3 → Intermediate risk
>3.0 → Insulin resistance
It also correlates with small dense LDL particles, which are more atherogenic.
9. Should everyone get Lipoprotein(a) tested?
Yes. Lipoprotein(a) [Lp(a)] should be measured at least once in adulthood. It is genetically determined and significantly increases cardiovascular risk, especially when combined with elevated ApoB or inflammation.
10. What role does the liver play in cardiometabolic risk?
The liver regulates glucose and lipid metabolism. Conditions like metabolic dysfunction-associated steatotic liver disease (MASLD) are strongly linked to insulin resistance, dyslipidemia, and increased cardiovascular risk—even before diabetes develops.
11. Why is GGT an important metabolic marker?
Gamma-glutamyl transferase (GGT) is a sensitive marker of oxidative stress and liver dysfunction. Elevated GGT predicts insulin resistance, type 2 diabetes, and cardiovascular events, often earlier than traditional liver enzymes.
12. What is the role of uric acid in cardiometabolic disease?
Elevated uric acid is associated with insulin resistance, hypertension, and endothelial dysfunction. It impairs nitric oxide production, contributing to vascular stiffness and increased cardiovascular risk.
13. Can continuous glucose monitoring (CGM) help non-diabetics?
Yes. CGM reveals glycemic variability and postprandial spikes, which are linked to oxidative stress and vascular damage—even in individuals with normal HbA1c. It is emerging as a tool for early metabolic risk detection.
14. How early can cardiometabolic disease be detected?
Cardiometabolic dysfunction can be detected 10–15 years before clinical diagnosis using markers like fasting insulin, ApoB, hsCRP, and liver fat assessment. Early detection allows for reversal through lifestyle intervention.
15. Can cardiometabolic risk be reversed?
Yes—especially in early stages. Effective interventions include:
Weight loss (5–10%)
Resistance training
Dietary modification (reduced refined carbohydrates)
Sleep and stress optimization
These strategies improve insulin sensitivity, reduce inflammation, and normalize multiple biomarkers simultaneously.
16. Why Is Muscle the Most Underrated Cardiometabolic Organ?
Key points:
Skeletal muscle disposes of approximately 80% of post-meal glucose.
Sarcopenia worsens insulin resistance.
Muscle acts as a glucose reservoir.
Resistance training improves insulin sensitivity independent of weight loss.
Muscle preservation should be considered a primary cardiometabolic intervention.
If you could only add one test to your standard panel, make it fasting insulin. It detects insulin resistance years — sometimes a decade — before glucose or HbA1c becomes abnormal. Combined with your fasting glucose, it allows calculation of HOMA-IR, giving you a direct window into your metabolic health at its earliest, most reversible stage.
Take Control of Your Cardiometabolic Health
Knowledge is only the beginning. Here is your practical next step checklist — bring it to your next doctor's appointment.
Request fasting insulin alongside your standard fasting glucose
Ask for ApoB to be added to your next lipid panel
Request hsCRP if you have any metabolic risk factors
Have your waist circumference measured and recorded
Ask for liver enzymes (ALT, AST, GGT) if not already included
Discuss Lp(a) testing — at minimum, once in your lifetime
Review your results as a pattern, not as isolated numbers
Clinical pearls
1. The "Pancreatic Compensation" Trap
Scientific Perspective: Fasting glucose is a "lagging indicator." The homeostatic system maintains euglycemia via hyperinsulinemia; therefore, a normal glucose reading often masks an underlying HOMA-IR > 2.0
Having "normal blood sugar" doesn't mean your metabolism is healthy. Your body might be working overtime (producing excess insulin) to keep that sugar normal. Testing fasting insulin reveals the struggle before the system fails.
2. ApoB as the "Particle Passport"
Scientific Perspective: LDL-C measures the mass of cholesterol, but Apolipoprotein B (ApoB) measures the total number of atherogenic particles (VLDL + IDL + LDL). Particle number is a superior predictor of subendothelial retention than cholesterol volume.
Think of LDL-C as the amount of cargo, but ApoB as the number of trucks on the highway. More trucks mean a higher chance of a crash (plaque buildup), even if the trucks aren't fully loaded.
3. The "Metaflammation" Signal (hsCRP)
Scientific Perspective: Atherosclerosis is an inflammatory disease of the arterial wall. High-sensitivity CRP (hsCRP) captures the systemic low-grade inflammation that "primes" the endothelium for lipid deposition and plaque instability.
Cholesterol is the fuel, but inflammation is the match. Even if your cholesterol is low, high inflammation (hsCRP > 2 mg/L) means your "internal fire" is high, which makes your arteries more vulnerable to damage.
4. The Liver as the Metabolic "Canary"
Scientific Perspective: Elevated GGT and ALT (even within the "high-normal" range) often signal the onset of MASLD (fatty liver). Hepatic insulin resistance is a primary driver of systemic dyslipidemia and increased VLDL production.
Your liver is your metabolic engine room. If your liver enzymes are creeping up, it’s an early warning sign that your body is struggling to process energy, often appearing years before a Type 2 Diabetes diagnosis.
5. Muscle as "Metabolic Sink"
Scientific Perspective: Skeletal muscle is responsible for 80 % of postprandial glucose disposal. Sarcopenia (muscle loss) directly reduces the body's glycemic "sink," accelerating the progression toward insulin resistance and cardiometabolic collapse.
Muscle isn't just for looks; it’s your largest "sugar sponge." Building and keeping muscle through resistance training is the most effective way to improve your lab results because it gives your blood sugar a place to go.
The Cardiometabolic Prevention Checklist
□ Fasting insulin measured
□ HOMA-IR calculated
□ ApoB measured
□ hsCRP checked
□ Waist circumference recorded
□ Blood pressure optimized
□ Resistance training performed at least twice weekly
□ Protein intake adequate for muscle preservation
□ Sleep duration 7–9 hours nightly
□ Liver enzymes reviewed
□ Lp(a) measured at least once
□ Smoking avoided
□ Alcohol minimized
□ Visceral fat monitored
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Ketone Bodies Explained: Are They the Missing Link Between Fasting, Longevity, and Better Health? | DR T S DIDWAL
Hyperinsulinemia: The Silent Driver of Weight Gain, Diabetes & Heart Disease | DR T S DIDWAL
The Cardiometabolic Cascade: How Disease Starts—and How to Reverse It (2026 Science) | DR T S DIDWAL
Bone as an Endocrine Organ: Does Osteocalcin Influence Weight Regulation? | DR T S DIDWAL
The Metabolic Engine: Why Lower Body Strength Is Central to Fat Oxidation | DR T S DIDWAL
References
Chong, B., et al. (2025). The global syndemic of modifiable cardiovascular risk factors projected from 2025 to 2050. Journal of the American College of Cardiology, 86(3), 165–177. https://doi.org/10.1016/j.jacc.2025.04.061
Macvanin, M., & Klisic, A. (2026). Editorial: Molecular biomarkers of cardiometabolic disease – volume II. Frontiers in Endocrinology, 17, 1792935. https://doi.org/10.3389/fendo.2026.1792935
Rizo-Roca, D., Henderson, J. D., & Zierath, J. R. (2025). Metabolomics in cardiometabolic diseases: Key biomarkers and therapeutic implications for insulin resistance and diabetes. Journal of Internal Medicine, 297(3), 584–607. https://doi.org/10.1111/joim.13864
Singh, K., Mehrotra, A., Singh, S., & Singh, S. (2025). Exploring the topical formulation for management of diabetes wound healing: A review. International Journal of Pharmaceutical Sciences and Research, 16(7), 1804–1821. https://doi.org/10.13040/IJPSR.0975-8232.16(7).1804-21
Tahir, U. A., & Gerszten, R. E. (2023). Molecular biomarkers for cardiometabolic disease: Risk assessment in young individuals. Circulation Research, 132(12), 1663–1673. https://doi.org/10.1161/CIRCRESAHA.123.322000
Tan, C. Y. H., Koh, J. Y. J., Ang, W. W., Tan, X. M., Koh, S. W. C., Lin, W., Lee, J. W. K., & Chew, H. S. J. (2026). State-of-the-art digital phenotyping methods for cardiometabolic risk prevention and management: a scoping review. International Journal of Medical Informatics, 206, 106133. https://doi.org/10.1016/j.ijmedinf.2025.106133
Yang, H. S. (2025). Lipid biomarkers and cardiometabolic diseases: Critical knowledge gaps and future research directions. Metabolites, 15(2), 108. https://doi.org/10.3390/metabo15020108