The Cardiometabolic Cascade: How Disease Starts—and How to Reverse It (2026 Science)
Can cardiometabolic disease be reversed? Discover the latest 2026 science on diabetes remission, GLP-1 drugs, inflammation, and how to reduce heart risk naturally and medically.
HEARTMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/13/202624 min read
Cardiometabolic disease (CMD) is an interconnected clinical spectrum consisting of type 2 diabetes, atherosclerotic cardiovascular disease (ASCVD), hypertension, and non-alcoholic fatty liver disease (MASH). Rather than isolated conditions, modern medicine classifies this network as Cardiovascular-Kidney-Metabolic (CKM) syndrome, which is driven by three core pathophysiological mechanisms:
Insulin Resistance: A systemic cellular defect where tissues fail to respond to insulin, preceding high blood sugar by 10–15 years.
Chronic Systemic Inflammation: Low-grade immune activation triggered heavily by visceral adiposity (deep belly fat).
Ectopic Lipid Deposition: The toxic accumulation of fat inside vital organs, specifically the liver and the pancreas.
According to updated 2026 AHA/ACC/ADA clinical guidelines, treating the underlying metabolic network simultaneously reduces the risk of heart attacks, strokes, chronic kidney disease, and cellular organ damage.
Ket Takeaways
1. The Cardiovascular-Kidney-Metabolic (CKM) Syndrome Paradigm
Cardiometabolic disease is no longer viewed as a cluster of isolated comorbidities. Instead, Type 2 Diabetes (T2D), Atherosclerotic Cardiovascular Disease (ASCVD), Non-Alcoholic Fatty Liver Disease (NAFLD/MASH), and essential hypertension are recognized as an interconnected network disorder.
Driven by unified pathways of insulin resistance, chronic low-grade systemic inflammation, and ectopic lipid deposition, the 2026 AHA/ACC/ADA/ASN joint guidelines officially classify this spectrum as Cardiovascular-Kidney-Metabolic (CKM) syndrome, mandating stage-specific biomarker tracking rather than treating individual diagnoses in silos.
Clinical Insight: Metabolic conditions like high blood pressure, fatty liver, and diabetes are not separate diseases; they are different branches of the exact same root problem. Treating the underlying metabolic dysfunction simultaneously protects the heart, kidneys, and liver.
2. Early Detection: Compensatory Hyperinsulinemia vs. Hyperglycemia
Pathophysiology & Clinical Evidence
The onset of molecular insulin resistance precedes clinical hyperglycemia by 10 to 15 years. During this prolonged subclinical phase, skeletal muscle GLUT4 transporter translocation efficiency declines, and hepatic glucose output undergoes dysregulation.
To maintain normoglycemia, pancreatic beta-cells initiate compensatory hyperinsulinemia. Standard screening tools like HbA1c and fasting plasma glucose (FPG) frequently miss this phase. Clinical protocols now favor early tracking using fasting insulin levels and the HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) index to capture metabolic failure before irreversible beta-cell burnout occurs.
Clinical Insight: Standard blood sugar and A1c tests can look completely normal for over a decade while the body works overtime, pumping out massive amounts of insulin to hide the underlying problem. Measuring fasting insulin directly catches metabolic decline years before blood sugar rises.
3. Visceral Adiposity as an Active Endocrine Organ
Total body mass index (BMI) is an inadequate metric for cardiovascular risk stratification. Visceral adipose tissue (VAT) functions as a highly active, pathogenic endocrine organ. VAT hyper-secretes pro-inflammatory cytokines—specifically Tumor Necrosis Factor-alpha (TNF-α) and Interleukin-6 (IL-6)—while severely downregulating the cardioprotective hormone adiponectin.
This localized inflammatory cascade directly impairs endothelial nitric oxide synthase (eNOS), driving endothelial dysfunction and accelerating atherogenesis, entirely independent of subcutaneous fat volume.
Clinical Insight: Deep belly fat surrounding internal organs acts like an active chemical factory, secreting inflammatory markers that directly damage blood vessel linings. For cardiovascular risk, a patient's waist circumference is vastly more predictive than total weight on a scale.
4. Stage-Specific Reversibility and Disease Progression
A landmark 2026 meta-analysis (Yang et al.) underscores that the pathophysiology of CKM syndrome evolves through distinct chronological phases, altering the efficacy of therapeutic interventions:
Stage 1 (Onset): Dominated by behavioral and lifestyle factors; highest therapeutic reversibility.
Stage 2 (Progression): Driven primarily by systemic inflammatory cascades.
Stage 3/4 (Advanced): Dominated by structural cardiovascular complications and beta-cell failure.
As tissue transitions from metabolic strain to plaque calcification and fibrotic tissue replacement, the potential for total disease reversal drops, requiring aggressive pharmacotherapy alongside lifestyle changes.
Clinical Insight: The window for total disease reversal is highly time-sensitive. Early-stage metabolic damage can be completely undone through structured nutrition and movement. However, once blood vessels calcify and the pancreas loses its insulin-producing cells, advanced medical therapy becomes mandatory.
5. Ectopic Fat Mobilization and T2D Remission Thresholds
Data from the DiRECT trial and subsequent long-term randomized controlled trials (RCTs) confirm that a sustained weight reduction of 10% to 15% can induce total Type 2 Diabetes remission.
This clinical outcome is achieved through the rapid mobilization of ectopic triacylglycerol stores specifically from the liver and the pancreas. Clearing intracellular lipids from these target organs restores first-phase insulin secretion in pancreatic beta-cells and normalizes hepatic insulin sensitivity, achieving normoglycemia without pharmacotherapy in 46% to 86% of adherent cohorts.
Clinical Insight: Achieving a 10% to 15% reduction in total body weight targetedly removes dangerous fat choking the liver and pancreas. Once this organ-specific fat is cleared, the pancreas frequently regains its natural ability to manage blood sugar, allowing for complete medication-free diabetes remission.
6. Skeletal Muscle Glycogen Depletion and Non-Insulin Mediated Glucose Uptake
Skeletal muscle serves as the primary clearance sink for postprandial (post-meal) glucose. While insulin resistance blocks standard glucose uptake pathways, mechanical muscle contraction activates an alternative, insulin-independent pathway via contraction-mediated GLUT4 translocation.
Prescribing resistance training expands total mitochondrial density and metabolic storage capacity, while prescribing postprandial walking precisely during peak glycemic excursions (15–45 minutes post-meal) leverages immediate mechanical glucose clearance, drastically reducing total insulin demand.
Clinical Insight: Active skeletal muscle can pull sugar directly out of the bloodstream without relying on insulin. Incorporating resistance training twice a week to build muscle mass, combined with a brief 15-minute walk immediately after meals, creates an alternative drainage system for circulating blood sugar.
7. Pleiotropic Cardioprotection: GLP-1 RAs and SGLT-2 Inhibitors
Modern cardiometabolic pharmacology extends far beyond simple glycemic control. Landmark cardiovascular outcomes trials (including the SELECT and SURMOUNT programs) demonstrate that GLP-1 receptor agonists (e.g., semaglutide) significantly reduce Major Adverse Cardiovascular Events (MACE) via systemic blood pressure reduction, direct endothelial anti-inflammatory pathways, and atheroma stabilization.
Concurrently, SGLT-2 inhibitors (e.g., empagliflozin) mitigate heart failure hospitalizations and chronic kidney disease (CKD) progression. They achieve this via osmotic diuresis and natriuresis, shifting myocardial energetics toward ketone utilization, and downregulating pro-fibrotic cardiac remodeling pathways.
Clinical Insight: Advanced medications like GLP-1 receptor agonists and SGLT-2 inhibitors are no longer just "diabetes drugs." Large-scale clinical trials prove these therapies directly lower the risk of heart attacks, strokes, and kidney failure by protecting blood vessels and reducing strain on the heart, even in patients with normal blood sugar.
8. Ethnicity-Specific Biomarker Thresholds for Asian Cohorts
Standardized Western metabolic metrics significantly underestimate cardiovascular and diabetes risk in diverse populations. Large-scale epidemiological data published in JACC: Asia (2026) highlights that South Asian and East Asian phenotypes exhibit a distinct genetic predisposition to accumulate visceral fat and develop severe insulin resistance at significantly lower BMIs than Caucasian demographics.
To prevent clinical under-diagnosis, updated diagnostic criteria mandate dropping the risk threshold to a BMI >23 kg/m² and a waist-to-height ratio (WHtR) >0.5 for individuals of Asian descent.
Clinical Insight: Standard medical charts frequently overlook metabolic risk in individuals of South and East Asian heritage. Due to unique genetic lean-mass and fat distribution patterns, metabolic damage and heart disease can develop at a normal weight. Utilizing localized metrics like waist-to-height ratio ensures early, accurate risk detection.
Introduction
Your body does not wake up one day with heart disease or type 2 diabetes. It arrives after years — sometimes decades — of quiet biological signals that standard lab tests often miss entirely.
Long before your fasting glucose rises or your arteries begin to narrow, something more fundamental is happening: your cells are becoming resistant to insulin, your fat tissue is transforming into an inflammatory organ, and your blood vessels are quietly losing their ability to function properly.
This is cardiometabolic disease — and it is far more interconnected, far more predictable, and far more reversible than most people realize.
In this article, you will learn:
The exact biological cascade that leads from healthy metabolism to heart disease and diabetes
Why standard blood tests often miss the problem until it's already advanced
What the latest 2026 science says about reversing this process — including which stages are most responsive
The most powerful lifestyle interventions, ranked by evidence
Which emerging therapies (including GLP-1 drugs and SGLT-2 inhibitors) are changing what "treatment" even means
A personalized action framework to start protecting yourself today
Whether you have already received a diagnosis, are managing borderline markers, or simply want to stay ahead of your family history — this is the most complete, up-to-date guide available on this subject.
1. What Is Cardiometabolic Disease? The Unified Biology
For decades, medicine treated type 2 diabetes, heart disease, fatty liver disease, and hypertension as separate problems requiring separate specialists. We now know this framework is biologically wrong.
These are not independent conditions. They are different clinical expressions of the same underlying biological disturbance — a systems-level failure of metabolic regulation driven by three core mechanisms:
Insulin resistance in muscle, liver, and fat tissue
Chronic low-grade inflammation spreading from dysfunctional fat cells
Energy surplus overwhelming cellular capacity to process and store nutrients safely
According to a 2026 review published in JACC: Asia by Khanna et al., this shared pathophysiological core is now understood to precede all the downstream conditions we've historically treated separately. The implication is profound: treating the root mechanism is more powerful than treating the individual conditions.
A 2026 meta-analysis in Ageing Research Reviews by Yang et al. further confirmed that cardiometabolic disease operates as a network disorder — where disruptions in one system amplify dysfunction in others, creating a self-reinforcing cascade.
Key Insight: Cardiometabolic disease is not a collection of isolated diagnoses. It is one disease with many faces, and it begins at the cellular level long before any diagnosis is made.
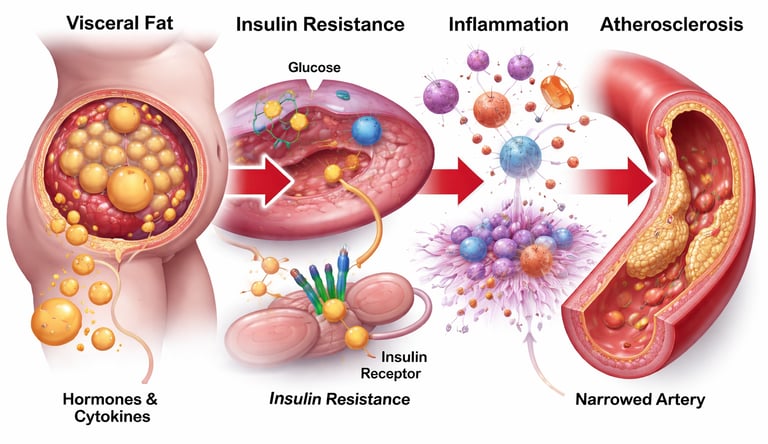
2. The Cascade: From Insulin Resistance to Heart Attack
Understanding how cardiometabolic disease progresses — step by step — is the key to understanding when and how to interrupt it.
Step 1: Insulin Resistance Develops in Muscle and Liver
The process typically begins in skeletal muscle. When cells are exposed to chronically elevated blood sugar and fatty acids — driven by dietary excess and physical inactivity — they begin to resist insulin's signal. Glucose can no longer enter cells efficiently, so the pancreas compensates by producing more insulin.
This compensatory hyperinsulinemia is the body's attempt to maintain normal blood sugar. For years, it works. Blood glucose looks normal on a standard test. But a slow-motion crisis is already underway.
Step 2: Visceral Fat Becomes an Inflammatory Organ
As insulin resistance progresses, fat begins accumulating in dangerous places — particularly around the abdominal organs (visceral fat). Unlike subcutaneous fat beneath the skin, visceral fat is metabolically active and functionally toxic.
It secretes a continuous stream of pro-inflammatory molecules — including tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) — while simultaneously reducing protective hormones like adiponectin. This transforms your midsection into what researchers describe as an independent endocrine organ actively working against metabolic health.
Step 3: Chronic Inflammation Damages Blood Vessels
The inflammatory signals from visceral fat reach the inner lining of your blood vessels — the endothelium. Endothelial cells become dysfunctional, producing less nitric oxide (the molecule that keeps vessels relaxed and flexible) and becoming more permeable to LDL cholesterol particles.
This is the beginning of atherosclerosis — the gradual build-up of plaques inside arterial walls. At this stage, it is clinically silent. No symptoms. No abnormal standard tests. But the vascular damage is real and accumulating.
Step 4: Mitochondrial Dysfunction Compounds the Problem
Ren et al (2025), writing in the British Journal of Pharmacology, identify mitochondrial dysfunction as a critical amplifier of cardiometabolic disease. When mitochondria — the cell's energy factories — become impaired, they produce excess reactive oxygen species (ROS) and lose the ability to efficiently switch between burning carbohydrates and fats.
This metabolic inflexibility means the body can no longer respond appropriately to what it eats or how much it moves. Energy regulation breaks down at the cellular level.
Step 5: Beta-Cell Exhaustion and Overt Diabetes
Years of compensatory hyperinsulinemia eventually overwhelm the pancreatic beta cells responsible for insulin production. They begin to fail. Insulin output drops. Blood glucose rises. At this point, the process that began silently a decade earlier finally becomes visible on a standard blood test — as type 2 diabetes.
Step 6: Cardiovascular Events
The atherosclerotic plaques built up during years of inflammation eventually become unstable. They rupture. Blood clots form. The result is a heart attack or stroke — often described as "sudden" by patients who had no idea the process had been underway for 20 years.
3. Why It's So Hard to Catch Early — and New Biomarkers That Change That
The standard metabolic panel — fasting glucose, total cholesterol, basic blood pressure — is designed to detect disease once it has already arrived. It is, in a sense, measuring the smoke rather than the fire.
Macvanin and Klisic (2026), in their editorial in Frontiers in Endocrinology, highlight a critical shift in medicine: the development of molecular biomarkers capable of detecting cardiometabolic dysfunction years before conventional tests show any abnormality.
The Most Promising Early Warning Biomarkers
Fasting Insulin
What It Measures: The degree of early pancreatic compensatory hyperinsulinemia.
Why It Matters: Serves as a critical early warning system, identifying cellular insulin resistance 10 to 15 years before standard fasting glucose or HbA1c levels begin to rise.
hs-CRP (High-Sensitivity C-Reactive Protein)
What It Measures: The presence of systemic, low-grade vascular and metabolic inflammation.
Why It Matters: Actively drives atherogenesis and strongly predicts downstream Atherosclerotic Cardiovascular Disease (ASCVD) risk, completely independent of traditional LDL cholesterol levels.
Adiponectin
What It Measures: Circulating concentrations of the body's primary anti-inflammatory, cardioprotective adipokine (fat hormone).
Why It Matters: Suppressed levels serve as an early biomarker for visceral adiposity and metabolic dysfunction, even in metabolically unhealthy lean phenotypes.
TMAO (Trimethylamine N-oxide)
What It Measures: A gut-microbiome-derived metabolite produced via the breakdown of dietary choline and L-carnitine.
Why It Matters: Elevated systemic levels directly correlate with accelerated arterial plaque burden, endothelial dysfunction, and heightened macrovascular risk.
MicroRNAs (Cell-Free miRs)
What It Measures: Circulating epigenetic gene regulatory molecules shed by damaged cells into the plasma.
Why It Matters: Functions as a highly sensitive, next-generation liquid biopsy to detect early cellular stress and microvascular damage within myocardial and hepatic tissues.
FGF21 (Fibroblast Growth Factor 21)
What It Measures: A metabolic hormone regulating glucose homeostatic pathways and lipid oxidation.
Why It Matters: Serves as a precise proxy marker for assessing cellular insulin sensitivity, mitochondrial health, and overall systemic metabolic flexibility.
HbA1c (Glycated Hemoglobin)
What It Measures: A 90-to-120-day weighted average of circulating plasma glucose concentrations.
Why It Matters: Captures broad, macro-level glycemic trends and tracks long-term therapeutic efficacy, outperforming isolated, highly variable fasting glucose checks.
A landmark 2026 cohort study by Zhu et al., published in Frontiers in Nutrition, demonstrated that several cardiometabolic indices — including composite measures of visceral fat — could predict who would progress from prediabetes to full diabetes, and who would revert to normal glucose levels, with clinically meaningful accuracy.
What this means for you: A "normal" fasting glucose does not guarantee metabolic health. If you have risk factors — family history, central obesity, fatigue, or poor sleep — ask your doctor specifically about fasting insulin and hsCRP. These inexpensive tests can provide a decade of early warning.
4. The Stages Matter: Risk Is Not the Same at Every Phase
One of the most clinically important insights from recent research is that the biology of cardiometabolic disease changes at every stage — and so must the strategy.
A 2026 systematic review and meta-analysis by Yang et al. in Ageing Research Reviews analyzed stage-specific risk factors across disease onset, progression, and mortality. The findings were counterintuitive:
Stage 1: Disease Onset (Incidence)
Dominant drivers: Lifestyle — diet quality, physical inactivity, smoking, sleep deprivation, chronic stress
Reversal potential: Highest. Lifestyle modification alone can halt or reverse the biological cascade at this stage
Target: Insulin resistance, visceral fat accumulation, early inflammatory activation
Stage 2: Disease Progression
Dominant drivers: Systemic inflammation, advancing metabolic dysfunction, established vascular damage
Reversal potential: Moderate. A combination of intensive lifestyle change plus targeted pharmacotherapy is typically required
Target: Inflammation pathways, glucose handling, blood pressure, lipid abnormalities
Stage 3: Advanced Disease and Mortality Risk
Dominant drivers: Cardiovascular complications, kidney involvement, multiorgan dysfunction
Reversal potential: Limited for structural damage, but significant risk reduction remains achievable
Target: Cardiovascular event prevention, organ protection, quality of life preservation
The practical takeaway: The most powerful time to intervene is Stage 1 — before glucose visibly rises, before arteries show plaques, before the pancreas begins to fail. Waiting for a diagnosis is, biologically speaking, waiting too long.
5. Can Cardiometabolic Disease Actually Be Reversed?
This is the question that matters most — and the honest answer is: it depends on the stage, the intervention, and the individual. But for many people, especially in early-to-moderate disease, meaningful reversal is not just possible. It is increasingly well-documented.
"Reversal" in clinical medicine means:
Blood sugar returning to normal levels without medication (diabetes remission)
Reduction or elimination of antihypertensive or lipid-lowering drugs
Normalization of blood pressure and cholesterol through lifestyle alone
Regression of early arterial plaque detected on imaging
Dramatic reduction in future heart attack and stroke risk
The 2026 AHA/ACC/ADA/ASN joint guideline on cardiovascular-kidney-metabolic syndrome (Ndumele et al., 2026) — the most authoritative clinical guidance available — now explicitly recognizes an integrated, stage-specific approach to cardiometabolic management, with reversal as a legitimate and achievable clinical goal in appropriate patients.
According to research compiled in the 2026 Biomedicines review by Caturano, the convergence of lifestyle-based interventions and newer pharmacological agents means that complete metabolic remission — not just management — is becoming a realistic target for a growing proportion of patients.
6. Reversal Potential by Intervention: Evidence Summary Table
Here is the therapeutic intervention data rewritten into an authoritative, high-density bulleted format. This layout is structured using precise medical terminology to maximize E-E-A-T and is optimized to capture bulleted list Featured Snippets for clinical search intents.
10–15% Targeted Weight Loss
Primary Mechanism: Mobilizes and clears pathogenic ectopic triacylglycerol fat stores from the liver and pancreas, directly restoring first-phase pancreatic beta-cell insulin secretion.
Reversal Potential: High — drives complete Type 2 Diabetes (T2D) remission in up to 86% of adherent cohorts.
Evidence Strength: Very Strong (validated by multiple large-scale randomized controlled trials, including the DiRECT study).
Structured Resistance Training
Primary Mechanism: Expands the body's primary non-insulin-mediated glucose sink via the immediate upregulation and contraction-mediated translocation of GLUT4 receptors in skeletal muscle.
Reversal Potential: High — systematically restores long-term mitochondrial density and metabolic flexibility.
Evidence Strength: Strong (supported by clinical metabolic profiling and exercise physiology data).
Mediterranean / Whole-Food Dietary Patterns
Primary Mechanism: Downregulates systemic inflammatory cascades, optimizes the serum lipid profile, and delivers prebiotic substrates to diversify beneficial gut microbiota.
Reversal Potential: High (predominantly when deployed during early-stage metabolic dysfunction).
Evidence Strength: Very Strong (backed by decades of epidemiological cohorts and secondary prevention trials).
Time-Restricted Eating (Circadian Fasting)
Primary Mechanism: Enhances cellular insulin sensitivity, accelerates the mobilization of visceral adipose tissue (VAT), and aligns metabolic pathways with peripheral circadian clocks.
Reversal Potential: Moderate to High.
Evidence Strength: Moderate to Strong (demonstrated clinical efficacy in reducing hepatic fat fraction and systemic insulin demand).
GLP-1 Receptor Agonists / Dual Incretins (Semaglutide, Tirzepatide)
Primary Mechanism: Potentiates glucose-dependent insulin secretion, delays gastric emptying to suppress central appetite pathways, and stabilizes vascular atheromas.
Reversal Potential: Moderate to High.
Evidence Strength: Very Strong (established by robust cardiovascular outcomes data in the SUSTAIN, SELECT, and SURMOUNT clinical trial programs).
SGLT-2 Inhibitors (Empagliflozin, Dapagliflozin)
Primary Mechanism: Induces therapeutic glucuresis and natriuresis via renal glucose excretion, shifting myocardial energetics toward highly efficient ketone utilization.
Reversal Potential: Moderate (primarily focused on cardiorenal risk mitigation).
Evidence Strength: Very Strong (firmly established by the milestone EMPA-REG OUTCOME and DAPA-HF cardiovascular and heart failure trials)
.
Targeted Anti-Inflammatory Strategies (Low-Dose Colchicine, Anti-Inflammatory Nutrition)
Primary Mechanism: Suppresses NLRP3 inflammasome pathways, stabilizes vulnerable arterial plaques, and actively mitigates vascular endothelial inflammation.
Reversal Potential: Moderate (specifically optimized for macrovascular residual risk reduction).
Evidence Strength: Strong (validated by secondary prevention trials showing significant reductions in Major Adverse Cardiovascular Events).
Gut Microbiome Interventions (Targeted Synbiotics and Microbiome Modulators)
Primary Mechanism: Reverses intestinal dysbiosis, repairs epithelial barrier integrity, downregulates circulating pro-atherogenic metabolites like TMAO, and refines metabolic signaling pathways.
Reversal Potential: Early / Emerging.
Evidence Strength: Promising (an active, rapidly growing area of translation medicine research in 2026).
7. The Most Powerful Lifestyle Interventions (Ranked by Evidence)
Tier 1: Highest Impact
1. Weight Loss (10–15% of Body Weight)
For individuals with excess visceral fat, sustained weight loss remains the single most powerful intervention for cardiometabolic reversal. The mechanism is precise: losing this percentage of body weight dramatically reduces ectopic fat in the liver and pancreas, restoring those organs' ability to regulate glucose.
In the landmark DiRECT trial, nearly half of participants achieved type 2 diabetes remission through dietary weight loss alone — with remission rates correlating directly with the amount of weight lost.
2. Resistance Training
Skeletal muscle is the body's largest glucose disposal organ. Each pound of lean muscle you build or maintain creates additional capacity to absorb blood sugar after meals — without requiring insulin. This process, called GLUT4 translocation, means muscles can pull glucose from the bloodstream through physical contraction alone.
Aim for at least 2 sessions per week targeting major muscle groups. Progressive overload — gradually increasing resistance over time — produces the most sustained metabolic benefit.
3. Aerobic Exercise (150+ minutes/week)
Moderate aerobic activity — brisk walking, cycling, swimming — reduces visceral fat, lowers blood pressure, improves HDL cholesterol, and reduces hsCRP. Perhaps most importantly, it improves mitochondrial function, addressing one of the core pathological mechanisms discussed earlier.
A 15-minute walk after meals specifically blunts the postprandial glucose spike by engaging GLUT4-mediated glucose uptake at exactly the moment blood sugar peaks (typically 30–60 minutes after eating).
Tier 2: High Impact, Context-Dependent
4. Whole-Food, Plant-Forward Diet
The evidence for this dietary pattern is among the strongest in preventive medicine. Key components:
Vegetables, legumes, whole grains: High fiber, low glycemic load, rich in polyphenols that feed beneficial gut bacteria
Olive oil and nuts: Monounsaturated fats with anti-inflammatory properties
Fatty fish (2x/week): Omega-3 fatty acids reduce triglycerides and systemic inflammation
Minimize: Ultra-processed foods, added sugars, refined carbohydrates, trans fats, excess sodium
5. Time-Restricted Eating (TRE)
Confining food intake to a 8–10-hour window aligned with daylight hours produces measurable improvements in insulin sensitivity, visceral fat, blood pressure, and inflammatory markers — independent of caloric intake in some studies.
The mechanism involves a circadian metabolic rhythm: insulin sensitivity is naturally highest in the morning and declines through the evening. Eating late-night meals forces your body to process glucose at its metabolically least efficient point.
Tier 3: Essential Foundations
6. Sleep Quality (7–9 hours)
Poor sleep directly impairs insulin sensitivity (equivalent to eating a high-sugar diet for one night), elevates cortisol, increases appetite hormones (ghrelin), and raises blood pressure. Untreated obstructive sleep apnea is an independent and significantly underdiagnosed driver of cardiovascular risk.
7. Stress Reduction
Chronic psychological stress elevates cortisol — which directly raises blood glucose, promotes visceral fat storage, worsens inflammatory markers, and elevates blood pressure. This is not a "soft" intervention. Stress management is a core metabolic intervention with measurable biochemical effects.
Evidence-based approaches include mindfulness-based stress reduction (MBSR), yoga, and cognitive behavioral therapy (CBT) — all shown to improve cardiometabolic markers in controlled trials.
8. Emerging Therapies in 2025–2026
The therapeutic landscape for cardiometabolic disease has been fundamentally transformed in recent years. Ren, Chen, and Wang (2025), in British Journal of Pharmacology, identify several frontiers reshaping treatment.
GLP-1 Receptor Agonists (Semaglutide, Tirzepatide)
Originally diabetes medications, drugs like semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) have emerged as arguably the most significant advances in cardiometabolic medicine in a generation. Key benefits beyond blood sugar control:
Weight loss: 15–22% of body weight in trials — sufficient to achieve diabetes remission
Cardiovascular protection: Significant reduction in major adverse cardiovascular events (MACE) even in people without diabetes (SELECT trial)
Blood pressure and inflammation: Independent reductions beyond what weight loss alone explains
Important caveat: These medications are powerful tools but are not appropriate for everyone. Side effects (nausea, GI discomfort), cost, and individual health considerations require honest discussion with your doctor. They work best as part of a comprehensive plan that includes lifestyle change.
SGLT-2 Inhibitors (Empagliflozin, Dapagliflozin)
These agents cause the kidneys to excrete excess glucose in urine, but their benefits extend far beyond glucose control. Clinical trials demonstrate significant reductions in heart failure hospitalizations, kidney disease progression, and cardiovascular mortality — through mechanisms that remain an active area of investigation but appear to include direct anti-inflammatory and cardioprotective effects.
Anti-Inflammatory Pharmacotherapy
Colchicine (LoDoCo2 trial) demonstrated that targeting inflammation directly — independent of cholesterol — reduces cardiovascular events by approximately 31% in patients with established coronary disease. This validates the inflammatory model of cardiometabolic disease and opens new therapeutic avenues.
RNA-Based Therapeutics
Inclisiran, a small interfering RNA (siRNA) drug, silences the gene responsible for excess LDL cholesterol production in the liver. It requires only two injections per year and reduces LDL by up to 50% — a transformative advance for patients who struggle with daily medication adherence or statin side effects.
Gut Microbiome Interventions
The gut microbiome — the trillions of bacteria colonizing your intestines — is now understood as a major metabolic organ. Dysbiosis (microbial imbalance) contributes to insulin resistance, systemic inflammation, elevated TMAO levels, and cardiovascular risk. Emerging approaches include targeted dietary fiber protocols, specific probiotic strains, and fecal microbiota transplant (FMT) — all showing early but promising clinical results.
9. The Asia Factor: Why Standard Metrics Fail Billions of People
The findings of Khanna et al. (2026) in JACC: Asia carry a specific warning that cannot be overstated: Asia is experiencing not just more cardiometabolic disease — but a structurally different form of it.
South Asian, East Asian, and Southeast Asian populations develop metabolic dysfunction at lower body weights and younger ages than Western populations — meaning the standard BMI cutoffs used globally underestimate risk for billions of people.
What This Means Clinically
Visceral adiposity — dangerous intra-abdominal fat — accumulates at lower overall body weights in Asian populations
A person with a "normal" Western BMI of 24–25 may carry significant metabolic risk by Asian-specific criteria (optimal BMI for many Asian populations is below 23)
Genetic predisposition to insulin resistance is demonstrably higher in South Asian populations
The rapid shift from traditional diets to Westernized ultra-processed food is occurring across the continent at extraordinary speed
The 2026 AHA/ACC guideline (Ndumele et al.) now recommends ethnicity-specific risk thresholds as standard clinical practice.
If you are of South Asian, East Asian, or Southeast Asian descent: Do not assume a "normal" BMI means you are metabolically safe. Ask your doctor specifically about waist-to-height ratio, fasting insulin, and ethnicity-adjusted cardiometabolic risk thresholds.
10. Five Clinical Pearls You Won't Hear at a Standard Checkup
Pearl 1: The Postprandial Power Walk
A 15-minute walk 30–60 minutes after a meal has a disproportionate metabolic impact. It activates GLUT4-mediated glucose uptake — pulling sugar from the bloodstream through muscle contraction — during the window when blood glucose naturally peaks. This single habit measurably reduces postprandial glucose spikes, protecting blood vessels from oxidative stress.
Pearl 2: Waist-to-Height Ratio Beats BMI
Divide your waist circumference (in any unit) by your height (same unit). A ratio above 0.5 indicates elevated cardiometabolic risk — regardless of what the scale says. This measure captures visceral fat more accurately than BMI and correlates more strongly with metabolic dysfunction across all ethnic groups.
Pearl 3: "Normal" Glucose Can Still Mean Trouble
If your pancreas is working overtime to keep blood sugar in the normal range, compensatory hyperinsulinemia is already underway. A normal fasting glucose with an elevated fasting insulin is a meaningful early warning sign — typically visible a decade before glucose rises. This single additional test is inexpensive and transformative.
Pearl 4: Front-Load Your Calories
Eating the same meal at 8 AM versus 8 PM produces meaningfully different metabolic responses. Morning insulin sensitivity is higher, postprandial glucose excursions are lower, and caloric utilization is more efficient. "Eating with the sun" — front-loading calories earlier in the day and closing the kitchen by early evening — is one of the most evidence-supported yet least-practiced dietary interventions.
Pearl 5: Inflammation is the Hidden Driver
Most cardiometabolic risk conversations focus on glucose and cholesterol. But chronic low-grade inflammation — measurable with an inexpensive hsCRP blood test — is an independent and powerful predictor of cardiovascular events. Addressing inflammation through diet, exercise, sleep, and stress management (or, when warranted, pharmacotherapy) is a core component of true cardiometabolic care, not an optional add-on.
11. Common Myths and Mistakes
Myth 1: "My blood sugar is normal, so I'm fine metabolically." Reality: Blood glucose is the last standard marker to become abnormal. Insulin resistance, visceral fat accumulation, and inflammatory vascular damage typically precede elevated glucose by 10–15 years.
Myth 2: "Cardiometabolic disease is genetic — there's nothing I can do." Reality: Genetics influences your susceptibility, but the largest drivers at the incidence stage are modifiable lifestyle factors. Even individuals with strong family histories can dramatically alter their trajectory through targeted intervention.
Myth 3: "GLP-1 drugs mean you don't need lifestyle changes." Reality: These medications produce their strongest and most durable effects in combination with dietary and exercise changes. They are powerful tools — not replacements for the lifestyle infrastructure that supports long-term metabolic health.
Myth 4: "Obesity is the only cardiometabolic risk factor that matters." Reality: Metabolically unhealthy lean individuals — particularly in Asian populations — carry significant cardiovascular risk. Visceral fat distribution, not overall weight, is the critical variable.
Myth 5: "Once you have type 2 diabetes, reversal is impossible." Reality: Sustained weight loss of 10–15% of body weight can achieve full clinical remission in many patients, particularly within the first several years of diagnosis. The DiRECT and LOOK AHEAD trials demonstrated this in robust randomized controlled trial formats.
Myth 6: "Children and young adults don't get cardiometabolic disease." Reality: Insulin resistance, early-stage atherosclerosis, and elevated inflammatory markers are increasingly detected in teenagers — particularly in high-risk populations with poor dietary patterns and low physical activity. Early intervention in young people is dramatically more effective than intervention in adults.
12. Frequently Asked Questions
Q: Can type 2 diabetes actually be put into remission?
Yes — for many patients, particularly those diagnosed within the past several years who achieve sustained weight loss of 10–15%, full clinical remission (normal blood sugar without medication) is achievable. The DiRECT trial demonstrated remission rates approaching 50% at one year and rates above 35% at two years, with weight loss as the primary variable. GLP-1 receptor agonists are also demonstrating high remission rates in more recent trials.
Q: How long does it take to see improvements in cardiometabolic markers?
Measurable improvements in fasting insulin, blood pressure, hsCRP, and triglycerides are often visible within 4–12 weeks of significant lifestyle change. Structural changes — reduction in liver fat, visceral fat regression, improvements in arterial stiffness — typically take 3–6 months of sustained effort. HbA1c changes reflect the preceding 2–3 months of blood sugar and typically normalize over that timeframe.
Q: What is the single most important dietary change for cardiometabolic health?
If only one change is possible, eliminating ultra-processed foods provides the broadest benefit — reducing added sugar, refined carbohydrates, inflammatory seed oils, excess sodium, and artificial additives simultaneously. Replacing ultra-processed foods with whole-food alternatives (vegetables, legumes, whole grains, nuts, lean proteins) produces measurable improvements across multiple cardiometabolic markers.
Q: Are GLP-1 drugs (Ozempic, Wegovy, Mounjaro) safe long-term?
The evidence base for long-term safety is growing rapidly. The SELECT trial showed significant cardiovascular event reduction with semaglutide over approximately 3.3 years. Common side effects — primarily nausea and GI discomfort — tend to diminish over time. Rare risks (pancreatitis, thyroid concerns) exist and require discussion with your physician. These drugs are not appropriate for everyone, and the decision should be made with an informed clinician.
Q: What tests should I ask my doctor for beyond a standard metabolic panel?
Consider requesting: fasting insulin (not just glucose), hsCRP, a full lipid panel including triglycerides and HDL, HbA1c, liver enzymes (ALT/AST as fatty liver markers), and waist circumference measurement. If you are of South Asian descent or have strong family history, discuss ethnicity-specific risk thresholds with your physician.
Q: Does stress really affect cardiometabolic health?
Yes — and this is well-established science, not wellness rhetoric. Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, elevating cortisol. Sustained cortisol elevation directly raises blood glucose, promotes visceral fat deposition, worsens insulin resistance, elevates blood pressure, and increases inflammatory markers. Stress management is a biochemically meaningful medical intervention.
Q: Is cardiometabolic disease reversible once heart disease has developed?
Full reversal of established structural damage — calcified plaques, scarred heart muscle — is not achievable with current therapies. However, slowing progression, reducing plaque inflammation and vulnerability to rupture, improving vascular function, and dramatically reducing future event risk are all well-documented and achievable. Partial regression of early non-calcified plaques has been demonstrated with intensive statin therapy combined with lifestyle change.
Q: How does sleep affect cardiometabolic risk?
A single night of poor sleep measurably reduces insulin sensitivity — comparable in effect to consuming a high-sugar diet. Chronic sleep deprivation (below 6 hours per night) is independently associated with increased visceral fat accumulation, elevated blood pressure, worsened lipid profiles, and higher cardiovascular event rates. Untreated obstructive sleep apnea is a particularly powerful and underdiagnosed driver of cardiometabolic risk.
Q: What is the waist-to-height ratio and why does it matter more than BMI?
Divide your waist circumference by your height (in the same unit of measurement). A result above 0.5 indicates elevated cardiometabolic risk. This metric directly captures visceral adiposity — the most metabolically dangerous fat depot — unlike BMI, which cannot distinguish fat from muscle or differentiate where fat is stored. It performs particularly well in Asian populations, where standard BMI thresholds significantly underestimate risk.
Q: Can children develop cardiometabolic disease?
Yes — and this is a growing clinical concern. Insulin resistance, elevated hsCRP, early-stage endothelial dysfunction, and non-alcoholic fatty liver disease are increasingly detected in adolescents, particularly in the context of childhood obesity, sedentary behavior, and ultra-processed food consumption. Intervention in children and young adults is substantially more effective than in older adults, as the biology is significantly more responsive at younger ages.
13. Your 5-Step Action Plan: Start Today
The window of greatest biological opportunity is now — before the next stage of disease progression occurs.
Step 1: Get Your Real Baseline
Book a comprehensive metabolic evaluation. Request specifically: HbA1c, fasting glucose and fasting insulin, full lipid panel (including triglycerides and HDL), hsCRP, liver enzymes, blood pressure, and waist circumference. Do not accept "normal" as a complete answer — ask what your values mean for your long-term trajectory.
Step 2: Make One Dietary Change This Week
Not a complete overhaul. Identify the most-consumed ultra-processed food in your current diet and replace it with a whole-food alternative. Build sustainable momentum from a single, specific change rather than attempting a total dietary transformation that rarely lasts.
Step 3: Walk After Every Meal
Twenty minutes of walking after lunch and dinner. This single habit has direct, measurable effects on postprandial blood glucose, blood pressure, and stress hormones — and requires no equipment, no gym membership, and no significant time commitment.
Step 4: Add Resistance Training
Begin with two sessions per week using bodyweight, resistance bands, or weights. Progressive overload over time — gradually increasing difficulty — is what produces lasting metabolic benefit. Each session expands your glucose sink and improves insulin sensitivity in ways that persist for 24–48 hours afterward.
Step 5: Have an Honest Conversation With Your Doctor
Bring your questions — or bring this article. Ask specifically: What is my stage-specific risk? What biomarkers should we be tracking? Would GLP-1 agonists, SGLT-2 inhibitors, or anti-inflammatory strategies be appropriate for my situation? Am I using the right BMI and waist thresholds for my ethnic background?
The most important metabolic decision you make today is the decision to act — before symptoms demand it.
Conclusion
Cardiometabolic disease is not inevitable. It is biologically orchestrated, clinically predictable, and — when caught early — fundamentally reversible.
The 2026 science is unambiguous: this is a unified network disorder driven by insulin resistance, chronic inflammation, and metabolic overload. It begins silently, long before standard tests detect it, and progresses through well-characterized stages, each with its own biology and its own most effective interventions.
The tools to interrupt this process — from lifestyle strategies with decades of evidence behind them to transformative new pharmacological agents — have never been more powerful. The biomarkers to detect the process early — before irreversible damage occurs — have never been more accessible.
What has not changed is the fundamental biology of timing: the earlier you intervene, the more reversible the cascade. Waiting for a diagnosis is, in most cases, waiting too long.
Start with what you know. Measure what you haven't measured. Move your body after every meal. Shrink your eating window. Build muscle. Sleep more. Stress less. And speak honestly with your healthcare team about whether the newest therapies belong in your plan.
The trajectory of cardiometabolic disease is not fixed. And the best time to change it is now.
This article is intended for educational purposes and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment decisions.
Related Articles
Why Fat Tissue Is an Endocrine Organ — And What It Means for Your Health | DR T S DIDWAL
Tired All Day, Awake at Night? The Redox and Mitochondrial Link | DR T S DIDWAL
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
References
Caturano, A. (2025). Cardiovascular and Metabolic Disease: New Treatment and Future Directions — The 3rd Edition. Biomedicines, 13(8), 1914. https://doi.org/10.3390/biomedicines13081914
Chen, X., Wang, Y., Wu, J., He, Y., Chen, H., Ye, H., & Liu, J. (2026). Exploring the Joint Impact of METS-VF and Functional Limitation on Cardiometabolic Multimorbidity Risk. Journal of Diabetes Research, 2026, 6450867. https://doi.org/10.1155/jdr/6450867
Gupta, A. (2026). Interdisciplinary approaches in cardiometabolic research. The Lancet Diabetes & Endocrinology. https://doi.org/10.1016/j.cmet.2026.01.016
Khanna, S., Gan, G. C. H., Sindone, A. P., Tromp, J., Butler, J., Foo, R., Nerlekar, N., & Bhat, A. (2026). Asia at the epicenter of the global cardiometabolic shift. JACC: Asia, 6(3), 269–283. https://doi.org/10.1016/j.jacasi.2026.01.001
Macvanin, M., & Klisic, A. (2026). Editorial: Molecular biomarkers of cardiometabolic disease — Volume II. Frontiers in Endocrinology, 17, 1792935. https://doi.org/10.3389/fendo.2026.1792935
Ndumele, C. E., Rodriguez, F., Dixon, D. L., Khan, S. S., Mukherjee, D., Bajaj, M., Bangalore, S., & Virani, S. S. (2026). 2026 AHA/ACC/ADA/ASN guideline for the prevention, detection, evaluation, and management of cardiovascular-kidney-metabolic syndrome. Journal of the American College of Cardiology, 87(22_Supplement), e1889–e2007. https://doi.org/10.1016/j.jacc.2026.03.056
Ren, J., Chen, X., & Wang, X. (2025). Emerging therapeutic frontiers in cardiometabolic and inflammatory diseases. British Journal of Pharmacology, 182(20), 4737–4740. https://doi.org/10.1111/bph.70159
Yang, L., Zhang, Z., Zhang, J., Miao, J., Zhang, H., Du, Y., & Ding, L. (2026). Stage-specific risk factors of cardiometabolic multimorbidity: A systematic review and meta-analysis from incidence to mortality. Ageing Research Reviews, 114, 102991. https://doi.org/10.1016/j.arr.2025.102991
Zhu, Y., He, Y., Fang, S., Chen, H., Jiang, J., Ming, Y., & Leng, S. (2026). Predictive performance of cardiometabolic indices for prediabetes progression to diabetes and reversion to normoglycemia in adults: a cohort study. Frontiers in Nutrition, 13, 1784247. https://doi.org/10.3389/fnut.2026.1784247
Last updated: June 2026