The Science of Strength Training: How Building Muscle Improves Fat Loss, Heart Health, and Longevity
Discover how strength training improves muscle mass, blood sugar control, cardiovascular health, bone density, and healthy aging—backed by the latest scientific research.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/19/202624 min read
Strength training is any exercise in which your muscles work against resistance to build strength, muscle mass, and resilience. Doing just 60 minutes per week is linked to a 15% lower risk of all-cause mortality, as well as improved blood pressure, blood sugar, and bone density.
Strength training benefits:
Live longer: ∼60 min/week linked to 15% lower all-cause mortality risk
Heart health: Lowers blood pressure 3–6 mmHg
Blood sugar: Improves insulin sensitivity
Bone health: Stimulates bone growth
Works at any age: Reverses muscle loss even in your 80s–90s
Key takeaways
1. How Much Strength Training Do You Actually Need?
The Quick Answer: Just 60 minutes per week.
You don't need to live in the gym to see massive health improvements. Research shows that just 60 minutes of strength training per week is linked to a significantly lower risk of early death from heart disease, cancer, and other chronic conditions. Breaking this down into two 30-minute sessions is highly effective. While more volume can increase muscle size, consistency is far more important than marathon workouts.
2. Neuromuscular Adaptation: Why You Feel Stronger Before Seeing Muscle Growth
If you’ve been working out for a month and don't see changes in the mirror, don't quit. During the first 1 to 6 weeks of a new routine, your brain is learning how to recruit muscle fibers more efficiently. This process, known as neuromuscular adaptation, makes you stronger before any visible muscle growth occurs. Hypertrophy (visible muscle growth) typically takes 6 to 8+ weeks of consistent training.
3. Strength Training vs. Weight Training: What’s the Difference?
Many people use these terms interchangeably, but they aren't the exact same thing:
Strength Training: The broad umbrella term for any exercise that challenges your muscles against resistance to build strength and endurance.
Weight Training: A specific type of strength training that utilizes external loads like dumbbells, barbells, or gym machines.
If you don't have access to a gym, bodyweight exercises (calisthenics) like push-ups, squats, and chair stands build real, functional strength.
4. The Law of Progressive Overload
To continually improve your fitness and build muscle, you must apply the principle of progressive overload. This means gradually increasing the demands placed on your musculoskeletal system over time. If you lift the exact same weight for the exact same repetitions every week, your body will stop adapting.
How to apply it: When an exercise starts to feel easy, increase the weight, add more repetitions, or choose a harder variation by roughly 5% to 10%.
5. Daily Protein Intake: How Much Do You Really Need?
While protein is essential for muscle repair and growth, there is a point of diminishing returns.
The Sweet Spot: For most active adults, 1.6 grams of protein per kilogram of body weight (approx. 0.73g per pound) per day is where the muscle-building benefits level off.
The Math: For a 70kg (154lb) individual, that equates to roughly 112 grams of protein per day.
Consuming more than this isn't harmful if you have healthy kidneys, but clinical studies show it provides little to no extra muscle-building benefit.
6. Myth Busting: Muscle Soreness (DOMS) Does Not Equal Success
Delayed Onset Muscle Soreness (DOMS) simply means your body performed an activity it isn't used to—it is not an accurate indicator of a good workout. You can have an incredibly effective, muscle-building session and feel zero soreness the next day. Do not use pain as your primary scorecard for progress.
7. The Ultimate Anti-Aging Medicine
After the age of 30, adults naturally begin to lose muscle mass and bone density—a condition known as sarcopenia. Strength training is one of the only proven ways to halt and reverse this process, even for individuals in their 80s and 90s. The ultimate goal of functional strength training isn't just aesthetics; it’s preserving the ability to get off the floor, carry groceries, prevent falls, and maintain independence.
8. Managing Chronic Disease with Resistance Training
Strength training acts as medicine for your cardiovascular and metabolic health. Consistent resistance training can:
Lower resting blood pressure by 3 to 6 points.
Improve insulin sensitivity by helping muscles pull glucose directly from the bloodstream.
Increase bone mineral density to fight off osteopenia and osteoporosis.
While it shouldn’t replace prescribed medical treatments, it serves as a powerful lifestyle intervention alongside them.
ntroduction
If you've ever wondered whether strength training is "worth it" compared to cardio, whether lifting three times a week is actually enough, or whether the supplement aisle is selling you something the data doesn't support — this guide is built to answer that, with the studies shown, not just cited.
Strength training (also called resistance training) is the practice of making your muscles work against an external load — a barbell, a band, your own bodyweight, or gravity — to build force-production capacity, muscle tissue, and the physiological resilience that comes with both. What separates this guide from most fitness content online is not the topic — it's the standard of evidence. Wherever a claim is made, you'll see the actual effect size, the confidence interval, and what that number does and doesn't tell us. Clinical relevance matters more than statistical significance, and we'll flag the difference every time it comes up.
By the end of this guide, you'll understand:
What's actually happening in your muscles and nervous system during resistance training
The real, quantified health outcomes — mortality risk, blood pressure, glycemic control — with the data behind each number
How to structure training for strength, hypertrophy, power, or endurance, with the evidence for each rep range
Where the protein and supplement research genuinely supports a recommendation, and where it doesn't
The most common mistakes and myths, debunked with actual study data
A practical, beginner-to-advanced framework you can start using today
1. What Is Strength Training? A Clinical Definition
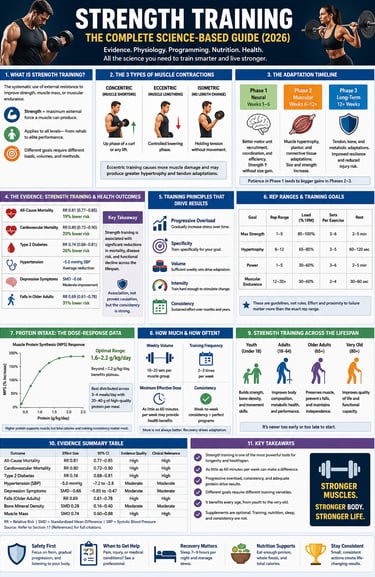
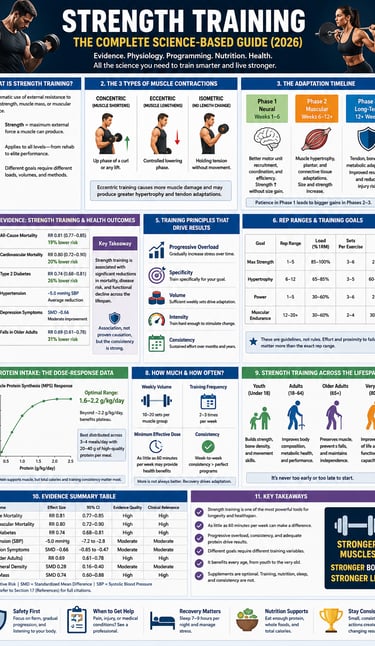
Strength training is the systematic application of external resistance to skeletal muscle, performed with the intent of producing adaptations in strength, muscle mass, or muscular endurance. Researchers define strength specifically as the maximum amount of external force a muscle or muscle group can generate against resistance — a distinct concept from internal force production (e.g., the heart contracting) or power (force production over time).
This distinction matters clinically. A rehabilitation patient working on isometric quad activation, a powerlifter chasing a 500-lb deadlift, and an office worker doing bodyweight squats at home are all "strength training," but the loading parameters, intent, and expected adaptations differ substantially. Generic advice ("just lift weights") glosses over this; good programming does not.
The Three Muscle Contraction Types
Every resistance exercise involves some combination of:
Concentric contraction — the muscle shortens under load (the "up" phase of a bicep curl)
Eccentric contraction — the muscle lengthens under load (the controlled "down" phase)
Isometric contraction — the muscle generates tension without changing length (a wall sit, a plank, the sticking point of a heavy squat)
Each contributes differently to adaptation. Eccentric-emphasised training, for example, tends to produce greater muscle damage and has been studied specifically for its disproportionate role in hypertrophy and tendon stiffness — which is clinically relevant for anyone managing tendinopathy, where controlled eccentric loading is a standard rehabilitation tool.
2. The Physiology: What's Actually Happening in Your Body
Understanding why strength training works helps you interpret the rest of this guide critically rather than taking dosing recommendations on faith. There are three overlapping adaptation phases.
Phase 1: Neuromuscular Adaptation (Weeks 1–6)
Early strength gains — often a 10–30% increase in maximal force production within the first few weeks — happen almost entirely without measurable increases in muscle size. This is a neural phenomenon: improved motor unit recruitment, reduced co-contraction of antagonist muscles, and better intermuscular coordination.
Clinical relevance: This is why a true beginner's rapid early progress is not a sign that their program is uniquely effective — it's a near-universal response to any novel loading stimulus. Be cautious about extrapolating early-phase results (yours or a program's marketing claims) to long-term outcomes.
Phase 2: Muscle Hypertrophy (Weeks 6+)
With continued progressive loading, muscle fibers increase in cross-sectional area through increased contractile protein (actin and myosin) synthesis. This is the phase most people associate with "getting bigger" or "toning up," and it requires a sustained training stimulus over months, not weeks.
Phase 3: Metabolic and Systemic Adaptation
Resistance-trained muscle is more metabolically active at rest. Beyond the muscle tissue itself, resistance training improves insulin sensitivity, alters lipid profiles, and produces what's sometimes called the "afterburn effect" (excess post-exercise oxygen consumption, or EPOC) — though it's worth being precise here: EPOC from a typical resistance session burns a modest number of additional calories (commonly cited in the range of roughly 6–15% of the session's total energy expenditure in controlled studies), not the dramatic "your metabolism is revved for days" framing often used in marketing.
3. Weight Training vs. Strength Training: Clearing Up the Confusion
These terms get used interchangeably online, but they aren't synonyms.
Term Definition Examples Weight training A subset of strength training using added external weight, specifically Barbells, dumbbells, weight machines, and weighted vests. Strength training: The broader category — any method that loads muscle against resistance Bodyweight exercise, free weights, machines, resistance bands, suspension trainers (TRX), plyometrics
Weight training is one tool inside the strength training toolbox. This matters practically: someone without gym access is not excluded from strength training — bodyweight progressions (push-up variations, pistol squat progressions, pull-up negatives) can drive meaningful strength and hypertrophy adaptations, particularly for beginners and intermediate trainees.
4. General vs. Specific Strength Training
General strength training targets overall musculoskeletal capacity — the foundation most people need for health, injury resilience, and daily function.
Specific strength training targets the force-production patterns of a particular sport or task. A sprinter trains explosive hip extension; a swimmer trains scapular stability and pulling strength; a rock climber trains grip endurance and pulling force at unusual joint angles.
The governing concept here is the SAID principle (Specific Adaptations to Imposed Demands): your body adapts specifically to the stress you place on it. This is why periodized programming for athletes typically shifts emphasis across a training year — maximal strength development in the off-season, maintenance plus sport-skill integration in-season — rather than running one static program year-round.
5. The Evidence on Health Outcomes — With Full Data Interpretation
This is the section where rigor matters most, because health claims in this space are routinely overstated. Below, each major outcome is presented with the actual effect size and an honest read on what it means.
All-Cause Mortality
A systematic review and meta-analysis pooling data on resistance training and mortality found that, compared with no resistance training, doing any amount of resistance training was associated with a 15% reduction in all-cause mortality risk, a 19% reduction in cardiovascular disease mortality, and a 14% reduction in cancer mortality
How to interpret this correctly:
These are observational, pooled associational data, not randomized controlled trial outcomes. Resistance-training adults differ from non-trainers in ways researchers can't fully control for (health-seeking behavior, baseline fitness, socioeconomic factors) — so causation is plausible but not proven with the same certainty as a drug RCT.
The dose-response relationship was nonlinear, with the meta-analysis identifying a peak risk reduction of roughly 27% around 60 minutes of resistance training per week — and risk reduction diminishing at higher volumes in the pooled data. This is a critical, underreported finding: the data does not support "more is always better" for mortality risk specifically, even though more volume may still benefit strength or hypertrophy goals.
The 95% confidence interval for cardiovascular mortality reduction (0.66–1.00) touches 1.00 at its upper bound, meaning the result sits at the edge of statistical significance — a detail that responsible reporting should not gloss over.
Clinical takeaway: A small, consistent dose of resistance training — well within what most beginner guidelines already recommend — appears to capture most of the mortality-risk benefit observed in the literature. This is good news for adherence: you don't need to train for hours to access this benefit.
Cardiovascular Health
Randomized controlled trial data on resistance training and blood pressure show meaningful, clinically relevant reductions — commonly cited in the range of 3–6 mmHg systolic and 2–4 mmHg diastolic for resistance-trained groups versus controls, depending on the specific meta-analysis and population studied.
Clinical relevance check: A 5 mmHg systolic reduction is not cosmetic — at a population level, blood pressure reductions of this magnitude are associated with meaningfully lower stroke and cardiovascular event rates in epidemiological models. However, individual results vary substantially, and resistance training should be discussed with a physician as an adjunct to, not automatic replacement for, prescribed antihypertensive therapy.
Type 2 Diabetes and Glycemic Control
Resistance exercise improves glycemic control through two distinct mechanisms: acute increases in muscle glucose uptake (largely insulin-independent during and shortly after exercise) and chronic improvements in insulin sensitivity from increased muscle mass and GLUT4 transporter expression.
Important nuance: Headlines sometimes claim resistance training is "more effective than medication" for glycemic control. This overstates the evidence. Resistance training is a well-supported adjunct therapy with meaningful effect sizes on HbA1c in trial data, but it is not positioned by major diabetes guidelines as a medication replacement. Anyone managing Type 2 diabetes should treat exercise as a complement to, not a substitute for, medical management — and should consult their physician before starting, especially if on insulin or sulfonylureas (hypoglycemia risk during exercise).
Bone Density and Osteoporosis
Weight-bearing and resistance exercise stimulate osteogenic (bone-building) responses through mechanical loading on bone tissue (Wolff's Law). Effect sizes on bone mineral density in postmenopausal women and older adults are generally modest but consistent across trials, and the functional benefit — improved balance, strength, and fall resilience — may matter as much for fracture prevention as the BMD change itself.
Mental Health
Meta-analytic data on resistance training and depressive symptoms shows a consistent, moderate effect — comparable in magnitude to what's seen with aerobic exercise interventions in similar populations. As with any psychological outcome measured by self-report scales, individual response varies, and resistance training should not be presented as a substitute for clinical treatment of moderate-to-severe depression or anxiety disorders.
6. The Five Training Principles That Actually Drive Results
Progressive overload — Continually increasing the demand placed on muscle (more load, more reps, more sets, less rest, higher frequency) is the single most consistent driver of continued adaptation across the literature.
Specificity — Adaptations mirror the demands imposed; training a movement pattern improves that pattern most directly.
Progression and periodization — Systematic, planned increases in training stress outperform random or aggressive jumps, both for results and injury-risk reduction.
Individual variation — Response to identical training stimuli varies meaningfully between individuals based on training history, genetics, recovery capacity, and lifestyle factors. Population-average results (like the ones cited throughout this guide) describe central tendencies, not guarantees for any one person.
Reversibility — Detraining reduces strength and muscle mass within weeks of cessation, though "muscle memory" (epigenetic and neural retention) allows faster reacquisition than initial acquisition.
7. Program Design by Goal: Strength, Hypertrophy, Power, Endurance
Evidence-Based Programming: To get the best results, match your training variables directly to your specific fitness goals. These guidelines are drawn from current resistance-training literature and recent network meta-analyses.
The Blueprint by Training Goal:
Maximal Strength: Lift 85%+ of 1RM | 2–6 sets | ≤6 reps | 2–5 min rest
Power: Lift 80–90% of 1RM | 3–5 sets | 1–5 reps | 2–5 min rest
Hypertrophy (Muscle Size): Lift 67–85% of 1RM | 3–6 sets | 6–12 reps | 30–90 sec rest
Muscular Endurance: Lift <67% of 1RM | 2–3 sets | 12+ reps | <30 sec rest
The Rep-Range Debate: Key Nuance
The Old Dogma: Traditional strength and conditioning held a rigid "6–12 reps for size" rule.
The Modern Science: Recent training-to-failure studies show that muscle growth can happen across a much wider range (6 to 30+ reps).
The Requirement: For high-rep sets to build muscle, they must be taken close to volitional fatigue (true effort) and total training volume must be matched.
The Practical Takeaway: The traditional 6–12 range isn't a hard physiological ceiling; it simply remains the most time-efficient, practical default for most lifters.
One-Rep Max (1RM) Testing: Safety Protocol
If you choose to test your true 1RM directly, follow this strict safety protocol:
Thorough Warm-Up: Spend 15–30 minutes warming up, including specific ramp-up sets for the movement you are testing.
Set 1 (Light): Perform 6–10 repetitions at roughly 50% of your estimated 1RM.
Set 2 (Moderate): Increase to roughly 80% of your estimated 1RM for 3 repetitions.
The Max Attempts: Increase the weight in 5% to 10% increments, resting 3–5 minutes between each attempt.
The Golden Rule: Stop immediately if your form breaks down. A "successful" lift achieved with compromised technique is invalid, dangerous, and a high injury risk.
💡 Smart Alternative: To completely avoid the injury risks of true maximal testing, use sub-maximal reps paired with validated prediction equations (like the Epley or Brzycki formulas) to safely estimate your 1RM.
8. How Much Protein Do You Actually Need? The Dose-Response Data
Protein intake is one of the most searched, most argued-about, and most overstated topics in strength training content. Here's what the dose-response data actually shows — and where the studies disagree.
A meta-analysis and meta-regression spanning 42 study arms and 723 participants on resistance-trained adults found that gains in fat-free mass plateaued at approximately 1.62 g/kg/day of total protein intake (95% CI: 1.03–2.20). A separate dose-response meta-analysis of RCTs found that muscle strength gains increased roughly 0.72% per 0.1 g/kg/day increase in protein intake up to about 1.5 g/kg/day, beyond which no further strength benefit was observed.
Where the evidence is genuinely mixed: Some researchers (e.g., work by Antonio and colleagues) have reported that intakes well above 3 g/kg/day were tolerated without adverse effects and associated with favorable body-composition outcomes in resistance-trained athletes — while other meta-analyses (e.g., Cintineo et al.) found only marginal additional lean-mass gains at higher intakes, reinforcing a diminishing-returns pattern. Current sports-nutrition guidance generally lands in the 1.2–2.0 g/kg/day range for resistance-trained individuals, with the upper end reserved for those in caloric restriction or high training volumes who are actively trying to preserve lean mass.
Practical, defensible takeaway: For most resistance-trained adults, targeting 1.6 g/kg/day of bodyweight sits right at the plateau point identified across multiple independent meta-analyses — a reasonable, well-supported target rather than a number to chase upward indefinitely. Going meaningfully above this is unlikely to be harmful for healthy individuals with normal kidney function, but the data does not support a meaningfully better outcome from doing so.
A caveat on confidence intervals: Notice that the fat-free-mass plateau estimate above (1.62 g/kg/day) has a 95% CI ranging from 1.03 to 2.20 — a wide interval. This tells you the "true" plateau point is uncertain at the individual level; treat 1.6 g/kg/day as a sensible population-level target, not a number with single-decimal precision for your specific body.
9. Training Frequency and Volume: What the Research Supports
For beginners: 2–3 full-body sessions per week, with 48–72 hours of recovery between sessions targeting the same muscle groups, is well-supported as a starting point across the literature.
For experienced trainees: Systematic review data on training frequency for hypertrophy (e.g., Schoenfeld, Grgic, and Krieger's frequency meta-analysis) suggests that total weekly volume — sets × reps × load, summed across the week — matters more than how that volume is distributed across sessions, once you control for total work performed. This means 2 higher-volume sessions per muscle group per week can produce comparable results to 4 lower-volume sessions, provided weekly volume is equated.
Important honesty note: Most volume-equating studies are short-to-medium duration (typically 6–12 weeks) and use trained or moderately trained populations. Be cautious extending these conclusions indefinitely or to complete beginners, whose primary limiting factor is often movement-pattern learning and adherence rather than precise volume optimization.
10. Strength Training Across the Lifespan
Aging, Sarcopenia, and Functional Independence
Sarcopenia — the age-related, progressive loss of muscle mass and strength — begins as early as the 30s and accelerates after age 60. Resistance training is one of the few interventions with consistent trial evidence for reversing, not just slowing, age-related strength decline, including in adults in their 80s and 90s.
A 2025 Bayesian network meta-analysis examining optimal resistance training dosing for older adults with sarcopenia specifically investigated the dose-response relationship between training parameters and handgrip strength — reflecting a broader and welcome shift in the field toward identifying minimum effective doses for older populations, rather than assuming "more training is always better" applies uniformly across age groups.
Clinical relevance: For older adults, the goal of resistance training is frequently functional — the ability to rise from a chair unassisted, climb stairs, or recover balance after a stumble — not aesthetic or performance-based. Programs for this population should prioritize movement patterns that transfer to daily function (sit-to-stand, step-ups, loaded carries) alongside traditional strength exercises, and should generally begin under the guidance of a physical therapist or qualified trainer experienced with older adults, particularly if osteoporosis, joint replacement history, or cardiovascular disease is present.
Special Populations
Resistance training has trial-level support for safety and benefit (with appropriate medical clearance and program modification) in:
Cardiovascular disease (including post-cardiac-event rehabilitation contexts)
Type 2 diabetes
Osteoarthritis and rheumatoid arthritis
Cancer survivors, during and after active treatment
COPD and other chronic respiratory conditions
In every one of these populations, individual medical clearance and program modification matter more than generic guidelines. This guide is educational and does not replace a conversation with your physician or a qualified clinical exercise physiologist, especially if you have an existing diagnosis.
11. Evidence Summary Tables
All-Cause Mortality: Tied to a 15% reduction in early death risk. Caveat: This is based on observational data, showing a strong link rather than direct proof of cause and effect.
Cardiovascular Disease (CVD) Mortality: Linked to a 19% reduction in death risk (RR 0.81; CI: 0.66–1.00). Caveat: Because the upper boundary of the confidence interval touches 1.00, the statistical certainty of this benefit is slightly weaker.
Cancer Mortality: Associated with a 14% reduction in risk (RR 0.86; CI: 0.78–0.95). Caveat: Like all-cause mortality, this proves a strong association rather than definitive causation.
The "Sweet Spot" for Longevity: Peak benefits occur at roughly 60 minutes of strength training per week, yielding an estimated 27% risk reduction (CI: 0.64–0.86). Beyond 60 minutes, data shows benefits tend to plateau or slightly decline.
Key Takeaways: Daily Protein Intake and Muscle Gains
For Building Muscle (Fat-Free Mass): Benefits plateau at roughly 1.62 grams of protein per kilogram of body weight per day
For Building Strength: Gains level off at a slightly lower threshold of roughly 1.50 grams per kilogram per day, according to spline-modeled clinical trials.
General Sports Consensus: Mainstream athletic guidelines universally recommend a wider bracket of 1.2 to 2.0 grams per kilogram per day depending on total training intensity.
Critical Thinking: How to Read the Science
Wide Intervals Mean High Variance: The wide confidence interval for building muscle (1.03 to 2.20 g/kg/day) shows that individual genetics and training styles cause highly varied responses. Use the 1.62g central estimate as a helpful baseline target, not a strict medical rule.
Beware of "The Null": When a statistical range touches 1.00 (as seen in the CVD mortality data), the math indicates a high likelihood of a benefit, but lacks total certainty. Communicate these specific metrics with realistic optimism rather than absolute guarantees.
12. Common Myths and Mistakes — Debunked With Data
Myth 1: "Lifting weights will make women bulky"
Reality: Significant muscle hypertrophy is substantially influenced by testosterone levels, which differ by roughly tenfold between men and women on average. Most women who strength train see improved muscle tone, strength, and body composition without the magnitude of size increase often feared — and achieving a heavily muscled physique as a woman typically requires years of dedicated, high-volume training plus deliberate caloric surplus, not three weekly gym sessions.
Myth 2: "Cardio is superior for fat loss"
Reality: Comparative trial data shows resistance training can match or exceed cardio-only protocols for body composition outcomes specifically because it preserves lean mass during a caloric deficit — cardio-only weight loss tends to come from a higher proportion of lean tissue loss alongside fat loss, which is a less favorable composition outcome even when scale weight drops similarly.
Myth 3: "You need to train every day to see results"
Reality: As shown in Section 9, total weekly volume — not daily frequency — is the stronger predictor of outcomes once volume is equated. Daily training without adequate recovery for a given muscle group can actually impair adaptation through accumulated fatigue.
Myth 4: "More protein is always better"
Reality: Multiple independent meta-analyses identify a plateau around 1.5–1.6 g/kg/day for strength and lean-mass outcomes specifically. Intakes well above this aren't typically harmful in healthy individuals, but they don't reliably produce additional muscle-building benefit either — the literature here genuinely supports "enough," not "more."
Myth 5: "Soreness means a good workout; no soreness means it didn't work"
Reality: Delayed-onset muscle soreness (DOMS) reflects unfamiliar mechanical stress, particularly eccentric loading, not training effectiveness. Well-adapted, consistently trained muscle often produces minimal soreness from a productive session — soreness is a poor proxy for whether you stimulated adaptation.
Mistake: Chasing 1RM testing as a beginner
Testing a true one-rep max requires technical proficiency under near-maximal load. Beginners without established movement competency face disproportionate injury risk relative to the information gained — submaximal-rep prediction formulas are safer and sufficiently accurate for program design at this stage.
13. Sample Programs
1. Beginner Full-Body Routine
Schedule: 3 days per week on non-consecutive days (e.g., Monday, Wednesday, Friday).
The Workout Split:
Goblet Squat or TRX Squat: 3 sets of 12–15 repetitions.
Hip Hinge (Romanian Deadlift, light load): 3 sets of 12–15 repetitions.
Lat Pulldown or Assisted Pull-Up: 3 sets of 12–15 repetitions.
Push-Up (knee-modified if needed): 3 sets of 12–15 repetitions.
Dumbbell Bicep Curl: 2 sets of 12–15 repetitions.
Tricep Extension: 2 sets of 12–15 repetitions.
Plank: 3 sets of a 20–40 second hold.
2. Intermediate/Advanced Strength-Focus Routine
Schedule: 4 days per week (Off-season structure).
The Workout Split:
Barbell Back Squat: 3 sets of 6–8 repetitions at roughly 80% of your 1RM.
Romanian Deadlift: 3 sets of 8 repetitions at roughly 75% of your 1RM.
Dumbbell Bench Press: 3 sets of 6–8 repetitions at roughly 80% of your 1RM.
Weighted Pull-Up or Barbell Row: 3 sets of 6–8 repetitions at roughly 75% of your 1RM.
Walking Lunge: 3 sets of 10 repetitions per leg with a moderate load.
Core Circuit (Planks, Dead Bugs, Side Planks): 2–3 sets of 30–45 second holds using body weight.
Weekly Training Structure (4x/Week Split)
To organize your intermediate routine effectively, follow this structured weekly flow to ensure proper recovery:
Day 1: Lower Body Focus (Push and Pull movements)
Day 2: Upper Body Focus (Push and Pull movements)
Day 3: Active Recovery / Rest Day
Day 4: Full Body Integration
Day 5: Upper/Lower Hypertrophy Focus
Day 6 & 7: Full Recovery / Rest Days14. Safety, Form, and When to See a Professional
Prioritize technical proficiency before load. Movement competency should precede progressive overload, not the reverse.
Progress load conservatively — roughly 5–10% increases once a given weight feels clearly manageable across all prescribed reps with good form.
Stop a set if form breaks down, regardless of whether the prescribed rep count is reached.
Consult a physician before beginning a resistance training program if you have cardiovascular disease, uncontrolled hypertension, are pregnant, have a recent injury or surgery, or have any condition where exertion-related risk is unclear.
Consider a qualified trainer or physical therapist for individualized programming, especially when returning from injury, managing a chronic condition, or starting resistance training for the first time after age 60.
15. Frequently Asked Questions
How long before I see results from strength training? Neuromuscular strength improvements can appear within 2–4 weeks of consistent training. Visible changes in muscle size typically take 6–8+ weeks of progressive, consistent training to become apparent, and longer for substantial change.
Can I strength train every day? Muscles generally need 48–72 hours of recovery before the same muscle group is trained again at meaningful intensity. Daily training is possible if you rotate which muscle groups are emphasized (a "split" routine), but daily full-body sessions at high intensity typically outpace recovery capacity for most people.
Is strength training safe for older adults? Yes — with appropriate medical clearance and program modification, resistance training is well-supported in the literature for older adults, including those with sarcopenia, osteoporosis, or cardiovascular disease. It's one of the few interventions shown to meaningfully improve functional independence in this population.
Should I do cardio or strength training first in the same session? Evidence suggests prioritizing whichever modality aligns with your primary goal — strength/hypertrophy work first if that's the priority, since fatigue from cardio can compromise lifting performance, and vice versa if cardiovascular fitness is the main goal.
How much weight should I start with as a beginner? A practical starting point: choose a load that allows 12–15 reps with good form, where the final 2–3 reps feel meaningfully challenging but technically clean.
Can strength training help with weight loss? Yes, primarily by preserving lean mass during a caloric deficit (improving body composition outcomes) and modestly increasing resting energy expenditure — though resistance training alone, without attention to overall caloric intake, is unlikely to produce significant weight loss by itself.
Do I need to take protein supplements, or can I get enough from food? Whole-food protein sources work equivalently to supplemental protein for muscle-building purposes when total daily intake is matched. Supplements (whey, casein, plant-based powders) are a convenience tool for hitting your total daily target, not a requirement.
What's the difference between training for strength versus training for muscle size (hypertrophy)? Strength-focused training emphasizes heavier loads (85%+ 1RM) and lower reps (≤6), prioritizing neuromuscular efficiency. Hypertrophy-focused training uses a broader, more moderate load range with sets typically taken close to fatigue. There's meaningful overlap in outcomes between the two approaches, particularly at moderate-to-high training volumes.
Is it normal to feel sore after every workout? No — soreness reflects unfamiliar mechanical stress more than training quality, and tends to diminish as your body adapts to a given exercise, even as you continue progressing the load.
Can resistance training replace my blood pressure or diabetes medication? No. Resistance training is well-supported as a beneficial adjunct for both conditions, but should not replace prescribed medication without your physician's explicit guidance based on your individual case.
What's the minimum effective dose of resistance training for health benefits? Pooled mortality-risk data suggests benefits are detectable with even a modest weekly dose, with one major meta-analysis identifying peak risk-reduction association around 60 minutes per week — though this is a population-level association, not an individual guarantee, and more volume may still benefit strength and hypertrophy goals specifically.
Is bodyweight training as effective as using weights? For beginners and intermediate trainees, yes — bodyweight progressions can produce comparable strength and hypertrophy outcomes to external weights, particularly when exercises are progressed in difficulty (e.g., single-leg variations, slowed tempo, added range of motion). Free weights offer more straightforward long-term progressive overload for advanced trainees who've maxed out bodyweight progressions.
16. Conclusion and Action Steps
Strength training is one of the most thoroughly studied, consistently beneficial interventions in all of exercise science — but the most useful version of that evidence is the honest version: effect sizes with confidence intervals, dose-response curves with plateaus, and a clear line between what's proven and what's still being worked out.
Your next steps:
Start with 2–3 full-body sessions per week if you're new to resistance training, allowing 48–72 hours recovery between sessions targeting the same muscles.
Pick your tools — bodyweight, free weights, machines, or bands — based on access and comfort, not because one is objectively superior for beginners.
Match your rep range to your primary goal using the program design table in Section 7.
Target roughly 1.6 g/kg/day of protein if muscle gain or retention is a goal — and don't feel pressured to exceed it based on supplement marketing.
Progress load conservatively (5–10% increases) once a given weight becomes clearly manageable.
Get medical clearance if you have any existing cardiovascular, metabolic, or musculoskeletal condition before starting.
Track your sessions so progressive overload is measurable, not guesswork.
The single biggest predictor of long-term results in the literature isn't the perfect program — it's consistency. Start where you are, apply the evidence above, and build from there.
Author's Note: A Clinician's Perspective
As a physician, one of the most striking observations in clinical practice is that muscle strength often predicts health outcomes more accurately than many people realize. Patients frequently focus on body weight, cholesterol levels, or blood sugar numbers, yet overlook one of the most powerful determinants of long-term health: the strength and function of their muscles.
Over the years, I have cared for individuals with obesity, type 2 diabetes, cardiovascular disease, osteoporosis, and age-related frailty. A common pattern emerges repeatedly. Patients who maintain muscle strength and physical function generally remain more independent, recover more effectively from illness, tolerate medical treatments better, and enjoy a higher quality of life than those with significant muscle loss.
Strength training is not merely about building larger muscles or improving appearance. Skeletal muscle is a metabolically active organ that influences blood sugar regulation, insulin sensitivity, mobility, bone health, cardiovascular health, and healthy aging. The scientific evidence reviewed in this article demonstrates that even modest amounts of resistance training can produce meaningful health benefits.
A Patient Example
One patient in his late 50s came to my clinic with type 2 diabetes, hypertension, excess abdominal weight, and increasing fatigue. He believed his only options were additional medications and stricter dieting. Although his weight was a concern, a more significant issue was his declining muscle strength and physical fitness.
After medical clearance, he began a simple strength-training program three times per week, focusing on basic movements such as squats, rowing exercises, push-ups, and resistance-band work. Initially, he could perform only a few repetitions before becoming fatigued.
Over the following year, he gradually became stronger, increased his lean muscle mass, improved his physical function, and gained confidence in his ability to exercise. His blood sugar control improved, his blood pressure decreased, and everyday tasks such as climbing stairs and carrying groceries became noticeably easier. Most importantly, he reported feeling healthier, more energetic, and more capable than he had in years.
While individual results vary, this example reflects what many clinicians observe regularly: improvements in strength often translate into improvements in overall health, independence, and quality of life.
Medical Disclaimer
The information in this article, including the research findings, is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Before starting a resistance exercise program, you must consult with a qualified healthcare professional, especially if you have existing health conditions (such as cardiovascular disease, uncontrolled hypertension, or advanced metabolic disease). Exercise carries inherent risks, and you assume full responsibility for your actions. This article does not establish a doctor-patient relationship.
Related Articles
Can Light Weights Build as Much Muscle as Heavy Weights? What Research Shows
The Hidden Muscle–Fat Communication Disorder That Accelerates Aging, Diabetes, and Frailty
Fat Communication Disorder That Accelerates Aging, Diabetes, and Frailt
How Exercise Reprograms Your Hormones to Burn Fat, Lower Cortisol & Boost Metabolism | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
No Time to Train? Science-Backed Workouts That Deliver | DR T S DIDWAL
References
Shailendra, P., Baldock, K. L., Li, L. S. K., Bennie, J. A., & Boyle, T. (2022). Resistance training and mortality risk: A systematic review and meta-analysis. American Journal of Preventive Medicine, 63(2), 277–285. https://doi.org/10.1016/j.amepre.2022.03.020
Booker, R., Wong, M., Boyer, W., Gorzelitz, J., Carnethon, M. R., & Alexandria, S. J. (2024). Associations between resistance training and all-cause mortality: NHANES 1999–2006. American Journal of Lifestyle Medicine. https://doi.org/10.1177/15598276241248107
Paluch, A. E., et al. (2024). [Cardiovascular disease and resistance training dose-response]. As cited in Frontiers in Physiology meta-analysis, 2025.
[Optimal dose of resistance training to improve handgrip strength in older adults with sarcopenia]. (2025). Frontiers in Physiology, 16. https://doi.org/10.3389/fphys.2025.1564988
Morton, R. W., Murphy, K. T., McKellar, S. R., et al. (2018). A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine, 52(6), 376–384.
Tagawa, R., Watanabe, D., Ito, K., et al. (2022). Synergistic effect of increased total protein intake and strength training on muscle strength: A dose-response meta-analysis of randomized controlled trials. Sports Medicine - Open, 8(1), 110. https://doi.org/10.1186/s40798-022-00508-w
[Current Perspectives on Protein Supplementation in Athletes: General Guidance and Special Considerations]. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12655512/
Nunes, J. P., et al. (2022). Systematic review and meta-analysis of protein intake to support muscle mass and function in healthy adults. PubMed. https://pubmed.ncbi.nlm.nih.gov/35187864/
Macnaughton, L. S., Wardle, S. L., Witard, O. C., et al. (2016). The response of muscle protein synthesis following whole-body resistance exercise is greater following 40 g than 20 g of ingested whey protein. Physiological Reports, 4(15), e12893.
Currier, B. S., McLeod, J. C., Banfield, L., et al. (2023). Resistance training prescription for muscle strength and hypertrophy in healthy adults: A systematic review and Bayesian network meta-analysis. British Journal of Sports Medicine, 57(18), 1211–1220. https://doi.org/10.1136/bjsports-2023-106807
Schoenfeld, B. J., Grgic, J., Van Every, D. W., & Plotkin, D. L. (2021). Loading recommendations for muscle strength, hypertrophy, and local endurance: A re-examination of the repetition continuum. Sports, 9(2), 32. https://doi.org/10.3390/sports9020032
Morton, R. W., Colenso-Semple, L., & Phillips, S. M. (2019). Training for strength and hypertrophy: An evidence-based approach. Current Opinion in Physiology, 10, 90–95. https://doi.org/10.1016/j.cophys.2019.04.006
Suchomel, T. J., Nimphius, S., Bellon, C. R., & Stone, M. H. (2018). The importance of muscular strength: Training considerations. Sports Medicine, 48(4), 765–785. https://doi.org/10.1007/s40279-018-0862-z
Schoenfeld, B. J., Grgic, J., & Krieger, J. (2019). How many times per week should a muscle be trained to maximize muscle hypertrophy? A systematic review and meta-analysis of studies examining the effects of resistance training frequency. Journal of Sports Sciences, 37(11), 1286–1295.
[Dose-response relationship of physical activity with all-cause mortality among older adults: An umbrella review]. (2024). Journal of the American Medical Directors Association, 25(3), 417–430. https://doi.org/10.1016/j.jamda.2023.09.028
American Diabetes Association. Standards of Care in Diabetes (current edition). https://diabetesjournals.org/care
National Institute on Aging. Exercise and Physical Activity. https://www.nia.nih.gov/health/exercise-and-physical-activity
National Osteoporosis Foundation / Bone Health and Osteoporosis Foundation. Exercise for Healthy Bones. https://www.bonehealthandosteoporosis.org
Physio-pedia. Strength Training. https://www.physio-pedia.com/index.php?title=Strength_Training&oldid=368519
American College of Sports Medicine. ACSM's Guidelines for Exercise Testing and Prescription (current edition).