The Hidden Muscle–Fat Communication Disorder That Accelerates Aging, Diabetes, and Frailty
Sarcopenic obesity silently combines muscle loss and fat gain, increasing the risk of diabetes, frailty, and premature aging. Learn how to reverse it
SARCOPENIA
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/20/202621 min read
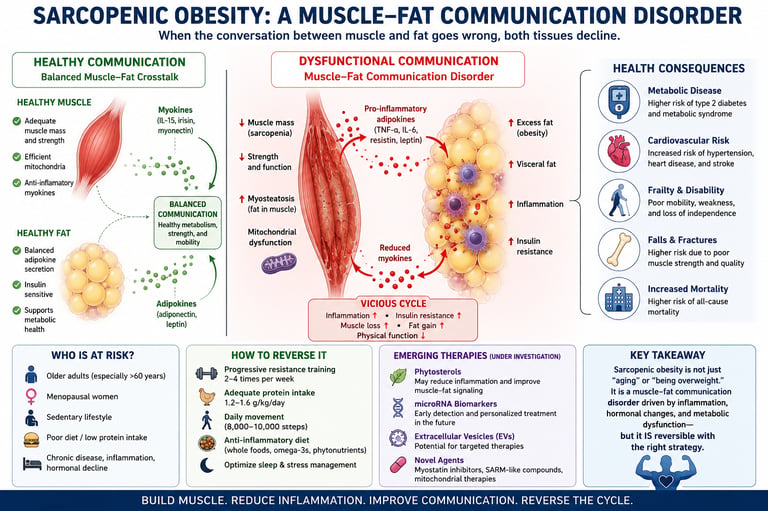
Sarcopenic obesity is a muscle-fat communication disorder in which excess body fat and declining muscle mass reinforce each other through inflammatory, hormonal, and metabolic pathways. This hidden condition increases the risk of diabetes, frailty, cardiovascular disease, falls, and premature aging, even in people with a normal BMI.
Clinician Pearls
BMI may miss sarcopenic obesity.
Grip strength predicts mortality.
Resistance training is the cornerstone intervention.
Rapid weight loss without protein can worsen muscle loss.
Menopause is a major risk window
Key takeaways
1. What is sarcopenic obesity?
Sarcopenic obesity is a condition where you lose muscle mass and strength while simultaneously gaining body fat. It is most common in adults over age 60. Unlike regular weight gain, these two issues lock together in a harmful loop, where the fat tissue actively weakens your muscles, and losing muscle makes it harder to manage body fat.
2. Can you have sarcopenic obesity with a normal weight?
Yes. Sarcopenic obesity is often called a "hidden" crisis because it can occur even if you have a normal weight or BMI on the scale. Because standard doctor visits frequently rely just on your overall weight, this condition is easily missed unless your doctor specifically checks your actual muscle strength and body composition.
3. How do fat and muscle "talk" to each other?
Your fat and muscle tissues act like communication centers, sending chemical signals throughout your body. In sarcopenic obesity, excess fat tissue sends out inflammatory signals that actively block your muscles from repairing and growing. This biological crosstalk creates an energy crisis inside your muscle cells, making them weaker over time.
4. Why does menopause increase the risk?
The risk of developing sarcopenic obesity rises sharply for women during and after menopause. This happens because the natural drop in estrogen removes a key hormonal shield that normally protects muscle health and prevents fat from gathering around your deep internal organs (visceral fat).
5. How is this condition diagnosed?
You cannot diagnose sarcopenic obesity with a standard bathroom scale. Doctors look for a combination of three things: low muscle mass (measured by a body scan like a DEXA scan), low muscle function (often checked with a quick hand-grip strength test), and an elevated body fat percentage.
6. What are the health risks of losing muscle while gaining fat?
Carrying too much fat with too little muscle is highly taxing on the body. This combination is linked to a much higher risk of developing type 2 diabetes, heart disease, and joint issues. Because muscles keep us stable, losing them also significantly increases your risk of falls and bone fractures.
7. What is the best way to reverse sarcopenic obesity?
The most proven, effective treatment is combining regular resistance training with adequate dietary protein. Simple cardio like walking is great for your heart, but you need strength exercises (using weights, resistance bands, or your own body weight) 2 to 3 times a week to force your muscles to rebuild and recover.
8. How much protein do you need to protect your muscles?
To combat muscle loss, older adults often need more protein than younger adults—typically 1.2 to 1.6 grams of protein per kilogram of body weight daily. For the best results, doctors recommend spreading your protein evenly across all your meals (about 25–30 grams per meal) using protein-rich foods like fish, eggs, poultry, and beans.
Introduction
You can be "overweight" on a scale and still be dangerously under-muscled underneath. That combination — excess body fat layered on top of shrinking, weakening muscle — is called sarcopenic obesity, and it's one of the most under-diagnosed health problems in adults over 50.
Unlike classic obesity, sarcopenic obesity doesn't always show up as a high number on the scale. Many people with this condition have a "normal" BMI, which is exactly why doctors miss it. What's happening underneath the surface, though, is anything but normal: fat tissue and muscle tissue are locked in a destructive biochemical conversation that accelerates frailty, insulin resistance, cardiovascular disease, and falls.
This article breaks down what the latest 2024–2026 research actually shows about sarcopenic obesity — the cellular crosstalk driving it, who is most at risk, how it's diagnosed, and most importantly, what you can do starting today to reverse the trajectory. We'll translate dense molecular biology (extracellular vesicles, myokines, adipokines, mitochondrial dysfunction) into plain language, while staying anchored to what the data can and cannot tell us about real-world outcomes.
By the end, you'll understand:
What sarcopenic obesity is and how it differs from "just being overweight" or "just losing muscle with age"
The molecular crosstalk between fat and muscle tissue that drives the condition
Who is at highest risk, including the special case of menopausal women
How clinicians diagnose it, and the limitations of current criteria
A practical, evidence-based nutrition and exercise protocol to reverse it
What emerging therapies (including phytosterols and microRNA biomarkers) can and can't promise yet
What Is Sarcopenic Obesity
Sarcopenic obesity (SO) is a clinical condition defined by the simultaneous presence of two problems that used to be studied separately: sarcopenia (progressive loss of skeletal muscle mass, strength, and function) and obesity (excess and often dysfunctional body fat).
It is not simply "sarcopenia plus obesity" added together. Research increasingly frames it as a distinct pathological entity, because the two conditions actively worsen one another through shared inflammatory and hormonal pathways — a feedback loop rather than two parallel problems.
According to a 2023 review published in Metabolism, excess adiposity creates a chronic pro-inflammatory environment that directly impairs muscle regeneration, while declining muscle mass reduces the body's capacity to regulate blood sugar and fat storage — each condition feeding the other.
Key distinguishing features of sarcopenic obesity:
Can occur at a normal BMI (sometimes called "normal-weight obesity with sarcopenia")
Often invisible on a standard scale-based check-up
Associated with myosteatosis — fat infiltrating directly into muscle tissue, not just surrounding it
Disproportionately affects people over 60, but can begin developing in midlife, especially during menopause
Sarcopenic obesity is a condition in which a person simultaneously has excess body fat and reduced skeletal muscle mass and strength, most common after age 60, where each condition accelerates the other through inflammatory and metabolic crosstalk between fat and muscle tissue.
The Science: How Fat and Muscle Talk to Each Other
This is the part most articles skip — and it's the part that actually explains why sarcopenic obesity is so hard to reverse with diet or exercise alone unless you understand the mechanism.
1. Adipokines vs. Myokines: A Chemical Tug-of-War
Both fat and muscle are endocrine organs — they secrete signaling molecules that travel through the bloodstream and influence each other.
Adipokines (signals from fat tissue) include leptin, resistin, and pro-inflammatory cytokines like TNF-α and IL-6.
Myokines (signals from muscle tissue) include irisin, IL-15, and myostatin.
In a healthy body, these signals stay balanced. In sarcopenic obesity, expanding and dysfunctional fat tissue (especially visceral fat) over-produces inflammatory adipokines. According to the 2023 review by Park and Choi in Metabolism, this chronic low-grade inflammation directly disrupts the signaling pathways muscle cells rely on for repair and growth, while simultaneously promoting fat storage — a self-reinforcing cycle.
2. Extracellular Vesicles: The Newest Piece of the Puzzle
One of the more exciting developments in this field involves extracellular vesicles (EVs) — tiny lipid-bound packages that cells use to send genetic material and proteins to other cells. A 2025–2026 review in Obesity Reviews (Macleod et al.) detailed how adipose tissue releases EVs that travel to skeletal muscle and directly alter gene expression inside muscle cells, promoting insulin resistance and impairing the muscle's ability to regenerate after damage.
Why this matters clinically: EVs may explain why sarcopenic obesity persists even when someone reduces their visible body fat. The molecular damage caused by years of EV-mediated crosstalk doesn't necessarily reverse on the same timeline as fat loss — which is one reason muscle-focused strategies (not just calorie-cutting) are essential.
3. Mitochondrial Dysfunction: The Energy Crisis Inside Your Muscle Cells
Muscle cells are packed with mitochondria, the organelles that generate cellular energy. In sarcopenic obesity, excess circulating fatty acids overwhelm muscle cells, leading to lipotoxicity — fat byproducts that damage mitochondrial function and trigger oxidative stress.
A notable 2026 study in the Journal of Future Foods examined how a phytosterol-rich intervention affected high-fat-diet-induced sarcopenic obesity in animal models. The researchers reported improvements in mitochondrial dynamics — the balance between mitochondrial fusion and fission that determines how efficiently muscle cells produce energy — alongside favorable shifts in gut microbiota composition.
Interpreting this result carefully: This is an animal (rodent) model study, not a human clinical trial. The mechanistic findings — improved mitochondrial fission/fusion balance and a reshaped gut microbiome — are biologically plausible and consistent with other research linking gut health to muscle metabolism (the so-called "gut-muscle axis"). However, translating an animal-model dose and effect size to a recommended human phytosterol intake would be premature. At this stage, it tells us where to look for future human research, not what to put into a daily supplement regimen.
4. Hormonal Decline: The Endocrine Layer
A 2026 review in Annals of Medicine (Minnetti et al.) emphasized the endocrinological dimension of sarcopenic obesity: declining growth hormone, testosterone, and estrogen levels with age reduce the body's anabolic (muscle-building) signaling, while insulin resistance and cortisol dysregulation push the body toward fat storage. This hormonal shift compounds the inflammatory mechanisms described above, which is part of why sarcopenic obesity accelerates so noticeably after major hormonal transitions like menopause.
5. The Menopause-Specific Pathway
A 2026 paper in Frontiers in Endocrinology (Zhang et al.) focused specifically on midlife women, outlining how the drop in estrogen during the menopausal transition removes a protective signal that normally supports muscle mitochondrial function and limits visceral fat accumulation. The researchers describe this as a mechanistic link explaining why sarcopenic obesity risk rises sharply in women during and after the menopausal transition, independent of chronological age alone.
Who Is Most at Risk?
While sarcopenic obesity is most prevalent in older adults, risk factors accumulate well before age 65.
Higher-risk groups include:
Adults over 60, with risk rising sharply after 70
Postmenopausal women, due to the estrogen-related mechanisms above
People with type 2 diabetes or insulin resistance
Individuals with a sedentary lifestyle, regardless of body weight
People who have lost significant weight rapidly without resistance training (including after bariatric surgery or while using GLP-1 medications)
Those with chronic low-grade inflammatory conditions
People with low dietary protein intake relative to their needs
A critical, often-missed risk group: normal-weight individuals with low muscle mass. Because BMI is the most commonly used screening tool in primary care, this group is frequently told they are "healthy weight" and given no further evaluation — despite carrying real metabolic risk.
How Sarcopenic Obesity Is Diagnosed {#diagnosis}
There is currently no single, universally agreed-upon diagnostic cutoff for sarcopenic obesity, which is one of the field's genuine limitations. Most clinical and research definitions combine:
Muscle mass assessment — typically via dual-energy X-ray absorptiometry (DEXA), bioelectrical impedance analysis (BIA), or CT/MRI muscle cross-sectional area
Muscle function/strength assessment — grip strength dynamometry and/or gait speed (commonly the 4-meter walk test)
Body fat assessment — body fat percentage by DEXA or BIA, since BMI alone is considered inadequate
Why this matters for you: If you ask your doctor to check for sarcopenic obesity, a scale and BMI calculation are not sufficient. You need (at minimum) a grip-strength test and a body composition measurement — both of which are quick, inexpensive, and increasingly available in primary care and physical therapy clinics.
Validity note: Because different studies use different combinations of cutoffs (some use appendicular lean mass divided by height squared, others use lean mass divided by fat mass, others use different grip-strength thresholds by sex and region), prevalence estimates for sarcopenic obesity vary widely across the literature — anywhere from under 5% to over 25% of older adults, depending on the criteria used. When you read a headline statistic about sarcopenic obesity prevalence, it's worth checking which diagnostic definition was used before treating the number as universal.
Why It Matters: Health Consequences
Sarcopenic obesity isn't just an aesthetic or fitness concern — it's consistently associated with worse outcomes than either obesity or sarcopenia alone, including:
Higher cardiovascular disease risk, including stroke risk, compared with either condition in isolation
Greater insulin resistance and elevated type 2 diabetes risk
Increased fall risk and fracture risk, due to combined low strength and excess load on joints
Reduced independence in activities of daily living among older adults
Higher all-cause mortality risk in several cohort studies, though absolute risk increases vary by population studied
Clinical relevance check: Most of the strongest mortality and cardiovascular data come from observational cohort studies, which can show association but cannot, by themselves, prove that sarcopenic obesity directly causes these outcomes rather than simply co-occurring with other risk factors like chronic disease burden or lower physical activity. This doesn't make the findings unimportant — but it does mean the appropriate clinical response is proactive risk management (the protocol below), not panic.
Evidence Summary Table: Key Studies
The Muscle-Fat Communication Breakdown (Park & Choi, 2023)
The Science: Researchers mapped out how fat and muscle act like communication centers. When fat tissue becomes dysfunctional, it floods the body with inflammatory signals that actively block muscles from repairing themselves.
The Bottom Line: This provides a clear biological blueprint of the condition, though as a summary review, it did not test new treatments on human patients.
Hidden "Cellular Packages" Cause Damage (Macleod et al., 2025/2026)
The Science: Fat tissue releases tiny, microscopic packages called extracellular vesicles that travel to your muscles. Once there, they actually alter muscle genes and trigger insulin resistance.
The Bottom Line: This explains why muscle weakness can persist even after you start losing weight. However, because this research is mostly limited to animal and cell models, human treatments targeting these packages are still a long way off.
The Menopause Risk Window (Zhang et al., 2026)
The Science: When estrogen levels drop during menopause, women lose a major hormonal shield that normally protects the energy factories (mitochondria) inside muscle cells. This loss accelerates fat storage and muscle wasting.
The Bottom Line: It highlights a highly specific, critical time in life when women should proactively screen for muscle loss. Large-scale human trials on how to medically prevent this specific hormonal trigger are still limited.
A Perfect Storm of Aging Hormones (Minnetti et al., 2026)
The Science: It isn't just one hormone causing the issue. Age-related drops in growth hormone, testosterone, and estrogen work together alongside insulin resistance to create a severe body imbalance that favors fat storage over muscle building.
The Bottom Line: Reversing the condition requires looking at your overall metabolic health rather than looking for a single "magic bullet" hormone fix.
The Promise of a Simple Blood Test (Chobolová et al., 2026)
The Science: Scientists discovered specific genetic markers (microRNAs) floating in the blood that are uniquely present in people with sarcopenic obesity.
The Bottom Line: This could eventually lead to a quick, inexpensive screening blood test, skipping the need for complex body scans. However, because this was a tiny pilot study, it must be validated in much larger human groups before doctors can use it.
Plant Compounds and Gut Health (Feng et al., 2026)
The Science: An animal study showed that supplementing a high-fat diet with plant sterols (phytosterols) fixed damaged muscle cells and favorably reshaped the gut microbiome.
The Bottom Line: It proves the "gut-muscle axis" is a real and exciting area of health. But because it was tested only on rodents, we do not yet know the correct, safe human doses or if it will yield the same benefits in people.
The Science is Moving Rapidly (Zhang et al., 2025)
The Science: A data analysis tracking medical papers showed that global research into nutrition and exercise for sarcopenic obesity has exploded exponentially since 2018.
The Bottom Line: This confirms that while the medical community is treating this as a high-priority health crisis, many of the specific dietary "rules" we have today are still new and will continue to evolve
How to Reverse Sarcopenic Obesity: A Practical Protocol
The consistent, well-supported finding across the literature — far more robust than any single supplement claim — is that combined resistance training and adequate protein intake is the most evidence-backed intervention for sarcopenic obesity. Here's how to apply it.
Step 1: Prioritize Resistance Training (Not Just Cardio)
Aim for 2–3 resistance training sessions per week, targeting all major muscle groups
Include compound movements: squats, rows, presses, and hip hinges (using bodyweight, bands, or weights based on ability)
Progressive overload matters more than the specific exercise — gradually increase resistance, reps, or sets over time
Step 2: Hit Your Protein Target
General target for older adults at risk of sarcopenia: 1.2–1.6 g of protein per kg of body weight per day (higher than the standard RDA for younger, healthy adults)
Distribute protein across meals (roughly 25–30g per meal) rather than concentrating it at dinner, since muscle protein synthesis responds better to evenly spaced intake
Prioritize leucine-rich sources (dairy, eggs, poultry, fish, legumes) which more strongly stimulate the muscle-building (mTOR) pathway
Step 3: Create a Modest, Not Aggressive, Calorie Deficit (If Weight Loss Is a Goal)
Aggressive caloric restriction without resistance training risks losing more muscle than fat — worsening sarcopenic obesity even as the scale goes down
A modest deficit (around 300–500 kcal/day) combined with high protein intake and resistance training better preserves lean mass during fat loss
Step 4: Address Inflammation Through Diet Pattern, Not Single Foods
Emphasize a Mediterranean-style eating pattern: vegetables, fruit, legumes, whole grains, olive oil, fatty fish
Limit ultra-processed foods and added sugars, which are associated with higher inflammatory markers
Adequate omega-3 intake (fatty fish 2x/week, or supplementation if dietary intake is low) has reasonable supporting evidence for reducing inflammatory load, though it should complement — not replace — resistance training
Step 5: Don't Neglect Sleep and Stress
Poor sleep is independently associated with reduced muscle protein synthesis and increased cortisol-driven fat storage
Aim for 7–9 hours of consistent sleep; chronic short sleep undermines both legs of the resistance-training-plus-protein strategy above
A Sample Weekly Framework
Monday: Full-Body (Lower Body Focus)
The Action: Focus your energy on major lower body movements like squats, glute bridges, or leg presses, while still doing a few light upper body exercises.
The Purpose: Rebuilding the large muscles in your legs and hips provides the biggest metabolic boost for blood sugar control and fat loss.
Tuesday: Cardio & Protein Nutrition
The Action: Go for a brisk walk, a steady bicycle ride, or light swimming. Pair this with a conscious effort to hit your targeted protein intake at every meal.
The Purpose: Light cardio burns extra calories and improves heart health without overtaxing your muscles while they recover from Monday's workout.
Wednesday: Full-Body Strength (Upper Body Focus)
The Action: Prioritize your upper body with pushing and pulling movements like chest presses, rows, or resistance band pull-aparts, rounded out with a light core or lower body exercise.
The Purpose: Maintaining upper body strength preserves your posture, protects your joints, and ensures you can easily perform everyday functional tasks like lifting groceries.
Thursday: Active Recovery & Flexibility
The Action: Avoid heavy lifting and intense cardio. Instead, dedicate 15 to 30 minutes to gentle stretching, yoga, or basic mobility exercises.
The Purpose: This keeps your blood circulating to soothe sore tissues and improves your joint range of motion, preparing your body for the final workout of the week.
Friday: Full-Body Strength (Compound Multi-Joint Lifts)
The Action: Focus on "compound movements" that recruit multiple muscle groups at the exact same time, such as deadlifts (or hip hinges), overhead presses, and rows.
The Purpose: Working multiple muscle groups simultaneously triggers a higher natural release of muscle-building signals and maximizes your time efficiency.
Saturday: Optional Cardio & Nutrition Prep
The Action: Enjoy some light, optional movement (like a casual hike or walk) and use some free time to batch-cook high-protein meals for the upcoming week.
The Purpose: Pre-cooking your chicken, fish, or beans on Saturday prevents you from reaching for low-protein, ultra-processed convenience foods when you are busy during the week.
Sunday: Deep Rest & Sleep Prioritization
The Action: Take the day completely off from formal exercise. Focus entirely on relaxing and keeping a strict bedtime to secure 7 to 9 hours of quality sleep.
The Purpose: Muscles do not grow while you are working out; they grow while you sleep. Missing out on deep rest actively spikes stress hormones that break down muscle and store fat.
Safety note: If you are over 65, have existing cardiovascular disease, joint conditions, or are new to resistance training, consult your doctor or a qualified physical therapist before starting a new exercise program. If you have kidney disease, talk to your physician before increasing protein intake, since recommendations differ for those with impaired kidney function.
Emerging Therapies: Phytosterols, microRNAs, and Beyond
It's worth separating what's promising from what's proven.
Circulating microRNAs as biomarkers. A 2026 pilot study in Biomedicines (Chobolová et al.) screened for candidate circulating microRNAs that might distinguish people with sarcopenic obesity from those without. This kind of biomarker research could eventually lead to a simple blood test for early detection — which would be a major advance over today's reliance on DEXA scans and grip-strength testing. However, as a pilot screening study, the findings need replication in larger, independent populations before any diagnostic test could be considered reliable.
Phytosterols and the gut-muscle axis. As discussed above, the 2026 Journal of Future Foods study on phytosterols showed improved mitochondrial dynamics and microbiota changes in a high-fat-diet animal model of sarcopenic obesity. The gut-muscle axis is a genuinely active and credible area of nutrition science, but readers should treat phytosterol supplementation as an area to watch, not a substitute for resistance training and adequate protein — which remain the highest-confidence interventions available today.
Where the research field is heading. A 2025 bibliometric analysis in Frontiers in Nutrition (Zhang et al.) mapped the explosive growth in sarcopenic obesity research output, particularly around nutrition and exercise interventions, since roughly 2018. This kind of trend analysis is useful context: it confirms that the science is moving fast, but it also means today's "emerging" findings will be refined — and sometimes overturned — within the next few years. Treat single-study supplement claims with appropriate caution until they're confirmed by independent human trials.
Common Myths & Mistakes
Myth 1: "If my BMI is normal, I don't need to worry about this." False. Sarcopenic obesity can occur at a normal BMI. Body composition matters more than the number on the scale.
Myth 2: "Cardio alone will fix it." Cardio supports cardiovascular health and fat loss but does not adequately stimulate muscle protein synthesis. Resistance training is non-negotiable for reversing sarcopenic obesity.
Myth 3: "Aggressive dieting is the fastest fix." Rapid, severe calorie restriction without resistance training and adequate protein often accelerates muscle loss, making the underlying problem worse even as weight drops.
Myth 4: "This only affects very elderly or frail people." Risk factors and early muscle decline can begin in midlife, particularly around menopause, well before someone would be considered "elderly."
Myth 5: "A specific supplement (collagen, a single amino acid, a trendy compound) can replace exercise." No current supplement, including promising candidates like phytosterols, has human clinical evidence strong enough to replace resistance training and total protein intake as the foundation of treatment.
Frequently Asked Questions
1. Can you have sarcopenic obesity and not know it? Yes. Because standard check-ups often rely on BMI and a basic scale weight, sarcopenic obesity frequently goes undiagnosed, especially in people who appear normal-weight or only mildly overweight.
2. What's the difference between sarcopenia and sarcopenic obesity? Sarcopenia is muscle mass and strength loss alone. Sarcopenic obesity is that same muscle loss occurring alongside excess body fat, with the two conditions actively worsening each other through inflammatory and hormonal crosstalk.
3. Is sarcopenic obesity reversible? Yes, to a meaningful degree. Resistance training combined with adequate protein intake has consistently been shown to improve muscle mass, strength, and function, even in older adults. Full reversal to "ideal" body composition isn't guaranteed for everyone, but functional improvement is achievable for most people.
4. What blood tests or scans diagnose sarcopenic obesity? There's no single confirmed blood test yet (microRNA biomarkers are still in early research). Diagnosis typically combines a body composition scan (DEXA or BIA) with a grip-strength test and/or gait speed assessment.
5. Does menopause cause sarcopenic obesity? Menopause doesn't directly cause it, but the drop in estrogen during the menopausal transition removes a hormonal signal that helps protect muscle mitochondrial function, which raises the risk significantly during this period.
6. How much protein do I need if I have sarcopenic obesity? Most research-based recommendations for older adults at risk fall in the range of 1.2–1.6 grams of protein per kilogram of body weight per day, spread across multiple meals — higher than general population guidelines.
7. Can GLP-1 medications (like semaglutide) cause sarcopenic obesity? Rapid weight loss from any method, including GLP-1 medications, can disproportionately reduce lean muscle mass if resistance training and adequate protein intake aren't included alongside the medication. This is an active area of clinical concern and ongoing research.
8. Is walking enough exercise to fix sarcopenic obesity? Walking supports cardiovascular health and general activity levels but does not provide sufficient mechanical stimulus to build or preserve muscle mass on its own. Resistance training is needed in addition to walking.
9. What foods should I avoid with sarcopenic obesity? There's no single "forbidden" food, but minimizing ultra-processed foods and added sugars supports lower inflammatory markers, which may help reduce the inflammatory drivers of muscle-fat crosstalk.
10. Are extracellular vesicles or microRNA tests available to the public yet? No. These remain research tools at this stage. They are promising avenues for future diagnostic blood tests but are not yet validated or available as a standard clinical test.
11. How common is sarcopenic obesity in older adults? Estimates vary widely (roughly 5% to over 25%) depending on which diagnostic criteria a study uses, which is an important limitation to keep in mind when comparing statistics from different sources.
12. Should I see a doctor or a trainer first? If you have existing health conditions or haven't exercised in a long time, start with a doctor's evaluation, ideally including a body composition assessment and grip-strength test, before beginning a structured resistance training program.
Conclusion & Action Steps
Sarcopenic obesity sits at the intersection of two conditions doctors have historically treated separately — and that gap is exactly why it's so often missed. The science is increasingly clear: fat tissue and muscle tissue are in constant biochemical communication, and when that communication turns inflammatory, both tissues suffer.
The good news is that the most effective intervention isn't an expensive or exotic one. Resistance training plus adequate, well-distributed protein intake remains the best-supported strategy, while emerging tools like microRNA biomarkers and phytosterol-based nutrition science continue to develop in the background.
Your next steps:
Ask your doctor about a body composition scan and grip-strength test — don't rely on BMI alone.
Add 2–3 resistance training sessions to your week, even if you start with bodyweight exercises.
Calculate your target protein intake (1.2–1.6 g/kg body weight) and distribute it across meals.
If you're in perimenopause or menopause, flag this proactively with your healthcare provider — don't wait for symptoms to become obvious.
Reassess your body composition every 3–6 months to track real progress, not just scale weight.
This isn't a condition you have to simply accept as an inevitable part of aging. With the right combination of consistent strength training, sufficient protein, and informed monitoring, the underlying biology can be meaningfully shifted in your favor.
Author's Note: A Clinician's Perspective
As a physician, one of the most common misconceptions I encounter is the belief that body weight alone reflects health. Many patients are reassured when their BMI falls within a "normal" range, yet some of the highest-risk individuals I see have quietly lost significant muscle mass while accumulating visceral fat. The scale often fails to reveal this hidden metabolic deterioration.
Sarcopenic obesity represents a shift in how we should think about aging. It is not simply a matter of carrying excess weight or losing muscle over time. Rather, it is a complex biological condition in which muscle and fat tissue engage in dysfunctional communication, creating a cycle of inflammation, insulin resistance, declining strength, and worsening metabolic health.
I often explain to patients that muscle is far more than a tissue that helps us move. It is a powerful metabolic organ that influences blood sugar control, energy expenditure, immune function, and healthy aging. When muscle mass and strength decline, the consequences extend far beyond physical appearance.
One patient who illustrates this well was a 67-year-old woman who came to clinic concerned about increasing fatigue and difficulty climbing stairs. Her BMI was 24.8 kg/m², placing her within the normal weight range. Because her weight appeared acceptable, she assumed aging was the only explanation for her symptoms. However, body composition analysis revealed significant loss of skeletal muscle mass accompanied by excess visceral fat accumulation. Her grip strength was below the expected range for her age, and laboratory testing showed worsening insulin resistance.
Rather than focusing solely on weight loss, we implemented a structured resistance-training program three times weekly, increased her daily protein intake, and emphasized adequate sleep and physical activity. Six months later, her strength had improved substantially, mobility was better, and her metabolic markers had moved in a healthier direction. Most importantly, she regained confidence in her ability to remain active and independent.
Cases like this remind us that successful aging is not defined by what the scale says. Preserving muscle mass and function may be one of the most important investments we can make in long-term health. For many adults, especially after midlife, the goal should not simply be to lose weight—it should be to build and maintain muscle while reducing excess body fat.
The encouraging message from current research is that sarcopenic obesity is not an inevitable consequence of aging. With evidence-based resistance training, adequate protein intake, and proactive monitoring of body composition, meaningful improvements are achievable at virtually any age.
This article is for educational purposes and does not replace personalized medical advice. Please consult your physician before beginning any new exercise or nutrition program, particularly if you have existing health conditions.
References
Seliem, M., & Ragab, M. (2026). Molecular and cellular mechanisms of muscle–adipose tissue crosstalk driving sarcopenic obesity: an integrative review of human, animal, and in vitro models. Nutrition & Metabolism, 23, 57. https://doi.org/10.1186/s12986-026-01123-2
Park, M. J., & Choi, K. M. (2023). Interplay of skeletal muscle and adipose tissue: Sarcopenic obesity. Metabolism, 144, 155577. https://doi.org/10.1016/j.metabol.2023.155577
Macleod, M., Price, J., Tsonou, E., Baker, D., Tsintzas, K., & Jones, S. (2025/2026). Adipose-derived extracellular vesicles and intercellular crosstalk with skeletal muscle: Implications for sarcopenic obesity and metabolic dysregulation. Obesity Reviews, 27(1), e70005. https://doi.org/10.1111/obr.70005
Zhang, W., Wu, Q., Chen, Q., Qin, W., Zhang, D., Xu, Q., Han, P., & Sun, J. (2026). Adipose-muscle crosstalk during the menopausal transition: Mechanistic links to sarcopenic obesity in midlife women. Frontiers in Endocrinology, 17, 1805067. https://doi.org/10.3389/fendo.2026.1805067
Minnetti, M., Poggiogalle, E., Frigerio, F., Piciocchi, C., Pierantozzi, G., Di Vincenzo, O., ... Donini, L. M. (2026). Endocrinological aspects of sarcopenic obesity. Annals of Medicine, 58(1). https://doi.org/10.1080/07853890.2026.2626085
Chobolová, N., Švagera, Z., Stejskal, D., & Bužga, M. (2026). Candidate circulating microRNAs in patients with sarcopenic obesity: Results of a pilot screening. Biomedicines, 14(6), 1377. https://doi.org/10.3390/biomedicines14061377
Zhang, G., Hu, J., Chen, C., Zhu, W., Chen, Y., Cheng, Y., Hu, W., & Rao, Z. (2025). Research trends in nutrition and exercise for sarcopenic obesity: A bibliometric analysis. Frontiers in Nutrition, 12, 1615101. https://doi.org/10.3389/fnut.2025.1615101
Feng, Z., Xia, J., ... & Sun, G. (2026). Phytosterols ameliorate high-fat diet-induced sarcopenic obesity and skeletal muscle mitochondrial dynamics dysfunction via intestinal microbiota reshaping. Journal of Future Foods. Advance online publication. https://doi.org/10.1016/j.jfutfo.2025.12.042
Jang, S. Y., & Choi, K. M. (2025). Impact of adipose tissue and lipids on skeletal muscle in sarcopenia. Journal of Cachexia, Sarcopenia and Muscle, 16(4), e70000. https://doi.org/10.1002/jcsm.70000
Wei, S., Nguyen, T. T., Zhang, Y., Ryu, D., & Gariani, K. (2023). Sarcopenic obesity: Epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Frontiers in Endocrinology, 14, 1185221.
Bellanti, F., Romano, A. D., Lo Buglio, A., Castriotta, V., Guglielmi, G., Greco, A., et al. (2018). Oxidative stress is increased in sarcopenia and associated with cardiovascular disease risk in sarcopenic obesity. Maturitas, 109, 6–12.
Evans, K., Abdelhafiz, D., & Abdelhafiz, A. H. (2021). Sarcopenic obesity as a determinant of cardiovascular disease risk in older people: A systematic review. Postgraduate Medicine, 133, 831–842.
Luo, Y., Wang, Y., Tang, S., Xu, L., Zhao, X., Han, M., et al. (2024). Prevalence of sarcopenic obesity in the older non-hospitalized population: A systematic review and meta-analysis. BMC Geriatrics, 24, 357.
Zou, Y.-Y., Chen, Z.-L., Sun, C.-C., Yang, D., Zhou, Z.-Q., Xiao, Q., et al. (2022). A high-fat diet induces muscle mitochondrial dysfunction and impairs swimming capacity in zebrafish: A new model of sarcopenic obesity. Nutrients, 14(9), 1975.
Choi, K. M. (2016). Sarcopenia and sarcopenic obesity. Endocrinology and Metabolism (Seoul), 28(2), 86.
Kim, T. N., et al. (2009). Prevalence of sarcopenia and sarcopenic obesity in Korean adults: The Korean Sarcopenic Obesity Study. International Journal of Obesity, 33, 885.
World Health Organization. Obesity and overweight fact sheet. who.int.
National Institute on Aging. What do we know about healthy aging and muscle mass? nia.nih.gov.