Phytosterols for Cholesterol: 8 Evidence-Based Clinical Facts on LDL Reduction and Heart Health
Learn how phytosterols lower LDL cholesterol, ideal dosing, timing, limits, and when they should (and shouldn’t) replace medical therapy.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/20/202622 min read
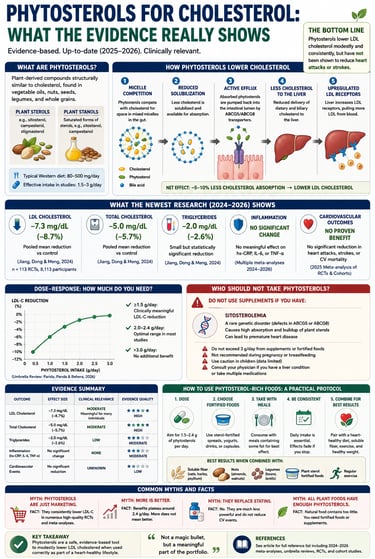
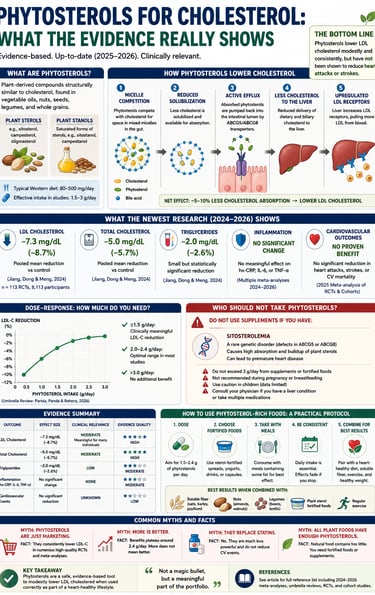
Phytosterols are plant-derived compounds that help lower LDL ("bad") cholesterol by competing with cholesterol for absorption in the small intestine. Research shows that consuming approximately 2 grams per day can reduce LDL cholesterol by about 8–10%. While their cholesterol-lowering effect is well established, large randomized trials have not yet demonstrated a reduction in heart attacks or stroke risk.
How Do Phytosterols Lower Cholesterol?
Compete with cholesterol in intestinal micelles.
Reduce cholesterol absorption from the gut.
Decrease cholesterol delivery to the liver.
Increase liver LDL receptor activity.
Lower blood LDL cholesterol by about 8–10%.
Most effective dose: ~2 g/day for at least 8 weeks.
Key takeaways.
1. Do phytosterols lower LDL cholesterol?
Yes, plant sterols and stanols can effectively lower your LDL "bad" cholesterol by roughly 8% to 10%. While phytosterols provide a clinically proven, natural reduction in cholesterol levels, their overall effect is modest compared to prescription lipid-lowering medications like statins.
2. What is the recommended daily dosage for phytosterols?
To achieve measurable cholesterol-lowering benefits, clinical studies show you need a daily target dose of 2 grams. Because natural foods like unfortified nuts, seeds, and vegetables provide only trace amounts, most people require fortified foods (like spreads and yoghurts) or high-quality supplements to reach this therapeutic dosage.
3. When is the best time to take phytosterols?
For maximum efficacy, you should take phytosterols with meals that contain dietary fat. Because plant sterols work directly inside your digestive tract to block cholesterol absorption, their active mechanism depends on the presence of fats in your stomach during a meal.
4. How long does it take for plant sterols to work?
You should expect measurable changes in your blood lipid levels after 8 to 12 weeks of consistent daily use. To accurately track your personal response to the supplement, schedule a baseline lipid panel blood test before you begin and a follow-up test after 2 to 3 months.
5. Do phytosterols lower triglycerides or C-reactive protein (CRP)?
No. Peer-reviewed research indicates that phytosterols do not reliably lower triglycerides or reduce high-sensitivity C-reactive protein (hs-CRP) inflammation markers. Their primary medical benefit is strictly isolated to reducing total cholesterol and low-density lipoprotein (LDL) particles.
6. Can plant sterols replace statin medications?
No, phytosterols are designed to be a complementary aid, not a natural substitute for prescription cholesterol medications. While plant sterols reduce LDL by up to 10%, statins typically lower it by 30% to over 50%. If your doctor has prescribed a statin, discuss using phytosterols as a safe add-on therapy instead of stopping your medication.
7. What are the side effects and contraindications of phytosterols?
The primary medical contraindication for plant sterols is a rare genetic condition called sitosterolemia, which causes the body to dangerously over-absorb plant fats. If you have a history of unexplained early cardiovascular disease or physical fat deposits (xanthomas), consult a physician before using these products.
8. What happens if you take too much phytosterol?
Consuming more than 2 to 3 grams of phytosterols per day results in a therapeutic plateau, meaning higher doses will not offer extra heart health benefits or further lower your numbers. To get the best value and absorption out of your daily 2-gram dose, split it evenly across your two largest meals of the day.
Introduction
If you've been told to add "plant sterols" or "phytosterol-fortified" margarine to your diet to fight high cholesterol, you've probably also wondered: does this actually work, or is it just clever food marketing?
It's a fair question. Phytosterols have been added to spreads, yogurt drinks, and supplements for more than two decades, and the claims on the packaging can sound almost too good to be true.
Here's the short, honest answer up front: phytosterols do lower LDL cholesterol, the effect is real and reproducible, but it is modest, it depends heavily on dose and consistency, and it has not been shown to reduce heart attacks or strokes in long-term trials. The lipid data are strong. The hard-outcome data are not yet there.
In this guide, we'll walk through exactly what phytosterols are, what the 2024–2026 systematic reviews and meta-analyses actually found, how to interpret those numbers in a clinically meaningful way, who should use them, who should avoid them, and how to use them correctly if you decide to try them.
By the end, you'll know:
What phytosterols are and how they lower cholesterol at a mechanistic level
The actual numbers from the newest meta-analyses (not just "may help lower cholesterol")
Why the effect on inflammation and triglycerides is much weaker than the effect on LDL-C
The one population that should never take phytosterol supplements
A practical, evidence-based protocol for using phytosterol-rich foods correctly
What Are Phytosterols?
Phytosterols are plant-derived compounds that are structurally almost identical to cholesterol, differing by only a side chain or double bond. They occur naturally — though in fairly small amounts — in vegetable oils, nuts, seeds, legumes, and whole grains.
There are two main categories:
Plant sterols (e.g., sitosterol, campesterol, stigmasterol)
Plant stanols (the saturated forms of sterols, e.g., sitostanol, campestanol)
Both work through essentially the same mechanism and are usually discussed together under the umbrella term "phytosterols."
A typical Western diet provides somewhere between roughly 80 and 500 mg of phytosterols per day from food alone, an amount too small to meaningfully change LDL cholesterol. That's why most of the research — and most of the products marketed for cholesterol management — use fortified foods or supplements that supply 1.5–3 grams per day, several times what a normal diet provides (Hui and colleagues, as cited in product literature; AbuMweis and colleagues, 2009; reviewed in Parida, Panda, and Behera, 2026).
This distinction matters enormously for interpreting headlines. "Eating more nuts and vegetable oil" and "taking a 2 g/day phytosterol supplement or fortified spread" are not the same intervention, and they don't produce the same magnitude of effect.
The Mechanism: How Phytosterols Lower Cholesterol
Phytosterols lower LDL cholesterol primarily by competing with dietary and biliary cholesterol for absorption in the small intestine — not by acting on the liver directly.
Here's the step-by-step mechanism, in plain terms:
Micelle competition. In the gut, cholesterol needs to be packaged into tiny fat-and-bile-acid particles called mixed micelles before it can be absorbed. Phytosterols compete for space in these micelles because they're chemically so similar to cholesterol.
Reduced cholesterol solubilization. Because phytosterols are less efficiently absorbed than cholesterol but occupy the same micelle "real estate," less dietary and biliary cholesterol actually gets dissolved and made available for uptake.
Active efflux back into the gut. Any phytosterols that do get absorbed by intestinal cells are mostly pumped straight back out into the intestinal lumen by transporter proteins called ABCG5 and ABCG8 (the same transporters that, when defective, cause the rare disease sitosterolemia — more on that later).
Compensatory LDL receptor upregulation. With less cholesterol arriving from the gut, the liver senses reduced cholesterol delivery and modestly upregulates LDL receptors on its surface, pulling more LDL particles out of the bloodstream to compensate.
The net effect: roughly 5–10% less dietary cholesterol absorption, translating into a measurable, if moderate, drop in circulating LDL-C (Jiang, Dong, and Meng, 2024; Parida, Panda, and Behera, 2026).
Animal and mechanistic studies also point to secondary effects on oxidative stress and membrane lipid composition. A 2025 study in Molecular Nutrition & Food Research by Gao, Pan, Xia, and colleagues reported that combining phytosterols with phospholipids produced synergistic improvements in lipid metabolism and markers of oxidative stress in both animal models and human randomized trials — suggesting the delivery format (phytosterols alone vs. phytosterols co-formulated with phospholipids) may influence how much benefit you actually get, not just the dose.
What the Newest Research Actually Shows
Let's get into the actual data, because this is where most articles on this topic get vague. We're going to be specific about effect sizes, confidence intervals, and — critically — heterogeneity, because heterogeneity tells you how much you should trust a pooled number.
The 2025 Frontiers in Pharmacology Meta-Analysis (Zhang et al.)
This is one of the most recent and most directly relevant meta-analyses specifically in hyperlipidemic patients (people who already have elevated cholesterol, not healthy volunteers). Published July 2025, it pooled 14 randomized controlled trials with 1,088 participants, searched across nine databases through February 2025, and used the Cochrane Risk of Bias tool for quality appraisal.
The pooled results:
Total cholesterol (TC): mean difference of −0.65 mmol/L (95% CI: −0.83 to −0.47), p < 0.00001
LDL-C: mean difference of −0.52 mmol/L (95% CI: −0.66 to −0.38), p < 0.00001
HDL-C: a small but statistically significant increase, MD = 0.08 mmol/L
Triglycerides: a borderline reduction, MD = −0.24 mmol/L (95% CI: −0.47 to −0.01), p = 0.04
C-reactive protein (CRP, inflammation marker): no significant effect
Here's the part that matters most for interpreting this honestly: the TC analysis showed substantial heterogeneity (I² = 86%, p < 0.00001). That's a statistical red flag meaning the individual trials disagreed with each other a great deal — likely due to differences in dose, food matrix (milk vs. spread vs. capsule), population, and trial duration. The authors specifically noted that intervention duration affected TC reduction independent of dose, while dose itself did not show a clear dose-response relationship with TC change in their pooled data — a somewhat unusual finding that runs counter to most other phytosterol literature (more on that below) and likely reflects the heterogeneity in the included trials rather than a true absence of dose-dependency.
The authors' own conclusion was appropriately cautious: phytosterol-rich foods meaningfully improve TC and LDL-C and modestly raise HDL-C in people with hyperlipidemia, but they found no anti-inflammatory effect on CRP, and the small triglyceride benefit should be interpreted cautiously given the heterogeneity. They explicitly called for larger, metabolomics-inclusive trials before drawing firm clinical conclusions (Zhang, Zhang, Wang, Jia, Niu, Ding, and Li, 2025).
The 2026 Umbrella Review (Zurbau, Sievenpiper, and Colleagues)
An umbrella review is a "review of reviews" — it pools findings across multiple existing systematic reviews and meta-analyses rather than individual trials, giving a higher-level, more stable estimate of the evidence base as a whole. This is one of the strongest forms of evidence we have for a nutrition question, and the 2026 paper in Clinical Nutrition by Zurbau, Haintz, Chen, Glenn, Kavanagh, Oguntala, Blanco Mejia, Khan, Leiter, Kendall, Chiavaroli, and Sievenpiper updated the dose-response relationship for phytosterols across cardiometabolic risk factors using randomized trial data.
This body of work builds on earlier dose-response modeling, including a widely cited continuous dose-response analysis showing that at a typical dose of about 2.15 g/day, phytosterols lower LDL-C by roughly 0.34 mmol/L, or about 8.8%, with higher baseline LDL-C predicting a larger absolute reduction — meaning the people who need it most tend to benefit the most in absolute terms.
Earlier Umbrella Reviews Confirm the Pattern
Two other recent umbrella reviews reinforce the same general picture. A 2024 critical umbrella review in Phytotherapy Research, pooling 17 meta-analyses across 23 study arms, found:
LDL-C: −11.47 mg/dL (95% CI: −12.76 to −10.17)
Total cholesterol: −13.02 mg/dL (95% CI: −15.68 to −10.37)
Triglycerides: −3.77 mg/dL (95% CI: −6.04 to −1.51)
HDL-C: no significant change (0.18 mg/dL, 95% CI: −0.13 to −0.51)
Notably, this review found the effect was concentrated in trials using ≥2 g/day for ≥8 weeks in hypercholesterolemic populations — almost an exact echo of the original National Cholesterol Education Program (NCEP) recommendation from decades ago.
Cohort Evidence: The UK Biobank Study
Trials tell you what happens under controlled conditions; cohort studies tell you what's associated with real-world habitual intake over years. The 2025 UK Biobank analysis by Qiao, Feng, Zhang, Zhang, Yang, Wu, Xie, Huang, Zhou, and Zhang, published in Food & Function, followed 167,209 participants using repeated 24-hour dietary recalls, comparing the highest to lowest quintiles of habitual dietary phytosterol intake.
The findings were notably favorable:
Cardiovascular mortality: hazard ratio 0.86 (95% CI: 0.80–0.94)
Coronary heart disease: hazard ratio 0.91 (95% CI: 0.84–0.98)
Stronger protective associations were seen in current smokers, people with lower BMI, and those with moderate-to-high physical activity
This is genuinely encouraging, but it's important to be precise about what kind of evidence this is: this is an observational association, not a randomized trial of supplementation. People who eat more naturally phytosterol-rich foods (nuts, seeds, vegetable oils, whole grains) are also more likely to have generally healthier diets and lifestyles overall. The authors did adjust for several confounders and ran sensitivity analyses excluding early events, which strengthens confidence in the association, but it cannot establish that phytosterols themselves caused the lower risk. Cohort data like this should be read as supportive and hypothesis-generating, not as proof of a causal cardioprotective effect of supplemental phytosterols.
Interpreting the Numbers: Clinical Relevance vs. Statistical Significance
This is the section that most "phytosterol" articles skip entirely, and it's the most important one for actually deciding whether this matters for your health.
A statistically significant result is not automatically a clinically meaningful one. With enough participants, even a tiny, irrelevant difference can reach statistical significance. So let's translate the numbers above into something you can actually use.
Is an 8–10% LDL-C reduction clinically meaningful?
Generally, yes — within context. For comparison:
Intervention Typical LDL-C reduction Statin therapy (moderate-intensity) 30–50% Statin therapy (high-intensity) ≥50% Ezetimibe ~15–20% Phytosterols (2 g/day) ~8–10% Soluble fiber (e.g., psyllium, 10 g/day) ~5–10% Plant-based "Portfolio Diet" (combining several of the above) ~20–30%
So phytosterols sit in roughly the same range as soluble fiber — a real but modest effect, well below what a statin delivers. The American Heart Association and most national guidelines treat phytosterols as a useful adjunct for diet-based LDL-C lowering, not a substitute for pharmacologic therapy in people who need substantial reductions (e.g., those with established cardiovascular disease or very high baseline LDL-C).
Where the effect is most clinically relevant
The evidence is most convincing, and most clinically actionable, in three specific scenarios:
Mild-to-moderate primary hyperlipidemia, where a patient and clinician are trying to avoid or delay statin initiation through lifestyle measures
As an add-on to statin therapy, where phytosterols have been shown in several trials to provide incremental LDL-C lowering — some research suggests an effect comparable to doubling a statin dose, without the dose-related side effects
As part of a combined dietary strategy (the "Portfolio Diet" approach — combining phytosterols, soluble fiber, plant protein, and nuts), where the cumulative effect on LDL-C becomes substantially larger and approaches what a low-dose statin might achieve
Where the evidence runs thin
Hard cardiovascular outcomes (heart attack, stroke, cardiovascular death) have not been directly tested in long-duration randomized outcome trials of phytosterol supplementation. The reductions in LDL-C are a strong surrogate marker — LDL-C lowering by other means (statins, PCSK9 inhibitors) reliably reduces cardiovascular events — but a surrogate marker improvement is not the same as proven outcome benefit specifically for phytosterols.
Inflammatory markers (CRP). As the 2025 Zhang meta-analysis found, there is currently no convincing evidence that phytosterol-rich foods reduce CRP in people with hyperlipidemia.
Triglycerides. The pooled effect is small, inconsistent across studies, and the available meta-analyses themselves flag high heterogeneity, meaning you shouldn't expect a reliable triglyceride benefit.
Phytosterols and Inflammation: A Weaker Story
Marketing materials and some review articles have promoted phytosterols as having "anti-inflammatory" properties, partly based on mechanistic and animal studies showing reduced markers of oxidative stress (Gao, Pan, Xia, et al., 2025; Zio, Tarnagda, Tapsoba, Zongo, and Savadogo, 2024).
But when it comes to clinical trial evidence in actual patients, the picture is much weaker. The 2025 Frontiers in Pharmacology meta-analysis — specifically designed to test both lipid and inflammatory outcomes in hyperlipidemic adults — found no significant reduction in CRP across the pooled trials.
This is a good example of why it's important to separate three distinct levels of evidence:
Mechanistic/in-vitro evidence (cell studies showing reduced oxidative markers)
Animal model evidence (rodent studies showing improved lipid and oxidative profiles)
Human randomized controlled trial evidence (the gold standard for clinical claims)
Phytosterols have reasonably strong evidence at levels 1 and 2 for anti-inflammatory and antioxidant activity, but the human RCT evidence specifically for inflammatory biomarkers in people with hyperlipidemia is currently insufficient to support a clinical anti-inflammatory claim. This is a meaningful distinction, and it's one reason regulatory bodies have approved phytosterol health claims specifically for cholesterol reduction — not for inflammation.
Dose-Response: How Much Do You Actually Need?
The dose-response relationship for phytosterols and LDL-C is one of the more consistently replicated findings in nutrition science, dating back to controlled feeding studies and confirmed repeatedly in subsequent meta-analyses.
The key reference points:
400 mg/day: minimal to no significant LDL-C effect in controlled feeding studies
~800 mg–1.5 g/day: modest, measurable LDL-C reduction begins
2–2.15 g/day: the most well-studied and most commonly recommended dose, associated with roughly 8–10% LDL-C reduction
2.3 g/day over 6.5 weeks (in familial hypercholesterolemia trials): total cholesterol and LDL-C reductions of 7–11% and 10–15% respectively
>2.5–3 g/day: evidence for additional benefit beyond ~2–2.5 g/day is inconsistent; most reviews describe a plateau effect, where doubling the dose does not double the benefit
This is the single most actionable number in the entire phytosterol literature: roughly 2 grams per day, taken consistently, for at least 8 weeks, is the threshold most associated with a meaningful and reproducible LDL-C reduction. Doses below 1 gram per day from regular food sources alone are unlikely to move the needle much.
It's also worth noting that single vs. multiple daily intakes may matter slightly — pooled dose-response modeling found a statistical trend (p = 0.054) toward slightly lower efficacy when the full daily dose was taken in one sitting rather than split across meals, although this didn't reach strict statistical significance.
Who Should NOT Take Phytosterols
This is the most clinically important safety section in this article, and it deserves to be stated plainly.
Sitosterolemia (Phytosterolemia)
Sitosterolemia is a rare, autosomal recessive genetic disorder caused by mutations in the ABCG5 or ABCG8 genes — the same transporter proteins responsible for pumping phytosterols back out of intestinal cells. People with this condition absorb phytosterols far more efficiently than normal and cannot clear them properly, leading to dramatically elevated blood phytosterol levels.
Clinical features include:
Tendon and skin xanthomas (lipid deposits)
Premature atherosclerosis, even with normal-to-mildly-elevated cholesterol
Hematologic abnormalities, including hemolytic anemia and macrothrombocytopenia in some cases
Joint pain and arthritis in some patients
People with sitosterolemia must strictly avoid phytosterol-fortified foods and supplements. Because the condition is rare and can be under-diagnosed, anyone with an unexplained family history of very early heart disease, unusual xanthomas, or unexplained hemolytic anemia should be evaluated before starting high-dose phytosterol supplementation (Bavli and Ahmad, 2025; Wu, Zhang, Tang, et al., 2026; Linus Pauling Institute, Oregon State University).
Other groups who should use caution
Pregnant or breastfeeding women: Long-term safety data at supplement-level doses in pregnancy is limited; routine dietary intake from whole foods is not a concern, but high-dose fortified products warrant a conversation with your physician.
Children: Most clinical trial data come from adults; pediatric dosing recommendations are less established outside of specific inherited lipid disorders managed by a specialist.
People on fat-soluble vitamin therapy or with malabsorption conditions: Phytosterols can modestly reduce absorption of beta-carotene and other fat-soluble compounds; this is usually manageable by increasing fruit and vegetable intake, but it's worth knowing about.
Evidence Summary
Here is a breakdown of the core findings, populations, and scientific caveats from these landmark phytosterol studies, organized into practical, easy-to-read points:
Clinical Trial Evidence for Blood Lipids (Zhang et al., 2025)
The Study Design: A meta-analysis combining data from 14 randomized controlled trials (RCTs).
The Population: 1,088 adults diagnosed with hyperlipidemia (high cholesterol).
The Main Finding: Plant sterol supplementation significantly lowered total cholesterol (TC) by 0.65 mmol/L and LDL "bad" cholesterol by 0.52 mmol/L.
The Caveats: There was high statistical variation (heterogeneity) across the trials. Furthermore, the treatment had no effect on C-reactive protein (CRP) inflammation markers, and the benefit for triglycerides (TG) was barely borderline.
The Umbrella Review Blueprint (Critical Umbrella Review, 2024)
The Study Design: A massive umbrella review pooling data across 17 different meta-analyses spanning 23 study groups.
The Population: Pooled data representing thousands of individual participants.
The Main Finding: On average, phytosterols lowered LDL-C by 11.47 mg/dL and total cholesterol by 13.02 mg/dL.
The Caveats: The benefits were strictly concentrated in people who already had high cholesterol, and only when they took a dose of 2 grams or more per day for at least 8 weeks.
Gold-Standard Dose Thresholds Verified (Zurbau, Sievenpiper et al., 2026)
The Study Design: A rigorous umbrella review combined with an updated dose-response meta-analysis.
The Population: Multiple pooled randomized controlled trials.
The Main Finding: This paper provides the strongest, highest-level evidence confirming that plant sterols lower LDL-C in a predictable, dose-dependent manner.
The Caveats: It serves as the definitive reference for exactly where the clinical dose thresholds sit to guarantee effectiveness.
Real-World Cardiovascular Outcomes (Qiao et al., 2025)
The Study Design: A large-scale prospective cohort study tracking participants over time.
The Population: 167,209 participants from the UK Biobank database.
The Main Finding: Higher dietary intake of plant sterols was linked to a 14% lower risk of cardiovascular disease (CVD) mortality and a 9% lower risk of coronary heart disease (CHD).
The Caveats: Because this is an observational study rather than a controlled experiment, it can show a strong association but cannot prove that phytosterols directly caused the reduction in heart disease deaths.
The Dosage Efficiency Plateau (Continuous Dose-Response Analysis)
The Study Design: A foundational meta-regression analysis mapping out dosage dynamics.
The Population: Compiled data from over 41 clinical trials.
The Main Finding: Consuming an average daily dose of 2.15 grams of phytosterols results in a reliable 8.8% reduction in LDL cholesterol.
The Caveats: The data clearly confirms a "plateau effect." Raising your daily intake above 2.5 grams yields no additional lipid-lowering benefits, proving that more is not better.Insert table-style infographic here: visually rendering the table above as a comparison chart, with color-coded confidence levels (high/moderate/low certainty) per outcome.
How to Use Phytosterol-Rich Foods: A Practical Protocol
If you and your healthcare provider decide phytosterols are a reasonable addition to your routine, here's an evidence-aligned way to approach it.
Step 1: Get a baseline lipid panel
You can't measure improvement without a starting point. Ask for a full lipid panel (TC, LDL-C, HDL-C, triglycerides) before starting.
Step 2: Choose your source
Fortified foods: Phytosterol-enriched spreads, milk, or yogurt drinks (commonly 1.5–3 g phytosterols per serving)
Supplements: Capsules or chewable tablets, typically standardized to deliver ~1–2 g per dose
Whole-food sources (lower dose, but contribute to overall intake): nuts, seeds, wheat germ, unrefined vegetable oils, legumes
Step 3: Hit the effective dose consistently
Target ~2 grams per day, the most evidence-supported dose
Split the dose across two meals if convenient (may offer a slight edge, based on dose-response modeling)
Take with meals containing some fat, since phytosterols need to be incorporated into the same micelles as dietary fat and cholesterol to compete effectively
Step 4: Give it adequate time — and recheck
Most trials showing significant effects ran 8 weeks or longer
Recheck your lipid panel at 8–12 weeks to see your individual response (responses vary meaningfully between individuals)
Step 5: Combine with other proven LDL-lowering strategies
The biggest realistic wins come from combining strategies, not relying on phytosterols alone:
Replace saturated fat with unsaturated fats
Add 10+ g/day of soluble fiber (oats, psyllium, legumes)
Include a daily source of plant protein (legumes, soy)
Maintain regular physical activity
If already on a statin, ask your prescriber whether phytosterols are appropriate as an add-on — several studies suggest meaningful incremental benefit
Step 6: Don't expect inflammation or triglyceride miracles
Based on current evidence, set your expectations specifically around LDL-C and total cholesterol — not CRP or triglycerides, where the data are weak or inconsistent.
Common Myths and Mistakes
Myth: "More is always better." Reality: Evidence points to a plateau above roughly 2–2.5 g/day. Megadosing doesn't reliably produce proportionally greater LDL-C reduction and may be unnecessary or even create avoidable cost and GI discomfort.
Myth: "Phytosterols work like a statin." Reality: They work through a completely different mechanism (reduced intestinal absorption vs. inhibited hepatic cholesterol synthesis) and produce a much smaller effect size — roughly 8–10% vs. 30–50%+ for statins.
Myth: "If it lowers LDL-C, it must also reduce inflammation and heart attack risk by the same amount." Reality: LDL-C is a strong surrogate marker, but the current trial evidence specifically for phytosterols doesn't show a CRP benefit, and no large outcome trial has directly tested phytosterol supplementation against hard cardiovascular endpoints.
Myth: "Natural means automatically safe for everyone." Reality: People with sitosterolemia can be seriously harmed by phytosterol intake. "Plant-derived" does not equal "risk-free for all individuals."
Myth: "You need a special supplement — food sources don't count." Reality: Fortified foods and food-format interventions (margarine, milk, yogurt drinks) have been used in the large majority of clinical trials and perform comparably to capsules when dosed appropriately.
Mistake: Taking phytosterols without dietary fat. Because the mechanism depends on micelle competition, taking phytosterols with a completely fat-free meal may reduce their effectiveness.
Mistake: Stopping after 2–3 weeks because "nothing changed." Most of the positive trial data required at least 8 weeks of consistent use before meaningful changes appeared.
Frequently Asked Questions
1. Do phytosterols actually lower cholesterol, or is it marketing hype? The lipid-lowering effect is genuine and supported by multiple independent meta-analyses, including a 2025 analysis of 14 randomized trials in hyperlipidemic patients showing significant reductions in total cholesterol and LDL-C. The effect size is modest (roughly 8–10% LDL-C reduction at typical doses), not dramatic, but it is real.
2. How much phytosterol do I need per day to see results? Most of the supporting evidence centers on approximately 2 grams per day, taken consistently for at least 8 weeks. Lower doses (under 1 g/day) generally show minimal effect in controlled trials.
3. Can phytosterols replace my statin? No. Phytosterols produce roughly 8–10% LDL-C reduction, compared to 30% or more with statins. They may be appropriate as a complementary strategy alongside statin therapy or as part of a diet-first approach in people with only mildly elevated cholesterol, but this decision should be made with your physician based on your overall cardiovascular risk.
4. Do phytosterols reduce inflammation? Current human trial evidence does not support a clinically meaningful anti-inflammatory effect, despite promising findings in animal and cell-based research. The most recent relevant meta-analysis found no significant change in CRP.
5. Are phytosterols safe for everyone? No. People with sitosterolemia, a rare genetic disorder affecting ABCG5/ABCG8 transporter function, should strictly avoid phytosterol supplementation, as it can worsen their condition. Most other adults tolerate phytosterols well at standard doses.
6. What foods naturally contain phytosterols? Vegetable oils, nuts, seeds, whole grains, and legumes contain phytosterols naturally, though typically not in amounts large enough (without fortification) to produce the LDL-lowering effects seen in clinical trials.
7. How long before I see a change in my cholesterol numbers? Most clinical trials measuring significant benefit used intervention periods of 8 weeks or longer. A recheck of your lipid panel at 8–12 weeks is a reasonable timeframe to assess your individual response.
8. Do phytosterols help with triglycerides? The evidence here is weak and inconsistent. Some meta-analyses report a small, borderline-significant reduction, but the finding carries substantial statistical heterogeneity and should not be relied upon as a primary benefit.
9. Is there a difference between plant sterols and plant stanols? Both work through the same basic mechanism (reduced intestinal cholesterol absorption) and produce similar magnitude effects on LDL-C in most comparative analyses. The choice between them is largely a matter of product formulation rather than clinical superiority of one over the other.
10. Can I get enough phytosterols from diet alone, without supplements or fortified foods? Generally no, if your goal is a clinically meaningful LDL-C reduction. Typical dietary intake (80–500 mg/day) falls well below the ~2 g/day threshold used in most successful trials. Fortified foods or supplements are usually necessary to reach an effective dose.
11. Do phytosterols interact with medications? Phytosterols can modestly reduce absorption of certain fat-soluble vitamins and carotenoids; this is generally manageable with a varied diet. If you take other lipid-lowering medications, phytosterols are often used as a complementary strategy rather than a conflicting one, but you should still discuss any new supplement with your prescriber or pharmacist.
12. Are there cardiovascular outcome trials, not just cholesterol trials, for phytosterols? Not yet, at least not large-scale, long-duration randomized outcome trials directly testing whether phytosterol supplementation reduces heart attacks or strokes. The evidence base currently rests on lipid biomarker trials and supportive (but non-causal) observational cohort data, such as the 2025 UK Biobank analysis.
Conclusion and Action Steps
Phytosterols are one of the better-supported "food-based" cholesterol interventions in nutrition science — but the honest, evidence-based picture is more nuanced than most marketing copy suggests.
What the science actually supports:
A reproducible, moderate reduction in LDL-C and total cholesterol (roughly 8–10% at ~2 g/day)
A small increase in HDL-C in some analyses
A favorable, though purely observational and non-causal, association with cardiovascular mortality in long-term cohort data
No convincing evidence yet for anti-inflammatory or strong triglyceride-lowering effects in human trials
Your action steps:
Get a baseline lipid panel before starting anything new.
If you don't have sitosterolemia or another contraindication, consider adding ~2 g/day of phytosterols through fortified foods or a supplement, taken with meals containing fat.
Give it at least 8 weeks, then recheck your lipid panel.
Combine it with other proven strategies — fiber, plant protein, exercise, and (if appropriate) medication — rather than relying on phytosterols alone.
Talk to your doctor, especially if you have a family history of very early heart disease or unusual cholesterol patterns, before starting high-dose supplementation.
Phytosterols won't replace medical therapy for significant cardiovascular risk, but for the right person, at the right dose, used consistently, they're a legitimate, evidence-supported tool — not just a label claim.
Related Articles
Plant Protein vs Animal Protein: Can Switching Help You Live Longer? What Research Reveals
Carb Counting vs Low-Carb Diets: Which Controls Blood Sugar Better?
Low-Fat vs Low-Carb: Which Diet Is Best for Weight Loss?
Can a Low-Carb Diet Reverse Metabolic Syndrome? Latest Research Explained
The Best Dietary Fat Balance for Insulin Sensitivity, Inflammation, and Longevity
How Many Carbs Should Diabetics Eat? 2026 Evidence-Based Guidelines for Better Blood Sugar
References
Zhang, Y., Zhang, Q., Wang, X., Jia, Y., Niu, Q., Ding, S., & Li, W. (2025). Effects of phytosterol-rich foods on lipid profile and inflammatory markers in patients with hyperlipidemia: A systematic review and meta-analysis. Frontiers in Pharmacology, 16, 1619922. https://doi.org/10.3389/fphar.2025.1619922
Gao, Y., Pan, D., Xia, J., et al. (2025). Phytosterols and phospholipids synergistically improve lipid metabolism and oxidative stress: Evidence from animal model and human randomized controlled trials. Molecular Nutrition & Food Research, 69(22), e70248. https://doi.org/10.1002/mnfr.70248
Parida, R., Panda, M. K., & Behera, S. K. (2026). Phytosterols: Natural compounds with multifaceted therapeutic potentials – A review. Pharmacological Research – Natural Products, 10, 100586. https://www.sciencedirect.com/science/article/pii/S2950199726000996
Jiang, C., Dong, Z., & Meng, Z. (2024). Artificial preparation, biosynthetic, health effects, and applications of phytosterol and phytosterol ester: A review. Food Bioscience, 59, 104023. https://doi.org/10.1016/j.fbio.2024.104023
Zurbau, A., Haintz, L., Chen, V., Glenn, A. J., Kavanagh, M. E., Oguntala, J. O., Blanco Mejia, S., Khan, T. A., Leiter, L. A., Kendall, C. W. C., Chiavaroli, L., & Sievenpiper, J. L. (2026). Efficacy of phytosterols for reduction of cardiometabolic risk factors: An umbrella review of systematic reviews and meta-analyses and updated dose-response meta-analyses of randomized trials. Clinical Nutrition, 63, 106698. https://doi.org/10.1016/j.clnu.2026.106698
Qiao, W., Feng, H., Zhang, Y.-F., Zhang, Z., Yang, J., Wu, M., Xie, J., Huang, J., Zhou, T., & Zhang, Y. (2025). Protective association between dietary phytosterol intake and cardiovascular health: An analysis of the UK Biobank cohort. Food & Function, 16(3), 1157–1168. https://doi.org/10.1039/D4FO05439C
Zio, S., Tarnagda, B., Tapsoba, F., Zongo, C., & Savadogo, A. (2024). Health interest of cholesterol and phytosterols and their contribution to one health approach: Review. Heliyon, 10(21), e40132. https://doi.org/10.1016/j.heliyon.2024.e40132
Genest, J., et al. (umbrella review). The effect of phytosterol supplementation on lipid profile: A critical umbrella review of interventional meta-analyses. (2024). Phytotherapy Research, 38(2), 507–519. https://doi.org/10.1002/ptr.8052
AbuMweis, S. S., Barake, R., & Jones, P. J. H. (2009). Plant sterols/stanols as cholesterol lowering agents: A meta-analysis of randomized controlled trials. Food & Nutrition Research, 52.
Demonty, I., Ras, R. T., van der Knaap, H. C. M., et al. (2009). Continuous dose-response relationship of the LDL-cholesterol-lowering effect of phytosterol intake. The Journal of Nutrition, 139(2), 271–284. https://doi.org/10.3945/jn.108.095125
Jones, P. J. H., AbuMweis, S. S., et al. Dose effects of dietary phytosterols on cholesterol metabolism: A controlled feeding study. American Journal of Clinical Nutrition. https://pmc.ncbi.nlm.nih.gov/articles/PMC2793103/
Trautwein, E. A., Vermeer, M. A., Hiemstra, H., & Ras, R. T. (2018). LDL-cholesterol lowering of plant sterols and stanols—which factors influence their efficacy? Nutrients, 10(9), 1262.
Bavli, N. R., & Ahmad, Z. (2025). Sitosterolemia due to a new combination of ABCG8 variants presenting as hemolytic anemia and macrothrombocytopenia. JCEM Case Reports. https://doi.org/10.1210/jcemcr/luaf234
Wu, L.-L., Zhang, L., Tang, T.-T., Zhou, Y.-Y., Chang, X.-X., Guo, W., Yan, H.-M., & Lin, H.-D. (2026). Sitosterolemia due to compound heterozygous mutations in ABCG5: A case report. Journal of Medical Case Reports. https://doi.org/10.1186/s13256-025-05814-x
Sabeva, N. S., Liu, J., & Graf, G. A. The ABCG5 ABCG8 sterol transporter and phytosterols: Implications for cardiometabolic disease. (Cited via MedlinePlus Genetics, ABCG5 gene summary, NIH/NLM.)
GeneReviews® (NCBI Bookshelf, NIH). Sitosterolemia. National Library of Medicine.
Linus Pauling Institute, Oregon State University. Phytosterols. Micronutrient Information Center.
Yang, Y., Xia, J., Yu, T., Wan, S., Zhou, Y., & Sun, G. Effects of phytosterols on cardiovascular risk factors: A systematic review and meta-analysis of randomized controlled trials. Phytotherapy Research, 39(1), 3–24. https://doi.org/10.1002/ptr.8308
Zhang, Y.-F., Qiao, W., Feng, H., Jiang, K., Yang, J., Zhou, T., & Zhang, Y. (2024). Effects of phytosterol supplementation on lipid profiles and apolipoproteins: A meta-analysis of randomized controlled trials. Medicine, 103, e40020.
Liu, B., Chen, K., Chen, X., Wang, J., Shu, G., Ping, Z., et al. (2024). Health outcomes associated with phytosterols: An umbrella review of systematic reviews and meta-analyses of randomized controlled trials. Phytomedicine, 122, 155151.
Shen, M., Yuan, L., Zhang, J., Wang, X., Zhang, M., Li, H., Jing, Y., & Zeng, F., Xie, J. (2024). Phytosterols: Physiological functions and potential application. Foods, 13(11), 1754.
Wang, T., Ma, C., Hu, Y., Guo, S., Bai, G., Yang, G., & Yang, R. (2023). Effects of food formulation on bioavailability of phytosterols: Phytosterol structures, delivery carriers, and food matrices. Food & Function, 14(12), 5478–5497.
Zou, X., Xu, T., Zhao, T., Xia, J., Zhu, F., Hou, Y., Lu, B., Zhang, Y., & Yang, X. (2024). Phytosterol organic acid esters: Characterization, anti-inflammatory properties and a delivery strategy to improve mitochondrial function. Current Research in Food Science, 8, 100702.
American Heart Association. Dietary cholesterol and cardiovascular disease guidance (current scientific statements). www.heart.org
National Cholesterol Education Program (NCEP), Adult Treatment Panel III. Recommendations on plant sterol/stanol intake for LDL-cholesterol reduction.
Disclaimer: This article is for general educational purposes only and does not constitute individualized medical advice. Always consult a qualified healthcare provider before starting, stopping, or changing any supplement, medication, or treatment plan — especially if you have a personal or family history of early cardiovascular disease, a known lipid disorder, or are pregnant, breastfeeding, or managing a chronic condition.