Can Correcting Vitamin D Deficiency Improve Testosterone and Erectile Dysfunction? What the Latest Research Really Shows
Can correcting vitamin D deficiency improve testosterone? Explore the science behind hormone health, fertility, and erectile function.
NUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/28/202617 min read
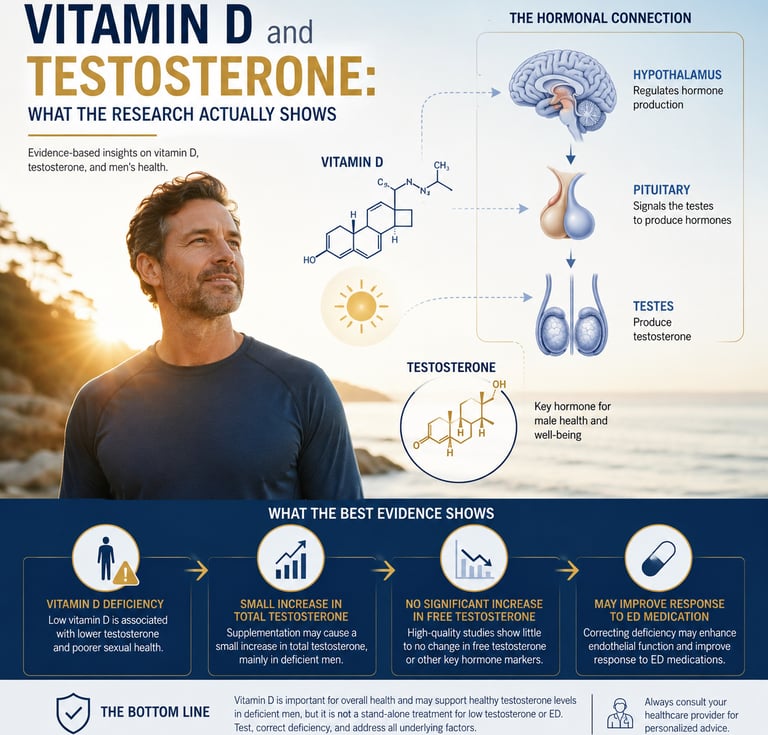
Current evidence suggests vitamin D supplementation may produce a small increase in total testosterone, primarily in men who are vitamin D deficient, but it has little or no effect on free testosterone. High-quality randomized trials indicate vitamin D is best viewed as a supportive therapy for correcting deficiency rather than a reliable treatment for low testosterone or erectile dysfunction.
Key Takeaways: What the Best Evidence Says About Vitamin D and Testosterone
Low vitamin D is consistently linked to lower testosterone, but association is not proof of causation. Men with vitamin D deficiency are more likely to have lower testosterone and erectile dysfunction, yet observational studies cannot determine whether vitamin D is the direct cause or simply a marker of poorer overall health.
Randomized clinical trials show only modest benefits from vitamin D supplementation. The strongest evidence indicates that vitamin D may produce a small increase in total testosterone, but the effect is inconsistent across studies and is generally not large enough to be considered a universal testosterone booster.
Free testosterone—the hormone that matters most clinically—usually does not increase. Despite slight improvements in total testosterone, high-quality meta-analyses show no significant changes in free testosterone, SHBG, LH, FSH, or other major reproductive hormone markers.
Men with vitamin D deficiency benefit the most. The clearest improvements are seen in individuals with serum 25(OH)D levels below approximately 20 ng/mL (50 nmol/L). For men with adequate vitamin D levels, supplementation is unlikely to provide meaningful hormonal benefits.
Vitamin D may improve erectile function indirectly rather than acting as a standalone treatment. Emerging evidence suggests correcting vitamin D deficiency may enhance endothelial health and improve the response to medications such as tadalafil, particularly in deficient men.
More vitamin D is not better. Current research shows no additional hormonal or fertility benefits from doses exceeding 4,000 IU/day, while excessive supplementation increases the risk of vitamin D toxicity and hypercalcemia.
Vitamin D should be viewed as supportive care—not a replacement for evidence-based treatment. Correcting a deficiency is an important part of optimizing health, but persistent low testosterone or erectile dysfunction requires a comprehensive medical evaluation to identify underlying hormonal, metabolic, vascular, or lifestyle factors.
The most evidence-based strategy is simple: test first, supplement only if needed. Measuring serum 25-hydroxyvitamin D [25(OH)D] before starting supplements allows treatment to be targeted to those most likely to benefit, avoiding unnecessary supplementation while supporting both hormonal and overall health.
Introduction
If you've spent any time researching natural ways to support testosterone or sexual function, you've almost certainly run into the claim that vitamin D is a "sunshine hormone" that boosts male hormones and libido. It's a tidy story, and it's partly true — men with low vitamin D do tend to have lower testosterone and more erectile difficulties, on average.
But there's an important distinction that most articles on this topic skip over: an association between low vitamin D and low testosterone is not the same as proof that taking vitamin D will raise your testosterone or fix erectile dysfunction. Correlation studies tell you two things tend to travel together. Only randomized controlled trials (RCTs) — where one group gets vitamin D and a comparable group gets a placebo — can tell you whether supplementing actually causes a benefit.
This article walks through what the highest-quality evidence available as of mid-2026 actually shows, including several systematic reviews and meta-analyses published in the past few months. The honest summary, which we'll unpack in detail: the supplementation evidence is real but modest, inconsistent, and concentrated almost entirely in men who started deficient. If you're already getting enough vitamin D, taking more is unlikely to move the needle on testosterone or sexual performance.
1. The Biological Plausibility: Why Vitamin D Could Matter
Vitamin D doesn't just regulate calcium and bone health. Receptors for vitamin D, and the enzymes that activate it, are present in the testes, the hypothalamus, and the pituitary gland — the entire hormonal chain involved in testosterone production. Vitamin D receptor expression and vitamin D-metabolizing enzymes have been identified in extra-skeletal tissues, including components of the male reproductive tract.
Researchers have proposed several mechanisms by which vitamin D could plausibly influence male sexual health, including effects on steroidogenesis (the process that produces testosterone) and effects on prolactin. Vitamin D has also been described as improving endothelial function by stimulating nitric oxide secretion and release, which plays a role in erection — nitric oxide is the same molecule that erectile dysfunction medications like sildenafil and tadalafil work through.
This is the "why it could work" part of the story, and it's genuinely interesting biology. But plausibility is not proof of effect — plenty of biologically plausible interventions fail to show real-world benefit when tested rigorously. That's exactly why the next two sections separate association from causation.
2. Observational Evidence: The Association Is Real
Cross-sectional and observational studies — the kind that measure vitamin D and testosterone in the same group of men at one point in time — consistently find a positive relationship between the two.
A 2025–2026 review focused specifically on andrology and erectile function patients summarized this pattern: in men with type 2 diabetes, those with hypogonadism had significantly lower vitamin D levels than those with normal testosterone, and cross-sectional data showed a positive association between serum vitamin D and total testosterone concentration.
A German andrology clinic study examining men with symptoms of hypogonadism (testosterone deficiency) was designed specifically to explore whether vitamin D and testosterone interact in their effects on sexual function and quality of life, reflecting how seriously clinicians now take this relationship in real patients, not just trial populations.
Similarly, a 2025 systematic review on vitamin D and erectile dysfunction that pooled data from 10 studies encompassing over 13,000 men found that observational studies consistently showed men with moderate-to-severe or arteriogenic erectile dysfunction had significantly lower serum vitamin D levels and poorer erectile function scores. That's a large, consistent signal across a lot of men.
The catch: this same systematic review was careful to flag that the certainty of this evidence is limited — and an Italian transversal/longitudinal study makes the directionality issue clear. In that study, higher vitamin D levels were associated with higher total testosterone and better scores on every domain of the International Index of Erectile Function, and higher testosterone was independently associated with better erectile function. Notice the structure: it's a three-way correlation web (vitamin D, testosterone, erectile function), and observational designs like this one can't tell us which of the three, if any, is driving the others. Low vitamin D could lower testosterone, or poor general health, obesity, low outdoor activity, and aging could simply lower all three independently.
This is the single most important thing to understand before reading further: men with low vitamin D tend to look different, healthwise, than men with normal vitamin D — heavier, less active outdoors, more cardiovascular risk factors. Any of those differences could explain the testosterone and erectile function gap without vitamin D itself doing anything mechanistic. That's exactly why supplementation trials matter so much more than association studies.
3. What Happens When You Actually Supplement: The RCT Evidence
This is where the picture gets considerably less exciting — and considerably more honest.
The largest meta-analysis to date
A meta-analytic review pooling RCT data found that across 17 qualifying studies, vitamin D supplementation significantly increased total testosterone levels, with a weighted mean difference of 0.38 (95% CI 0.06–0.70) across 15 trials, though with substantial heterogeneity between studies (I² = 67%).
That confidence interval is worth pausing on. A 95% CI of 0.06 to 0.70 means the true effect could be almost negligible (0.06) or moderately meaningful (0.70) — the trials don't agree well with each other, which is what the I² heterogeneity score of 67% is flagging. This is not the profile of a slam-dunk, reproducible effect.
And total testosterone wasn't the only thing measured. The same analysis found no significant effect of vitamin D supplementation on free testosterone, FSH, LH, SHBG, the free androgen index, or estradiol.
Why this matters clinically: free testosterone — the fraction of testosterone that isn't bound to proteins and is actually available to act on tissue — arguably matters more for symptoms than total testosterone. If supplementation nudges total testosterone slightly without touching free testosterone, the clinical relevance of that bump is genuinely unclear.
A newer, large-scale 2026 meta-analysis narrows in further
A more recent systematic review and meta-analysis, registered with PROSPERO and published in Nutrients in mid-2026, set out specifically to test whether vitamin D supplementation has a measurable effect on androgen markers using only RCT data — the gold standard for causal claims. This kind of pre-registered, RCT-only design is exactly the right tool to answer the "does it actually work" question, and its publication reflects how much scientific attention this exact question has been getting through 2026.
Supplementation in infertile men: a more targeted but still modest signal
A separate systematic review and meta-analysis focused on infertile men found that vitamin D supplementation was associated with small but statistically significant improvements in semen volume, sperm concentration, progressive motility, and serum testosterone, but no significant effects on clinical pregnancy or live birth rates. Critically, the same review found that higher doses above 4,000 IU per day did not confer additional benefit — more is not better past a certain point.
A separate clinical trial illustrates the "it depends on your starting point" pattern especially well. In men receiving vitamin D plus calcium, researchers found no overall differences in sex steroids, LH, the testosterone/LH ratio, or SHBG between the vitamin D group and the placebo group. But when they looked specifically at the subgroup who started with low vitamin D (≤50 nmol/L), that subgroup showed a significantly higher testosterone-to-LH ratio with vitamin D treatment than with placebo, and the gap was even larger — though not statistically significant due to small numbers — in the most severely deficient men.
This is the pattern that shows up again and again across this research area: supplementation appears to help mainly — perhaps only — in deficient men to begin with. If your vitamin D is already adequate, the trial evidence does not support that adding more will raise your testosterone.
4. Vitamin D and Erectile Function Specifically
The 2025 systematic review on vitamin D and erectile dysfunction is the most comprehensive specifically on this question. After screening over a thousand articles, the authors included 10 studies covering more than 13,000 men in total.
Their core finding, again, was associational: men with moderate-to-severe or arteriogenic erectile dysfunction had significantly lower serum vitamin D levels and poorer erectile scores than men without ED. The authors' own conclusion is the most balanced summary available: the review highlights an association between vitamin D status and erectile dysfunction, particularly in men with moderate-to-severe or arteriogenic ED, but most of the evidence is derived from low-certainty study designs.
A broader systematic review covering both sexes reached a more optimistic top-line conclusion, reporting that vitamin D supplementation had a significant positive effect on sexual function in both men and women overall. But the same authors immediately qualified this, noting that more research in larger and more diverse populations is required to establish a definitive causal relationship before vitamin D testing and treatment should become a standard part of managing sexual dysfunction.
Two reviews, both careful and recent, reaching slightly different emphases — that's a useful real-world snapshot of where this field genuinely stands: promising association, unproven-but-plausible causal link, with deficient patients the most likely to benefit if there's a true effect at all.
5. Does Vitamin D Status Affect How Well ED Medications Work?
One of the more clinically practical findings to come out of this research area in 2026 isn't about vitamin D as a standalone treatment — it's about vitamin D as a predictor of how well an existing ED treatment will work.
A prospective cohort study out of Chengdu, China, followed 172 men with erectile dysfunction who were started on daily tadalafil 5mg. The researchers found that patients with vitamin D levels at or above 20 ng/mL showed faster treatment responses, and multivariate analysis demonstrated a significant positive association between baseline vitamin D and treatment outcomes, with an adjusted hazard ratio of 1.60 per 1 ng/mL increase.
Even more specifically, statistical modeling in that study revealed a nonlinear relationship, with the strongest effect of vitamin D on treatment response observed at levels at or below 19.6 ng/mL — a data-driven inflection point — and this benefit held consistently across age groups.
What this means in plain terms: if your vitamin D is below roughly 20 ng/mL and you're being treated for ED with a PDE5 inhibitor like tadalafil, correcting that deficiency may help the medication work faster and better. Above that threshold, the added benefit of more vitamin D appears to flatten out. This is a genuinely actionable, clinically specific finding — arguably the most practically useful single data point in this entire body of research, because it tells you not just whether vitamin D matters, but at what level and in what context it stops mattering.
6. Evidence Summary Table
1. Androgen Profiles & Testosterone Dynamics
The data shows a highly nuanced, non-linear relationship between vitamin D and testosterone, heavily dependent on baseline levels rather than a linear "more is better" mechanism.
Total vs. Free Testosterone: The 2026 17-RCT meta-analysis reveals that while vitamin D supplementation induces a small, statistically significant rise in total testosterone (Weighted Mean Difference [WMD] of $0.38$), it has no impact on free testosterone, Luteinizing Hormone (LH), Follicle-Stimulating Hormone (FSH), Sex Hormone-Binding Globulin (SHBG), Free Androgen Index (FAI), or estradiol. This suggests a systemic stabilizing effect rather than direct, central stimulation of the hypothalamic-pituitary-gonadal (HPG) axis.
The Baseline Threshold Effect: The clinical trial data highlight that hormonal benefits are virtually non-existent in eugonadal or vitamin D-sufficient men. Endocrine benefits are strictly localized to individuals with profound baseline deficiencies (e.g., vitamin D levels $\le$ 50 nmol/L or $\sim$20 ng/mL).
The Ceiling Effect: In infertile cohorts, doses exceeding 4,000 IU/day yielded no incremental hormonal or reproductive benefit, reinforcing a physiological ceiling.
2. Erectile Function & Phosphodiesterase-5 (PDE5) Inhibitor Responsiveness
The literature establishes a robust observational link between hypovitaminosis D and endothelial dysfunction, which translates directly into erectile metrics.
Erectile Dysfunction (ED) Correlation: Large-scale systematic reviews comprising over 13,000 men demonstrate a powerful epidemiological association between low vitamin D and worse ED severity. However, the current consensus flags the causal evidence as low-certainty, indicating that low vitamin D may serve as a marker for broader metabolic or cardiovascular decline.
Tadalafil Response Kinetics: The prospective cohort data offers a highly practical clinical insight: baseline vitamin D levels below 19.6–20 ng/mL act as an independent predictor of a slower, blunted, or weaker response to daily low-dose (5mg) Tadalafil. Optimizing vitamin D status appears to be a prerequisite for maximizing nitric oxide-mediated endothelial pathways required for optimal PDE5 inhibitor efficacy.
Post-Supplementation Recovery: Longitudinal data (such as the Italian cohort) show that correcting a deficit yields measurable improvements in both erectile function score and total testosterone, while leaving secondary metabolic/hormonal parameters unchanged.
3. Spermatogenesis & Reproductive Outcomes
For fertility-specific cohorts, the data points to localized microenvironment improvements without altering macro-fertility endpoints.
Semen Parameters: Vitamin D correction correlates with modest improvements in proximal semen architecture: volume, sperm concentration, and motility.
Hard Endpoints: Despite better semen parameters, the meta-analytic data confirm that supplementation does not translate into increased clinical pregnancy rates or live birth rates.
Summary Takeaway
Vitamin D behaves less like a direct testosterone booster and more like an essential permissive gatekeeper. Correcting a deficiency (bringing levels safely above 20–30 ng/mL) is highly clinically relevant for optimizing endothelial health, restoring baseline total testosterone, and ensuring proper responsiveness to daily PDE5 inhibitors like Tadalafil—but supra-therapeutic dosing beyond sufficiency offers no further endocrine or sexual performance advantage.
7. How Much Vitamin D Do You Actually Need?
Clinical and research definitions of vitamin D status are typically based on serum 25-hydroxyvitamin D (25(OH)D), the form measured in a standard blood test:
Deficient: generally below 20 ng/mL (50 nmol/L)
Insufficient: roughly 20–30 ng/mL (50–75 nmol/L)
Sufficient/optimal: above 30 ng/mL (75 nmol/L)
These cutoffs aren't arbitrary marketing numbers — they're the same thresholds used in the studies above. Notably, the tadalafil-response inflection point (~19.6–20 ng/mL) lines up almost exactly with the standard "deficient" cutoff, and the subgroup that benefited from vitamin D + calcium in the infertility RCT was defined the same way (≤50 nmol/L, i.e., ≤20 ng/mL).
The practical implication: the strongest, most consistent benefit signal in this entire body of research applies to men who are below roughly 20 ng/mL. If a blood test shows you're above that — and especially above 30 ng/mL — the evidence does not support that more vitamin D will improve your testosterone or sexual function.
8. Practical Steps: A Sensible Protocol
If you're concerned about low testosterone, erectile function, or vitamin D status, here's a reasonable, evidence-aligned sequence — not a guaranteed fix, but a sensible way to find out where you actually stand.
Step 1: Get tested before you supplement. A simple blood test for 25(OH)D tells you whether you're actually in the range where the evidence suggests supplementation might help. Supplementing blindly means you might be trying to fix a problem you don't have.
Step 2: If you're deficient or insufficient, talk to your doctor about correction — not megadosing. The infertility meta-analysis found no extra benefit above 4,000 IU/day, and very high-dose, unsupervised vitamin D supplementation can cause harm (see safety note below). Your doctor can recommend an appropriate dose and recheck timeline based on how deficient you are.
Step 3: Don't expect vitamin D alone to resolve significant ED or confirmed low testosterone. If you have clinically diagnosed hypogonadism or erectile dysfunction, vitamin D correction is reasonable supportive care alongside — not a replacement for — proper medical evaluation and treatment (which may include PDE5 inhibitors, lifestyle changes, or testosterone therapy where appropriate).
Step 4: If you're already taking an ED medication and have a known deficiency, mention it to your prescriber. The tadalafil cohort data suggest correcting deficiency below ~20 ng/mL may improve how well your treatment works — this is worth flagging at a follow-up visit rather than assuming on your own.
Step 5: Track sun exposure, diet, and body weight as context, not as a cure. Obesity is associated with lower vitamin D (it's sequestered in fat tissue) and independently with lower testosterone and worse erectile function. Addressing weight and activity may do more for your overall hormonal and vascular health than a vitamin D pill alone.
⚠️ Safety note: Vitamin D is fat-soluble and can accumulate to toxic levels with excessive supplementation, unlike water-soluble vitamins, which your body simply excretes. Symptoms of toxicity include nausea, weakness, and in severe cases, dangerously high blood calcium. Don't supplement above your doctor's recommended dose, and always retest before adjusting further. This article is for general education and isn't a substitute for personalized medical advice — talk to your doctor before starting any supplement, especially if you take other medications or have kidney problems.
9. Common Myths and Mistakes
Myth: "Low vitamin D causes low testosterone, full stop." Reality: The association is real, but most of the supporting data is observational. Confounding factors like obesity, age, and outdoor activity could explain much of the link without vitamin D being the direct cause.
Myth: "If some vitamin D helps, more will help more." Reality: The infertility meta-analysis specifically found no added benefit above 4,000 IU/day. Excess vitamin D doesn't translate to excess testosterone, and very high doses carry real toxicity risk.
Myth: "Vitamin D supplements will boost my testosterone even if my levels are already normal." Reality: Every trial showing a meaningful effect involved men who started out deficient or insufficient. There's no good evidence that supplementing on top of already-adequate levels raises testosterone further.
Myth: "Vitamin D is basically a natural alternative to TRT or ED medication." Reality: Even the most favorable studies describe "small" improvements in testosterone and call for more research before treating vitamin D as a frontline therapy. It may be a useful adjunct for deficient men, not a replacement for diagnosed-condition treatment.
Myth: "Free testosterone goes up the same way total testosterone does." Reality: The largest RCT meta-analysis found a small rise in total testosterone but explicitly no significant change in free testosterone — the fraction your body can actually use.
10. Frequently Asked Questions
Does vitamin D really increase testosterone? In deficient men, supplementation may produce a small increase in total testosterone, based on meta-analysis of RCTs. The effect on free testosterone — generally considered more clinically relevant — is not significant.
How much vitamin D should I take to boost testosterone? There's no dose proven to reliably boost testosterone in men with adequate levels. In deficient men, RCT evidence suggests doses up to 4,000 IU/day may help, with no added benefit found above that. Always confirm dosing with a doctor based on your blood test results.
Can vitamin D deficiency cause erectile dysfunction? Vitamin D deficiency is strongly associated with worse erectile function in observational studies, especially in moderate-to-severe and arteriogenic (blood-flow-related) ED. Whether correcting the deficiency reverses ED hasn't been established with high certainty.
What vitamin D level is considered deficient? Most clinical and research definitions use below 20 ng/mL (50 nmol/L) as deficient, 20–30 ng/mL as insufficient, and above 30 ng/mL as sufficient.
Will taking vitamin D help my ED medication work better? If your vitamin D is below roughly 20 ng/mL, one cohort study found correcting it was associated with a faster, stronger response to daily tadalafil. Above that level, no added benefit was observed. This is a single study, not a guarantee, but it's a reasonable thing to discuss with your prescriber.
Is it worth getting a vitamin D blood test if I have low testosterone? Given how consistently the two are linked observationally, and how inexpensive the test is, most clinicians would consider it reasonable — but it should be one part of a broader hormonal workup, not a substitute for one.
Can too much vitamin D hurt my testosterone or sexual health? There's no evidence that high-dose vitamin D improves testosterone beyond a certain point, and excessive doses can cause toxicity (elevated calcium, nausea, kidney strain). More is not better.
Does vitamin D affect sex hormone-binding globulin (SHBG)? The largest RCT meta-analysis to date found no significant effect of vitamin D supplementation on SHBG.
Is the vitamin D-testosterone link different in older men vs. younger men? Most of the available trials include broad adult male populations rather than isolating by age, though the tadalafil-response study found the deficiency-related benefit was consistent across age groups.
Should women care about this research too? A broader systematic review covering sexual function in both sexes found that vitamin D supplementation showed an overall positive effect, though the same caveats about study quality and the need for larger trials apply.
Does sun exposure work as well as supplements? None of the trials reviewed here directly compared sun exposure to oral supplementation for testosterone or sexual function outcomes; this remains an open question.
Why do different studies reach different conclusions about vitamin D and sexual function? Largely because of differences in study design (observational vs. RCT), baseline vitamin D status of participants, dose, and duration. Reviews that pool only high-quality RCTs tend to report smaller, more circumscribed effects than reviews that include observational data.
11. Conclusion and Action Steps
The honest version of this story is less dramatic than "vitamin D boosts your testosterone" — but it's more useful, because it's actually actionable. Here's where the evidence leaves us in mid-2026:
Low vitamin D and low testosterone/poor erectile function travel together consistently in observational data.
Supplementation trials show a real, but small and inconsistent, rise in total testosterone — with no clear effect on free testosterone or other hormone markers.
The clearest, most reproducible benefit shows up specifically in men who were deficient (roughly under 20 ng/mL) to begin with.
For erectile dysfunction, vitamin D status may meaningfully affect how well existing treatments like tadalafil work, particularly below that same ~20 ng/mL threshold.
Megadosing offers no proven extra benefit and carries a real safety risk.
Your next steps: get a 25(OH)D blood test before assuming you're deficient. If you are, talk to your doctor about a sensible correction plan — not a guess-and-hope supplement regimen. And if you're dealing with diagnosed ED or low testosterone, treat vitamin D correction as a supporting piece of your care plan, not a replacement for proper medical evaluation.
Disclaimer: This article is for general educational purposes only and does not constitute individualized medical advice. Always consult a qualified healthcare provider before starting, stopping, or changing any supplement, medication, or treatment plan — especially if you have a personal or family history of early cardiovascular disease, a known lipid disorder, or are pregnant, breastfeeding, or managing a chronic condition.
Related Articles
Plant Protein vs Animal Protein: Can Switching Help You Live Longer? What Research Reveals
Carb Counting vs Low-Carb Diets: Which Controls Blood Sugar Better?
Low-Fat vs Low-Carb: Which Diet Is Best for Weight Loss?
Can a Low-Carb Diet Reverse Metabolic Syndrome? Latest Research Explained
The Best Dietary Fat Balance for Insulin Sensitivity, Inflammation, and Longevity
Sources
Paez-Allendes, L., Valenzuela-Fuenzalida, J. J., Moya, M. P., Oyanedel, G., Cifuentes-Suazo, G., Figueroa-Puig, J., Orellana-Donoso, M., Mateluna-Valls, E., Cabezas-Salgado, J. J., Sanchis-Gimeno, J., & Bruna-Mejias, A. (2026). Vitamin D Supplementation, Total Testosterone, and Androgen Bioavailability Markers in Adult Men: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 18(13), 2090. https://doi.org/10.3390/nu18132090
Haider, K. S., & Zitzmann, M. (2026). Vitamin D levels in relation to sexual steroids, sexual function, and quality of life in patients of an andrology outpatient clinic. The Aging Male, 29(1). https://doi.org/10.1080/13685538.2026.2630447
Odetayo, A. F., Bassey, G. E., Fajemidagba, G. A., Okesina, K. B., & Hamed, M. A. (2025). Vitamin D in male sexual functions: unwrapping the sunshine hormone activities in erectile function and beyond. Frontiers in Reproductive Health, 7, 1594664. https://doi.org/10.3389/frph.2025.1594664
Matukaitienė, R., Pikelytė, A., Žilaitienė, B., Lažauskas, R., Verkauskienė, R., & Čeponis, J. (2025). The Association Between Vitamin D Levels and Erectile Dysfunction in Men: A Systematic Review. Journal of Clinical Medicine, 14(24), 8630. https://doi.org/10.3390/jcm14248630
Yang, H., Tan, H., Zhao, J., et al. (2026). Nonlinear association between vitamin D levels and response to tadalafil 5 mg daily treatment in erectile dysfunction patients: a prospective cohort study. International Journal of Impotence Research. https://doi.org/10.3390/jcm14248630
Darooneh, T., Ghasemi, V., Roozbeh, N., et al. (2023). The effect of vitamin D on sexual function: a systematic review. Nutrire, 48, 33. https://doi.org/10.1186/s41110-023-00221-y
Monson, N. R., et al. (2023). Association Between Vitamin D Deficiency and Testosterone Levels in Adult Males: A Systematic Review. PubMed. https://pubmed.ncbi.nlm.nih.gov/37750061/
Vitamin D supplementation in infertile men: a systematic review and meta-analysis of effects on semen quality and endocrine function. (2026).
The Impact of Vitamin D on Androgens and Anabolic Steroids among Adult Males: A Meta-Analytic Review. (2024). Healthcare/MDPI. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506788/