Could Erectile Dysfunction Be an Early Warning Sign of Heart Disease? What the Latest Research Reveals
Is erectile dysfunction a vascular disease? Learn how inflammation, cholesterol, and endothelial dysfunction influence ED risk according to recent studies.
AGINGHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/28/202620 min read
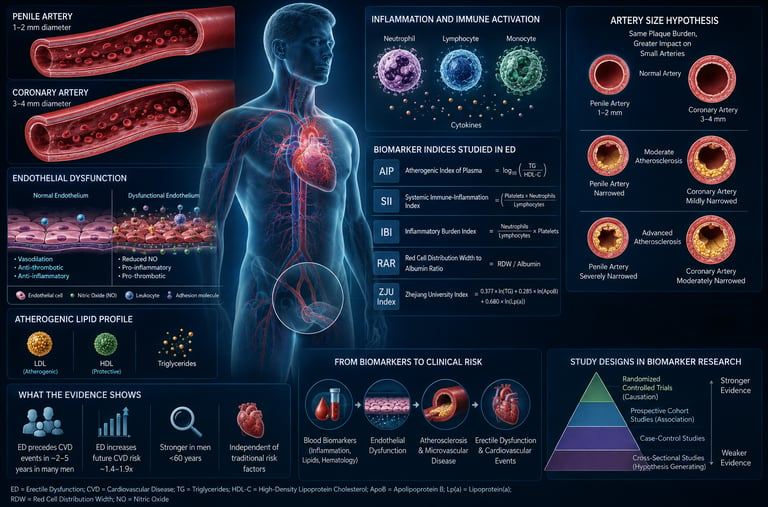
The latest medical studies show that erectile dysfunction (ED) is closely tied to your overall blood vessel and metabolic health. Because the arteries supplying the penis are very small (only 1 to 2 millimetres wide), they often show signs of plaque buildup or damage long before the larger arteries in your heart do. This makes new-onset ED an important early warning sign for cardiovascular health.
Recent research has focused on new blood-test ratios—like the Inflammatory Burden Index (IBI) and the Atherogenic Index of Plasma (AIP)—to track this underlying inflammation and cholesterol balance.
Kry Points
The Sentinel Vascular Signal: Erectile dysfunction (ED) is fundamentally a microvascular event before it is a macrovascular crisis. Because penile arteries are exceptionally small, 1–2 mm compared to the heart's 3-4mm, they act as an anatomical early-warning system—occluding from plaque buildup long before larger coronary arteries trigger chest pain
.
The NHANES Data Recycling Limitation: A critical share of recent "breakthrough" studies are not analyzing fresh patient populations. They are independently mining variations of the same legacy dataset (NHANES 2001–2004)—the only period the national survey included a validated ED questionnaire. This creates an artificial echo chamber of data replication.
The Correlation vs. Causation Trap: The overwhelming majority of modern biomarker papers utilize cross-sectional designs. These provide a static snapshot in time that cannot determine directionality: while chronic inflammation may structurally impair blood vessels, the psychological stress, poor sleep, and reduced physical activity of living with ED can just as easily drive up inflammatory markers.
Inflammatory Burden Index (IBI) Holds the Strongest Signal: Among the flurry of new immune metrics, the Inflammatory Burden Index—which blends C-Reactive Protein (CRP) with the neutrophil-to-lymphocyte ratio—demonstrates the most robust statistical association, more than doubling the odds of an ED diagnosis .
The Atherogenic Index (AIP) Contradiction: Despite heavy media coverage framing the Atherogenic Index of Plasma (triglycerides relative to HDL) as a definitive diagnostic tool, the latest 2026 data shows deeply conflicting results, including a major case-control study that found no significant difference between ED patients and healthy controls.
Non-Linear Complexity in Blood Metrics: The relationship between erectile health and biomarkers like the Red Cell Distribution Width-to-Albumin Ratio (RAR) is not a simple "higher is worse" linear progression. It follows a complex, J-shaped curve, meaning both clinical extremes (abnormally low and abnormally high ratios) carry elevated risk.
Shift from Testosterone to Endothelial Health: While popular culture reflexively treats ED as a hormonal deficit ("low T"), the modern biochemical consensus heavily favors endothelial health—the structural integrity and dilating capacity of the microscopic cell layer lining the blood vessels.
The Actionable Framework: Novel indices remain valuable academic exploratory concepts, not verified clinical screeners. The immediate, doctor-backed protocol for new-onset ED requires bypass of experimental ratios in favor of strict cardiometabolic screening (blood pressure, HbA1c, and standard lipid monitoring) combined with targeted microvascular support via aerobic exercise and sleep apnea screening
Introduction
If you've searched for "erectile dysfunction" recently, you may have come across headlines about a new blood test or "index" that claims to predict your risk — the ZJU index, the atherogenic index of plasma, the inflammatory burden index, and a half-dozen others with similar acronym-heavy names.
These studies are real. They're also frequently misreported.
Here's the short version: erectile dysfunction (ED) is, in the great majority of cases in men over 40, a vascular and metabolic condition first, not primarily a "testosterone problem" or a purely psychological one, though both can play a role. The blood vessels that supply the penis are small, and they tend to show signs of trouble before the larger arteries that feed the heart do. That's the genuinely important, clinically actionable finding underlying this whole research area.
The newer biomarker studies — measuring things like inflammation ratios and lipid indices from a standard blood panel — are an attempt to quantify that vascular risk more precisely. Some of the findings are solid. Some are weak, contradicted by other studies, or come from datasets and statistical methods that can't tell us what headline writers claim they tell us.
1. Why Erectile Function Is a Window Into Vascular Health
An erection is fundamentally a plumbing event. Nerve signals trigger the smooth muscle in the penis to relax, blood vessels widen, and blood flows in faster than it flows out, creating rigidity. Anything that damages or narrows those blood vessels — or interferes with the nerve signals controlling them — can interfere with that process.
This is where penile artery size becomes clinically important. According to a 2026 narrative review in Frontiers in Clinical Diabetes and Healthcare, the arteries supplying the penis are roughly 1–2mm in diameter, compared to 3–4mm for the coronary and carotid arteries that supply the heart and brain. Because they're smaller, the same amount of atherosclerotic plaque buildup causes proportionally more blockage in penile arteries than in larger ones — which means erectile blood flow can be compromised well before someone notices chest pain or other classic heart disease symptoms.
This "artery size hypothesis" is the mechanistic reason ED is sometimes called a sentinel symptom — an early warning sign — for cardiovascular disease, particularly in men under 60. It's not folklore; it has real anatomical and physiological logic behind it, and it's why urologists and cardiologists increasingly view a new ED diagnosis as a reason to check on someone's broader cardiovascular risk profile.
The same review describes several overlapping mechanisms that connect ED to metabolic and cardiovascular disease, particularly type 2 diabetes:
Endothelial dysfunction — damage to the thin layer of cells lining blood vessels, impairing their ability to dilate properly
Oxidative stress — a buildup of unstable molecules that damages cells and tissues over time
Chronic low-grade inflammation — sustained immune activation that contributes to vessel damage
Autonomic neuropathy — nerve damage (common in long-standing diabetes) that disrupts the signals needed to trigger an erection
Hypogonadism — lower-than-normal testosterone, which can independently affect libido and erectile function
This is the backbone of the established science. The newer biomarker studies discussed below are, for the most part, trying to find blood-test-based proxies for this same underlying vascular and inflammatory process — not discovering an entirely new cause of ED.
2. The Well-Established Risk Factors for ED
Before getting into the newer, more speculative research, it's worth being clear about what's already firmly established. These are risk factors with decades of consistent research behind them, not single cross-sectional studies:
Based on the data provided, here is the breakdown of erectile dysfunction (ED) risk factors, categorized strictly by their strength of evidence and relative clinical impact.
Very Strong Evidence (Primary Risk Drivers)
Age: The most pervasive factor; ED prevalence rises sharply and progressively after age 40 to 50.
Type 2 Diabetes: Carries a heavy 2x to 4x increased risk, with erectile difficulties frequently manifesting years before a formal diabetes diagnosis is made.
Cardiovascular Disease / Atherosclerosis: Shares an identical vascular mechanism with ED. Because penile arteries are smaller than coronary arteries, ED often serves as an early warning sign that precedes a formal cardiovascular diagnosis.
Strong Evidence (Major Modifiable & Lifestyle Factors)
Obesity: Risk scales directly with BMI, showing a particularly strong correlation with central and visceral (belly) fat accumulation.
Smoking: Directly damages the endothelial lining of blood vessels. On a positive note, this risk is often reversible after quitting.
High Blood Pressure (Hypertension): Causes progressive, long-term structural damage to arterial vessel walls, limiting necessary blood flow.
Depression and Anxiety: Operates via a powerful bidirectional relationship—psychological distress can be the root cause, a direct consequence of physical ED, or both simultaneously.
Moderate to Strong Evidence (Functional Factor)
Low Physical Activity: Sedentary lifestyles negatively impact vascular health, whereas regular exercise actively improves endothelial (blood vessel) function.
Moderate Evidence (Secondary or Inconsistent Drivers)
Low Testosterone: While relevant, it is generally more significant in older populations and is not the primary underlying driver of ED for the majority of men.
Certain Medications: Side effects from specific prescriptions—most notably certain antihypertensives (blood pressure drugs) and antidepressants—can directly impair erectile function.
Heavy Alcohol Use: Chronic, excessive alcohol consumption inflicts long-term damage on both nerve signaling and vascular pathways.
The Massachusetts Male Aging Study, one of the foundational pieces of ED epidemiology, found that mild-to-moderate ED affects roughly half of men aged 40–70, with severe ED prevalence climbing from about 5% to 15% with advancing age. The prevalence of ED in U.S. men aged 20 and older has been estimated at around 18%, based on NHANES data from the early 2000s — the same dataset, incidentally, that underlies most of the newer biomarker studies discussed below.
This is the foundation. Now let's look at what's new.
3. The New Wave of Biomarker Research: What's Actually Being Studied
Over the past three to four years, there's been a surge of studies — overwhelmingly from research groups in China and Turkey — examining whether various "composite" blood-test indices are associated with ED. These indices combine two or more values from a standard blood panel (like a complete blood count or basic lipid panel) into a single ratio or score, in an attempt to capture inflammation or metabolic dysfunction more precisely than any single marker alone.
Common ones include:
AIP (Atherogenic Index of Plasma) — triglycerides relative to HDL cholesterol
SII (Systemic Immune-Inflammation Index) — combines neutrophil, platelet, and lymphocyte counts
NLR, MLR, SIRI, AISI — other neutrophil/lymphocyte/monocyte-based inflammation ratios
RAR (Red cell distribution width-to-Albumin Ratio) — a marker combining a red blood cell measure with a nutrition/inflammation marker
IBI (Inflammatory Burden Index) — combines CRP with the neutrophil-to-lymphocyte ratio
ZJU index — combines triglycerides, fasting glucose, the ALT/AST liver enzyme ratio, and BMI; originally developed as a marker for fatty liver disease
A large share of these studies — including several referenced in this article — draw from the same source: the 2001–2002 and 2003–2004 cycles of the National Health and Nutrition Examination Survey (NHANES), often pooled together and referred to as "NHANES 2001–2004." This is the only period in NHANES history where participants were asked a validated, self-reported question about erectile function, so it's the dataset every group doing this kind of analysis has to use. That's a real methodological constraint, not a sign anything is wrong with any individual study — but it does mean dozens of papers are independently mining variations of the same roughly 2,000–4,000-person dataset, which has real implications for how much weight any single finding should carry.
4. Breaking Down Each Biomarker: What the Studies Found
The Atherogenic Index of Plasma (AIP)
AIP is calculated as the logarithm of the ratio of triglycerides to HDL cholesterol — essentially a more sensitive way of looking at the same "bad fat vs. good fat" balance your standard lipid panel already measures.
The evidence here is genuinely mixed, which is worth sitting with rather than smoothing over:
An earlier Turkish study found AIP values were meaningfully higher in men with ED than in controls (0.45 vs. 0.37, p = 0.015), with AIP rising as ED severity increased.
A 2024 NHANES-based study similarly found a significant positive association between AIP and ED risk.
But a newer 2026 cross-sectional study published in World Journal of Urology, comparing 142 men with ED to 54 without, found no significant difference in AIP or other lipid-based atherogenic indices between the two groups.
This kind of disagreement between studies happens constantly in biomarker research, especially with smaller sample sizes, different populations, and different control groups. It doesn't mean AIP is useless — but it does mean you shouldn't treat any single AIP number as a definitive verdict on your erectile health.
Systemic Immune-Inflammation Index (SII)
SII is derived from neutrophil, platelet, and lymphocyte counts — all routine parts of a complete blood count.
A NHANES 2001–2004 analysis of 3,601 men found an ED prevalence of 6.28% in that sample, with men in the highest SII category having about 45% higher odds of ED after adjusting for other factors (odds ratio 1.45, 95% confidence interval 1.01–2.17, p = 0.045).
Why the confidence interval matters here: notice that the lower bound of that interval (1.01) is barely above 1.0 — the threshold for "no effect." This is a statistically significant finding, but a modest and somewhat fragile one. It's evidence of a real association, not evidence of a strong one.
Inflammatory Burden Index (IBI)
IBI combines CRP (a well-established inflammation marker) with the neutrophil-to-lymphocyte ratio. This is one of the more robust findings in this body of research:
A NHANES-based study of 2,117 men found 30.42% had a history of ED, and after full statistical adjustment, men with higher IBI had more than double the odds of ED (odds ratio 2.26, 95% CI 1.54–3.31).
A separate, independent case-control study (published in BMC Urology) examined IBI in a retrospective ED population specifically, lending some support from a different study design — though full details from that paper weren't independently verified for this article and should be checked against the original before being cited as definitive.
An odds ratio above 2.0 with a confidence interval that doesn't come close to crossing 1.0 is a notably stronger signal than most of the other markers on this list.
Red Cell Distribution Width-to-Albumin Ratio (RAR)
RAR combines a measure of variation in red blood cell size (RDW) with serum albumin, a marker partly reflecting nutritional and inflammatory status.
A 2025 study of 3,950 NHANES participants found 1,157 reported a history of ED, and identified what researchers called a "J-shaped" relationship — meaning ED risk wasn't simply higher at higher RAR levels in a straight line, but instead dipped at moderate RAR levels and rose again at both the low and high extremes. This kind of non-linear pattern is a meaningfully different (and more complex) claim than the simple "higher is worse" associations reported for most other markers, and it's a good example of why headlines that flatten "RAR linked to ED risk" into a simple takeaway can be misleading.
A related but distinct paper from the same general research community examined RAR's mirror-image cousin, the haemoglobin-to-RDW ratio, and found a 69% reduction in ED odds per unit increase in that ratio (odds ratio 0.31) — consistent directionally with the RAR findings, but again, a different specific marker.
The ZJU Index
Originally developed to flag risk of metabolic-associated fatty liver disease, the ZJU index combines triglycerides, fasting glucose, the ALT-to-AST liver enzyme ratio, and BMI.
A 2026 study in The Aging Male, using 1,906 NHANES participants, examined this index against ED risk using logistic regression and smooth curve fitting. Because this paper sits squarely in the same genre as the others — a single cross-sectional analysis of the same dataset — it should be read with the same caveats: an association finding, not a causal one, and one that would benefit from independent replication in a different population before being treated as established.
Multi-Marker Panels (MLR, NLR, SII, SIRI, AISI Combined)
One 2024 study took a broader approach, jointly analyzing five different inflammation ratios derived from blood cell counts in the same NHANES population, then comparing how well each one predicted ED using ROC curve analysis (a statistical method for comparing how good different tests are at distinguishing between groups). This kind of head-to-head comparison is genuinely useful, since it tells us something about which markers carry more signal relative to each other, rather than just confirming each one individually shows some association.
5. Evidence Summary Table
Moderate-to-Strong Associations
Inflammation-Bleeding Index (IBI):
Data: Studied in 2,117 men.
Impact: Shows a moderate-to-strong association, carrying an Odds Ratio (OR) of 2.26 (95% CI: 1.54–3.31). This makes it one of the more robust single-index hematological predictors in recent cross-sectional data.
Systemic Immune-Inflammation Index (SII):
Data: Studied in a larger cohort of 3,601 men.
Impact: Demonstrates a modest but statistically significant association with an OR of 1.45 (95% CI: 1.01–2.17), linking systemic, low-grade immune activation to endothelial dysfunction.
Non-Linear & Inconsistent Associations
Red Blood Cell Distribution Width-to-Albumin Ratio (RAR):
Data: Studied in 3,950 participants.
Impact: Exhibits a distinct J-shaped, non-linear relationship. This implies that risk does not scale linearly; instead, both very low and progressively higher ratios carry different risk profiles, making interpretation more nuanced.
Atherogenic Index of Plasma (AIP):
Data: Sample sizes vary across cross-sectional data.
Impact: Weak and inconsistent. While older data suggested a link, a definitive 2026 case-control study returned entirely null findings, indicating it is a less reliable standalone marker for ED risk than hematological inflammation scores.
Preliminary & Emerging Indicators
ZJU Index:
Data: Studied in 1,906 participants.
Impact: Preliminary. While a significant association has been reported, further validation is required to establish its precise predictive weight in broader clinical settings.
Multi-Marker Panels (MLR / NLR / SII / SIRI / AISI):
Data: Sample sizes vary across comparative datasets.
Impact: Preliminary/Comparative. Rather than relying on a single marker, evaluating these immune-inflammatory ratios simultaneously using ROC (Receiver Operating Characteristic) curves is being used to determine if a combined panel yields superior predictive accuracy over individual markers.
Limitations that apply to every row in this table: all of these are cross-sectional studies (a single snapshot in time, not tracking people over years), most draw on the same NHANES 2001–2004 dataset, none can establish causation, and self-reported ED questionnaires — while validated — are still subject to recall and reporting bias.
6. Why Cross-Sectional Studies Can't Prove Cause and Effect
This is the single most important concept for interpreting this entire body of research, so it's worth slowing down on.
A cross-sectional study measures everything — your blood markers and your ED status — at the same single point in time. It can tell you that two things tend to occur together more often than chance would predict. It cannot tell you which one came first, or whether either one caused the other.
Here's a concrete way to see why that matters: it's entirely plausible that chronic inflammation contributes to vascular damage that causes ED. But it's equally plausible that the chronic stress, reduced physical activity, and disrupted sleep that often accompany living with ED themselves drive up inflammatory markers. A cross-sectional snapshot literally cannot distinguish between these two stories — both would produce the exact same statistical association.
This is exactly why most of the papers covered above include their own version of a sentence like "further prospective studies are needed to establish causality" — that's not boilerplate modesty, it's an accurate description of what cross-sectional data can and can't support.
What would be stronger evidence?
Prospective cohort studies that measure biomarkers in healthy men, then track who develops ED over subsequent years
Randomized controlled trials testing whether lowering a specific biomarker (through medication or lifestyle change) actually reduces ED rates
Mendelian randomization studies, which use genetic variants as a kind of natural experiment to get closer to causal inference without a traditional trial
A few studies in this space have started using Mendelian randomization for related questions (such as inflammatory cytokines and ED), and that's a meaningfully stronger form of evidence than a standard cross-sectional analysis — worth specifically looking for if you want to dig deeper into any one biomarker.
7. What This Means for You: A Practical Framework
Given everything above, here's a grounded way to think about your own situation — focused on what's actually actionable, rather than chasing any single index.
Step 1: Don't fixate on any single biomarker
No study here has validated AIP, SII, RAR, or any of these indices as a clinical diagnostic tool you should ask your doctor to calculate and act on in isolation. They're research findings, not approved screening tests.
Step 2: Focus on the established, modifiable risk factors
These overlap heavily with the mechanisms the biomarker studies are indirectly trying to capture anyway:
Cardiovascular risk reduction: blood pressure control, LDL cholesterol management, not smoking
Metabolic health: maintaining a healthy weight, particularly reducing visceral fat; managing blood sugar if you have prediabetes or diabetes
Physical activity: regular aerobic exercise improves endothelial function — the same vessel-lining health implicated in nearly every mechanism described above
Sleep: poor sleep, particularly undiagnosed sleep apnea, is an underappreciated contributor to both ED and the inflammatory markers discussed in this article
Alcohol moderation: heavy chronic use impairs both vascular and nerve function
Mental health: depression and anxiety have a well-documented bidirectional relationship with ED
Step 3: Treat new or worsening ED as a reason to get a cardiovascular check-up, not just an ED prescription
Given the artery-size mechanism discussed earlier, a doctor evaluating new ED — especially in a man under 60 without an obvious cause like a recent injury or new medication — has good reason to also check blood pressure, lipid panel, fasting glucose or HbA1c, and discuss family cardiovascular history.
Step 4: If you want your blood panel evaluated thoroughly, ask your doctor to interpret it in context
If you're curious about your triglyceride-to-HDL ratio or inflammatory markers from a standard panel, a clinician can absolutely discuss them with you. But the right context is your overall cardiometabolic risk picture — not as a stand-alone ED predictor.
A simple self-check before your appointment
It can help to jot down, before you see a doctor:
When the ED started and whether it's constant or situational
Any new medications, including over-the-counter ones
Recent changes in mood, sleep, stress, or relationship circumstances
Family history of heart disease or diabetes
Current smoking, alcohol, and exercise habits
This kind of information is far more useful to a clinician in the room than any biomarker calculation you could do yourself beforehand.
8. Common Myths and Mistakes
Myth: "My biomarker score is high, so I have heart disease." These indices show statistical associations across populations. An individual elevated value doesn't mean you personally have a cardiovascular condition — it's one data point a doctor would weigh alongside many others.
Myth: "These studies prove inflammation causes ED." Cross-sectional studies show association, not causation, for the reasons covered in Section 6. Some studies in this space explicitly say so in their own conclusions.
Myth: "ED biomarker research is all junk science / fabricated." Not the case. These are generally real, published, peer-reviewed studies analyzing real datasets, even when individual findings are preliminary, sometimes contradictory between studies, or limited by their cross-sectional design. Healthy skepticism about strength of evidence is different from dismissing the research outright.
Myth: "If my numbers look fine on these new indices, my erectile health is fine." These indices were studied as additional possible markers, not as having superseded or replaced the well-established risk factors (diabetes, blood pressure, smoking, weight, mental health) discussed in Section 2.
Myth: "Lowering one biomarker (like AIP) will fix ED." No randomized controlled trial in this body of research has tested whether deliberately lowering any of these specific indices improves erectile function. The honest, current answer is: we don't know yet.
Mistake: Treating ED purely as a "bedroom problem" rather than a potential health signal. Given the vascular mechanisms involved, particularly in men over 40, new ED is frequently worth a broader medical conversation — not just a prescription.
9. Frequently Asked Questions
Is erectile dysfunction a sign of heart disease? It can be an early warning sign, particularly in men under 60 with no other obvious cause. The penile arteries are smaller than the coronary arteries, so vascular narrowing tends to show up there first. New ED is a reasonable trigger for a cardiovascular risk check-up.
What is the atherogenic index of plasma (AIP) and is it linked to ED? AIP is a ratio of triglycerides to HDL cholesterol used as a marker of cardiovascular risk. Evidence linking it specifically to ED is mixed — some studies find a significant association, while a 2026 case-control study found none. It shouldn't be treated as a settled finding.
What is the systemic immune-inflammation index (SII)? SII is calculated from neutrophil, platelet, and lymphocyte counts on a standard blood test, used as a marker of systemic inflammation. One large NHANES-based study found a modest but statistically significant association between higher SII and ED risk.
Can blood tests diagnose erectile dysfunction? No single blood test diagnoses ED — diagnosis is clinical, generally based on symptoms and validated questionnaires like the IIEF-5. Blood tests (testosterone, blood sugar, lipids, and sometimes the inflammation markers discussed here) can help identify underlying contributing causes once ED is already suspected or diagnosed.
Does inflammation cause erectile dysfunction? Chronic low-grade inflammation is one of several plausible contributing mechanisms, alongside endothelial dysfunction, oxidative stress, and others. Current evidence shows inflammation markers are associated with ED; it hasn't been proven that inflammation itself is a primary cause in a way that's been demonstrated through controlled trials.
Are these new biomarkers (ZJU index, RAR, IBI) better than checking cholesterol and blood sugar? There's no evidence yet that they outperform established risk factors for clinical decision-making. They're being studied as potentially more sensitive composite measures, but haven't been validated as replacements for standard cardiometabolic screening.
Why do so many ED studies use NHANES data from 2001–2004? Because that's the only period in NHANES history that included a validated self-reported erectile function questionnaire. Many independent research groups analyze this same dataset looking at different biomarkers, which is why you'll see "NHANES 2001–2004" repeated across many otherwise-unrelated papers.
Can lifestyle changes reverse erectile dysfunction caused by vascular issues? For many men, especially when ED is linked to obesity, smoking, or sedentary behavior, meaningful improvements in cardiovascular risk factors (weight loss, exercise, smoking cessation) have been associated with improved erectile function in various studies — though individual results vary, and severe or longstanding vascular damage may not fully reverse.
Is erectile dysfunction primarily a testosterone problem? For most men, no — vascular and metabolic factors are typically more significant contributors, especially after age 40. Low testosterone can contribute, particularly to reduced libido, but a full hormonal work-up is something a doctor would order based on your specific symptoms, not something to assume by default.
What's the difference between a cross-sectional study and a study that proves cause and effect? A cross-sectional study measures everything at one point in time and can only show that two things are statistically associated. Proving causation generally requires either a randomized controlled trial or a long-term study that tracks people over time to see what develops first.
Should I ask my doctor to test my AIP, SII, or IBI? You can ask, and a doctor may already have the underlying values (triglycerides, HDL, CRP, complete blood count) from routine bloodwork — calculating these specific ratios is simple arithmetic from numbers you may already have. But treat any single result as a data point for discussion, not a diagnosis.
10. Conclusion and Action Steps
The honest summary of this research area is this: erectile dysfunction is, for most men, tightly connected to cardiovascular and metabolic health — a connection backed by decades of solid evidence and a clear anatomical explanation (the artery-size mechanism). The newer wave of biomarker studies — AIP, SII, IBI, RAR, the ZJU index, and others — are a real but early-stage attempt to refine that picture using routine blood test values, with findings ranging from reasonably consistent (IBI) to genuinely mixed (AIP) to still preliminary (ZJU index, multi-marker panels).
None of them are ready to be treated as a diagnostic tools, and none has been shown — through the kind of trial that would actually prove it — to be something you can act on directly by "lowering your number."
What's worth doing instead:
If you're experiencing new or worsening ED, see a doctor rather than self-diagnosing from a blood panel
Ask specifically about a cardiovascular and metabolic risk check-up, given how often ED and heart disease share root causes
Focus on the well-established levers: blood pressure, blood sugar, weight, physical activity, sleep, smoking, and mental health
Stay appropriately skeptical of any single study or headline claiming a new biomarker "predicts" or "causes" ED — read for the actual odds ratios and confidence intervals, and notice when studies disagree with each other
If you want to track or discuss any of these specific indices, bring the conversation to your doctor rather than interpreting the numbers alone
This is a genuinely evolving area of research, and we'll likely have better-designed, longer-term studies in the next few years that can finally start to answer the causation question this current generation of cross-sectional studies can't.
Related Articles
Beyond Fat Cells: The Hidden Lymphatic Link to Obesity, Insulin Resistance, and Inflammation
How Excess Weight May Be Aging Your Brain Faster Than You Think
The mTOR Switch: Why Your Cells Stopped Listening to Insulin | DR T S DIDWAL
Why Protein After 55 Isn’t Optional — The Science Behind Why the RDA Is Too Low | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
Sources and References
Arslan, A., Benli, E., Yüce, A., et al. (2026). Association between inflammatory burden index and erectile dysfunction: A retrospective case–control study. BMC Urology. https://doi.org/10.1186/s12894-026-02215-0
Association of erectile dysfunction and peripheral arterial disease in NHANES 2001–2004: A cross-sectional study. (2024). Frontiers in Endocrinology.
Association between the inflammatory burden index and erectile dysfunction: A cross-sectional study based on NHANES 2001–2004 (2,117 male participants). (2025). Journal of Health, Population and Nutrition. https://doi.org/10.1186/s41043-025-01093-w
Ermis, E., Ozbay Ozyilmaz, S., Salabas, E., et al. (2020). The relationship between erectile dysfunction and the Atherogenic Index of Plasma. International Journal of Impotence Research, 32(4), 462–468. https://doi.org/10.1038/s41443-019-0167-2
Feldman, H. A., Goldstein, I., Hatzichristou, D. G., Krane, R. J., & McKinlay, J. B. (1994). Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. The Journal of Urology.
Guo, L., Nan, Y., & Yao, L. (2024). Association between atherogenic indexes and erectile dysfunction: A cross-sectional analysis of the National Health and Nutrition Examination Survey 2001–2004. International Urology and Nephrology, 56, 2877–2885. https://doi.org/10.1007/s11255-024-04050-4
Hemoglobin-to-Red Blood Cell Distribution Width Ratio and Erectile Dysfunction Among U.S. Adults: A Moderated Mediation Analysis of Body Roundness Index. (2026). American Journal of Men's Health. https://doi.org/10.1177/15579883251414645
Liu, D., et al. (2024). Inflammatory cytokine profiles in erectile dysfunction: A bidirectional Mendelian randomization. Frontiers in Immunology, 15, Article 1342658. https://doi.org/10.3389/fimmu.2024.1342658
Liu, H., Dong, H., Guo, M., & Cheng, H. (2024). Association between inflammation indicators (MLR, NLR, SII, SIRI, and AISI) and erectile dysfunction in US adults: NHANES 2001–2004. Journal of Health, Population and Nutrition, 43(1), Article 169. https://doi.org/10.1186/s41043-024-00667-4
Martínez Mores, S., Franch-Nadal, J., Mauricio, D., & Vlacho, B. (2026). Erectile dysfunction, type 2 diabetes, and cardiovascular disease: A narrative review and insights from a global real-world cohort analysis. Frontiers in Clinical Diabetes and Healthcare, 7, Article 1781581. https://doi.org/10.3389/fcdhc.2026.1781581
Ning, W., Jia, S., Li, L., Chen, D., & Wu, B. (2026). Examining the relationship between erectile dysfunction and the ZJU index in US adults: Results from NHANES 2001–2004. The Aging Male, 29(1), Article 2627017. https://doi.org/10.1080/13685538.2026.2627017
Selvin, E., Burnett, L. A., & Platz, E. A. (2007). Prevalence and risk factors for erectile dysfunction in the US. The American Journal of Medicine, 120(2), 151–157.
Shao, Y., Zhang, G., Liu, Y., et al. (2026). Association between red blood cell distribution width-to-albumin ratio with erectile dysfunction in US men: Insights from national cross-sectional study in NHANES 2001 to 2004. Medicine, 105(26), Article e49411. https://doi.org/10.1097/MD.0000000000049411
Turkoglu, A. R., Ustundag, Y., Koç, A., et al. (2026). The relationship between atherogenic index of plasma and erectile dysfunction: A cross-sectional observational study. World Journal of Urology, 44, Article 272. https://doi.org/10.1007/s00345-026-06308-1
Xu, M., Zhou, H., Zhang, R., Pan, Y., & Liu, X. (2023). Correlation between visceral adiposity index and erectile dysfunction in American adult males: A cross-sectional study based on NHANES. Frontiers in Endocrinology. https://doi.org/10.3389/fendo.2023.1301284
Xu, Y., & Li, S. (2025). J-Shaped relationship between the red cell distribution width to albumin ratio and erectile dysfunction: A cross-sectional study from NHANES 2001–2004. Frontiers in Endocrinology. https://doi.org/10.3389/fendo.2025.1545272
Zhang, Y., Li, T., Chen, Q., Shen, M., Fu, X., & Liu, C. (2024). The relationship between complete blood cell count-derived inflammatory biomarkers and erectile dysfunction in the United States. Scientific Reports, 14, Article 32014. https://doi.org/10.1038/s41598-024-83733-5
Zhong, L., Zhan, X., & Luo, X. (2023). Higher systemic immune-inflammation index is associated with increased risk of erectile dysfunction: Result from NHANES 2001–2004. Medicine. https://doi.org/10.1097/MD.0000000000035724
This article is for informational purposes only and does not constitute medical advice. If you are experiencing erectile dysfunction, particularly if it is new, sudden, or accompanied by chest pain, shortness of breath, or other symptoms of concern, please consult a licensed healthcare provider.