How Excess Weight May Be Aging Your Brain Faster Than You Think
Discover how obesity reshapes the brain through neuroinflammation, insulin resistance, and reward-system dysfunction. Learn why excess weight increases the risk of cognitive decline and dementia.
OBESITY
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/17/202617 min read
Obesity changes brain structure and function by shrinking gray matter in the prefrontal cortex and hippocampus, disrupting dopamine reward pathways, and triggering neuroinflammation. Chronically high leptin and insulin levels cause central resistance, impairing satiety signals. These changes reduce impulse control, increase food cravings, and raise long-term risk of cognitive decline and Alzheimer’s disease, especially with midlife obesity.
Key Points:
1. Obesity rewires brain structure
2024-2026 MRI studies show consistent gray matter loss in prefrontal cortex and hippocampus — areas controlling impulse control, decision-making, and memory. White matter connectivity also degrades, slowing information processing.
2. Your reward system gets hijacked
Chronic overeating downregulates dopamine D2 receptors, like in addiction. The brain then needs more food for the same pleasure. Leptin + insulin resistance in the hypothalamus further kills satiety signals.
3. Neuroinflammation is the core mechanism
Fat tissue releases TNF-α, IL-6, and IL-1β that cross the blood-brain barrier, activating microglia. This drives synaptic pruning, impaired neurogenesis, and oxidative stress — the main pathway linking obesity to cognitive decline.
4. Midlife is the danger zone for dementia risk
Obesity ages 40-60 shows the strongest link to later Alzheimer’s. It accelerates amyloid-β buildup, tau pathology, and vascular damage. The “obesity paradox” in late-life is likely reverse causality from pre-dementia weight loss.
5. Genetics prove it’s not just willpower
GWAS data show obesity-risk genes like FTO and MC4R are expressed in the brain, not just fat tissue. Monogenic obesity cases confirm appetite circuits in the CNS are master regulators of weight.
6. Damage may be partly reversible
Bariatric surgery and major weight loss show improvements in cognition, white matter integrity, and inflammatory markers. But full recovery is uncertain — duration and severity matter. Prevention in midlife is key.
7. GLP-1 drugs may protect the brain directly
Semaglutide/liraglutide show early evidence of reducing neuroinflammation and improving brain energy metabolism, beyond just weight loss. Human cognitive outcome trials are still ongoing.
8. Exercise + MIND diet = best brain defense
Aerobic exercise boosts BDNF and hippocampal neurogenesis even before weight loss. Mediterranean/MIND dietary patterns reduce neuroinflammation and are linked to lower dementia incidence.
Introduction
You may have heard that obesity affects your heart, joints, and metabolism. But what if the most significant damage is happening somewhere far less visible — inside your brain?
Over the past decade, neuroscientists have uncovered something both alarming and actionable: obesity doesn't just sit passively in your fat cells. It actively alters the architecture, chemistry, and function of the brain in ways that make weight loss harder, accelerate cognitive decline, and increase the risk of neurological disease.
A wave of high-quality studies published between 2024 and 2026 has sharpened this picture considerably. And crucially, understanding the mechanisms — not just the associations — changes how we think about treating obesity altogether.
In this article, you'll learn:
Exactly how obesity restructures the brain at the cellular and systems level
What the newest neuroimaging and genetic studies reveal (and where the evidence is strong vs. preliminary)
Which neurological conditions is obesity most convincingly linked to — and why
What does this mean clinically for you or your patients
Practical, evidence-informed steps to protect brain health
1. The Obesity–Brain Connection: Why It Matters
Obesity — defined as a body mass index (BMI) ≥ 30 kg/m² — affects over 650 million adults worldwide. It is conventionally framed as a metabolic disorder, a condition of excess energy storage. But this framing is increasingly incomplete.
The brain is both a victim and a perpetuator of obesity.
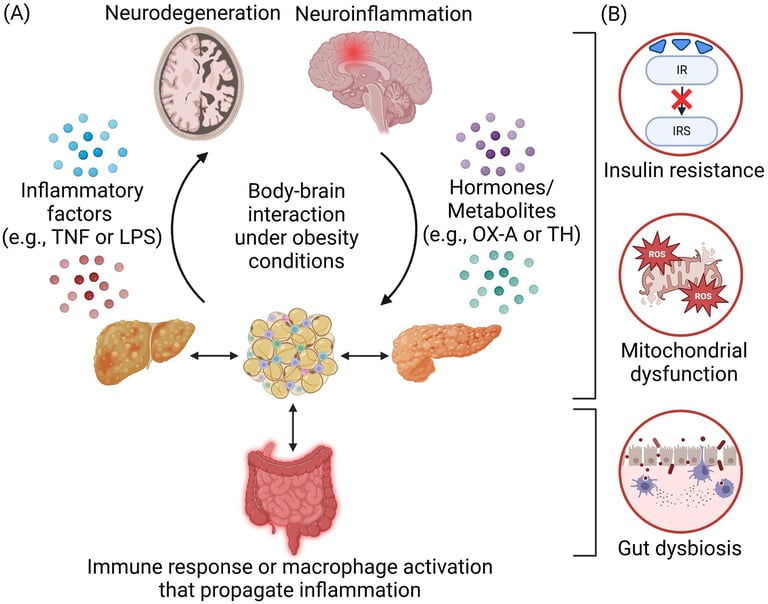
On one hand, brain changes caused by excess adiposity — including neuroinflammation, altered hormone signaling, and structural volume loss — make it biologically harder to lose weight. On the other hand, the brain's reward and homeostatic circuits are among the first systems that obesity begins to dysregulate, creating a self-reinforcing cycle.
A 2026 study published in Molecular Neurobiology by Zand et al. frames this clearly: obesity "hacks" the brain's regulatory systems, creating neurobiological resistance to weight loss that goes well beyond willpower or motivation. This is not a metaphor. It reflects measurable changes in dopamine receptor density, hypothalamic inflammation, and leptin signaling pathways.
Why does this matter clinically?
Because if we treat obesity purely as a behavioral problem — eat less, move more — we ignore the neurobiological substrate that makes those behaviors so difficult to change. Understanding the brain's role offers both explanatory power and therapeutic targets.
2. How Obesity Changes Brain Structure
Gray Matter Atrophy: The Shrinking Brain
One of the most replicated findings in obesity neuroscience is structural gray matter reduction. A 2025 critical review in Brain Research by Majumder, Menon, and Borotikar synthesized evidence from MRI studies and found consistent associations between elevated BMI and gray matter volume loss — particularly in regions governing cognition, appetite, and emotional regulation.
The most commonly affected areas include:
Prefrontal cortex — involved in executive function, impulse control, and decision-making
Hippocampus — critical for memory consolidation and spatial navigation
Orbitofrontal cortex — central to reward valuation and behavioral flexibility
Insula — involved in interoception (body awareness) and taste processing
How strong is this evidence?
The MRI literature is large and reasonably consistent. However, most studies are cross-sectional — they compare obese and non-obese individuals at one time point. This means we cannot definitively say obesity caused the gray matter loss; it's possible that structural differences precede or predispose to obesity. Longitudinal studies are fewer and their findings more mixed.
Clinical takeaway: Gray matter differences are real and measurable. Whether they are fully reversible with weight loss remains an open and important question. Early intervention likely matters.
White Matter and Connectivity
Beyond gray matter, obesity is associated with alterations in white matter integrity — the "wiring" of the brain that allows different regions to communicate. Disruptions in white matter tracts have been linked to slower information processing and reduced cognitive flexibility.
A 2024 study in Communications Biology by Morys et al. examined neural correlates of obesity across the lifespan, finding that white matter changes accumulate progressively and are especially pronounced in middle-aged adults with long-duration obesity.
3. Neurochemical Disruption: The Reward System Takeover
Dopamine Dysregulation
Highly palatable foods — high in fat, sugar, and salt — activate the brain's mesolimbic dopamine system in ways that parallel the effects of addictive substances. Over time, chronic activation leads to downregulation of dopamine D2 receptors, a phenomenon also seen in drug addiction.
The result: the brain requires more food (or more rewarding food) to produce the same sense of pleasure and satisfaction. This is not a character flaw. It is a neuroadaptation.
The 2026 article by Zand et al. in Molecular Neurobiology describes this as a form of "reward hijacking" — the brain's incentive salience system becomes disproportionately weighted toward food cues, making it genuinely harder to resist overeating even when the individual is cognitively motivated to do so.
Leptin and Insulin Resistance in the Brain
Leptin, a hormone secreted by fat cells, signals satiety to the hypothalamus. In obesity, chronically elevated leptin levels lead to central leptin resistance — the hypothalamus stops responding appropriately.
Similarly, insulin resistance, typically considered a metabolic phenomenon, extends to the brain. Insulin signaling in the hippocampus and prefrontal cortex plays a role in learning, memory, and mood. Disruption of this signaling contributes to both cognitive impairment and increased hunger.
Neuroinflammation: The Hidden Mechanism
Perhaps the most important mechanistic link between obesity and brain dysfunction is neuroinflammation. Adipose tissue in obesity is metabolically active, releasing pro-inflammatory cytokines — including TNF-α, IL-6, and IL-1β — into systemic circulation.
These cytokines cross the blood-brain barrier (particularly in states of increased permeability, which obesity also promotes) and activate microglia — the brain's resident immune cells. Chronic microglial activation leads to:
Synaptic pruning (loss of neuronal connections)
Impaired neurogenesis (reduced new neuron formation)
Accelerated oxidative stress
Progressive neurodegeneration
A comprehensive 2026 review by Soliman, Fahmy, and Mahmoud Ahmed in Diabetology & Metabolic Syndrome positions neuroinflammation as the central mechanistic driver of the obesity-brain axis, linking it to conditions ranging from cognitive decline to depression and Alzheimer's disease.
Clinical validity note: Neuroinflammation is difficult to measure directly in living humans. Much of the mechanistic evidence comes from animal models or post-mortem tissue studies. However, the convergence of indirect evidence — elevated CSF inflammatory markers, neuroimaging changes, and epidemiological associations — is compelling.
4. Obesity as a Catalyst for Neurodegeneration
Alzheimer's Disease and Dementia Risk
The relationship between obesity and Alzheimer's disease (AD) has been debated for years, partly because some studies show an "obesity paradox" in older adults where higher BMI appears protective. However, newer research is clarifying this picture.
A landmark 2026 paper in Nature Metabolism by Chen, Rodríguez-Díaz, Schneeberger et al. positions obesity as a genuine "catalyst for neurodegeneration," acting through multiple converging pathways:
Amyloid-β accumulation: Obesity-associated insulin resistance impairs amyloid clearance mechanisms
Tau pathology: Neuroinflammation accelerates tau hyperphosphorylation
Vascular damage: Obesity-related hypertension and dyslipidemia damage cerebral microvasculature
Mitochondrial dysfunction: Lipotoxicity in neurons impairs energy metabolism
Critically, the authors argue that the obesity paradox in late-life largely reflects reverse causality — people who develop dementia often lose weight in the years before diagnosis, making low BMI appear "protective" in cross-sectional snapshots.
What this means clinically: Midlife obesity (ages 40–60) carries the strongest evidence for increased dementia risk. Early intervention during this window may be the most impactful.
Parkinson's Disease
Emerging evidence suggests links between obesity and Parkinson's disease risk, potentially through shared mechanisms of mitochondrial dysfunction and alpha-synuclein aggregation. However, this association is less well-established than the AD link and requires further longitudinal research.
Cerebrovascular Disease and Stroke
The evidence here is among the most robust in the field. Obesity elevates risk for hypertension, atrial fibrillation, atherosclerosis, and dyslipidemia — all major stroke risk factors. The brain damage from stroke compounds any primary obesity-related neurological changes.
5. The Genetics of Obesity and Brain Function
Shared Genetic Architecture
A 2025 study in Molecular Psychiatry by Saeed, Bonnefond, and Froguel examined genome-wide association studies (GWAS) to explore the genetic overlap between obesity and brain function. Their findings are illuminating:
Many genetic variants associated with obesity risk are expressed in the brain, not just in peripheral metabolic tissues
Variants in genes like FTO, MC4R, and BDNF influence both body weight regulation and cognitive function
This shared genetic architecture suggests that the obesity–brain relationship is not purely one-directional — brain biology shapes obesity risk from the outset
Monogenic Obesity: What Extreme Cases Reveal
Rare forms of severe early-onset obesity caused by single gene mutations (e.g., leptin deficiency, MC4R mutations) have proven invaluable for understanding the central nervous system's role in weight regulation. These cases demonstrate that the brain's appetite circuits — not peripheral tissues — are the master regulators of energy balance.
Clinical relevance: Genetic findings underscore that obesity is not simply a lifestyle choice. For many individuals, the neurobiological deck is stacked against them from the start. This has profound implications for how we communicate about obesity in clinical practice and public health.
6. Obesity Across the Lifespan: When Does It Do the Most Damage?
The 2024 Communications Biology paper by Morys, Tremblay, Rahayel et al. takes a particularly valuable developmental perspective. Their analysis of neural correlates across the lifespan reveals that the timing of obesity matters enormously.
Childhood and Adolescence
The developing brain is especially vulnerable. Obesity in childhood is associated with:
Reduced hippocampal volume (affecting memory and learning)
Altered prefrontal development (affecting impulse control)
Earlier onset of neuroinflammation
However, the brain's plasticity during development also means intervention at this stage may yield the greatest neurological benefit.
Midlife (Ages 40–60)
This appears to be the highest-risk window for long-term neurological consequences. Obesity during midlife shows the strongest associations with later dementia risk, possibly because:
Cumulative inflammatory exposure is significant by this point
Vascular risk factors (hypertension, diabetes) compound neurological damage
Neuroplasticity is reduced compared to earlier decades
Older Adults
As noted earlier, the picture becomes more complex in older age due to reverse causality concerns. Some degree of weight loss with aging is common and may independently signal neurodegeneration.
Key clinical takeaway: The neurological impact of obesity is not uniform across age. Risk stratification should account for age of onset, duration of obesity, and comorbid metabolic conditions.
7. Clinical Relevance: What Do These Findings Actually Mean?
This is the question that matters most. Much of the obesity-brain literature is compelling in terms of associations, but clinical application requires careful interpretation.
Strength of Evidence: A Realistic Appraisal
Here are the key points summarizing the evidence quality and structural limitations across different areas of brain research, organized from the strongest evidence bases to the emerging ones:
Genetic Links (Strongest Evidence)
Status: Backed by highly robust data.
Limitation: Researchers are still working to definitively separate true causality from mere correlation.
Structural Brain Changes & Midlife Obesity Dementia Risk (Moderate to Strong Evidence)
Status: Strong indicators connect structural brain changes (via MRI) and midlife obesity to cognitive decline and dementia.
Limitations: MRI data is mostly cross-sectional, making actual causality uncertain. Additionally, the dementia risk linked to midlife obesity is frequently clouded by overlapping vascular risk factors.
Neuroinflammation & Reward System Disruption (Moderate Evidence)
Status: Clear associations found through a mix of human neuroimaging and animal studies.
Limitations: Evidence for neuroinflammation relies heavily on animal models or post-mortem data, while reward system disruptions depend heavily on combining animal behaviors with human brain scans.
Childhood Brain Effects (Moderate Evidence)
Status: Early-life impacts on the brain show consistent trends.
Limitations: Findings are restricted by smaller study sample sizes and a critical need for longer-term follow-up data.
Does Weight Loss Reverse Brain Changes?
This is perhaps the most clinically urgent question — and the most underresearched. Available evidence suggests:
Structural changes may partially reverse with significant weight loss, particularly after bariatric surgery
Cognitive function shows improvement in several (though not all) post-weight-loss studies
Neuroinflammatory markers tend to decrease with adiposity reduction
Dopaminergic function may partially recover, though this is less well-studied
The honest answer is: we don't yet know the full extent of reversibility, particularly for long-duration obesity. This makes prevention — especially in childhood and midlife — the most evidence-backed strategy.
Therapeutic Interventions: What the Neuroscience Suggests
The 2026 review by Soliman et al. provides a comprehensive overview of neurologically relevant interventions:
Pharmacological approaches:
GLP-1 receptor agonists (e.g., semaglutide, liraglutide) — showing promise not just for weight loss but for direct neuroprotective effects; preliminary evidence suggests reduced neuroinflammation
Insulin sensitizers — may address central insulin resistance
Emerging anti-inflammatory targets — still experimental
Bariatric surgery:
Associated with improvements in cognitive function, white matter integrity, and reduced dementia incidence in some studies
Effect size and durability vary; mechanisms not fully elucidated
Lifestyle interventions:
Caloric restriction with adequate nutrition reduces inflammatory cytokines
Aerobic exercise has robust independent effects on hippocampal neurogenesis and BDNF levels
Mediterranean and MIND dietary patterns are associated with reduced cognitive decline
⚠️ Safety note: No weight loss intervention should be undertaken without medical supervision, particularly in individuals with existing neurological or cardiovascular conditions.
8. Evidence Summary Table
Here is the summary of the 6 studies rewritten as clear, actionable points, structured by their specific brain and metabolic insights:
Brain Defense Mechanisms & Weight-Loss Resistance
Study: Zand et al. 2026 (Molecular Neurobiology)
Key Finding: Obesity actively overrides and compromises the brain’s built-in weight-regulation and weight-loss systems.
Clinical Value: Provides a clear biological explanation for why keeping weight off is so difficult.
Limitation: It is a literature review and does not present new primary data.
Age-Specific Brain Risks & Lifespan Variation
Study: Morys et al. 2024 (Communications Biology)
Key Finding: The way obesity maps onto brain structures shifts as we age, identifying midlife as the highest-risk period for brain health.
Clinical Value: Pinpoints exactly when clinical weight interventions can protect long-term brain health most effectively.
Limitation: Relies on cross-sectional study elements.
The Neuroinflammation Pathway
Study: Soliman et al. 2026 (Diabetology & Metabolic Syndrome)
Key Finding: Chronic neuroinflammation (brain inflammation) acts as a central driver in the progression of metabolic dysfunction.
Clinical Value: Reveals a specific therapeutic target for next-generation metabolic treatments.
Limitation: Highly mechanistic and depends heavily on animal models.
The Genetic Link & Destigmatization
Study: Saeed et al. 2025 (Molecular Psychiatry)
Key Finding: Obesity shares a distinct, overlapping genetic architecture with various neurodevelopmental and psychiatric conditions.
Clinical Value: Aids in destigmatizing the condition and opens doors for personalized, precision medicine.
Limitation: Based on Genome-Wide Association Studies (GWAS) showing strong correlation rather than direct causation.
Accelerated Brain Aging & Dementia Prevention
Study: Chen et al. 2026 (Nature Metabolism)
Key Finding: Long-term metabolic dysfunction acts as a catalyst, speeding up neurodegenerative processes in the brain.
Clinical Value: Strengthens the argument that managing metabolic health early is an essential strategy for preventing dementia.
Limitation: Data is derived partly from animal models.
Structural Gray Matter Loss
Study: Majumder et al. 2025 (Brain Research)
Key Finding: Clear MRI evidence proves a distinct relationship between elevated body mass index (BMI) and structural grey matter loss.
Clinical Value: Offers a concrete, objective structural biomarker to track neuroanatomical changes.
Limitation: Cross-sectional design with standard BMI measurement constraints
9. Common Myths and Misconceptions
Myth 1: "Brain changes from obesity are just consequences of laziness." The science is clear: obesity induces measurable neurobiological changes in reward circuitry, inflammatory pathways, and hormonal signaling that actively impair the cognitive and behavioral capacity to lose weight. Framing this as a matter of willpower is factually inaccurate and clinically counterproductive.
Myth 2: "If you lose weight, the brain fully recovers." Partial recovery is likely; full recovery is uncertain. Duration and severity of obesity, age, and the presence of comorbidities all influence the degree of neurological reversibility. Prevention remains more powerful than reversal.
Myth 3: "The obesity paradox means being overweight protects the brain in older age." This is a methodological artifact. Weight loss preceding dementia diagnosis biases cross-sectional studies. Longitudinal data controlling for this reverse causality show that midlife obesity is harmful, not protective.
Myth 4: "Brain scans can diagnose obesity-related damage." Currently, no clinical brain imaging protocol is validated as a diagnostic tool specifically for obesity-related neurological damage. MRI findings from research settings are not yet clinically actionable in routine practice.
Myth 5: "Only severe obesity affects the brain." Evidence suggests a dose-response relationship — even overweight (BMI 25–29.9) is associated with measurable brain changes, though smaller in magnitude than in obesity.
10. Practical Checklist: Protecting Your Brain
You can act on this evidence today. Here's what the research supports:
Dietary strategies:
[ ] Adopt a Mediterranean or MIND dietary pattern (fish, vegetables, legumes, olive oil, whole grains, nuts)
[ ] Reduce ultra-processed food intake — high-fat, high-sugar foods drive dopaminergic dysregulation
[ ] Maintain adequate omega-3 fatty acid intake (anti-neuroinflammatory effects)
[ ] Avoid extended periods of hypercaloric eating, especially in midlife
Physical activity:
[ ] Aim for 150+ minutes/week of moderate aerobic exercise (promotes hippocampal neurogenesis via BDNF)
[ ] Include resistance training 2x/week (improves insulin sensitivity, including central)
[ ] Even 20–30 minutes of daily walking reduces inflammatory markers
Metabolic monitoring:
[ ] Track waist circumference, not just BMI (visceral fat is the more harmful phenotype neurologically)
[ ] Screen for insulin resistance, dyslipidemia, and hypertension — addressing these reduces vascular brain risk
[ ] Prioritize sleep: poor sleep drives both obesity and neuroinflammation (aim for 7–9 hours)
Cognitive engagement:
[ ] Maintain social connection (protective against cognitive decline)
[ ] Engage in cognitively challenging activities
[ ] Manage chronic stress (cortisol exacerbates both obesity and hippocampal atrophy)
11. FAQs
Q: Can obesity cause permanent brain damage? Current evidence suggests that some structural and functional brain changes associated with long-duration obesity may be partially — but not fully — reversible. The extent depends on age, duration, and severity of obesity. Early intervention offers the best chance of recovery.
Q: Does losing weight improve memory and cognitive function? Multiple studies show cognitive improvements following significant weight loss, particularly after bariatric surgery. These improvements are seen in domains including memory, attention, and executive function. The mechanisms likely include reduced neuroinflammation and improved insulin signaling.
Q: Is there a connection between obesity and depression or anxiety? Yes. Neuroinflammatory pathways, HPA axis dysregulation, and disrupted reward signaling all create biological links between obesity and mood disorders. The relationship appears bidirectional — depression also increases obesity risk.
Q: Which part of the brain is most affected by obesity? Based on neuroimaging research, the prefrontal cortex and hippocampus show the most consistent and clinically significant changes. These regions govern executive function, decision-making, impulse control, and memory — all relevant to both daily function and long-term cognitive health.
Q: At what age does obesity start affecting the brain? Brain changes can be detected in obese children and adolescents. Midlife obesity (40–60 years) carries the strongest evidence for long-term neurodegeneration risk. However, the brain is dynamic — changes likely begin accumulating from the onset of obesity, regardless of age.
Q: How does exercise protect the brain in the context of obesity? Aerobic exercise stimulates production of brain-derived neurotrophic factor (BDNF), which promotes neurogenesis (new neuron formation) in the hippocampus, reduces neuroinflammatory markers, and improves central insulin sensitivity. These effects are observed even before significant weight loss occurs.
Q: Is the obesity-dementia link proven or just associational? The evidence is associational with increasingly plausible biological mechanisms. Randomized controlled trials proving causation are not feasible for long-term dementia outcomes. However, the convergence of epidemiological, genetic, neuroimaging, and mechanistic data makes the link biologically credible and clinically meaningful.
Q: Do GLP-1 drugs like Ozempic protect the brain? Early evidence is promising. GLP-1 receptor agonists may have direct neuroprotective effects beyond weight loss, including reduced neuroinflammation and improved brain energy metabolism. Clinical trials specifically examining cognitive and neurological outcomes are ongoing. We do not yet have definitive evidence for cognitive protection in humans.
Q: Can the Mediterranean diet reverse obesity-related brain changes? Direct evidence for reversal is limited. However, the Mediterranean diet is one of the most evidence-backed dietary patterns for reducing neuroinflammation, supporting cognitive function, and reducing dementia risk. It is a rational component of any brain-protective obesity management strategy.
Q: Should I get a brain scan if I have obesity? Currently, brain MRI is not part of routine obesity management. Research MRI findings are not yet translated into validated clinical biomarkers or actionable thresholds. Discuss any cognitive concerns with your doctor, who can assess whether neurological evaluation is appropriate.
12. Conclusion and Action Steps
The evidence accumulated through 2024–2026 makes one thing undeniable: obesity is a neurological condition as much as a metabolic one.
From gray matter atrophy to reward system disruption, from neuroinflammation to accelerated neurodegeneration — excess adiposity reshapes the brain in ways that are biologically consequential and clinically underappreciated.
But this knowledge is not cause for despair. It is cause for urgency and precision.
Here's what the science supports as action steps:
Shift the frame: Treat obesity as a neurobiological condition, not a failure of character. This applies to how you talk to yourself and how clinicians talk to patients.
Intervene in midlife: The evidence most strongly supports midlife as the critical window to prevent long-term neurological consequences.
Prioritize aerobic exercise: Even before significant weight loss, exercise triggers BDNF production and reduces neuroinflammation.
Adopt a brain-protective diet: Mediterranean or MIND dietary patterns offer the most evidence-based nutritional approach.
Address metabolic comorbidities: Treating hypertension, insulin resistance, and dyslipidemia is as important for brain health as weight loss itself.
Ask about emerging pharmacotherapy: GLP-1 receptor agonists may offer both metabolic and direct neurological benefits. Discuss with your physician.
Don't wait for symptoms: Neurological changes from obesity often precede detectable cognitive symptoms by years or decades. Prevention is more effective than reversal.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Managing Diabesity: A Complete Guide to Weight Loss and Blood Sugar Control | DR T S DIDWAL
Weight Loss as Immunotherapy: The Science Behind Reversing Chronic Inflammation | DR T S DIDWAL
Your Body Fat Is an Endocrine Organ—And Its Hormones Shape Your Heart Health | DR T S DIDWA
References
Zand, H., Pourvali, K., Shakery, A. et al. Obesity Hacks the Brain's Systems for Weight Loss Resistance. Mol Neurobiol 63, 236 (2026). https://doi.org/10.1007/s12035-025-05570-5
Morys, F., Tremblay, C., Rahayel, S. et al. Neural correlates of obesity across the lifespan. Commun Biol 7, 656 (2024). https://doi.org/10.1038/s42003-024-06361-9
Soliman, A.R., Fahmy, E. & Mahmoud Ahmed, R. The obesity-brain axis: a comprehensive review of neurological complications and therapeutic interventions in metabolic syndrome. Diabetol Metab Syndr 18, 105 (2026). https://doi.org/10.1186/s13098-026-02115-1
Saeed, S., Bonnefond, A. & Froguel, P. Obesity: exploring its connection to brain function through genetic and genomic perspectives. Mol Psychiatry 30, 651–658 (2025). https://doi.org/10.1038/s41380-024-02737-9
Chen, B., Rodríguez-Díaz, A., Schneeberger, M. et al. Obesity as a catalyst for neurodegeneration. Nat Metab 8, 546–558 (2026). https://doi.org/10.1038/s42255-026-01477-0
Majumder, S., Menon, K., & Borotikar, B. Impact of obesity on brain structure: A critical review of the evidence from Magnetic Resonance imaging studies. Brain Research 1865, Article 149823 (2025). https://doi.org/10.1016/j.brainres.2025.149823
Kivipelto, M., Ngandu, T., Fratiglioni, L. et al. Obesity and vascular risk factors at midlife and the risk of dementia and Alzheimer disease. Arch Neurol 62(10):1556–1560 (2005). https://doi.org/10.1001/archneur.62.10.1556
Hassing, L.B. et al. Overweight in midlife and risk of dementia: a 40-year follow-up study. Int J Obes 33(8):893–898 (2009).
Kullmann, S., Heni, M., Hallschmid, M. et al. Brain Insulin Resistance at the Crossroads of Metabolic and Cognitive Disorders in Humans. Physiol Rev 96(4):1169–1209 (2016).
Thaler, J.P., Yi, C.X., Schur, E.A. et al. Obesity is associated with hypothalamic injury in rodents and humans. J Clin Invest 122(1):153–162 (2012).
Wang, G.J., Volkow, N.D., Logan, J. et al. Brain dopamine and obesity. Lancet 357(9253):354–357 (2001).
Nummenmaa, L., Karjalainen, T., Isojärvi, J. et al. Brain μ-opioid receptor availability predicts reward sensitivity and motivation in obesity. Nat Commun 13, 7073 (2022).
Morris, M.C., Tangney, C.C., Wang, Y. et al. MIND diet associated with reduced incidence of Alzheimer's disease. Alzheimers Dement 11(9):1007–1014 (2015).
Heyn, P., Abreu, B.C., Ottenbacher, K.J. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 85(10):1694–1704 (2004).
Erickson, K.I., Voss, M.W., Prakash, R.S. et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci 108(7):3017–3022 (2011).
Luppino, F.S., de Wit, L.M., Bouvy, P.F. et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry 67(3):220–229 (2010).
Heymsfield, S.B. & Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N Engl J Med 376(3):254–266 (2017).
Witte, A.V., Fobker, M., Gellner, R. et al. Caloric restriction improves memory in elderly humans. Proc Natl Acad Sci 106(4):1255–1260 (2009).
World Health Organization. Obesity and overweight fact sheet. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (2024).
Wilding, J.P.H., Batterham, R.L., Calanna, S. et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med 384(11):989–1002 (2021).
Last updated: June 2026. This article will be reviewed and updated as new evidence emerges.