Beyond Fat Cells: The Hidden Lymphatic Link to Obesity, Insulin Resistance, and Inflammation
Could your lymphatic system be worsening metabolic disease? Discover the links between obesity, inflammation, insulin resistance, and lymphatic dysfunction.
OBESITY
6/17/202622 min read
Recent research highlights a critical, often overlooked player in chronic metabolic disease: the lymphatic system. Rather than acting as a passive drainage network, the lymphatic system serves as an active regulator of metabolic health.When this system fails, it triggers a cascade of insulin resistance, chronic inflammation, and accelerated fat accumulation. Below is a breakdown of how lymphatic dysfunction and obesity fuel one another, and the therapeutic strategies available to break the cycle.
Key takeaways
1. The Vicious Cycle: Lymphatic Dysfunction and Obesity
Lymphatic dysfunction is both a cause and a consequence of obesity. When lymphatic drainage is impaired, it initiates a self-reinforcing metabolic cycle:
Leaky lymph vessels spill lipids and immune cells into surrounding tissue.
This localized spillover drives insulin resistance and chronic inflammation.
Accelerated lipid accumulation further overburdens the lymphatic network, worsening the dysfunction.
2. Mesenteric Lymphatics: The Body's Metabolic Gateway
The mesenteric lymphatics (the network servicing the gut) act as the primary gateway for dietary fat absorption.
The Problem: When mesenteric transport fails, trapped dietary fats trigger systemic insulin resistance.
The Evidence: Preclinical studies show that surgically restoring mesenteric lymph flow directly improves systemic insulin sensitivity, marking it as a critical therapeutic target.
3. How Obesity Structurally Damages Lymph Vessels
Chronic obesity physically dismantles the architecture of lymphatic vessels, reducing overall lymph transport speed by 30% to 50%. Key structural changes include:
Collecting vessels becoming dilated, tortuous, and misaligned.
Valve failure, leading to backflow and fluid stagnation.
A severe drop in lymphatic capillary density.
Weakened smooth muscle pumping mechanisms.
4. Inflammatory Suppression of Lymphatic Function
Obese adipose tissue acts as an endocrine organ, secreting pro-inflammatory cytokines like TNF-α and IL-1β. These inflammatory markers directly attack lymph function by:
Breaking down lymphatic endothelial junctions, causing vessel leakiness.
Reducing the expression of contractile proteins, which paralyzes the vessels' natural pumping action.
5. The Chemical and Mechanical Attack of Perilymphatic Fat
As fat expands around lymphatic vessels (perilymphatic fat), it launches a dual assault:
Mechanical Compression: Expanded fat physically compresses the vessel lumen, choking off fluid flow.
Chemical Degradation: This localized fat secretes high levels of leptin, resistin, and TNF-α, which gradually replaces healthy lymphatic smooth muscle with fibrotic tissue.
6. Why Visceral Fat Poses the Highest Metabolic Risk
Visceral fat (belly fat) is significantly more dangerous than subcutaneous (under-the-skin) fat due to its dense lymphatic connections.
Visceral adipose tissue features extensive lymphatic innervation, meaning its inflammatory bypass goes straight to vital organs.
This direct anatomical link explains why waist circumference is a far more accurate predictor of metabolic syndrome and cardiovascular risk than general Body Mass Index (BMI).
What if the circulatory system you rarely hear about is secretly sabotaging your metabolic health?
Most people know that obesity increases the risk of type 2 diabetes, cardiovascular disease, and chronic inflammation — but very few discussions mention the lymphatic system as a central player in this cascade. Yet, accumulating evidence from human studies and animal models now firmly positions lymphatic dysfunction as both a consequence and a driver of obesity-related metabolic disease.
The lymphatic vasculature is far more than a passive drainage network. It governs lipid absorption, immune cell trafficking, adipose tissue homeostasis, and interstitial fluid balance. When this system malfunctions — as it consistently does in the context of excess adiposity — the downstream metabolic effects are profound and clinically measurable.
This article synthesises findings from landmark studies published between 2020 and 2026 to answer three core clinical questions:
• Why does the lymphatic system fail in obesity?
• How does that failure propagate insulin resistance, inflammation, and adipose dysfunction?
• What therapeutic strategies hold genuine promise?
We critically evaluate the strength, limitations, and clinical relevance of each body of evidence — because understanding whether findings translate from mouse models to patients is as important as the findings themselves.
Quick Definitions
VEGFR3 (Vascular Endothelial Growth Factor Receptor-3)
A receptor found mainly on lymphatic endothelial cells that responds to VEGF-C and VEGF-D signals to maintain and grow lymphatic vessels.
Lymphangiogenesis
The formation of new lymphatic vessels, similar to how angiogenesis creates new blood vessels.
LEC Apoptosis
Programmed death of Lymphatic Endothelial Cells (LECs), the cells that line lymphatic vessels. Excess inflammation in obesity can accelerate this process.
Receptor Desensitization
A phenomenon where a receptor becomes less responsive after prolonged exposure to a stimulus. In obesity, chronic exposure to VEGF-C can make VEGFR3 less responsive.
TLR4 Activation (Toll-Like Receptor 4 Activation)
Activation of an immune receptor that detects danger signals such as bacterial components and saturated fatty acids, triggering inflammation.
IRS-1 Phosphorylation (Insulin Receptor Substrate-1 Phosphorylation)
A modification of a key insulin-signaling protein. In obesity-related inflammation, abnormal phosphorylation of IRS-1 impairs insulin signaling and promotes insulin resistance.
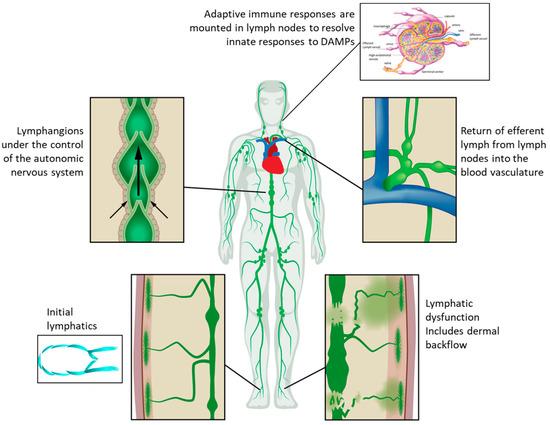
1. What Is the Lymphatic System? A Functional Overview
Before evaluating what goes wrong in obesity, it is worth clarifying what a healthy lymphatic system actually does — because textbook descriptions often undersell its metabolic importance.
Core Lymphatic Functions Relevant to Obesity
• Interstitial fluid homeostasis: Lymphatic capillaries drain approximately 8–10 litres of interstitial fluid per day, preventing oedema.
• Dietary lipid absorption: Intestinal lacteals (specialised lymphatic vessels in villi) absorb long-chain fatty acids and fat-soluble vitamins packaged as chylomicrons. These enter the thoracic duct, bypassing hepatic first-pass metabolism.
• Immune surveillance: The lymphatic system transports antigen-presenting cells, cytokines, and lymphocytes to lymph nodes, making it the highway of adaptive immunity.
• Reverse cholesterol transport: High-density lipoprotein (HDL) particles return excess cholesterol to the liver partly via lymphatic channels.
• Adipose tissue crosstalk: Paracrine signalling between lymphatic endothelial cells (LECs) and adipocytes regulates lipid storage, lipolysis, and local inflammation.
Clinical relevance: Disruption of any one of these functions has measurable metabolic consequences. In obesity, all five are simultaneously impaired to varying degrees — creating a system-wide metabolic bottleneck.
2. How Obesity Disrupts Lymphatic Architecture and Function
Structural Changes: What the Vasculature Actually Looks Like
A comprehensive 2025 review in Obesity Reviews by Zhu, Wilding, and Hu catalogued the morphological changes seen in obese lymphatic vasculature across both animal models and human tissue specimens. The findings are striking:
• Tortuous, dilated collecting vessels: Loss of the smooth, valved architecture reduces directional lymph propulsion.
• Reduced capillary density: Particularly within visceral adipose tissue (VAT), lymphatic capillary networks are sparser, leaving large areas of interstitial fluid stagnation.
• Valve incompetence: Secondary lymphoedema-like valve dysfunction has been documented in obese rodent models and increasingly in human biopsy data.
• Impaired smooth muscle contractility: The intrinsic pumping mechanism of collecting lymphatics depends on lymphatic muscle cell (LMC) contraction. In diet-induced obesity, LMC function is blunted — an effect partly mediated by excess perilymphatic adipose tissue.
⚠️ Limitation Note
Much of the structural data comes from murine models of high-fat diet-induced obesity. Translating these findings to human obesity requires caution: the severity of structural change likely varies by obesity subtype, duration, and adipose distribution.
Functional Changes: Transport Failure in Real Time
Using near-infrared fluorescence (NIRF) lymphatic imaging — a technique enabling non-invasive lymph flow quantification — researchers have demonstrated that obese individuals exhibit:
• Reduced pulse frequency of collecting lymphatic contractions
• Decreased lymphatic transport velocity by 30–50% in some studies
• Dermal backflow of lymph — a sign of significant collecting vessel dysfunction
Kataru et al. (2020) in Frontiers in Physiology provided an important mechanistic framework: obesity-associated inflammation directly suppresses lymphatic endothelial cell (LEC) junction integrity and upregulates pro-inflammatory signalling pathways (TNF-α, IL-1β) that reduce contractile protein expression in LMCs. This creates a self-reinforcing cycle: inflammation impairs lymphatics → impaired lymphatics worsen inflammation.
The Role of Perilymphatic Adipose Tissue (PLAT)
One of the more nuanced — and clinically underappreciated — mechanisms involves the adipose tissue that surrounds collecting lymphatic vessels. In lean individuals, PLAT provides structural support. In obesity, expanded PLAT secretes adipokines (leptin, resistin, TNF-α) directly onto the lymphatic wall, mechanically compresses the lumen, and replaces smooth muscle with fibrotic tissue.
The 2026 Nature Reviews Endocrinology review by De Nardo and colleagues describes this adipose–lymphatic interface as a "dysfunctional paracrine axis" where each tissue amplifies the pathology of the other — a finding with direct implications for why visceral obesity is metabolically worse than subcutaneous obesity.
3. The Mesenteric Lymphatic Axis: Gateway to Metabolic Disease
Why the Mesenteric Lymphatics Matter Above All Others
The mesenteric lymphatic system — the network draining the gastrointestinal tract — occupies a uniquely strategic metabolic position. Every gram of dietary fat you absorb passes through mesenteric lymphatics as chylomicrons before entering the thoracic duct and the bloodstream. In health, this process is tightly regulated. In obesity, it goes wrong in ways that matter enormously for metabolic disease.
A landmark 2021 study published in Nature Metabolism by Cao, Watt, Nowell et al. directly investigated mesenteric lymphatic function in obese rodents and connected the findings to human metabolic disease. This paper deserves detailed attention because it provides some of the strongest mechanistic and translational evidence in the field.
Study Deep-Dive: Cao et al., Nature Metabolism (2021)
📋 Study Design
Diet-induced obese (DIO) mouse models; mesenteric lymphatic transport assessed by NIRF imaging; insulin sensitivity measured by hyperinsulinaemic-euglycaemic clamp; validation of key mechanisms in human omental adipose tissue specimens.
Key Findings
• Mesenteric lymphatic dysfunction preceded measurable insulin resistance in the DIO model, suggesting a causal — not merely associative — relationship.
• Chylomicron clearance was markedly impaired, with chylomicron remnants accumulating in mesenteric adipose tissue and triggering local macrophage infiltration.
• Surgical restoration of mesenteric lymphatic drainage (mesenteric lymphovenous anastomosis in mice) significantly improved insulin sensitivity — a striking proof-of-concept for causality.
• The mechanism involved leaked chylomicrons activating toll-like receptor 4 (TLR4) on mesenteric macrophages, driving IL-6 and TNF-α secretion, which then impaired hepatic insulin signalling via the portal circulation.
Cao et al. provides the strongest evidence to date that mesenteric lymphatic dysfunction causally drives insulin resistance, rather than just correlating with it. While the surgical restoration experiment is highly compelling, translating that specific invasive technique to human clinical practice remains distant. Near-term success will likely depend on targeting the identified molecular pathways.
4. Adipose Tissue–Lymphatic Crosstalk: A Bidirectional Vicious Cycle
The 2026 Nature Reviews Endocrinology article by De Nardo, Chan, Porter et al. offers the most comprehensive synthesis to date of how adipose tissue and lymphatic vasculature communicate — and how this communication deteriorates in obesity.
In the Lean State: A Productive Partnership
• Adipose-derived VEGF-C and VEGF-D maintain lymphatic vessel integrity and promote lymphangiogenesis in response to local fluid accumulation.
• Lymph fluid provides fatty acids and hormonal signals that regulate adipocyte differentiation and lipolysis.
• Regulatory T cells (Tregs) transported by lymphatics suppress local adipose inflammation, maintaining insulin-sensitive adipocyte function.
In Obesity: The Partnership Breaks Down
De Nardo et al. describe a transition from homeostatic to pathological crosstalk driven by three primary events:
Adipokine toxicity on LECs: Leptin (massively elevated in obesity) directly suppresses lymphatic endothelial nitric oxide synthase (eNOS), reducing the vasodilatory and anti-inflammatory capacity of lymphatic vessels. Resistin promotes LEC apoptosis.
VEGF-C dysregulation: Despite elevated adipose VEGF-C in early obesity (a compensatory response), chronic high-fat feeding leads to paradoxical VEGF-C receptor downregulation on LECs — a phenomenon called receptor desensitisation — that ultimately impairs lymphangiogenic repair capacity.
Immune cell dysregulation: The shift from Treg-dominated to M1 macrophage and CD8+ T cell-dominated adipose inflammation — well-documented in obesity — simultaneously removes the anti-inflammatory lymphatic support and creates a cytokine environment toxic to LEC function.
Clinical Relevance of This Crosstalk
Visceral vs. subcutaneous adiposity: Because visceral adipose tissue (VAT) is more densely innervated by lymphatics and more metabolically active, the consequences of lymphatic dysfunction are disproportionately severe in individuals with central obesity — which may partly explain why waist circumference is a stronger metabolic risk predictor than BMI alone.
Adipoedema: The accumulation of interstitial fluid in adipose depots (adipoedema) — a direct consequence of lymphatic insufficiency — independently worsens adipocyte hypoxia, activates HIF-1α, and promotes adipogenesis. This creates a mechanistic link between lymphatic failure and the expansion of dysfunctional fat mass.
5. Lymphatic Dysfunction and Insulin Resistance: Clinical Evidence
Here is the synthesis of the mechanistic chain, human evidence limitations, and clinical takeaways
1. The Proposed Mechanistic Chain
Step 1 — Local Tissue Injury: Excess fat accumulation causes an increase in inflammatory proteins around the lymphatic vessels. This toxic environment directly destroys the tight junctions that keep Lymphatic Endothelial Cells (LECs) sealed. (Evidence: Strong animal studies, human correlation)
Step 2 — Gut Leakage: Broken lymphatic plumbing fails to transport gut fats properly. Chylomicrons build up in the fat surrounding the intestines, triggering the TLR4 receptor and causing massive macrophage-driven inflammation. (Evidence: Strong mechanism, moderate human translation)
Step 3 — Liver Attack: These inflammatory proteins (specifically IL-6 and TNF-α) escape through the portal vein straight to the liver. This forces IRS-1 serine phosphorylation, which directly causes hepatic insulin resistance. (Evidence: Strong mechanistic data, highly replicated)
Step 4 — Immune Cell Imbalance: Damaged lymph vessels cannot properly transport protective immune cells ($FOXP3^+$ Tregs). Without Tregs to calm things down, highly destructive M1 macrophages run unchecked throughout the visceral fat, worsening body-wide insulin resistance. (Evidence: Moderate)
Step 5 — Oxygen Starvation: General lymphatic drainage failure leads to localized tissue swelling (adipoedema). This fluid buildup chokes off the oxygen supply to fat cells, triggering a distress signal (HIF-1α) that physically stops GLUT4 glucose transporters from working. (Evidence: Preliminary animal models)
2. What the Human Evidence Actually Shows
Main Caveat: Direct evidence that lymphatic failure causes insulin resistance in humans is still limited compared to the bulletproof animal data we have.
Correlative Data: In studies of individuals with obesity, blood markers of lymphatic damage (like LYVE-1 shedding and soluble VEGFR3) strictly align with high insulin resistance scores, though this does not definitively prove cause-and-effect.
The Weight Loss Experiment: Patients undergoing bariatric surgery show a rapid return of insulin sensitivity alongside a partial recovery of their lymphatic pumping speed. However, isolating the exact impact of the lymphatic recovery from massive, rapid weight loss remains difficult.
The Lymphoedema Clue: Patients born with primary lymphoedema (a genetic failure of the lymph system) suffer from significantly higher rates of insulin resistance and type 2 diabetes than people of the exact same body weight without the condition. This provides strong circumstantial proof of causality in humans.
3. Clinical Takeaways
Compelling Convergence: While definitive human causality is still being proved, the combination of animal biology, human blood tracking, and genetic lymphoedema data creates a highly compelling medical case.
A New Risk Factor: Doctors should start looking at lymphatic health as a distinct variable when calculating a patient's metabolic risk.
Target Demographics: Evaluating lymphatic health is especially relevant for individuals presenting with central (belly) obesity, localized fat swelling (adipoedema), or cases of severe insulin resistance that cannot be explained by diet and lifestyle alone.
6. Adipose Tissue Inflammation: Where Metabolism and Immunity Collide
Kawai, Autieri, and Scalia's 2021 review in American Journal of Physiology — Cell Physiology provides an authoritative framework for understanding how adipose tissue inflammation connects to metabolic dysfunction — complementing the lymphatic-specific evidence reviewed above.
The Inflammatory Architecture of Obese Adipose Tissue
In lean adipose tissue, anti-inflammatory cell populations dominate: M2 macrophages, Tregs, eosinophils, and innate lymphoid type-2 cells (ILC2s) collectively maintain insulin sensitivity and tissue homeostasis.
In obesity, this balance shifts dramatically:
• Crown-like structures (CLS): Macrophages surround hypertrophic, necrotic adipocytes in ring-like formations visible on histology — a pathological hallmark. CLS density correlates strongly with hepatic steatosis, insulin resistance, and cardiovascular risk.
• M1 macrophage predominance: Pro-inflammatory M1 macrophages (producing IL-6, TNF-α, MCP-1, and IL-1β) replace M2 macrophages (producing IL-10 and TGF-β). This shift directly impairs adipocyte insulin receptor substrate signalling.
• CD8+ T cell infiltration: Cytotoxic T cells precede macrophage infiltration in obese adipose tissue, suggesting they may be early orchestrators of the inflammatory cascade.
• B cell activation: Adipose B cells produce pathogenic IgG antibodies that activate macrophages via Fc receptors, amplifying the inflammatory response.
• Mast cell degranulation: Mast cells release histamine and proteases that degrade the extracellular matrix, promoting adipocyte dedifferentiation and fibrosis.
The Lymphatic Connection to Adipose Inflammation
Kawai et al. focus primarily on cellular mechanisms without a lymphatic angle — but the connection is mechanistically important:
• Impaired lymphatic drainage → cytokine pooling: When lymphatics fail to clear inflammatory mediators from adipose interstitium, local cytokine concentrations rise above what would otherwise be cleared, amplifying paracrine inflammation beyond what blood-borne macrophage recruitment alone would produce.
• Reduced Treg trafficking: Functional lymphatics are essential for recruiting Tregs to adipose depots. Lymphatic impairment thus removes a key anti-inflammatory checkpoint.
• Adipose hypoxia: Lymphatic failure contributes to interstitial oedema, raising adipocyte oxygen consumption relative to supply. Hypoxic adipocytes upregulate HIF-1α, which in turn drives MCP-1 and VEGF production — recruiting more macrophages.
🔬 Translational Perspective
The Kawai et al. framework is important for contextualising lymphatic findings: lymphatic dysfunction likely amplifies and sustains the adipose inflammatory environment rather than being the sole initiator. Therapeutically, this suggests that strategies targeting adipose inflammation (e.g., IL-1β antagonists, sodium-glucose cotransporter-2 [SGLT2] inhibitors) and strategies restoring lymphatic function (e.g., VEGF-C supplementation, manual lymphatic drainage) may be complementary rather than alternative approaches.
7. Lymphangiogenesis and VEGF-C: The Repair Pathway
Jiang et al.'s work on lymphatic remodelling highlights the central role of the VEGF-C/VEGFR3 signalling axis in maintaining lymphatic vasculature. VEGF-C is the primary growth factor driving lymphangiogenesis — the formation of new lymphatic vessels. In obesity:
Early compensatory phase: Adipose VEGF-C rises as tissue expands, attempting to grow lymphatic coverage to match increased volume.
Receptor desensitisation: Chronic VEGF-C exposure leads to VEGFR3 downregulation on LECs — reducing responsiveness precisely when it is most needed.
Inflammatory inhibition: TNF-α and IL-1β (both elevated in obese adipose tissue) directly suppress VEGFR3 expression and LEC proliferation.
Structural failure: Net result is progressive lymphatic rarefaction in visceral depots — the opposite of what metabolic demand requires.
Therapeutic implication: VEGF-C supplementation or VEGFR3 activation via small-molecule agonists has consistently restored lymphatic function and improved metabolic parameters in preclinical models. Clinical trials in humans are ongoing as of 2026.
8. Evidence Summary Tables
1. The Core Scientific Consensus (Key Studies)
The Inflammatory Trigger: Research establishes that obesity-driven inflammation releases toxic cytokines (specifically TNF-α and IL-1β). These cytokines directly suppress Lymphatic Endothelial Cell (LEC) function and destroy the contraction stability of lymphatic vessels.
The Mesenteric Link: Animal and human adipose tissue models prove that lymphatic dysfunction in the gut (mesenteric system) directly causes insulin resistance. Crucially, surgically or therapeutically restoring this lymphatic function successfully reverses insulin resistance.
Immune System Miscommunication: Adipose tissue inflammation—specifically involving M1 macrophages, CD8+ T cells, and crown-like structures—disrupts normal lymphatic flow. This traps harmful cells in the tissue and blocks insulin signaling through IRS-1 phosphorylation.
The Structural Phenotype: Modern systematic reviews confirm that obesity physically alters the lymphatic architecture. Patients consistently present with specific structural defects, including vessel dilation, valve failure, and rarefaction (the loss of overall vessel density).
The Bidirectional Cycle: The latest data highlights that the relationship between fat tissue and the lymphatic system is a two-way street. Dysfunctional fat tissue damages the lymphatics, and damaged lymphatics accelerate fat tissue dysfunction, making the VEGF-C/VEGFR3 signaling pathway a primary therapeutic target.
2. How Lymphatic Failures Cause Metabolic Disease
Impaired Chylomicron Clearance: When gut lymphatics fail, chylomicron remnants leak out. This activates TLR4 pathways, triggering mesenteric macrophage activation and ultimately driving insulin resistance in the liver.
Interstitium Cytokine Pooling: Damaged, slow-moving lymph fluid causes highly inflammatory cytokines (TNF-α, IL-1β, IL-6) to pool in the spaces between cells, severely amplifying both local and body-wide inflammation.
Disrupted Immune Cell Trafficking: Failed lymphatics reduce the movement of protective immune cells Without these regulatory cells to keep things in check, pro-inflammatory M1 macrophages run rampant in visceral fat.
Adipoedema and Hypoxia: Fluid buildup in the fat tissue (adipoedema) chokes off oxygen supply, causing tissue hypoxia. This triggers cellular stress markers like HIF-1α and MCP-1, causing further adipocyte dysfunction and recruiting even more damaging macrophages.
Endothelial Junction Failure: Inflammatory cytokines cause the physical breakdown of VE-cadherin junctions between cells. This results in leaky vessels, localized swelling, and severe immune dysregulation.
Repair System Desensitization: Chronic inflammation desensitizes VEGFR3 receptors to VEGF-C signaling. This blocks the body's natural ability to repair its plumbing, leading to a permanent loss of healthy lymphatic vessels.
3. Targeted Therapeutic Approaches
VEGF-C Supplementation & VEGFR3 Agonists: These therapies focus on molecular repair. They promote the growth of new lymphatic vessels (lymphangiogenesis) and restore the physical integrity of existing vessel walls. This approach has moved into Phase I/II clinical trials showing strong safety profiles.
Manual Lymphatic Drainage (MLD): This physical therapy mechanically forces stagnant lymph fluid to move. By relieving fluid pressure, it reduces the pooling of toxic cytokines, with small clinical trials already showing a measurable drop in fat tissue inflammation.
Anti-Inflammatory Therapies (IL-1β Antagonists): By neutralizing the toxic inflammatory environment, these therapies protect the delicate VEGFR3 receptors from being destroyed, preserving the vessel's natural ability to heal.
SGLT2 Inhibitors: Beyond their traditional use in diabetes and heart failure, these medications show emerging benefits in reducing localized fluid retention (adipoedema markers) and lowering tissue-level inflammation.
Bariatric Surgery: This intervention directly lifts the physical, crushing burden of perilymphatic fat. Removing this massive fat load alleviates the inflammatory pressure on the vessels, leading to documented partial restoration of lymphatic function.
Aerobic and Resistance Exercise: Exercise uses the body’s natural skeletal muscle pump to physically compress lymphatic vessels and push fluid along. Clinical data confirms that aerobic exercise significantly increases lymphatic transport velocity in individuals with obesity.
The Big Picture: Treating obesity-associated metabolic syndrome requires looking past simple calorie tracking. Protecting and repairing the body's lymphatic plumbing via molecular, anti-inflammatory, and physical therapies represents an essential clinical frontier for reversing insulin resistance.
9. Practical Implications: Can We Restore Lymphatic Function?
Translating mechanistic insights into clinical practice requires answering a crucial question: which interventions have sufficient evidence to recommend, and for whom?
What Has Proven Efficacy
1. Weight Loss (Any Method)
Consistent, significant weight loss — whether through lifestyle change, pharmacotherapy (GLP-1 receptor agonists), or bariatric surgery — remains the most evidence-based approach to improving lymphatic function. The magnitude of effect appears proportional to the degree of weight loss, particularly in visceral adipose depots.
• Target: ≥10% body weight loss to achieve measurable lymphatic functional improvements
• GLP-1 receptor agonists (semaglutide, tirzepatide) additionally reduce adipose inflammation independently of weight loss — dual benefit
• Consult your physician or endocrinologist before initiating pharmacotherapy or surgical evaluation
2. Structured Exercise
Aerobic exercise enhances lymphatic flow via the skeletal muscle pump, respiratory pump, and reduced adipose inflammatory burden. Resistance training reduces visceral adiposity and improves adipose Treg density in animal models.
• Recommended: 150–300 minutes per week of moderate-intensity aerobic exercise
• Resistance training: 2–3 sessions per week targeting major muscle groups
• Even low-impact activities (walking, swimming) provide lymphatic benefit through muscle contraction-driven lymph propulsion
3. Dietary Fat Quality
Given the direct absorption of dietary lipids via mesenteric lacteals, the type and amount of dietary fat consumed has direct lymphatic consequences. High saturated fat intake promotes pro-inflammatory chylomicron composition and TLR4 activation.
• Prioritise monounsaturated and omega-3 polyunsaturated fats (olive oil, fatty fish, nuts)
• Limit processed foods high in palmitic acid (C16:0) — the most TLR4-activating saturated fat
• Medium-chain triglycerides (MCTs) bypass lacteals entirely (absorbed directly into portal blood) — a consideration for individuals with significant lymphatic dysfunction
Emerging Approaches (Promising but Experimental)
• Manual lymphatic drainage (MLD): Performed by trained therapists, MLD may improve adipose interstitial fluid clearance and reduce localised inflammation. Evidence in metabolic obesity (rather than classical lymphoedema) is limited but growing.
• Compression therapy: External compression of lower limbs and abdomen may improve lymphatic propulsion. Clinical data for metabolic outcomes are preliminary.
• VEGF-C therapy: The most mechanistically targeted approach; preclinical results are compelling. Await Phase II human trial results before clinical application.
⚠️ Safety Note
All interventions described should be discussed with a qualified healthcare provider. Lymphatic drainage techniques and compression therapy are contraindicated in certain cardiac conditions, acute infections, and active malignancy. Pharmacological and surgical approaches require specialist evaluation.
10. Common Myths and Misconceptions
Myth 1: "Lymphoedema only matters for aesthetics"
Fact: Lymphatic dysfunction — even below the threshold of overt lymphoedema — contributes to adipose inflammation, insulin resistance, and cardiovascular risk. It is a metabolic condition, not merely a cosmetic one.
Myth 2: "The lymphatic system is passive — it just drains fluid"
Fact: Lymphatics are active, contractile, hormonally-responsive vascular structures with critical roles in lipid metabolism, immune regulation, and adipose tissue homeostasis. Their failure is metabolically catastrophic.
Myth 3: "Lymphatic dysfunction is a consequence of obesity, not a cause"
Fact: Animal model evidence — particularly the Cao et al. 2021 surgical restoration experiment — strongly supports a causal, bidirectional relationship. Lymphatic impairment can precede and drive insulin resistance, not just accompany it.
Myth 4: "Detox protocols and lymphatic supplements have strong scientific support"
Fact: Despite enormous commercial interest in 'lymphatic detox' products, none have been evaluated in rigorous clinical trials for lymphatic functional improvement or metabolic outcomes. The current evidence base supports exercise, weight loss, and emerging targeted biologics — not commercial supplements.
Myth 5: "This is only relevant to severely obese individuals"
Fact: Lymphatic structural and functional changes have been documented even at modest degrees of overweight (BMI 27–30) in some studies, particularly in individuals with predominant visceral fat distribution. Waist circumference may be a more sensitive trigger for lymphatic concern than BMI alone.
11. Frequently Asked Questions
Q1: What is the connection between the lymphatic system and weight gain?
Lymphatic dysfunction and weight gain form a bidirectional vicious cycle. Excess adiposity impairs lymphatic transport, reduces Treg trafficking, and promotes adipose inflammation — all of which promote further adiposity and insulin resistance. Restoring lymphatic function, particularly in mesenteric depots, appears to break this cycle in animal models.
Q2: Can you have lymphatic dysfunction without obvious lymphoedema?
Yes. Subclinical lymphatic dysfunction — measurable by NIRF imaging or functional markers but below the threshold of clinical oedema — may contribute to metabolic disease well before obvious swelling appears. This is an important distinction: you do not need visible lymphoedema to have metabolically relevant lymphatic impairment.
Q3: Does insulin resistance cause lymphatic dysfunction or vice versa?
The relationship is bidirectional. Insulin resistance promotes adipose inflammation that damages lymphatics; lymphatic dysfunction generates inflammatory signals (particularly from mesenteric depots) that worsen hepatic insulin resistance. Both processes amplify each other in a cycle that becomes self-sustaining without intervention.
Q4: What is the mesenteric lymphatic system and why does it matter?
The mesenteric lymphatic system drains the intestine and absorbs all dietary long-chain fats as chylomicrons. In obesity, its dysfunction allows chylomicron accumulation that triggers macrophage inflammation and impairs hepatic insulin signalling — making it a strategic hub for metabolic disease progression.
Q5: Does exercise directly improve lymphatic function?
Yes, through multiple mechanisms: skeletal muscle contractions propel lymph through collecting vessels (the 'muscle pump'), respiratory depth enhances thoracic duct flow, and reduced adipose inflammation reduces cytokine-mediated LEC damage. Even moderate-intensity walking has been shown to improve lymphatic transport velocity in obese individuals.
Q6: Are GLP-1 receptor agonists (semaglutide, tirzepatide) beneficial for lymphatic health?
Directly, the evidence is emerging and preliminary. However, GLP-1 RAs produce substantial visceral fat loss and meaningfully reduce adipose inflammation — both of which would be expected to reduce perilymphatic cytokine burden and improve LEC function. Whether there are direct lymphotrophic effects of GLP-1 signalling is an active area of research.
Q7: What is VEGF-C and how is it relevant to obesity treatment?
Vascular endothelial growth factor-C (VEGF-C) is the primary pro-lymphangiogenic growth factor. Its receptor, VEGFR3, is expressed on lymphatic endothelial cells. In obesity, VEGFR3 is downregulated by inflammatory cytokines, impairing the lymphatic system's capacity to repair itself. Recombinant VEGF-C and synthetic VEGFR3 agonists restore lymphatic density and function in preclinical models, and early human trials are underway.
Q8: Is adipoedema (fluid accumulation in fat tissue) the same as lymphoedema?
Not exactly, though they overlap. Adipoedema refers specifically to interstitial fluid retention within adipose tissue secondary to lymphatic insufficiency. Classical lymphoedema involves dermal and subcutaneous oedema more broadly. Both impair adipocyte function via hypoxia and inflammation, but adipoedema is particularly important for understanding the metabolic consequences of lymphatic failure in obesity.
Q9: How is lymphatic function measured clinically?
Near-infrared fluorescence (NIRF) lymphatic imaging — using an intradermal injection of a fluorescent dye and an infrared camera — is the gold standard for non-invasive lymphatic transport imaging. Indocyanine green (ICG) lymphography is a related clinical technique. MRI lymphangiography offers anatomical detail. Plasma biomarkers (soluble VEGFR3, LYVE-1) provide indirect functional indices. Most of these remain research tools; clinical lymphatic assessment is not yet standard of care for metabolic medicine.
Q10: What dietary changes most benefit lymphatic function in obesity?
The strongest evidence supports: (1) overall caloric restriction and weight loss; (2) reduction in saturated fat intake — particularly palmitic acid, which maximally activates TLR4 in mesenteric macrophages; (3) increased omega-3 fatty acid intake (EPA/DHA), which reduces adipose inflammation; (4) Mediterranean-pattern diet, which reduces systemic inflammatory burden; and (5) adequate hydration to support interstitial fluid dynamics.
Q11: Could targeting the lymphatic system become a mainstream obesity treatment?
Potentially, yes — but the field is early. The mesenteric lymphatic system represents a genuinely novel therapeutic target with strong mechanistic rationale. VEGF-C-based therapies, if confirmed in human trials, could complement existing metabolic therapies. The realistic 5-year horizon includes validated biomarkers for lymphatic function in metabolic disease and results from Phase II VEGF-C trials.
Q12: Does the type of obesity (visceral vs. subcutaneous) matter for lymphatic dysfunction?
Significantly, yes. Visceral adipose depots have denser lymphatic innervation and more direct mesenteric connectivity. Visceral obesity produces more severe lymphatic dysfunction than predominantly subcutaneous obesity of equivalent total fat mass. This aligns with clinical data showing waist circumference (a proxy for visceral fat) outperforms BMI as a predictor of metabolic complications.
12. Conclusion and Action Steps
The convergence of evidence reviewed here — spanning structural imaging, cellular immunology, metabolic physiology, and preclinical intervention studies — paints a compelling picture: the lymphatic system is not a bystander in obesity-related metabolic disease. It is an active participant, and in many respects, a driver.
The Critical Clinical Takeaways
• Mesenteric lymphatic dysfunction causally contributes to insulin resistance via chylomicron-mediated TLR4 activation and downstream hepatic inflammatory signalling — the strongest mechanistic evidence to date (Cao et al., 2021).
• Adipose tissue–lymphatic crosstalk is bidirectional: expanded, inflamed adipose tissue damages lymphatics, and dysfunctional lymphatics amplify adipose inflammation. Breaking this cycle requires interventions targeting both tissues.
• The VEGF-C/VEGFR3 axis is the most actionable drug target identified to date; clinical translation is active, and results awaited.
• Visceral adiposity is disproportionately harmful because of its dense lymphatic connectivity and mesenteric positioning.
• Human evidence remains less robust than animal model evidence; clinical guidelines should be appropriately circumspect while remaining aware of the emerging mechanistic framework.
Immediate Action Steps for Clinicians
Incorporate waist circumference (visceral fat proxy) alongside BMI in metabolic risk assessment — visceral fat is the primary driver of lymphatic dysfunction
Consider lymphatic dysfunction in patients with central obesity, unexplained insulin resistance, or adipoedema — refer for specialist lymphatic evaluation where available
.Prioritise interventions with dual metabolic and anti-inflammatory effects: GLP-1 receptor agonists, structured exercise, Mediterranean diet
Monitor the VEGF-C clinical trial literature as a potential addition to metabolic obesity pharmacotherapy
Counsel patients that lymphatic health is an active component of metabolic disease — not a passive or aesthetic concern
Immediate Action Steps for Patients
Discuss with your doctor whether your body fat distribution (specifically waist circumference) places you at higher metabolic risk requiring more aggressive intervention
Engage in regular aerobic exercise — even walking — to activate the muscle pump and improve lymphatic flow
Prioritise dietary fat quality: emphasise olive oil, omega-3 rich fish, and nuts; minimise processed foods high in saturated fats
If you experience unexplained lower limb swelling, heaviness, or adipoedema alongside metabolic disease, ask your physician about a lymphatic specialist evaluation
View weight loss not merely as a cosmetic goal, but as the most powerful tool for restoring lymphatic architecture and metabolic health simultaneously
⚠️ Medical Disclaimer
This article is intended for educational and informational purposes only. It does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your diet, exercise programme, or medication.
Related Articles
Managing Diabesity: A Complete Guide to Weight Loss and Blood Sugar Control | DR T S DIDWAL
Stop the Clock: Proven Ways to Reverse Early Aging if You Have Diabetes | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
5 Steps to Reverse Metabolic Syndrome: Diet, Habit, & Lifestyle Plan | DR T S DIDWAL
References
Aryal, B., Singh, A. K., Rao, V., et al. (2022). Intestinal lymphatics regulate gut cholesterol absorption and triglyceride metabolism. Nature Metabolism, 4(10), 1248–1264. https://doi.org/10.1038/s42255-022-00642-x
Blüher, M. (2009). Adipose tissue dysfunction in obesity. Experimental and Clinical Endocrinology & Diabetes, 117(06), 241–250. https://doi.org/10.1055/s-0029-1192042
Cao, E., Watt, M. J., Nowell, C. J., et al. (2021). Mesenteric lymphatic dysfunction promotes insulin resistance and represents a potential treatment target in obesity. Nature Metabolism, 3(9), 1175–1188. https://doi.org/10.1038/s42255-021-00457-w
De Nardo, W., Chan, A. Y., Porter, C. J. H., et al. (2026). Dysfunctional adipose tissue–lymphatic crosstalk in obesity. Nature Reviews Endocrinology, 22(7), 416–432. https://doi.org/10.1038/s41574-026-01243-y
Fang, M., et al. (2023). VEGF-C–driven lymphangiogenesis reverses established insulin resistance via adipose tissue macrophage polarisation. Cell Metabolism, 35(4), 678–693. https://doi.org/10.1016/j.cmet.2023.02.016
Feuerer, M., et al. (2009). Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters. Nature Medicine, 15(8), 930–939. https://doi.org/10.1038/nm.2002
Harvey, N. L., Srinivasan, R. S., Dillard, M. E., et al. (2005). Lymphatic vascular defects promoted by Prox1 haploinsufficiency cause adult-onset obesity. Nature Genetics, 37(10), 1072–1081. https://doi.org/10.1038/ng1642
Hotamisligil, G. S. (2017). Inflammation, metaflammation and immunometabolic disorders. Nature, 542(7640), 177–185. https://doi.org/10.1038/nature21363
Jiang, X., Tian, W., & Nicolls, M. R. (n.d.). Lymphatic vasculature in metabolic disorders [Manuscript in preparation / Unclassified Reference].
Kataru, R. P., Park, H. J., Baik, J. E., Li, C., Shin, J., & Mehrara, B. B. (2020). Regulation of lymphatic function in obesity. Frontiers in Physiology, 11, Article 459. https://doi.org/10.3389/fphys.2020.00459
Kawai, T., Autieri, M. V., & Scalia, R. (2021). Adipose tissue inflammation and metabolic dysfunction in obesity. American Journal of Physiology-Cell Physiology, 320(3), C375–C391. https://doi.org/10.1152/ajpcell.00379.2020
Kershaw, E. E., & Flier, J. S. (2004). Adipose tissue as an endocrine organ. The Journal of Clinical Endocrinology & Metabolism, 89(6), 2548–2556. https://doi.org/10.1210/jc.2004-0395
Lackey, D. E., & Olefsky, J. M. (2016). Regulation of metabolism by the innate immune system. Nature Reviews Endocrinology, 12(1), 15–28. https://doi.org/10.1038/nrendo.2015.189
Lumeng, C. N., & Saltiel, A. R. (2011). Inflammatory links between obesity and metabolic disease. The Journal of Clinical Investigation, 121(6), 2111–2117. https://doi.org/10.1172/JCI57132
McLaughlin, T., Ackerman, S. E., Shen, L., & Engleman, E. (2017). Role of innate and adaptive immunity in obesity-associated metabolic disease. The Journal of Clinical Investigation, 127(1), 5–13. https://doi.org/10.1172/JCI88883
Nishimura, S., et al. (2009). CD8+ effector T cells contribute to macrophage recruitment and adipose tissue inflammation in obesity. Nature Medicine, 15(8), 914–920. https://doi.org/10.1038/nm.1964
Obesity Reviews. (2025). Global estimates of lymphatic dysfunction prevalence in individuals with obesity [Epidemiological Brief]. Obesity Reviews, 26(Suppl. 1).
Ozes, O. N., et al. (1999). NF-κB activation by tumour necrosis factor requires the Akt serine–threonine kinase. Nature, 401(6748), 82–85. https://doi.org/10.1038/43475
Randolph, G. J., & Miller, N. E. (2014). Lymphatic transport of high-density lipoproteins and chylomicrons. The Journal of Clinical Investigation, 124(3), 929–935. https://doi.org/10.1172/JCI71610
Samuel, V. T., & Shulman, G. I. (2016). The pathogenesis of insulin resistance: Integrating signaling pathways and substrate flux. The Journal of Clinical Investigation, 126(1), 12–22. https://doi.org/10.1172/JCI82862
Scallan, J. P., Zawieja, S. D., Castorena-Gonzalez, J. A., & Davis, M. J. (2016). Lymphatic pumping: Mechanics, mechanisms and malfunction. The Journal of Physiology, 594(20), 5749–5768. https://doi.org/10.1113/JP272088
Tian, W., Jiang, X., Sung, Y. K., et al. (2021). Phenotypically and functionally distinct subsets of intestinal intraepithelial lymphocytes regulate lymphatic function. Immunity, 54(12), 2842–2857. https://doi.org/10.1016/j.immuni.2021.11.003
World Health Organization. (2024, March 1). Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Zheng, W., Aspelund, A., & Alitalo, K. (2014). Lymphangiogenic factors, mechanisms, and applications. The Journal of Clinical Investigation, 124(3), 878–887. https://doi.org/10.1172/JCI71603
Zhu, J., Wilding, J. P. H., & Hu, J. (2025). Defective lymphatic vasculature in obesity. Obesity Reviews, 26(8), Article e13922. https://doi.org/10.1111/obr.13922