Obesity as a Cardiometabolic Disease: New Science & Treatments
Obesity is now recognized as a cardiometabolic disease. Learn how modern therapies reduce diabetes, heart, and kidney risks.
OBESITYMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/26/202624 min read
Cardiometabolic disease refers to the linked cluster of obesity, insulin resistance, type 2 diabetes, heart disease, and kidney disease. According to 2025–2026 research, the most effective treatments are GLP-1 receptor agonists (semaglutide, tirzepatide) and SGLT2 inhibitors, which reduce weight, protect the heart and kidneys, and improve metabolic health far beyond glucose control alone (SELECT, SURMOUNT, DAPA-CKD trials).
Early intervention targeting visceral fat and using multi-organ protective medications offers the best outcomes. Lifestyle changes (Mediterranean diet, resistance training, time-restricted eating) remain foundational
Clinical Pearls:
1. Adopt the CKM Syndrome Framework for Integrated Care.
Cardiovascular, kidney, and metabolic systems form a bidirectional network. Staging patients using the American Heart Association’s CKM framework (Stage 0–4) enables earlier intervention and prioritizes therapies with multi-organ benefits over single-disease targets (Fernando et al., 2025; Pohlman et al., 2025).
2. Prioritize Visceral Adiposity Over Total BMI.
Waist circumference (>90 cm men / >80 cm women in South Asian populations) and Body Roundness Index are superior to BMI for cardiometabolic risk stratification. Visceral fat drives insulin resistance, metaflammation, and endothelial dysfunction more potently than subcutaneous fat (Lin & Tandar, 2026).
3. GLP-1 Receptor Agonists and SGLT2 Inhibitors Provide Additive Cardiorenal Protection.
High-dose semaglutide and tirzepatide achieve 15–22% weight loss with proven MACE reduction (SELECT trial), while SGLT2 inhibitors deliver robust heart failure and CKD protection (DAPA-CKD, EMPEROR-Reduced). Combination therapy should be considered early in patients with overlapping risk factors.
4. Insulin Resistance Precedes and Drives Multiple Manifestations.
Elevated HOMA-IR (>2.5), fasting triglycerides, and hs-CRP are sensitive early markers. Addressing hyperinsulinemia and visceral fat yields broader cardiometabolic benefits than glucose-centric approaches alone (Chakaroun et al., 2026).
5. Not All Weight Loss is Metabolically Equivalent.
Preservation of lean mass and preferential reduction of visceral and hepatic fat (as seen with GLP-1/GIP agonists) produce superior improvements in insulin sensitivity, inflammation, and ectopic fat compared to caloric restriction alone. Long-term pharmacotherapy is often required to prevent weight regain in chronic obesity.
6. Precision Biomarkers Guide Risk Assessment and Therapy Selection.
Routine measurement of ApoB, UACR, hs-CRP, fasting insulin, and eGFR enables detection of subclinical disease. South Asian patients warrant lower thresholds for intervention due to a higher prevalence of “lean metabolic syndrome.”
Bottom Line (2026): Cardiometabolic disease demands a unified, mechanism-based strategy. Early identification of visceral adiposity and insulin resistance, combined with multi-organ protective agents (GLP-1 RAs ± SGLT2i), offers the greatest opportunity to alter long-term trajectories.ining, time-restricted eating) remain foundational.
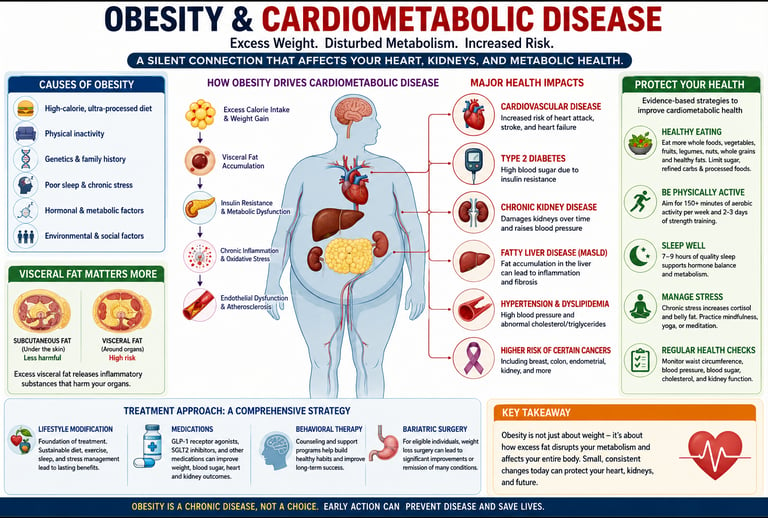
If you have ever been told you have high blood sugar, high blood pressure, or carry extra weight around your abdomen, your doctor may not have told you the full story — these are not separate, unrelated problems. They are chapters in the same book, and that book is called cardiometabolic disease.
Cardiometabolic disease is now recognized as the defining health challenge of the 21st century. It is an umbrella term for the deeply interconnected web of conditions — type 2 diabetes, obesity, cardiovascular disease, and chronic kidney disease — that share the same biological roots and, left unchecked, accelerate each other's progression.
The good news? The science of understanding and treating cardiometabolic disease has never been more powerful. A new generation of therapies — GLP-1 receptor agonists, SGLT2 inhibitors, and groundbreaking triple agonists — are delivering simultaneous benefits across blood sugar, body weight, blood pressure, and kidney health. And early intervention, guided by precision biomarkers, can alter your health trajectory for decades to come.
In this comprehensive guide, you will learn:
What cardiometabolic disease really is and why it cannot be treated in silos
The biological mechanisms driving it, including insulin resistance and visceral fat
The latest 2025–2026 research on breakthrough medications and their multi-organ benefits
Practical, science-backed strategies you can use starting today
How to use biomarkers to detect risk before symptoms appear
Whether you are a patient, a caregiver, or simply someone who wants to stay ahead of chronic disease, this is the most complete resource you will find on cardiometabolic health.
1. What Is Cardiometabolic Disease?
Cardiometabolic disease refers to a cluster of conditions that arise from shared, underlying metabolic dysfunction. Rather than treating type 2 diabetes, heart disease, and kidney disease as separate conditions that happen to co-exist, modern medicine now recognizes them as expressions of the same progressive pathophysiological process.
The five core components of cardiometabolic risk are:
Abdominal (central) obesity
Elevated fasting blood glucose or insulin resistance
High blood pressure (hypertension)
Dyslipidemia (high triglycerides and/or low HDL cholesterol)
Chronic low-grade systemic inflammation
When three or more of these are present together, the condition is called metabolic syndrome — a powerful predictor of future heart attack, stroke, type 2 diabetes, and kidney failure.
Cardiometabolic disease is a term for the interconnected cluster of conditions — including type 2 diabetes, obesity, cardiovascular disease, and chronic kidney disease — that share common biological origins in insulin resistance, inflammation, and metabolic dysfunction.
How common is it? Globally, metabolic syndrome affects approximately 25–35% of adults. In South Asian populations, including India, the prevalence may be even higher due to a genetic predisposition to central adiposity and insulin resistance at lower body weights — a phenomenon researchers call the "lean metabolic syndrome" or "thin-fat Indian" phenotype.
2. The CKM Syndrome Framework: Your Organs Are a Network
One of the most significant conceptual advances in modern medicine is the Cardiovascular-Kidney-Metabolic (CKM) syndrome — a framework that recognizes the heart, kidneys, and metabolic system as a deeply integrated physiological network rather than three separate organ systems.
A 2025 narrative review published in Diabetes Therapy by Fernando et al. articulates this clearly: traditional siloed approaches — treating diabetes separately from heart disease or kidney disease — miss crucial opportunities for synergistic therapeutic benefit. Instead, clinicians must think in terms of the entire cardiometabolic continuum.
How Each System Affects the Others
Organ/System When It Fails What It Does to the Others Metabolic system (insulin, glucose, fat) Insulin resistance, high blood sugar Damages blood vessels, accelerates kidney decline, inflames the heart Cardiovascular system (heart, blood vessels) Hypertension, atherosclerosis Reduces blood supply to kidneys, worsens metabolic clearance Renal system (kidneys) Reduced filtration, proteinuria Causes fluid overload for the heart, worsens hypertension
Think of these three systems as an interconnected electrical grid. A surge — like chronically high blood sugar — does not just damage one appliance. It puts strain on the entire grid, and eventually causes system-wide failures.
The Four Stages of CKM Syndrome
The American Heart Association has formally staged CKM syndrome from Stage 0 (no risk factors) to Stage 4 (established cardiovascular disease with metabolic or kidney dysfunction). This staging framework helps clinicians intervene at the right time — ideally in Stages 1 or 2, before irreversible organ damage occurs.
Key Insight: According to Pohlman et al. (2025), the CKM framework demands a shift in therapeutic decision-making — away from selecting medications based on a single outcome (like HbA1c) and toward choosing agents that optimize outcomes across glucose metabolism, cardiovascular risk, and renal function simultaneously.
3. Visceral Adiposity: Why Fat Location Matters More Than Fat Amount {#visceral-fat}
Not all fat is equal. You can have a "normal" BMI and still carry dangerous amounts of fat deep within your abdominal cavity — and that visceral fat is metabolically far more harmful than subcutaneous fat (the fat you can pinch under your skin).
A landmark 2026 study published in Nature Reviews Endocrinology by Lin and Tandar examined global patterns of visceral adiposity and cardiometabolic disease across diverse populations. The findings were striking: visceral fat accumulation was a stronger predictor of cardiometabolic risk than total body weight or BMI in nearly every population studied.
Why Visceral Fat Is So Dangerous
Visceral fat is metabolically active — it behaves almost like an endocrine organ. It secretes pro-inflammatory cytokines (such as TNF-α, IL-6, and resistin), disrupts insulin signaling, raises blood pressure, promotes dyslipidemia, and drives the systemic inflammation that underpins cardiometabolic disease progression.
How to Measure Visceral Fat Risk Without a Scanner
You do not need a DEXA scan or MRI to estimate visceral fat risk. Simpler proxies include:
Waist circumference: >90 cm (men) or >80 cm (women) signals elevated risk in South Asian populations (lower thresholds than Western guidelines)
Waist-to-hip ratio: >0.90 (men) or >0.85 (women) indicates central adiposity
Body Roundness Index (BRI): An emerging measurement that accounts for height and waist circumference and may be more accurate than BMI for predicting cardiometabolic risk
4. The Biological Mechanisms Driving Cardiometabolic Disease
Understanding why cardiometabolic disease develops — not just what it is — is essential for choosing effective prevention and treatment strategies.
Insulin Resistance: The Central Driver
Insulin resistance occurs when cells no longer respond efficiently to insulin's signal to absorb glucose from the bloodstream. The pancreas compensates by producing more insulin, creating hyperinsulinemia — high circulating insulin levels that themselves promote fat storage, hypertension, and dyslipidemia.
Over time, pancreatic beta cells exhaust themselves, blood glucose rises unchecked, and type 2 diabetes develops. But long before the diabetes diagnosis, insulin resistance has already been silently damaging blood vessels, kidneys, and the heart.
Mitochondrial Dysfunction
Mitochondria are the cell's energy factories, and their impaired function is a central feature of cardiometabolic disease. When mitochondria malfunction, cells produce excess reactive oxygen species (free radicals), which damage cellular membranes, impair insulin signaling, and promote inflammation — creating a self-reinforcing cycle of metabolic deterioration.
Adipose Tissue Inflammation
In obesity, fat cells (adipocytes) enlarge and become stressed, releasing inflammatory signals that recruit immune cells (particularly macrophages) into adipose tissue. This creates a chronic, low-grade inflammatory state — sometimes called "metaflammation" — that acts as a key upstream driver of cardiometabolic pathology.
A 2026 study in Nature Medicine by Chakaroun, Pradhan, Björnson et al. revealed a previously underappreciated dimension of this process: the gut microbiome and adipose tissue interact through multi-omic pathways to define different metabolic obesity subtypes. This finding has profound implications for precision medicine, suggesting that interventions targeting gut bacteria may someday be tailored to individual metabolic phenotypes.
Endothelial Dysfunction and Atherosclerosis
The endothelium — the thin inner lining of blood vessels — is extraordinarily sensitive to metabolic disruption. Insulin resistance, hyperglycemia, dyslipidemia, and inflammation all impair endothelial function, impairing vasodilation, promoting blood clotting, and accelerating atherosclerotic plaque formation. This is the direct pathway from metabolic dysfunction to heart attack and stroke.
5. Obesity as a Chronic Disease: The Evidence Is Clear
For too long, obesity was dismissed as a lifestyle choice, a matter of willpower, or simply an aesthetic concern. That era is over.
A major 2025 narrative review in Advances in Therapy by Singh, Sun, Cheng et al. traces the evolution of how medicine has come to understand obesity — and the conclusion is unambiguous: obesity is a chronic, relapsing, neurobiologically driven disease with profound cardiometabolic consequences.
This matters clinically because it changes everything — from how we talk to patients about weight, to how aggressively we intervene, to which tools we use.
The Cardiometabolic Burden of Obesity
Obesity does not simply coexist with cardiometabolic disease — it actively drives it through multiple pathways:
Accelerates insulin resistance through excess free fatty acid release from visceral adipose tissue
Raises blood pressure through sympathetic nervous system activation and sodium retention
Promotes dyslipidemia through increased hepatic VLDL production
Drives systemic inflammation through adipokine dysregulation
Impairs kidney function through glomerular hypertension and inflammation
Promotes heart failure through hemodynamic overload and myocardial lipid deposition
A seminal 2025 commentary by Clemmensen et al. in Nature Metabolism emphasizes that obesity represents "a critical intersection of cardiometabolic complications" — making its treatment not a cosmetic intervention, but a disease-modifying medical necessity.
Moving Beyond the Scale: "Metabolic Quality" of Weight Loss
One of the most important recent conceptual shifts is the recognition that not all weight loss is equally beneficial from a cardiometabolic standpoint. Losing predominantly lean mass (muscle) while preserving fat is metabolically counterproductive. The most beneficial weight loss:
Preferentially reduces visceral fat
Preserves or increases lean muscle mass
Reduces systemic inflammation
Improves insulin sensitivity
Improves lipid profiles and blood pressure
This is precisely why modern pharmacological interventions — particularly GLP-1 receptor agonists — are considered superior to simple caloric restriction for cardiometabolic benefit.
6. The Liver's Hidden Role: MASLD, MASH, and the Metabolic Spillover Effect
The CKM framework traditionally focuses on three pillars: heart, kidneys, and metabolic system. But there is a fourth organ deserving urgent attention — the liver.
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) — formerly known as non-alcoholic fatty liver disease (NAFLD) — and its inflammatory form, Metabolic Dysfunction-Associated Steatohepatitis (MASH), are now recognized as integral components of the cardiometabolic disease picture.
The "Toxic Smoke" Effect
A fatty, inflamed liver does not simply store excess fat passively. It becomes a source of lipotoxic inflammation, releasing pro-inflammatory signals and atherogenic lipoproteins into the circulation. This inflammation "spills over" into the bloodstream, directly damaging the endothelium, worsening insulin resistance, and accelerating kidney decline.
Think of the liver as the body's metabolic furnace and filter. When that furnace is clogged with fat, it produces toxic exhaust that affects every organ downstream.
The Bidirectional Relationship
The relationship between liver disease and cardiometabolic disease is bidirectional:
As CKM syndrome stages advance, the risk of liver fibrosis (scarring) more than doubles
Conversely, even modest liver fat accumulation is now a recognized cardiovascular risk enhancer — predictive of future heart attacks even in young individuals who appear otherwise healthy
Therapeutic Implications
This is one reason why medications like semaglutide and tirzepatide — which act on GLP-1 (and GIP/glucagon) receptors — have shown such impressive results. By simultaneously reducing visceral fat, resolving liver inflammation, improving insulin sensitivity, and protecting the heart, they address the CKM and liver disease simultaneously.
7. Breakthrough Medications: GLP-1, SGLT2, and Triple Agonists
The last decade has witnessed a genuine therapeutic revolution in cardiometabolic medicine. What began as glucose-lowering drugs has proven to be multi-system disease-modifying agents with benefits far beyond their original indications.
GLP-1 Receptor Agonists (GLP-1 RAs)
Glucagon-like peptide-1 (GLP-1) is a gut hormone that stimulates insulin secretion, suppresses glucagon, slows gastric emptying, and signals satiety to the brain. GLP-1 receptor agonists (like semaglutide and liraglutide) amplify these effects.
Key benefits beyond blood sugar:
Weight loss: Up to 15–20% body weight reduction with high-dose semaglutide (STEP trials)
Cardiovascular protection: Significant reduction in major cardiovascular events (MACE), including heart attack and stroke (LEADER, SUSTAIN-6, SELECT trials)
Blood pressure reduction: Modest but consistent reductions in systolic BP
Renal protection: Reduced albuminuria and slower GFR decline
Liver fat reduction: Significant reduction in MASLD/MASH severity
Systemic inflammation: Reduction in high-sensitivity CRP and other inflammatory markers
A comprehensive 2025 review by Kim in the CardioMetabolic Syndrome Journal highlights that GLP-1 RAs are now demonstrating extraordinary efficacy "across the entire spectrum of cardiometabolic diseases" — including in patients without diabetes, particularly for cardiovascular event prevention (the SELECT trial showed a 20% reduction in MACE in non-diabetic obese individuals).
SGLT2 Inhibitors (SGLT2i)
Sodium-glucose cotransporter-2 (SGLT2) inhibitors (including empagliflozin, dapagliflozin, and canagliflozin) work by blocking the kidney's reabsorption of glucose, causing excess glucose to be excreted in the urine.
But the true story of SGLT2 inhibitors is not about glucose. Their most clinically significant effects include:
Heart failure prevention and treatment: Dramatically reduce hospitalizations for heart failure — one of the most robust effects in cardiology trials (EMPEROR-Reduced, DAPA-HF)
Chronic kidney disease protection: Slow progression of kidney disease across a wide range of CKD stages (CREDENCE, DAPA-CKD trials) — including in non-diabetic patients
Blood pressure reduction: Modest but meaningful reductions in systolic BP (3–5 mmHg)
Weight loss: Modest weight reduction (2–4 kg), largely fluid-independent
Uric acid reduction: Potential benefit in gout and its cardiorenal associations
The mechanism behind their cardiac and renal benefits is not simply glucose excretion. Current evidence suggests they act by reducing intraglomerular pressure (protecting the kidney's filtration units), reducing cardiac preload and afterload, improving mitochondrial function in heart and kidney cells, and perhaps through ketone body signaling that provides alternative fuel for stressed organs.
Di Fiore et al. (2024) specifically identify SGLT2 transporters as among the most "pivotal therapeutic pathways" in precision cardiometabolic medicine — targets that address root molecular mechanisms rather than downstream symptoms.
Dual and Triple Receptor Agonists: The New Frontier
The most exciting innovation in cardiometabolic medicine is the development of dual and triple receptor agonists — single molecules that simultaneously activate multiple metabolic hormone receptors.
Tirzepatide (GLP-1/GIP dual agonist): Activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. In the SURMOUNT-1 trial, tirzepatide at the highest dose produced an average weight loss of 22.5% of body weight — exceeding the results seen with GLP-1 monotherapy. It also demonstrated superior glycemic control compared to semaglutide in head-to-head trials (SURPASS-2).
Triple agonists (GLP-1/GIP/Glucagon): Emerging agents that add glucagon receptor activation to the GLP-1/GIP dual mechanism. By also activating glucagon receptors (which increase energy expenditure), these agents theoretically produce greater weight loss and metabolic benefit than dual agonists. Early clinical data is extremely promising, though these agents are still in late-stage clinical development.
Clemmensen et al. (2025) describe triple receptor agonists as "the frontier of cardiometabolic therapeutics, offering unprecedented metabolic benefits" — with the potential to redefine what is achievable in obesity and metabolic disease management.
Comparison of Key Cardiometabolic Drug Classes
GLP-1 Receptor Agonists (e.g., Semaglutide)
Primary Mechanism: Mimics the GLP-1 hormone to increase insulin secretion, slow stomach emptying, and lower appetite.
Weight Loss Effectiveness: ★★★★☆ (Very High)
Cardiovascular (CV) Benefit: ★★★★★ (Exceptional)
Renal (Kidney) Benefit: ★★★☆☆ (Moderate)
Heart Failure Benefit: ★★★☆☆ (Moderate)
SGLT2 Inhibitors (e.g., Empagliflozin, Dapagliflozin)
Primary Mechanism: Blocks the kidneys from reabsorbing glucose, causing excess sugar to be excreted through urine.
Weight Loss Effectiveness: ★★☆☆☆ (Modest)
Cardiovascular (CV) Benefit: ★★★★☆ (High)
Renal (Kidney) Benefit: ★★★★★ (Exceptional)
Heart Failure Benefit: ★★★★★ (Exceptional)
Dual GLP-1/GIP Receptor Agonists (e.g., Tirzepatide)
Primary Mechanism: Activates both GLP-1 and GIP metabolic pathways for enhanced blood sugar control and appetite suppression.
Weight Loss Effectiveness: ★★★★★ (Exceptional)
Cardiovascular (CV) Benefit: ★★★★☆ (High)
Renal (Kidney) Benefit: ★★★☆☆ (Moderate)
Heart Failure Benefit: ★★★☆☆ (Moderate)
Triple Agonists (Emerging Therapies)
Primary Mechanism: Simultaneously targets three metabolic pathways (typically GLP-1, GIP, and Glucagon receptors).
Weight Loss Effectiveness: ★★★★★ (Exceptional)
Cardiovascular, Renal, & Heart Failure Benefits: Currently under active clinical study.
Metformin
Primary Mechanism: Activates the AMPK pathway, primarily reducing glucose production in the liver and improving insulin sensitivity.
Weight Loss Effectiveness: ★☆☆☆☆ (Mild)
Cardiovascular (CV) Benefit: ★★★☆☆ (Moderate)
Renal (Kidney) Benefit: ★★☆☆☆ (Mild)
Heart Failure Benefit: ★☆☆☆☆ (Mild)★
Ratings are relative and based on current clinical evidence; individual results vary
8. The Role of Precision Medicine and Biomarkers
The era of "one-size-fits-all" cardiometabolic medicine is ending. The future belongs to precision medicine — matching treatment to the individual's specific metabolic profile, genetic background, and biomarker signature.
Di Fiore et al. (2024) emphasize that advanced biomarker profiling enables clinicians to detect subclinical cardiometabolic disease long before irreversible organ damage occurs. The key is knowing which biomarkers to measure — and what to do with the results.
Essential Cardiometabolic Biomarkers
For metabolic dysfunction:
Fasting insulin + glucose (HOMA-IR): Calculates insulin resistance. A HOMA-IR score >2.5 suggests meaningful insulin resistance
HbA1c: Reflects average blood glucose over 3 months. Pre-diabetes: 5.7–6.4%; Diabetes: ≥6.5%
Fasting triglycerides: Elevated levels (>150 mg/dL) signal hepatic insulin resistance
Fasting glucose: Pre-diabetes threshold: 100–125 mg/dL
For cardiovascular risk:
High-sensitivity CRP (hs-CRP): Marker of systemic inflammation; elevated levels (>2 mg/L) indicate increased cardiovascular risk independent of LDL cholesterol
ApoB: A superior marker of atherogenic particle burden compared to LDL-C alone
Lipoprotein(a) [Lp(a)]: Genetically determined risk factor for cardiovascular disease; should be measured at least once in every adult
Non-HDL cholesterol: Captures all atherogenic lipoprotein fractions
For renal health:
Urine albumin-to-creatinine ratio (UACR): The most sensitive early marker of kidney damage. Even mildly elevated UACR (>10 mg/g) signals risk
eGFR (estimated glomerular filtration rate): Measures kidney filtration capacity
Serum cystatin C: More accurate than creatinine for detecting early GFR decline
The Microbiome: A New Biomarker Frontier
The 2026 Nature Medicine study by Chakaroun et al. introduces a powerful new dimension: the gut microbiome as a determinant of metabolic obesity subtype. Using multi-omic analysis (genomics, metabolomics, and metagenomics), the researchers demonstrated that distinct microbiome signatures in adipose tissue correlate with specific patterns of metabolic dysfunction — opening the door to microbiome-guided treatment selection. While this is not yet clinically actionable in standard practice, it represents the direction precision cardiometabolic medicine is heading.
9. Evidence Summary: Key Clinical Trials and Landmark Studies
GLP-1 & Dual-Agonist Trials (Weight Management & Cardiovascular Health)
SELECT (2023)
Intervention: Semaglutide 2.4 mg
Target Population: Individuals with obesity and a prior cardiovascular (CV) event, but without diabetes.
Key Outcome: Demonstrated a 20% reduction in MACE (Major Adverse Cardiovascular Events), proving that the cardiovascular benefits of semaglutide extend to non-diabetic populations.
SURMOUNT-1 (2022)
Intervention: Tirzepatide 15 mg
Target Population: Individuals with obesity but without diabetes.
Key Outcome: Achieved an extraordinary 22.5% average body weight loss, setting a new benchmark for non-surgical weight management efficacy.
LEADER (2016)
Intervention: Liraglutide
Target Population: Individuals with Type 2 Diabetes (T2DM) and high cardiovascular risk.
Key Outcome: Showed a 13% reduction in MACE, establishing early evidence for the cardioprotective benefits of GLP-1 receptor agonists.
SGLT2 Inhibitor Trials (Kidney Health & Heart Failure)
DAPA-CKD (2020)
Intervention: Dapagliflozin
Target Population: Individuals with Chronic Kidney Disease (CKD), both with and without diabetes.
Key Outcome: Resulted in a 39% reduction in kidney disease progression or death, securing its role as a foundational renal therapy.
EMPEROR-Reduced (2020)
Intervention: Empagliflozin
Target Population: Patients with Heart Failure with reduced ejection fraction (HFrEF), with or without diabetes.
Key Outcome: Demonstrated a 25% reduction in CV death or heart failure hospitalization.
CREDENCE (2019)
Intervention: Canagliflozin
Target Population: Patients with both Chronic Kidney Disease (CKD) and Type 2 Diabetes (T2DM).
Key Outcome: Achieved a 30% reduction in the primary renal composite endpoint, confirming potent kidney-protective properties.
Recent 2025–2026 Research (Mechanisms & Disease Frameworks
Lin & Tandar (2026)
Study Type: Global multi-ethnic observational study.
Key Outcome: Confirmed that visceral adiposity (deep belly fat) serves as a significantly more accurate predictor of cardiometabolic risk than standard Body Mass Index (BMI).
Chakaroun et al. (2026)
Study Type: Multi-omic analysis of adults with obesity.
Key Outcome: Revealed that specific microbiome–adipose tissue interactions define unique metabolic subtypes, paving the way for personalized obesity treatments.
Singh et al. (2025)
Study Type: Broad narrative review.
Key Outcome: Delivered an updated clinical framework firmly defining obesity as a primary, chronic cardiometabolic disease rather than just a lifestyle factor.
10. Practical Strategies for Cardiometabolic Health
Science is only as useful as your ability to apply it. Here are evidence-based strategies for reducing cardiometabolic risk — organized by the level of effort and impact.
Tier 1: Foundational Lifestyle Strategies (Start Here)
1. Reduce visceral fat through targeted nutrition:
Follow a Mediterranean or DASH dietary pattern: high in vegetables, legumes, whole grains, olive oil, nuts, and fish; low in ultra-processed foods and refined carbohydrates
Minimize added sugars and sweetened beverages — the primary dietary drivers of hepatic fat accumulation and insulin resistance
Practice time-restricted eating (12:10 or 16:8): evidence supports reductions in visceral fat and insulin resistance independent of caloric intake
2. Exercise as cardiometabolic medicine:
A combination of aerobic exercise + resistance training is superior to either modality alone for cardiometabolic health:
Aerobic (150+ minutes/week moderate intensity): Reduces visceral fat, improves insulin sensitivity, lowers blood pressure
Resistance training (2–3 sessions/week): Increases muscle mass (improves glucose disposal), reduces insulin resistance independently of weight loss
VILPA (Vigorous Intermittent Lifestyle Physical Activity): Even brief bouts of incidental vigorous activity (stair climbing, carrying groceries briskly) of just 3–4 minutes per day can significantly reduce cardiometabolic mortality
3. Prioritize sleep quality:
Poor sleep (especially <6 or >9 hours per night, or disordered sleep from sleep apnea) is an independent driver of insulin resistance, cortisol elevation, and cardiometabolic risk. Address sleep apnea aggressively — it is far more than a nuisance.
4. Manage chronic stress:
Chronic psychological stress elevates cortisol and adrenaline, promotes visceral fat accumulation, raises blood pressure, and worsens insulin sensitivity. Evidence-based stress reduction strategies include mindfulness-based stress reduction (MBSR), regular nature exposure, and social connection.
Tier 2: Medical Monitoring (Know Your Numbers)
Here is a practical Cardiometabolic Health Screening Checklist — minimum frequency for adults with any metabolic risk factors:
High-Frequency Monitoring (Every Visit to 6 Months)
Blood Pressure
Frequency: Checked at every clinical visit.
Clinical Target: Less than 130/80 mmHg
Waist Circumference
Frequency: Every 3 to 6 months.
Clinical Target:
Men: Less than 90 cm
Women: Less than 80 cm
Standard Annual Screenings (Every 12 Months)
Fasting Glucose & HbA1c
Frequency: Annually.
Clinical Target:
Fasting Glucose: Less than 100 mg/dL
HbA1c: Less than 5.7%
Lipid Panel (with ApoB)
Frequency: Annually.
Clinical Target: LDL less than 100 mg/dL or lower if the individual has an elevated cardiovascular risk profile.
hs-CRP (High-Sensitivity C-Reactive Protein)
Frequency: Annually if the patient has an elevated metabolic or cardiovascular risk profile.
Clinical Target: Less than 1 mg/L is considered optimal.
Liver Enzymes (ALT, AST)
Frequency: Annually if the patient is classified as overweight or obese.
Clinical Target: To remain strictly within standard normal reference ranges.
Targeted Annual Screenings (For High-Risk Groups)
Note: The following tests should be run at least once a year for patients with existing diagnoses of Diabetes or Hypertension.
UACR (Urine Albumin-to-Creatinine Ratio)
Frequency: Annually for diabetic or hypertensive patients.
Clinical Target: Less than 30 mg/g
eGFR (Estimated Glomerular Filtration Rate)
Frequency: Annually for diabetic or hypertensive patients.
Clinical Target: Greater than 60 mL/min/1.73m² .
Tier 3: Pharmacological Intervention (When Lifestyle Is Not Enough)
For many patients, lifestyle modification alone — while essential — is insufficient to fully address cardiometabolic risk. This is not a failure; it reflects the neurobiological complexity of metabolic disease.
When to consider medication:
HbA1c ≥6.5% (type 2 diabetes diagnosis)
Persistent visceral obesity with metabolic syndrome despite lifestyle efforts
Established cardiovascular disease or high cardiovascular risk
Evidence of kidney damage (elevated UACR or reduced eGFR)
Heart failure diagnosis
Medication selection should be individualized based on dominant risk factors, organ function, drug interactions, and patient preferences — always in partnership with a qualified healthcare provider.
Important: The decision to start, change, or stop any cardiometabolic medication should always be made in consultation with your physician or specialist. Drug choices should be personalized based on your complete medical history, kidney function, and cardiovascular risk profile.
11. Common Myths and Mistakes About Cardiometabolic Disease
Myth 1: "I'm not overweight, so I don't have cardiometabolic risk."
Wrong. Visceral fat can accumulate in individuals with a normal BMI — a condition called Metabolically Obese Normal Weight (MONW) or "TOFI" (Thin Outside, Fat Inside). Research published in 2026 by Lin and Tandar confirms that visceral adiposity, not total weight, is the more accurate predictor of cardiometabolic risk. Waist circumference and UACR are more informative than BMI alone.
Myth 2: "GLP-1 drugs are just for diabetics."
Outdated. The SELECT trial demonstrated significant cardiovascular benefit from semaglutide in obese individuals without diabetes. Multiple GLP-1 receptor agonists are now approved for weight management (not just diabetes) in many countries, and their indications are expanding rapidly.
Myth 3: "Once I lose the weight, I can stop the medication."
Often incorrect. Obesity is a chronic, relapsing disease. Discontinuing GLP-1 RAs after weight loss typically results in significant weight regain within 12 months (STEP 4 extension trial). For many patients, long-term treatment — like antihypertensives or statins — is the appropriate paradigm.
Myth 4: "Cardiometabolic disease only matters when I get older."
Dangerous misconception. Metabolic memory is real. Studies consistently show that metabolic damage accumulates silently across decades — and that early, effective intervention in the 30s and 40s delivers protective effects that persist into the 70s and 80s. The "legacy effect" of good metabolic control is one of the strongest arguments for early screening and intervention.
Myth 5: "High blood sugar is the main problem to fix."
Incomplete. Blood glucose is one variable in a multi-dimensional cardiometabolic equation. Many patients with well-controlled blood sugar still progress to cardiovascular disease because their blood pressure, visceral fat, inflammation, or kidney function was not adequately addressed. Modern treatment must target the whole picture — not just HbA1c.
Myth 6: "Statins alone protect my heart if I have diabetes."
Partially true, but insufficient. Statins reduce LDL cholesterol and cardiovascular risk, but do not address insulin resistance, kidney damage, or heart failure risk. In patients with type 2 diabetes and established cardiovascular disease, adding a GLP-1 RA and/or SGLT2 inhibitor on top of optimal statin therapy produces additive, often dramatic, reductions in cardiovascular events.
12. Frequently Asked Questions
Q1: What is the difference between cardiometabolic disease and metabolic syndrome?
Metabolic syndrome is a diagnostic cluster of five risk factors (central obesity, high blood pressure, high fasting glucose, high triglycerides, low HDL). Cardiometabolic disease is a broader term encompassing metabolic syndrome, type 2 diabetes, cardiovascular disease, and chronic kidney disease — all understood as manifestations of the same underlying metabolic dysfunction. You can think of metabolic syndrome as an early warning stage within the cardiometabolic disease spectrum.
Q2: Can GLP-1 receptor agonists help even if I don't have diabetes?
Yes. Clinical trials — including the SELECT trial using semaglutide in non-diabetic obese individuals — have demonstrated significant cardiovascular and weight-related benefits in people without diabetes. Several GLP-1 RAs are now specifically approved for chronic weight management in non-diabetic individuals. Discuss eligibility with your physician.
Q3: Are SGLT2 inhibitors safe for people with kidney disease?
In many cases, yes — and they are now among the most important kidney-protective agents we have. The DAPA-CKD trial showed dapagliflozin reduced kidney disease progression by 39% in patients with chronic kidney disease (with or without diabetes). However, SGLT2 inhibitors should not be used when eGFR is very low (typically below 20 mL/min/1.73m²). Always work with your nephrologist or physician to determine appropriateness.
Q4: How do I know if I have insulin resistance before I develop diabetes?
The earliest clinical signs of insulin resistance include abdominal weight gain, fatigue after meals, sugar cravings, difficulty losing weight despite effort, elevated fasting triglycerides, low HDL cholesterol, and mild elevation of fasting glucose (>90 mg/dL is concerning even below the prediabetes threshold of 100 mg/dL). The HOMA-IR score — calculated from fasting insulin and glucose — is a practical clinical tool. Ask your doctor to include fasting insulin in your next blood panel.
Q5: What lifestyle change has the biggest single impact on cardiometabolic risk?
The evidence points to reducing visceral fat as the highest-yield target. The most effective strategies for doing so are: eliminating sugar-sweetened beverages and ultra-processed carbohydrates, incorporating regular resistance training, improving sleep quality, and — when necessary — adding a GLP-1 RA or SGLT2 inhibitor. No single lifestyle change trumps addressing the central adiposity driving systemic insulin resistance and inflammation.
Q6: Is the gut microbiome really relevant to my cardiometabolic health?
Increasingly, yes. Research published in 2026 in Nature Medicine demonstrates that adipose tissue–microbiome interactions shape distinct metabolic obesity subtypes. While microbiome-guided prescribing is not yet standard practice, consuming a high-fiber, diverse plant-based diet is one of the most effective ways to support a healthy microbiome — and this independently reduces cardiometabolic risk.
Q7: How quickly do cardiometabolic medications produce measurable benefits?
It depends on the benefit in question. Appetite suppression and early weight loss with GLP-1 RAs can begin within weeks. Blood pressure improvements with SGLT2 inhibitors often appear within days to weeks. However, the most important benefits — reduction in cardiovascular events, kidney disease progression, and long-term mortality — emerge over months to years of consistent treatment. Patience and persistence are essential.
Q8: Can children and adolescents develop cardiometabolic disease?
Sadly, yes. Pediatric obesity, insulin resistance, and even type 2 diabetes are increasing globally. Metabolic syndrome is now diagnosed in adolescents. The importance of addressing diet quality, physical activity, and screen time in childhood cannot be overstated — cardiometabolic damage can begin in the second decade of life and accumulate silently across decades.
Q9: What is the "legacy effect" and why does it matter?
The legacy effect (also called "metabolic memory") refers to the long-lasting protective benefits of early, effective cardiometabolic management — even if control becomes less optimal later. Landmark diabetes trials (UKPDS, ACCORD) demonstrated that patients who achieved tight glucose control early in their diagnosis had significantly fewer cardiovascular events decades later, even after the period of tight control ended. Think of it as compound interest for your health: early investment pays dividends for life.
Q10: Do cardiometabolic drugs ever interact dangerously with each other?
Drug interactions exist and require careful management. For example, SGLT2 inhibitors increase the risk of urinary tract infections and (rarely) diabetic ketoacidosis. GLP-1 RAs can cause nausea, vomiting, and rarely pancreatitis. Combining multiple antihypertensive agents with SGLT2 inhibitors can occasionally cause hypotension. All medication decisions — including combinations — must be made in close partnership with a physician who knows your complete medication list, kidney function, and clinical history.
Q11: Are there racial or ethnic differences in cardiometabolic risk?
Yes, significant ones. South Asians develop insulin resistance, type 2 diabetes, and cardiovascular disease at lower body weights and younger ages compared to European populations — a well-documented phenomenon that demands lower waist circumference thresholds and earlier screening. African populations have higher rates of hypertension-driven CKM syndrome. Hispanic and Latino populations face high rates of MASLD/MASH. Precision cardiometabolic care requires recognition of these important differences.
Q12: What is the most important single thing I can do to protect my cardiometabolic health starting today?
Know your numbers. Get a fasting blood glucose, HbA1c, lipid panel with ApoB, hs-CRP, UACR, eGFR, and a waist circumference measurement. Cardiometabolic disease is largely silent until it is advanced — and what you do not know, you cannot treat. The "check engine light" of your cardiometabolic health comes from your lab results, not your symptoms.
13. Conclusion and Action Steps
Cardiometabolic disease is no longer a collection of separate conditions — it is a unified, progressive, and preventable syndrome that demands an equally unified response. The science is clear: insulin resistance, visceral adiposity, inflammation, and mitochondrial dysfunction are the shared upstream drivers. And the therapeutic tools available today — GLP-1 receptor agonists, SGLT2 inhibitors, and the emerging triple agonists — offer genuinely unprecedented opportunities to halt and even reverse this process.
But the most powerful medicine of all remains early action.
Your 5-Step Cardiometabolic Health Action Plan:
Measure what matters. Schedule a comprehensive cardiometabolic blood panel that includes fasting insulin, HbA1c, ApoB, hs-CRP, UACR, and eGFR. Measure your waist circumference today.
Address visceral fat first. Reduce sugar and ultra-processed carbohydrates, incorporate resistance training, and prioritize 7–9 hours of quality sleep. These changes directly target the central driver of cardiometabolic disease.
Understand your risk stage. Ask your physician to evaluate you through the CKM syndrome framework — not just for blood sugar or blood pressure in isolation, but as an integrated cardiometabolic profile.
Have an honest conversation about medication. If lifestyle changes alone are insufficient — and for many people, they will be — evidence-based pharmacological support is not a failure. It is appropriate, effective, and potentially life-saving.
Commit to the long game. Cardiometabolic health is not a sprint. The most important decisions you make in your 40s and 50s will determine your quality of life in your 70s and 80s. The legacy effect is real — start building it now.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Obesity and Fatty Liver Disease: What Science Says About Risk and Health | DR T S DIDWAL
Intermittent Fasting: Metabolic Health Benefits and the Evidence on Longevity | DR T S DIDWAL
Activate Your Brown Fat: A New Pathway to Longevity and Metabolic Health | DR T S DIDWAL
Leptin vs. Adiponectin: How Your Fat Hormones Control Weight and Metabolic Health | DR T S DIDWAL
Lower Blood Pressure Naturally: Evidence-Based Exercise Guide for Metabolic Syndrome | DR T S DIDWAL
Movement Snacks: How VILPA Delivers Max Health Benefits in Minutes | DR T S DIDWAL
The BMI Paradox: Why "Normal Weight" People Still Get High Blood Pressure | DR T S DIDWAL
How Insulin Resistance Accelerates Cardiovascular Aging | DR T S DIDWAL
References
Chakaroun, R.M., Pradhan, M., Björnson, E., et al. (2026). Multi-omic definition of metabolic obesity through adipose tissue–microbiome interactions. Nature Medicine, 32, 113–125. https://doi.org/10.1038/s41591-025-04009-7
Clemmensen, C., Gerhart-Hines, Z., Schwartz, T.W., Zierath, J.R., & Sakamoto, K. (2025). Shaping the future of cardiometabolic innovation: Advances and opportunities. Nature Metabolism, 7(8), 1495–1497. https://doi.org/10.1038/s42255-025-01343-5
Di Fiore, V., Cappelli, F., Del Punta, L., et al. (2024). Novel techniques, biomarkers and molecular targets to address cardiometabolic diseases. Journal of Clinical Medicine, 13(10), 2883. https://doi.org/10.3390/jcm13102883
Fernando, K., Connolly, D., Darcy, E., et al. (2025). Advancing cardiovascular, kidney, and metabolic medicine: A narrative review of insights and innovations for the future. Diabetes Therapy, 16(5), 1155–1176. https://doi.org/10.1007/s13300-025-01738-3
Kim, H.-J. (2025). Expanding the role of novel therapeutics in cardiometabolic syndrome: Beyond heart failure and diabetes. CardioMetabolic Syndrome Journal, 5(1), 9–22. https://doi.org/10.51789/cmsj.2025.5.e4
Lin, J.C., & Tandar, C.E. (2026). Global patterns of visceral adiposity and cardiometabolic disease. Nature Reviews Endocrinology, 22, 8. https://doi.org/10.1038/s41574-025-01191-z
Pohlman, N., Patel, P.N., Essien, U.R., Tang, J.J., & Joseph, J.J. (2025). Novel cardiometabolic medications in the cardiovascular-kidney-metabolic syndrome era. The Journal of Clinical Endocrinology and Metabolism, 110(8), 2105–2122. https://doi.org/10.1210/clinem/dgaf295
Singh, V., Sun, J., Cheng, S., et al. (2025). Obesity as a chronic disease: A narrative review of evolving definitions, management strategies, and cardiometabolic prioritization. Advances in Therapy, 42, 5341–5364. https://doi.org/10.1007/s12325-025-03352-y
Lincoff, A.M., Brown-Frandsen, K., Colhoun, H.M., et al. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes (SELECT). New England Journal of Medicine, 389, 2221–2232.
Jastreboff, A.M., Aronne, L.J., Ahmad, N.N., et al. (2022). Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). New England Journal of Medicine, 387, 205–216.
Heerspink, H.J.L., Stefánsson, B.V., Correa-Rotter, R., et al. (2020). Dapagliflozin in patients with chronic kidney disease (DAPA-CKD). New England Journal of Medicine, 383, 1436–1446.
Packer, M., Anker, S.D., Butler, J., et al. (2020). Cardiovascular and renal outcomes with empagliflozin in heart failure (EMPEROR-Reduced). New England Journal of Medicine, 383, 1413–1424.
Marso, S.P., Daniels, G.H., Brown-Frandsen, K., et al. (2016). Liraglutide and cardiovascular outcomes in type 2 diabetes (LEADER). New England Journal of Medicine, 375, 311–322.
Kahn, S.E., Lachin, J.M., Zinman, B., et al. (UKPDS legacy effect analysis). Long-term follow-up of intensive glucose control in type 2 diabetes. New England Journal of Medicine.
Grundy, S.M., Cleeman, J.I., Daniels, S.R., et al. (2005). Diagnosis and management of the metabolic syndrome: An AHA/NHLBI Scientific Statement. Circulation, 112, 2735–2752.
Mechanick, J.I., Farkouh, M.E., Newman, J.D., & Garvey, W.T. (2019). Cardiometabolic-based chronic disease, adiposity and dysglycemia drivers: JACC State-of-the-Art Review. Journal of the American College of Cardiology, 75(5), 525–538.
Sattar, N., & Gill, J.M. (2014). Type 2 diabetes as a disease of ectopic fat? BMC Medicine, 12, 123.
Després, J.-P., & Lemieux, I. (2006). Abdominal obesity and metabolic syndrome. Nature, 444, 881–887.
Written by Dr. T.S. Didwal, M.D. (Internal Medicine) | Last Updated: 2026
This article synthesizes peer-reviewed research published between 2019 and 2026. It is intended for educational purposes and does not constitute individualized medical advice. Treatment decisions should always be made in consultation with a qualified healthcare professional who is familiar with your complete medical history.