GLP-1 Receptor Agonists and Cardiovascular Protection: Evidence from CVOT Trials Explained
Learn how GLP-1 receptor agonists improve cardiovascular health by reducing inflammation, atherosclerosis, heart attack, and stroke risk in diabetes and obesity.
DIABETESHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/2/202624 min read
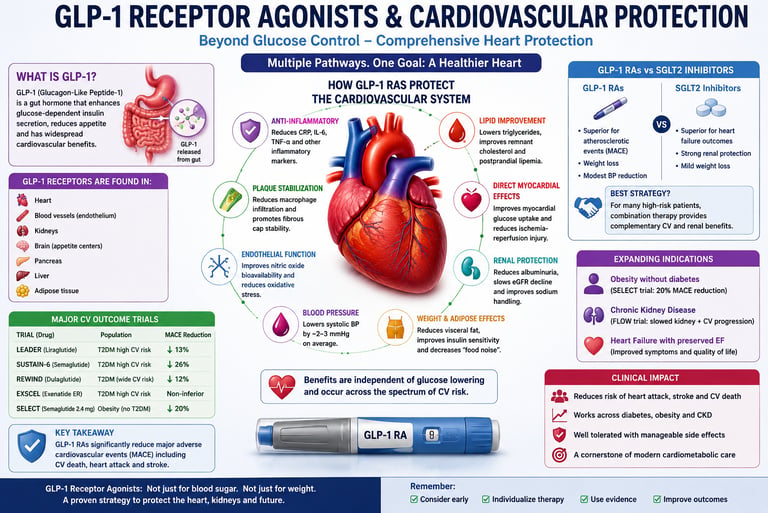
GLP-1 receptor agonists protect the heart by reducing atherosclerosis, inflammation, and visceral fat while improving blood vessel function. Clinical trials show these medications can lower major adverse cardiovascular events (MACE) by 12–26%, making them important therapies for diabetes, obesity, and cardiovascular disease.
Key Takeaways: GLP-1 RAs & Heart Protection
They’re heart drugs, not just diabetes or weight drugs. GLP-1 RAs like semaglutide and liraglutide cut heart attack, stroke, and CV death by 12–26% in landmark trials.
Benefit happens even without diabetes. SELECT proved that semaglutide 2.4 mg reduces major heart events by 20% in people with obesity but normal blood sugar.
It’s not just about weight or A1c. Heart protection comes from anti-inflammatory, plaque-stabilising, and blood vessel effects that work independently of glucose or pounds lost.
Not all GLP-1s are equal. Semaglutide, liraglutide, and dulaglutide have proven CV superiority. Exenatide ER showed safety but not superiority. Agent choice matters.
They pair with SGLT2 inhibitors. GLP-1s are the “vascular shield” for atherosclerosis; SGLT2s are the “fluid & filter guard” for heart failure and kidneys. Using both is the standard of care for high-risk patients.
Primary prevention is real. REWIND included patients without prior heart disease and still showed benefit. You don’t need to wait for a heart attack to qualify.
Side effects are manageable. Nausea is common early but usually fades with slow titration. Start low, go slow.
Ask if you qualify. Consider a GLP-1 RA if you have: type 2 diabetes + CV disease/risk, OR obesity + established heart disease. Don’t stop therapy without talking to your clinician.
For years, GLP-1 receptor agonists were seen as “sugar drugs” or “weight-loss shots.” The science in 2025–2026 has changed that story. Today, agents like semaglutide and liraglutide are proven heart protectors — and that benefit shows up even if your blood sugar is normal.
Big trials told us why. LEADER showed liraglutide cut major heart events by 13% in people with type 2 diabetes, driven largely by fewer cardiovascular deaths (Marso et al., 2016). SUSTAIN-6 found weekly semaglutide lowered heart attack, stroke, and CV death by 26%, with stroke dropping 39% (Marso et al., 2016). REWIND proved that dulaglutide helps even if you haven’t had a heart attack yet — a 12% risk cut in primary prevention (Gerstein et al., 2019).
Then came the game-changer: SELECT. In 17,604 people with obesity but no diabetes, semaglutide 2.4 mg reduced heart events by 20% (Lincoff et al., 2023). That means the heart benefit isn’t just from lowering glucose or pounds on the scale.
How? GLP-1s calm inflammation, stabilize artery plaques, improve blood vessel function, lower blood pressure 2–3 mmHg, and trim dangerous visceral fat (Westermeier & Fisman, 2025). A 2025 meta-analysis of 99,599 patients confirmed these drugs cut heart attack and stroke consistently, regardless of starting A1c (Galli et al., 2025).
What this means for you: If you have type 2 diabetes with heart disease, or obesity with prior heart problems, ask your clinician about a GLP-1 RA with proven heart benefit. They pair well with SGLT2 inhibitors — one shields the arteries, the other protects the heart and kidneys (Yang, 2025).
Side effects like nausea are common at first but usually fade with slow dose increases. Not all GLP-1s are equal — exenatide ER didn’t show superiority (Holman et al., 2017). So agent choice matters.
We’re no longer just treating numbers. We’re treating risk. And for many, a once-weekly GLP-1 is now frontline heart medicine.
1. What Are GLP-1 Receptor Agonists?
Glucagon-like peptide-1 (GLP-1) is a hormone released by cells in the gut lining after you eat. Its main job is to signal the pancreas to release insulin — but only when blood sugar is actually elevated, making it inherently safer than older insulin-stimulating drugs. In the body, this hormone is destroyed within 1–2 minutes by the enzyme DPP-4.
GLP-1 receptor agonists are engineered versions of this hormone, redesigned to survive much longer in the bloodstream. The result: sustained stimulation of GLP-1 receptors across multiple organs, not just the pancreas.
Where GLP-1 receptors are found
This is where things get interesting. GLP-1 receptors are expressed throughout the body:
Pancreas — stimulates insulin, suppresses glucagon
Brain (hypothalamus & hindbrain) — reduces appetite and "food noise"
Heart — direct cardioprotective signalling
Blood vessels — improve endothelial function
Kidneys — modulate sodium handling, reduces proteinuria
Liver — reduces hepatic fat accumulation
This widespread receptor distribution is why GLP-1 RAs produce effects that ripple across entire organ systems — a property that distinguishes them from every other class of glucose-lowering medication.
Short-acting vs. long-acting agents: does it matter for the heart?
Not all GLP-1 RAs carry equal cardiovascular evidence. Agents differ in duration, receptor engagement, and trial outcomes:
Here is a breakdown of the cardiovascular outcome trials for each GLP-1 receptor agonist, highlighting their dosing schedules and impacts on Major Adverse Cardiovascular Events (MACE):
Semaglutide (injectable, weekly): In the SUSTAIN-6 trial, it demonstrated a significant 26% reduction in MACE.
Semaglutide 2.4 mg (weekly): In the SELECT trial—notably conducted in patients without type 2 diabetes—it achieved a 20% reduction in MACE.
Oral Semaglutide (daily): The SOUL trial confirmed that the oral formulation delivers a 14% reduction in MACE.
Liraglutide (daily): In the LEADER trial, it showed a 13% reduction in MACE.
Dulaglutide (weekly): In the REWIND trial, it demonstrated a 12% reduction in MACE.
Exenatide ER (weekly): In the EXSCEL trial, it achieved non-inferiority, meaning it was proven safe and did not increase cardiovascular risk compared to the control group, though it did not show a statistically significant reduction.⚠ Important: Cardiovascular benefits are NOT a uniform class effect
The degree of heart protection varies significantly between agents. Semaglutide and liraglutide have the strongest evidence. Exenatide twice-daily has not demonstrated superiority. Always consider individual trial data, not just the drug class, when prescribing.
2. How GLP-1 Receptor Agonists Protect the Heart
The cardiovascular benefits of GLP-1 RAs cannot be explained by glucose lowering alone. A landmark 2025 meta-analysis of 99,599 patients in the Journal of the American College of Cardiology (Galli et al.) confirmed that multiple parallel pathways operate simultaneously. Here is what the science shows:
Anti-inflammatory action
Reduces CRP, IL-6, and TNF-α — the chronic inflammatory signals that accelerate plaque formation and damage arterial walls.
Plaque stabilisation
Decreases macrophage infiltration into atherosclerotic plaques and promotes fibrous cap integrity, reducing the risk of rupture-triggered heart attack.
Endothelial restoration
Increases nitric oxide bioavailability and reduces oxidative stress, restoring the flexibility and health of arterial linings.
Visceral fat reduction
Preferentially targets metabolically active visceral adipose tissue, reducing pro-inflammatory adipokines and insulin resistance.
Blood pressure reduction
Delivers a mild but consistent 2–3 mmHg reduction in systolic blood pressure through renal sodium handling and vasodilation.
Lipid profile improvement
Significant triglyceride reduction, improved remnant cholesterol, and reduced postprandial lipemia — lowering "hidden" cardiovascular risk.
Direct myocardial effects
Improves myocardial glucose uptake and reduces ischaemia-reperfusion injury — a cardioprotective role independent of metabolic effects.
Appetite & weight regulation
Acts on hypothalamic GLP-1 receptors to reduce food intake, "food noise," and caloric consumption — driving meaningful, sustained weight loss.
"We are no longer treating glucose — we are treating risk. GLP-1 receptor agonists represent a therapeutic inflection point."
Why weight loss alone doesn't explain it
A common assumption is that cardiovascular benefits come purely from the weight patients lose on these drugs. The evidence says otherwise. In LEADER and SUSTAIN-6, patients lost a modest 2–4 kg of body weight on average — yet showed robust MACE reductions. The anti-inflammatory, anti-atherosclerotic, and endothelial mechanisms operate independently of the scale.
Key Insight
Westermeier & Fisman (2025) in Cardiovascular Diabetology document that cardiovascular protection from GLP-1 RAs is mechanistically multi-layered, and that individual agents differ in their receptor pharmacokinetics — which may explain differences in trial outcomes between agents.
3. CVOT Trials: The Evidence That Changed Clinical Practice
Since 2008, the FDA has required all new diabetes drugs to prove cardiovascular safety through large, dedicated cardiovascular outcome trials (CVOTs). GLP-1 RAs didn't just prove safety — several agents demonstrated a significant reduction in cardiovascular events.
LEADER Trial — Liraglutide
Published in the New England Journal of Medicine, LEADER enrolled 9,340 patients with type 2 diabetes and high cardiovascular risk. Liraglutide produced a statistically significant 13% reduction in MACE (composite of cardiovascular death, non-fatal MI, and non-fatal stroke), with a particularly notable reduction in cardiovascular mortality. This was the first GLP-1 RA trial to show superiority over placebo for cardiovascular outcomes.
SUSTAIN-6 — Semaglutide (injectable)
SUSTAIN-6 enrolled 3,297 patients and demonstrated a striking 26% reduction in MACE with weekly injectable semaglutide, driven primarily by a 39% reduction in non-fatal stroke and a 26% reduction in non-fatal MI. The effect size was larger than in LEADER, though the trial was shorter and designed as a safety trial rather than an event-driven superiority study.
REWIND — Dulaglutide
REWIND is arguably the most clinically important trial for broadening prescribing. It enrolled 9,901 patients, a large proportion of whom (~31%) had no prior cardiovascular disease — making it relevant for primary prevention. Dulaglutide demonstrated a 12% MACE reduction across this mixed-risk population, suggesting that cardiovascular protection is not restricted to patients with established heart disease.
Clinical Pearl: Why REWIND changes everything
Most CVOTs only enroll patients with established cardiovascular disease (secondary prevention). REWIND's inclusion of lower-risk patients — many with only cardiovascular risk factors — opens the door for GLP-1 RAs in primary prevention. This is a significant expansion of potential benefit.
EXSCEL — Exenatide extended-release
EXSCEL enrolled 14,752 patients and showed cardiovascular non-inferiority (i.e., safety) but failed to demonstrate superiority over placebo. This result is important: it confirms that cardiovascular benefits are not a uniform class effect and reinforces the need to use agents with proven superiority when heart protection is the goal.
SELECT — Semaglutide 2.4 mg in obesity without diabetes
Published in 2023–2024, SELECT is a landmark trial that enrolled 17,604 patients with obesity but no diabetes. Weekly semaglutide 2.4 mg (Wegovy) reduced MACE by 20% compared to placebo. This trial repositions GLP-1 RAs as primary cardiometabolic agents — not merely antidiabetic drugs. It establishes cardiovascular benefit independent of any glucose-lowering effect.
Here is a breakdown of the key data and distinct clinical takeaways from each cardiovascular outcome trial, organized by trial:
SUSTAIN-6 (Semaglutide SC): Enrolled 3,297 patients with type 2 diabetes and high cardiovascular risk. It achieved the highest overall MACE reduction at 26%, driven heavily by a notable 39% reduction in stroke.
SELECT (Semaglutide 2.4 mg): The largest trial in the group with 17,604 participants. It evaluated individuals with obesity but no diabetes, achieving a 20% reduction in MACE and proving that these cardiovascular benefits occur independently of blood glucose lowering.
LEADER (Liraglutide): Enrolled 9,340 patients with type 2 diabetes and high cardiovascular risk. It demonstrated a 13% reduction in MACE and a powerful 22% reduction in cardiovascular mortality.
REWIND (Dulaglutide): Studied 9,901 patients with type 2 diabetes. Unlike most other trials, it featured a mixed-risk population that included primary prevention (patients with risk factors but no established cardiovascular disease), achieving a 12% reduction in MACE.
EXSCEL (Exenatide ER): A massive trial of 14,752 patients with type 2 diabetes and a mixed cardiovascular risk profile. It met its safety endpoint for non-inferiority, meaning it is safe to use, though it did not show a statistically significant superiority over the control group.
4. What Meta-Analyses Confirm: The Bigger Picture
Individual trials are powerful, but meta-analyses — pooling data across thousands of patients and multiple drugs — offer a higher level of certainty. The evidence here is consistent and compelling.
Galli et al., 2025 — JACC (99,599 patients)
This systematic review and meta-analysis, published in the Journal of the American College of Cardiology, is one of the largest analyses of GLP-1 RA cardiovascular data to date. Across 99,599 patients, GLP-1 RAs significantly reduced MACE, with the benefit primarily driven by reductions in non-fatal MI and stroke. Effects on cardiovascular mortality were also observed. Importantly, the benefit was consistent regardless of baseline HbA1c levels, reinforcing the independence from glucose lowering.
Kong et al., 2026 — Nature Communications (Umbrella Review)
An umbrella review published in Nature Communications synthesised evidence across multiple systematic reviews and meta-analyses, confirming class-wide MACE reduction for GLP-1 RAs. The review highlighted that the benefit extended across multiple diseases beyond diabetes, including heart failure and chronic kidney disease, though effects were more modest in these areas compared to SGLT2 inhibitors.
Peter, Roka, Sepp et al., 2026 — Long-term safety meta-analysis
A 2026 meta-analysis in Cardiovascular Diabetology – Endocrinology Reports specifically examined long-term cardiovascular safety and efficacy in high-risk populations. Findings supported the durability of MACE benefits over extended follow-up, with an acceptable safety profile when standard contraindications are observed.
Bottom line from the data
Across multiple meta-analyses and umbrella reviews, GLP-1 RAs consistently reduce atherosclerotic events (MI and stroke) by approximately 12–26% depending on agent and population. Their effect on heart failure hospitalisation is more modest compared to SGLT2 inhibitors — a distinction that matters clinically.
5. GLP-1 RAs vs. SGLT2 Inhibitors: Complementary, Not Competing
Patients and clinicians often ask which drug class is "better." The honest answer is: they protect the cardiovascular system through entirely different mechanisms — and that complementarity makes the combination more powerful than either agent alone.
GLP-1 Receptor Agonists
The "Vascular Shield"
Primary benefit: atherosclerotic heart disease (ASCVD)
Reduces MI and stroke (MACE)
Anti-inflammatory, plaque-stabilising
Weight loss: 5–15%+ of body weight
Modest blood pressure reduction (2–3 mmHg)
Emerging renal (proteinuria) benefit
Significant benefit in obesity without diabetes (SELECT)
SGLT2 Inhibitors
The "Fluid & Filter Guard"
Primary benefit: heart failure and chronic kidney disease
Reduces HF hospitalisations dramatically
Natriuretic — reduces preload/afterload
Weight loss: 2–3% of body weight
Significant blood pressure reduction
Gold standard for slowing CKD progression
Benefits extend to HFpEF and HFrEF
Why combination therapy is now the standard of care
For patients with both atherosclerotic cardiovascular disease and kidney disease or heart failure, current 2025–2026 guidelines strongly recommend combining GLP-1 RAs with SGLT2 inhibitors. Think of it as protecting both the "pipes" (arteries) and the "pump and filters" (heart and kidneys) simultaneously.
Yang et al. (2025) in the Journal of Clinical Medicine describe this dual-pathway approach as the most comprehensive cardiometabolic defence strategy currently available, recommending the combination as foundational therapy in high-risk patients regardless of starting HbA1c.
🔑 For clinicians
Do not frame this as a choice. When a patient has established ASCVD plus CKD or heart failure, initiating both a GLP-1 RA and an SGLT2 inhibitor (alongside a statin) represents best evidence-based practice. Nauck (2025) in The Lancet provides a framework for this combination as next-generation incretin-based therapy.
6. Expanding Indications: GLP-1 RAs Beyond Diabetes
One of the most exciting developments in modern medicine is that GLP-1 RAs benefit patients regardless of their blood sugar status. Rosen and Ingelfinger (2026) in the New England Journal of Medicine summarise the expanding therapeutic frontier:
Obesity without diabetes
The SELECT trial definitively established that semaglutide 2.4 mg reduces cardiovascular events in patients who are obese but have normal glucose metabolism. A 20% MACE reduction in non-diabetic patients reshapes how we classify this drug — it is now a cardioprotective agent in its own right, not just an antidiabetic medication repurposed for weight.
Non-alcoholic fatty liver disease (NAFLD / NASH)
GLP-1 RAs reduce hepatic fat content and liver inflammation. Semaglutide has shown histological improvement in early trials for non-alcoholic steatohepatitis (NASH). With NAFLD affecting up to 25% of the global population and strongly linked to cardiovascular risk, this emerging indication could have population-scale impact.
Chronic kidney disease
Emerging data from the FLOW trial (semaglutide in CKD) and meta-analyses suggest GLP-1 RAs attenuate proteinuria and may slow eGFR decline — complementing SGLT2 inhibitors in the diabetic kidney disease population. This renal benefit is still being characterised, but early signals are promising.
The next frontier: dual and triple agonists
Tirzepatide (Mounjaro/Zepbound), a dual GLP-1/GIP receptor agonist, has demonstrated superior weight loss and glycaemic control compared to semaglutide monotherapy in head-to-head trials. Cardiovascular outcome data from SURPASS-CVOT is eagerly awaited. Meanwhile, triple agonists targeting GLP-1, GIP, and glucagon receptors simultaneously are in Phase 2 and 3 development — designed to address NASH, metabolic syndrome, and obesity with even greater potency.
🔭 Looking ahead
We are entering the era of precision cardiometabolic polypharmacy — targeted, mechanism-driven therapies addressing the root causes of cardiovascular disease, not just its biochemical markers.
7. GLP-1 RAs and Heart Failure: What the 2026 Evidence Shows
Heart failure is a nuanced area for GLP-1 RAs. Earlier trials were not designed to assess this endpoint specifically, and some showed neutral effects on HF hospitalisation. However, new 2026 data has added important clarity.
Neves, Lobato, Leite et al., 2026 — Obesity Reviews meta-analysis
A 2026 systematic review and meta-analysis published in Obesity Reviews specifically examined GLP-1 RAs for the prevention of new-onset heart failure in placebo-controlled trials. The analysis found a statistically significant reduction in the incidence of new heart failure, particularly in patients with obesity and metabolic risk factors — suggesting a preventive role even for this endpoint.
This is a meaningful distinction: while SGLT2 inhibitors remain superior for treating established heart failure, GLP-1 RAs may play a role in preventing heart failure from developing in the first place — likely through their anti-inflammatory, weight-reducing, and blood pressure-lowering effects.
📋 Practical takeaway
For patients with established heart failure with reduced ejection fraction (HFrEF): prioritise an SGLT2 inhibitor. For patients at risk of developing heart failure due to obesity, insulin resistance, or metabolic syndrome, a GLP-1 RA may offer meaningful preventive benefit. The combination remains the optimal strategy for high-risk patients.
8. Practical Clinical Guide: Who Should Be Offered a GLP-1 RA?
Translating evidence into real-world practice requires a structured, patient-centred approach. Here is a framework grounded in the latest 2025–2026 evidence.
Ideal patient profile
Type 2 diabetes with established ASCVD or high cardiovascular risk
BMI ≥ 27 kg/m² with at least one weight-related comorbidity
Obesity without diabetes but with established cardiovascular disease (SELECT-eligible)
Features of atherogenic dyslipidaemia (high triglycerides, low HDL, elevated remnant cholesterol)
Patients with "controlled" HbA1c but persistent residual cardiovascular risk
Prescribing strategy
In T2DM + established ASCVD: Use a GLP-1 RA with proven cardiovascular benefit (semaglutide, liraglutide, dulaglutide) as first-line or add-on to metformin, independent of HbA1c. Combine with an SGLT2 inhibitor if heart failure or CKD is also present.
In obesity without diabetes: Consider semaglutide 2.4 mg (Wegovy) if the patient has established cardiovascular disease — SELECT-level evidence now supports this indication.
Monitoring protocol
HbA1c every 3 months initially, then every 6 months once stable
Body weight at every clinical visit
eGFR and urine albumin-to-creatinine ratio (ACR) every 6–12 months
Full lipid panel including non-HDL-C and remnant cholesterol every 6–12 months
Blood pressure at every visit
Screen for gallbladder symptoms in patients with significant weight loss
Document ASCVD status clearly to support insurance prior authorisation
Start low, go slow: the titration principle
Gastrointestinal side effects — especially nausea — are the primary reason patients discontinue therapy. These are largely dose-dependent and transient. Slow titration allows the enteric nervous system to adapt:
Semaglutide: begin at 0.25 mg weekly for 4 weeks, then titrate to 0.5 mg, then 1 mg
Liraglutide: begin at 0.6 mg daily, titrate weekly up to 1.8 mg (or 3.0 mg for obesity)
Advise taking with a small meal
If nausea persists: hold dose rather than discontinue — most patients tolerate therapy long-term
Smart combination therapy framework
Use complementary therapies based on the patient's dominant risk:
Here is the clinical guidance reformatted into clear, actionable points organized by your patient's dominant risk profile:
Atherosclerosis (History of MI or Stroke):
Priority Drug: A GLP-1 receptor agonist with proven cardiovascular benefit.
Add-On Therapy: Intensive statin therapy, adding ezetimibe if needed to reach cholesterol targets.
Heart Failure:
Priority Drug: An SGLT2 inhibitor (critical for reducing heart failure hospitalizations).
Add-On Therapy: Introduce a GLP-1 receptor agonist if the patient has concurrent atherosclerotic risk factors.
Chronic Kidney Disease (CKD):
Priority Drug: An SGLT2 inhibitor to protect renal function.
Add-On Therapy: Add a GLP-1 receptor agonist if persistent proteinuria (excess protein in the urine) is present.
Obesity + Cardiovascular Disease:
Priority Drug: High-dose Semaglutide (2.4 mg) to target both weight loss and major adverse cardiovascular events.
Add-On Therapy: Layer in an SGLT2 inhibitor if the patient also has co-existing heart failure or CKD.
Universal Care (All Patients):
Baseline Management: Every patient requires optimal statin therapy.
Clinical Framework: Guide long-term care using the ABCS framework: optimize A1C, manage Blood pressure, aggressively lower Cholesterol, and mandate Smoking cessation.💡 Clinical pearl
In patients with "normal" LDL-C but persistent atherogenic dyslipidaemia (high TG, low HDL, elevated remnant cholesterol) and insulin resistance, GLP-1 RAs target the metabolic drivers of residual cardiovascular risk that statins alone cannot address.
9. Safety Profile and Side Effects
GLP-1 RAs have a well-characterised safety profile across tens of thousands of patient-years of exposure. Understanding the common and rare adverse effects helps clinicians and patients make informed decisions.
Common: gastrointestinal effects
Nausea, vomiting, diarrhoea, and constipation affect approximately 30–40% of patients, particularly during dose escalation. These are generally transient and diminish within 4–8 weeks as the body adapts. The "start low, go slow" titration strategy is the most effective mitigation approach.
Gallbladder disease
Rapid weight loss increases bile lithogenicity. Gallstones and acute cholecystitis occur at higher rates in GLP-1 RA users — a clinically meaningful consideration in patients with a prior history of gallbladder disease. Screen with imaging if abdominal symptoms arise.
Pancreatitis (rare and debated)
Current evidence does not establish a causal relationship between GLP-1 RAs and pancreatitis. The absolute risk appears very low. However, avoid use in patients with a personal or family history of pancreatitis and monitor for unexplained, severe abdominal pain.
Anaesthetic considerations
GLP-1 RAs delay gastric emptying. Patients undergoing elective surgery should inform their anaesthetic team. Many anaesthetic societies now recommend extending pre-procedural fasting times or temporarily withholding GLP-1 RAs before surgery — though guidance continues to evolve.
Thyroid considerations
Rodent studies showed C-cell thyroid tumours at suprapharmacological doses, but no confirmed human signal has been identified across the large CVOT programmes. GLP-1 RAs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2).
Risk of hypoglycaemia
Extremely low as monotherapy. GLP-1 RAs stimulate insulin secretion only when blood glucose is elevated — a glucose-dependent mechanism that essentially eliminates the risk of drug-induced hypoglycaemia. When combined with sulphonylureas or insulin, the sulphonylurea dose may need to be reduced.
⛔ Contraindications
Personal or family history of medullary thyroid carcinoma or MEN2. History of pancreatitis (relative contraindication). Severe gastrointestinal disease. Pregnancy. Always consult current prescribing guidelines and patient-specific factors.
10. Common Myths & Misconceptions
❌ Myth: These drugs only work for heart patients because they control blood sugar.
✅ Fact: The SELECT trial enrolled patients without diabetes and found a 20% MACE reduction. The cardiovascular benefits are mechanistically independent of glucose lowering — operating through anti-inflammatory, anti-atherosclerotic, and endothelial pathways.
❌ Myth: "All GLP-1 drugs protect the heart equally."
✅ Fact: This is false. Exenatide twice-daily (EXSCEL) showed non-inferiority but not superiority. Short-acting agents in general have weaker cardiovascular evidence than long-acting weekly formulations. Agent selection matters.
❌ Myth: The side effects are too bad — most patients stop taking them.
✅ Fact: Nausea is common early but transient in most patients. With a slow titration schedule, long-term tolerability is high. In the large CVOT trials, discontinuation rates due to adverse effects were generally similar to placebo arms over multi-year follow-up.
❌ Myth: "You only need one or the other — GLP-1 or SGLT2 inhibitor."
✅ Fact: Current 2025–2026 guidelines strongly support combination use in high-risk patients. The two classes protect complementary aspects of cardiometabolic health — atherosclerosis versus heart failure and renal function. Most high-risk patients benefit from both.
❌ Myth: My HbA1c is fine, so I don't need a GLP-1 RA."
✅ Fact: Cardiovascular benefit is independent of baseline HbA1c in multiple trials. The underlying biology of atherogenesis, insulin resistance, and inflammation continues to drive risk even when glucose metrics appear controlled.
❌ Myth: "These are just 'diet drugs' with heart marketing."
✅ Fact While GLP-1 RAs do reduce body weight, their cardiovascular benefits in trials like LEADER and SUSTAIN-6 were not explained by weight loss alone. Direct anti-inflammatory and vascular mechanisms operate independently of changes on the scale.
11. Frequently Asked Questions
Can I take a GLP-1 medication if I don't have diabetes?
Yes. Semaglutide 2.4 mg (Wegovy) is FDA-approved for chronic weight management in adults with obesity (BMI ≥ 30) or overweight (BMI ≥ 27) with at least one weight-related condition. The SELECT trial proved a 20% reduction in major cardiovascular events in obese non-diabetic patients with established cardiovascular disease. Talk to your doctor about whether you meet these criteria.
Which GLP-1 drug is the best for heart protection?
Based on available trial evidence, injectable semaglutide (Ozempic) showed the largest MACE reduction (26% in SUSTAIN-6), followed by liraglutide (13% in LEADER) and dulaglutide (12% in REWIND). However, "best" depends on your personal health profile, tolerability, and whether you need once-weekly versus daily dosing. Semaglutide 2.4 mg also has the broadest evidence in non-diabetic populations. Discuss agent selection with your prescribing physician based on your individual risk factors.
Can GLP-1 drugs be used together with SGLT2 inhibitors?
Yes — and current guidelines increasingly recommend this for high-risk patients. GLP-1 RAs primarily protect against atherosclerotic events (heart attack, stroke), while SGLT2 inhibitors protect against heart failure progression and kidney disease. Used together, they provide complementary protection across the full cardiometabolic risk spectrum. This combination is now considered a foundational therapy in patients with type 2 diabetes who have both cardiovascular disease and chronic kidney disease or heart failure, regardless of their starting HbA1c.
How long does it take to see cardiovascular benefit?
The CVOTs typically ran for 2–5 years, and benefits in MACE were often apparent within the first 1–2 years of treatment. Anti-inflammatory and blood pressure benefits can begin within weeks to months of starting therapy. Weight loss peaks over 12–18 months in most patients. Like statins, GLP-1 RAs likely require sustained use to maintain their cardiovascular protective effects.
What are the most common side effects — and do they go away?
The most common side effects are gastrointestinal — nausea, vomiting, diarrhoea, and constipation — affecting 30–40% of patients. These are dose-dependent and typically resolve within 4–8 weeks as the body adjusts. The key is slow dose titration: starting at the lowest dose and increasing gradually over several weeks. Most patients who experience nausea early on can tolerate long-term therapy once titrated appropriately.
Are GLP-1 drugs safe for kidneys?
Yes, and emerging evidence suggests they may actively protect kidney function. GLP-1 RAs have been shown to reduce proteinuria (protein in the urine, a marker of kidney damage). The FLOW trial (semaglutide in CKD) showed significant renoprotective effects. In patients with both cardiovascular and kidney disease, combining a GLP-1 RA with an SGLT2 inhibitor provides comprehensive coverage across both risk domains.
Can GLP-1 medications cause thyroid cancer?
The concern arises from rodent studies showing C-cell thyroid tumours at very high doses — but no confirmed human signal has been identified across the large CVOT populations involving tens of thousands of patients. GLP-1 RAs are contraindicated in people with a personal or family history of medullary thyroid carcinoma (MTC) or MEN2 syndrome as a precautionary measure. Outside of these groups, the available evidence does not support a meaningful thyroid cancer risk in humans.
What is the difference between semaglutide and tirzepatide?
Semaglutide (Ozempic/Wegovy) is a single GLP-1 receptor agonist. Tirzepatide (Mounjaro/Zepbound) is a dual agonist targeting both GLP-1 and GIP receptors. By engaging two metabolic pathways, tirzepatide generally produces greater weight loss and glycaemic reduction than semaglutide in head-to-head trials. Cardiovascular outcome data from tirzepatide's dedicated CVOT (SURPASS-CVOT) is being closely watched — early signals are promising but full results are pending.
Do I need to stay on this medication forever?
For patients using GLP-1 RAs primarily for cardiovascular protection, the evidence supports long-term, sustained use — similar to statins or antihypertensives. The LEADER and REWIND trials showed benefit over 2–5 years of continuous therapy. When GLP-1 RAs are discontinued, weight tends to return and cardiometabolic risk markers worsen. In most high-risk patients, these are intended as chronic medications rather than short-term interventions.
Does insurance cover GLP-1 drugs for heart disease prevention?
Coverage varies significantly by insurer and indication. Most plans cover GLP-1 RAs when prescribed for type 2 diabetes. Coverage for obesity (without diabetes) and cardiovascular prevention is expanding but often requires prior authorisation — documentation of ASCVD, BMI criteria, or prior treatment attempts. The FDA approval of semaglutide 2.4 mg for cardiovascular risk reduction (post-SELECT) has strengthened the coverage argument for obesity + CVD patients. Manufacturer patient assistance programmes are available for eligible patients.
Can I take a GLP-1 RA if I have pancreatitis?
This is a relative contraindication. While large trials have not established a clear causal link between GLP-1 RAs and pancreatitis, current guidelines advise against their use in patients with a history of pancreatitis. If you have had pancreatitis, discuss the risks and benefits carefully with your doctor — the absolute risk appears low, but caution is warranted.
12. Clinical pearls
1. The "Plaque Stabilizer" Effect
Scientific Perspective: GLP-1 RAs are essentially anti-atherosclerotic agents. They reduce macrophage accumulation and the expression of pro-inflammatory cytokines (IL-6, TNF-alpha) within the vascular wall. This stabilizes the fibrous cap of atherosclerotic plaques, making them less likely to rupture and cause a myocardial infarction.
Think of these drugs like "internal armor" for your blood vessels. Beyond just lowering sugar, they help calm down inflammation in your arteries, making it less likely that existing blockages will break off and cause a heart attack or stroke.
2. Glucose-Dependent Safety
Scientific Perspective: The insulinotropic effect of GLP-1 RAs is glucose-dependent. This means they only stimulate the pancreas to release insulin when blood glucose levels are elevated. As glucose levels normalize, the insulin secretion stimulus diminishes, resulting in a negligible risk of therapy-induced hypoglycemia.
One of the biggest fears with diabetes medicine is "going too low" (hypoglycemia). Because this medication only works when your sugar is actually high, it’s much safer than older treatments and won't cause your blood sugar to crash unexpectedly.
3. The "Twinning" Strategy (Synergy with SGLT2i)
Scientific Perspective: Combining GLP-1 RAs with SGLT2 inhibitors provides dual-pathway protection. GLP-1 RAs target Atherosclerotic Cardiovascular Disease (ASCVD) via anti-inflammatory pathways, while SGLT2 inhibitors target Heart Failure (HF) and Chronic Kidney Disease (CKD) via natriuresis and osmotic diuresis.
If your doctor prescribes two different types of "diabetes" drugs, they aren't just doubling up. One protects the "pipes" (your arteries) from clogging, while the other protects the "pump" (your heart) and the "filters" (your kidneys).
4. Brain-Gut Reset (Not Just "Fullness")
Scientific Perspective: GLP-1 receptors in the hypothalamus and hindbrain modulate reward-based eating and homeostatic hunger. These agents decrease "food noise"—the intrusive, obsessive thoughts about eating—by slowing gastric emptying and signaling the brain's satiety centers.
This isn't just "willpower in a pen." It actually changes how your brain communicates with your stomach. Many people find that the "chatter" in their head about food finally goes quiet, making it easier to make healthy choices without feeling like they are constantly fighting an urge.
5. The "Start Low, Go Slow" Mandate
Scientific Perspective: Gastrointestinal side effects (nausea/vomiting) are the primary reason for discontinuation. These are often transient and related to the rate of dose titration. Initiating at the sub-therapeutic dose (e.g., 0.25 mg semaglutide) allows the enteric nervous system to adapt to the delay in gastric emptying.
You might feel some nausea or a "heavy" stomach for the first few weeks, but this is usually temporary. The secret to success is patience—starting at a very low dose and increasing it slowly gives your body time to adjust, ensuring you get the heart-saving benefits without the side effects.
13. Conclusion: A Paradigm Shift in Cardiometabolic Medicine
The evidence is clear and consistent: GLP-1 receptor agonists represent far more than a blood sugar lowering drug class. They are multi-system cardiometabolic agents that simultaneously address inflammation, atherosclerosis, visceral adiposity, endothelial dysfunction, and direct cardiac risk — all through a single weekly injection for many formulations.
The question for 2026 is no longer whether these agents protect the heart, but which patients should have access to them and why are not more people receiving them? Barriers, including cost, insurance restrictions, and limited clinical awareness, continue to delay the real-world implementation of therapies with substantial evidence behind them.
Action steps for patients
If you have type 2 diabetes and cardiovascular disease or high CV risk, ask your doctor whether a GLP-1 RA with proven MACE benefit is appropriate for you
If you have obesity and established cardiovascular disease without diabetes, ask about semaglutide 2.4 mg based on SELECT trial data
If you are on a GLP-1 RA: do not discontinue without discussing with your prescriber — the benefits are sustained with long-term use
If nausea is a problem, ask about slow titration before giving up on therapy
Combine with lifestyle: low-refined-carbohydrate diet, post-meal walks, omega-3 supplementation where indicated
Action steps for clinicians
Shift prescribing framework: use cardiovascular risk, not HbA1c alone, to guide agent selection
Use agents with demonstrated superiority (semaglutide, liraglutide, dulaglutide) — not all GLP-1 RAs are equivalent
Combine GLP-1 RAs + SGLT2 inhibitors in patients with overlapping atherosclerosis and heart failure/CKD
Document ASCVD status clearly to support prior authorisation and insurance approval
Counsel patients on GI side effects proactively — adherence depends on appropriate expectations
Inform anaesthetic teams about GLP-1 RA use ahead of elective procedures
We are at the beginning of the era of metabolic cardiology. GLP-1 RAs are not the endpoint — they are a foundation on which dual and triple agonists, precision patient selection, and multi-axis combination therapy will be built. The future of cardiovascular medicine lies in addressing the root causes of heart disease, not just its downstream biomarkers.
Explore related reads on this site:
GLP-1s and Muscle Loss: What’s Normal, What’s Not, and How to Protect Lean Mass
Your Cholesterol Isn’t the Whole Story: The Hormone Imbalances Driving Heart Disease
Can GLP-1 Drugs Prevent Heart Attacks? New Trial Data Changes Everything
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Remnant Cholesterol: The Hidden Link Between Insulin Resistance, Type 2 Diabetes, and Heart Disease
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
Why Belly Fat Causes Insulin Resistance: Portal Theory Explained Simply
References & Sources
American Diabetes Association. (2025). Standards of care in diabetes—2025. Diabetes Care, 48(Suppl. 1), S1–S325. https://doi.org/10.2337/dc25-S001
Galli, M., Benenati, S., Laudani, C., ... [Include up to 20 authors if available; if more, list first 19, add an ellipsis (...), then the last author]. (2025). Cardiovascular effects and tolerability of GLP-1 receptor agonists: A systematic review and meta-analysis of 99,599 patients. Journal of the American College of Cardiology. Advance online publication. https://doi.org/10.1016/j.jacc.2025.08.027
Gerstein, H. C., Colhoun, H. M., Dagenais, G. R., Diaz, R., Lakshmanan, M., Pais, P., Probstfield, J., Riesmeyer, J. S., Riddle, M. C., Rydén, L., Xavier, D., Atisso, C. M., Dyal, L., Hall, S., Rao-Melacini, P., Wong, G., Avezum, A., Basile, J., Chung, N., . . . Yusuf, S. (2019). Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. The Lancet, 394(10193), 121–130. https://doi.org/10.1016/S0140-6736(19)31149-3
Holman, R. R., Bethel, M. A., Mentz, R. J., Thompson, V. P., Lokhnygina, Y., Buse, J. B., Chan, J. C., Choi, J., Gustavson, S. M., Iqbal, N., Maggioni, A. P., Marso, S. P., Öhman, C. R., Pagidipati, N. J., Poulter, N., Ramachandran, A., Zinman, B., & Hernandez, A. F. (2017). Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, 377(13), 1228–1239. https://doi.org/10.1056/NEJMoa1612917
Kong, F., Zhao, Y., Zhang, W., [Include up to 20 authors here], & [Last Author]. (2026). Comprehensive evaluation of GLP-1 receptor agonists: An umbrella review of clinical outcomes across multiple diseases. Nature Communications, 17, Article 972. https://doi.org/10.1038/s41467-025-67701-9
Lincoff, A. M., Brown-Frandsen, K., Colhoun, H. M., Deanfield, J., Emerson, S. S., Esbjerg, S., Hardt-Rasmussen, O., Hovingh, G. K., Kahn, S. E., Kushner, R. F., Lingvay, I., Oral, T. K., Michelsen, M. M., Plutzky, J., Tornøe, C. W., & Ryan, D. H. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine, 389(24), 2221–2232. https://doi.org/10.1056/NEJMoa2310775
Marso, S. P., Bain, S. C., Consoli, A., Eliaschewitz, F. G., Jódar, E., Leiter, L. A., Lingvay, I., Rosenstock, J., Seufert, J., Warren, M. L., Woo, V., Hansen, O., Holst, A. G., Pettersson, J., & Vilsbøll, T. (2016). Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. New England Journal of Medicine, 375(19), 1834–1844. https://doi.org/10.1056/NEJMoa1607141
Marso, S. P., Daniels, G. H., Brown-Frandsen, K., Kristensen, P., Mann, J. F., Nauck, M. A., Nissen, S. E., Pocock, S., Poulter, N. R., Ravn, L. S., Steinberg, W. M., Stockner, M., Zinman, B., Bergenstal, R. M., & Buse, J. B. (2016). Liraglutide and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, 375(4), 311–322. https://doi.org/10.1056/NEJMoa1603827
McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., Burri, H., Butler, J., Čelutkienė, J., Chioncel, O., Cleland, J. G. F., Coats, A. J. S., Crespo-Leiro, M. G., Farmakis, D., Gilard, M., Heymans, S., Hoes, A. W., Jaarsma, T., Jankowska, E. A., . . . Skibelund, A. K. (2023). 2023 Focused update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 44(37), 3627–3639. https://doi.org/10.1093/eurheartj/ehad360
Nauck, M. A. (2025). Glucagon-like peptide-1 receptor agonists and next-generation incretin-based therapies. The Lancet. Advance online publication. https://doi.org/10.1016/S0140-6736(25)02105-1
Neves, J., Lobato, C., Leite, A., [Include intermediate authors], & [Last Author]. (2026). GLP-1 receptor agonists for the prevention of new-onset heart failure: A systematic review and meta-analysis of placebo-controlled randomized clinical trials. Obesity Reviews, 27(4), Article e70043. https://doi.org/10.1111/obr.70043
Perkovic, V., Tuttle, K. R., Rossing, P., Mahaffey, K. W., Mann, J. F. E., Bakris, G. L., Baeres, F. M. M., Idorn, T., Lange, M., Nguyen, T. Q., Nauck, M. A., & Pratley, R. E. (2024). Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. New England Journal of Medicine, 391(2), 109–121. https://doi.org/10.1056/NEJMoa2403539
Peter, K., Roka, O., Sepp, E., [Include intermediate authors], & [Last Author]. (2026). The long-term cardiovascular safety and efficacy of GLP-1 receptor agonists in high-risk cardiovascular populations: A systematic review and meta-analysis. Cardiovascular Diabetology Endocrinology Reports, 12, Article 36. https://doi.org/10.1186/s40842-026-00295-3
Rosen, C. J., & Ingelfinger, J. R. (2026). GLP-1 receptor agonists. New England Journal of Medicine, 394(13), 1313–1324. https://doi.org/10.1056/NEJMra2500106
Westermeier, F., & Fisman, E. S. (2025). GLP-1 receptor agonists and cardiometabolic protection: Historical development and future challenges. Cardiovascular Diabetology, 24, Article 44. https://doi.org/10.1186/s12933-025-02608-9
Yang, H. M. (2025). GLP-1 agonists in cardiovascular diseases: Mechanisms, clinical evidence, and emerging therapies. Journal of Clinical Medicine, 14(19), Article 6758. https://doi.org/10.3390/jcm14196758
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. All content is based on peer-reviewed scientific literature available at time of publication (April 2026). Individual medical decisions should always be made in consultation with a qualified healthcare provider who can assess your personal clinical context. Never start, stop, or alter any medication without professional guidance.