ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Discover why Apolipoprotein B (ApoB) is a more accurate predictor of heart disease than LDL cholesterol. Learn target levels, hidden risk, and when to test ApoB.
HEARTMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
4/5/202616 min read
What is ApoB?
Apolipoprotein B (ApoB) is a protein found on all atherogenic lipoproteins, including LDL, VLDL, IDL, and lipoprotein(a). Each of these particles carries exactly one ApoB molecule, making ApoB a direct measure of the total number of cholesterol-carrying particles that can enter artery walls and cause plaque buildup. Because cardiovascular risk is driven by particle number—not just cholesterol content—ApoB is considered a more accurate marker of heart disease risk than LDL cholesterol alone.
ApoB vs LDL: What Most People Miss
We’ve been focusing on the wrong number.
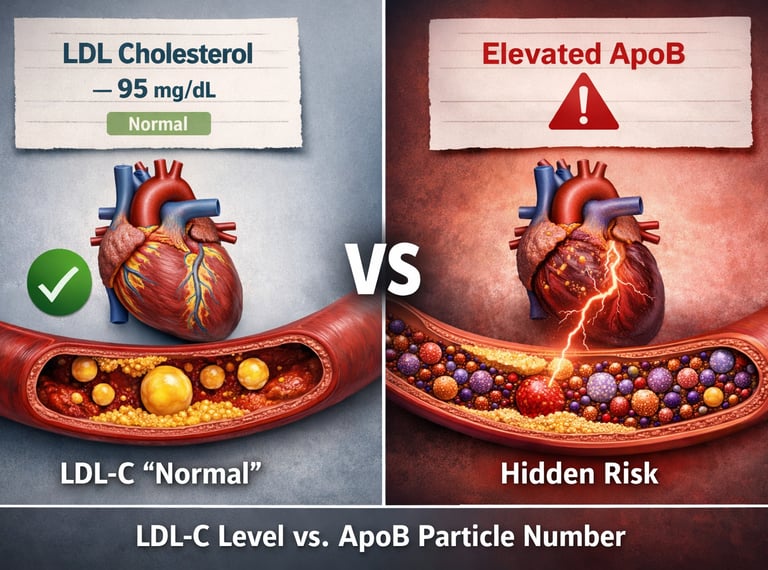
For years, LDL cholesterol (LDL-C) has been the main test used to assess heart risk. If it’s “normal,” most people are reassured. But this can be misleading.LDL-C measures cholesterol, not the actual problem.
Think of LDL particles as tiny carriers in your blood. LDL-C tells you how much cholesterol they carry—but not how many carriers there are.ApoB counts the number of dangerous particles.
Every atherogenic particle (LDL, VLDL, IDL, Lp(a)) has one ApoB protein. So ApoB gives a direct count of how many particles are circulating—and potentially damaging your arteries.More particles = higher risk.
Even if each particle carries less cholesterol, a higher number of particles increases the chance they enter the artery walls and start plaque formation.This is why “normal LDL” can still be risky.
Many people—especially those with insulin resistance, diabetes, or belly fat—have lots of small particles. LDL-C looks fine, but ApoB is high.This mismatch is called “discordance.”
It’s one of the most important hidden risk patterns in modern cardiometabolic disease—and it often goes undetected.ApoB reflects the real driver of atherosclerosis.
Plaque builds from particle entry into arteries—not just cholesterol levels. ApoB aligns directly with this mechanism.Guidelines are starting to catch up.
Major cardiovascular societies now recommend ApoB, especially in high-risk or metabolically unhealthy patients.The bottom line:
If you only measure LDL-C, you may miss the real risk. Measuring ApoB gives a clearer, more complete picture of cardiovascular danger.
Clinical pearls
1. The "Truck vs. Cargo" Distinction
LDL-C measures the cumulative mass of cholesterol (the cargo) within particles, whereas ApoB provides a direct quantification of the total number of atherogenic particles (the trucks). Risk is driven by the frequency of particle-wall interactions, making particle concentration a superior predictor of events than cholesterol volume.
Think of your arteries like a highway. Your standard LDL test measures how much "stuff" is inside the delivery trucks. ApoB counts the actual number of trucks on the road. Even if the trucks are nearly empty, having too many of them increases the chances of a crash.
2. The Trap of Metabolic Discordance
In patients with insulin resistance or hypertriglyceridemia, LDL particles become "small and dense." This leads to a discordance where LDL-C appears low or normal, but ApoB is significantly elevated. Relying solely on LDL-C in these phenotypes results in a gross underestimation of residual cardiovascular risk.
If you have type 2 diabetes or carry extra weight around your middle, your standard cholesterol test might "lie" to you. It might show a healthy LDL level because your particles are small and "light," but you could actually have a dangerously high number of them circulating in your blood.
3. ApoB as a "Universal Multi-Tool"
Unlike LDL-C, which only captures cholesterol in LDL particles, a single ApoB molecule is present on every single artery-clogging particle, including VLDL, IDL, and the highly inflammatory Lp(a). Measuring ApoB provides a holistic "sum" of the total atherogenic burden.
Standard tests only look at one type of bad cholesterol. An ApoB test is like an all-in-one security camera—it catches every single type of particle that can cause a heart attack, including the ones your normal blood test completely ignores.
4. Treatment Targets: Go Low, Go Early
Mendelian randomization studies confirm that the cumulative exposure to ApoB-containing particles is the primary driver of atherosclerosis. Lowering ApoB early in life significantly shifts the trajectory of plaque accumulation, suggesting that "lower for longer" is the optimal preventative strategy.
Heart disease doesn't happen overnight; it’s like a slow-growing rust inside your pipes. The lower you keep your ApoB, starting as early as possible, the less "rust" accumulates, drastically lowering your risk of a heart attack when you're older.
5. Stability and Convenience in Testing
ApoB is measured directly by immunoassay and is highly standardised, showing significantly less biological and analytical variation than calculated LDL-C. Furthermore, because it is not significantly altered by recent fat intake, it can be accurately measured in a non-fasting state.
You don't need to skip breakfast for this test. Because ApoB is a direct count of proteins rather than a calculated guess based on fats, the results are more consistent and reliable than a standard cholesterol panel, regardless of what you ate that morning.
ApoB vs LDL Cholesterol: The Most Important Heart Risk Marker You Are Probably Not Measuring
Your LDL cholesterol looks perfect. Your doctor smiles and says you're in the clear—no statins needed. You breathe a sigh of relief and walk out feeling safe.
But hidden within your arteries, an entirely different, far more dangerous story may be unfolding.
A growing number of people who suffer heart attacks and strokes had “normal” LDL-C levels at their last check-up. Some were even on cholesterol-lowering medication. What these standard tests missed is the real driver of plaque buildup: the sheer number of atherogenic particles circulating in the blood.
That hidden threat is best revealed by a single protein called Apolipoprotein B, or ApoB.
Unlike LDL-C, which only measures the amount of cholesterol cargo inside lipoprotein particles, ApoB counts the actual number of dangerous “delivery trucks” on the road. Each atherogenic particle—LDL, VLDL, IDL, and Lp(a)—carries exactly one ApoB molecule. More particles mean more opportunities to penetrate and damage artery walls, regardless of how much cholesterol each one carries (De Oliveira-Gomes et al., 2024).
This discordance is surprisingly common. Studies show that up to 20–30% of individuals with apparently normal LDL-C still have elevated ApoB, particularly those with insulin resistance, type 2 diabetes, high triglycerides, or central obesity (Galimberti et al., 2023). In these metabolically complex patients, relying solely on LDL-C can create a dangerous false sense of security.
Science has now caught up. Landmark reviews confirm that ApoB consistently outperforms LDL-C as a predictor of atherosclerotic cardiovascular disease (ASCVD) events (Galimberti et al., 2023). Even the 2026 ACC/AHA Dyslipidemia Guidelines (Blumenthal et al., 2026) now give ApoB a Class 2a recommendation for assessing residual risk once LDL-C and non-HDL-C targets are achieved—especially in diabetes, elevated triglycerides, and cardiovascular-kidney-metabolic syndrome
The era of LDL-C alone is ending. For millions, ApoB is the missing piece that could prevent the next heart attack.
What is LDL Cholesterol and How is it Measured?
LDL-C refers to the amount of cholesterol found within low-density lipoprotein particles. Most laboratories estimate it using the Friedewald equation—a formula that calculates LDL-C indirectly from total cholesterol, HDL, and triglycerides. Direct LDL measurement is also available but less commonly used in routine practice.
LDL-C became the dominant lipid marker through landmark trials in the 1980s and 1990s, showing that lowering it with statins dramatically reduced cardiovascular events. That evidence remains valid. The problem is not that LDL-C is wrong—it is that it is incomplete.
LDL-C can look perfectly normal in people who have a high number of small, dense LDL particles packed with relatively little cholesterol. These cholesterol-depleted particles are just as dangerous—arguably more so—because they penetrate artery walls more easily. But because each one carries less cholesterol, the total LDL-C reading does not reflect how many of them are circulating.
1 ApoB molecule per every atherogenic particle
~ 30%Of patients with "normal" LDL may have elevated ApoB
5 Lipoprotein types measured by one ApoB test (LDL, VLDL, IDL, Lp(a), chylomicron remnants)
ApoB vs LDL-C: Key Differences
What it measures
LDL-C: Amount of cholesterol carried within LDL particles
ApoB: Total number of atherogenic lipoprotein particles
Reflection of cardiovascular risk
LDL-C: Indirect estimate of risk
ApoB: Direct measure of atherogenic burden
Effect of particle size
LDL-C: Influenced by particle size; may appear falsely low with small, dense LDL
ApoB: Not affected by particle size
Lipoproteins included
LDL-C: Primarily LDL particles
ApoB: Includes LDL, VLDL, IDL, lipoprotein(a), and remnant particles
Fasting requirement
LDL-C: Often recommended, especially when triglycerides are elevated
ApoB: Not required
Predictive power (evidence-based)
LDL-C: Good predictor of cardiovascular risk
ApoB: Superior predictor in most studies
Use in discordance (mismatch between LDL-C and particle number)
LDL-C: Limited clinical utility
ApoB: Essential for accurate risk assessment. Galimberti et al. (2023) conducted a comprehensive review in Pharmacological Research comparing ApoB and LDL-C across multiple cohort studies and concluded that ApoB consistently outperforms LDL-C in predicting atherosclerotic cardiovascular disease (ASCVD) events—particularly in patient populations where LDL-C and particle number diverge.
The Discordance Problem: When Normal LDL Hides Real Risk
"Discordance" is the technical term for what happens when LDL-C and ApoB tell different stories. A person has discordant results when their LDL-C appears normal or even low, yet their ApoB count is elevated—indicating a high number of atherogenic particles actively depositing in artery walls.
Who is most at risk of discordance? Patients with insulin resistance, type 2 diabetes, high triglycerides, central obesity, or low HDL are at the highest risk of having elevated ApoB despite an apparently normal LDL-C. In these individuals, relying on LDL-C alone may be dangerously misleading.
Genedy and Zouwail (2025 ) in the Journal of Clinical Lipidology examined ApoB/LDL-C discordance specifically in patients with genetically confirmed heterozygous familial hypercholesterolaemia (HeFH). Their findings were hypothesis-generating but compelling: discordance in this high-risk group carried meaningful implications for ASCVD prediction, reinforcing the view that ApoB provides clinically independent information even when the underlying genetic risk profile is already known.
This matters enormously in practice. A patient with metabolic syndrome may have LDL-C of 2.5 mmol/L (97 mg/dL)—below most treatment thresholds—yet have 150 mg/dL of ApoB, indicating a high particle burden and substantially elevated risk. That patient may go untreated for years, only to present with a myocardial infarction that could have been prevented.
Pathophysiology: Why Does Particle Number Drive Atherosclerosis?
The process of atherosclerosis begins when ApoB-containing particles penetrate the arterial endothelium (the inner lining of blood vessels) and become trapped in the vessel wall. Once there, they are oxidised and engulfed by immune cells, initiating the inflammatory cascade that builds into plaque.
The critical insight is this: each particle event is independent. It does not matter whether a particle carries a lot of cholesterol or a little—if it crosses the endothelial barrier, it contributes to plaque. Therefore, total particle count (measured by ApoB) is the primary driver of atherogenic exposure, not the total cholesterol load per particle.
Tsimikas and Bittner (2024), writing in the Journal of the American College of Cardiology, provided an elegant analysis of how ApoB, LDL particle number, and Lp(a) each contribute independently to ASCVD risk. Their paper highlights that ApoB encompasses all atherogenic lipoprotein particles—not just LDL—making it a more comprehensive measure of cardiovascular threat than any cholesterol-based metric alone.
The Role of ApoB in Insulin Resistance and Metabolic Syndrome
If you have been diagnosed with type 2 diabetes, prediabetes, fatty liver, PCOS, or simply carry excess weight around your abdomen, your liver is likely overproducing VLDL particles. This is a consequence of insulin resistance: when insulin cannot efficiently suppress fat release from adipose tissue, the liver is flooded with fatty acids and responds by packaging and exporting them as VLDL. Each VLDL carries one ApoB molecule.
Over time, those VLDL particles are converted to IDL and then LDL, but they may be smaller and denser than usual, carrying less cholesterol per particle. The net result: high ApoB, high particle burden, high cardiovascular risk—and a completely unremarkable LDL-C on a standard lab report.
This is why ApoB functions as what some researchers call a "unifying marker" of metabolic dysfunction. Elevated ApoB, high triglycerides, low HDL-C, and a raised TG/HDL ratio are all features of the same underlying pathological process—and ApoB may be the single most informative number for capturing that risk in one test.
Lipoprotein(a): The Hidden Atherogenic Particle ApoB Captures
Lipoprotein(a)—or Lp(a)—is a modified form of LDL with an additional protein called apolipoprotein(a) attached. It is genetically determined, largely resistant to lifestyle modification, and is an independent risk factor for heart attack, stroke, and aortic valve disease. Crucially, each Lp(a) particle carries one ApoB molecule.
This means that in patients with elevated Lp(a), their total ApoB count includes their Lp(a) particle contribution—something that LDL-C measurement entirely ignores. As Tsimikas and Bittner (2024) noted, this is one of the underappreciated advantages of ApoB as a composite measure: it captures the full atherogenic burden across all lipoprotein species simultaneously.
What Does the Evidence Say? Key Trials and Meta-Analyses
Mortensen (2024), in an editorial in the European Heart Journal, reviewed the cumulative evidence base comparing ApoB, LDL-C, and non-HDL-C as predictors of cardiovascular events. The conclusion was unambiguous: ApoB triumphs once more. Not marginally—but consistently and across diverse populations.
Mendelian randomisation studies—which use genetic variants as natural experiments to test causal relationships—have repeatedly confirmed that ApoB particle number, not cholesterol content, is causally linked to atherosclerosis. This is particularly powerful evidence because it is not confounded by diet, medication, or other lifestyle variables.
Major cohort studies including MESA (Multi-Ethnic Study of Atherosclerosis) and INTERHEART, have demonstrated that ApoB reclassifies cardiovascular risk in a meaningful proportion of individuals who would otherwise be considered low-risk by LDL-C criteria alone.
What Do the Guidelines Say?
Guideline bodies are progressively acknowledging ApoB's clinical value:
The European Society of Cardiology (ESC) recommends ApoB as a secondary treatment target and a preferred marker in patients with hypertriglyceridaemia, diabetes, metabolic syndrome, or very low LDL-C.
The Canadian Cardiovascular Society (CCS) has gone furthest, formally recognising ApoB as an alternative primary target for lipid-lowering therapy.
The American Heart Association (AHA) acknowledges ApoB's utility for risk refinement, particularly in patients where LDL-C may be unreliable.
As De Oliveira-Gomes et al. (2024) highlighted, the evidence base for ApoB as a primary clinical target is now robust enough to support broader adoption, and guideline recommendations are expected to evolve accordingly over the next cycle of updates.
What Are the Target ApoB Levels?
Although there is no single universal cutoff, commonly accepted target—based on clinical studies and guideline recommendations—are as follows:
<90 mg/dL
Appropriate for individuals at low or average cardiovascular risk<70 mg/dL
Recommended for those at high cardiovascular risk<55 mg/dL
Advised for very high-risk patients or those in secondary prevention (established cardiovascular disease)
These thresholds broadly align with traditional LDL-C targets but are not direct equivalents. ApoB reflects particle number rather than cholesterol content, and therefore provides independent clinical insight, particularly in patients where LDL-C and ApoB levels are discordant.
Practical Applications: What This Means for Your Health
When Should You Ask for an ApoB Test?
Not everyone needs an ApoB test—but the following scenarios represent high-yield indications where ApoB provides information that a standard lipid panel cannot:
You have a normal LDL but high triglycerides. Elevated triglycerides are a marker of excess VLDL production, which directly increases ApoB. This combination is a textbook discordance scenario.
You have type 2 diabetes, prediabetes, or insulin resistance. These conditions reliably drive VLDL overproduction and elevate ApoB independently of LDL-C.
You carry excess abdominal (central) fat. Visceral adiposity is the metabolic engine behind dyslipidaemia. ApoB often tells the real story when the waist circumference is high.
You have a family history of premature heart disease. Especially if genetic conditions like familial hypercholesterolaemia are suspected, ApoB helps quantify the particle burden that may be driving inherited risk.
You are on statin therapy, but your LDL appears very low. Statins can increase LDL particle size, which lowers LDL-C more than ApoB. ApoB helps confirm whether residual particle risk has truly been addressed.
How to Reduce Your ApoB: Practical Strategies
Lifestyle
Reduce refined carbohydrates and added sugars
Low-carbohydrate or Mediterranean diet
Resistance training + HIIT exercise
Visceral fat loss (most impactful single change)
Reduce alcohol intake
Improve sleep quality
Pharmacotherapy
Statins — reduce hepatic ApoB production
Ezetimibe — an additive for ApoB reduction
PCSK9 inhibitors — powerful particle reduction
Bempedoic acid — statin-intolerant patients
ANGPTL3 inhibitors — emerging agents
Inclisiran — siRNA-based approach
Monitoring
Pair ApoB with TG/HDL ratio
Check fasting insulin or HOMA-IR
Include hs-CRP for inflammation
Measure Lp(a) at least once
Repeat ApoB 3 months post-intervention
Track waist circumference regularly
A Stepwise Clinical Algorithm for Patients and Clinicians
Start with a standard lipid panel. Obtain total cholesterol, LDL-C, HDL-C, and triglycerides. This is your baseline map.
Identify discordance risk factors. Are triglycerides above 1.7 mmol/L? Is HDL low? Is there central obesity, insulin resistance, or diabetes? If yes, LDL-C may be unreliable.
Order ApoB and Lp(a). These two tests together provide a comprehensive picture of atherogenic particle burden. Lp(a) needs to be measured only once in most people.
Adjust treatment targets to ApoB. If ApoB is above goal, intensify lifestyle and/or pharmacotherapy regardless of LDL-C. Monitor ApoB to track response.
Integrate with broader metabolic markers. HOMA-IR, hs-CRP, waist circumference, and fasting glucose complete the cardiometabolic picture and guide the most targeted interventions.
Common Misconceptions — Addressed Plainly
"My LDL is fine, so I'm not at risk." As discussed throughout this article, LDL-C can be entirely normal while ApoB is elevated—particularly in people with metabolic syndrome. Normal LDL does not equal zero risk.
"ApoB is an expensive, specialist test." ApoB testing is inexpensive in most health systems—typically costing similar to or less than a direct LDL measurement. It does not require fasting and is available in most standard pathology laboratories.
"Only cardiologists need to worry about ApoB." GPs, diabetes specialists, endocrinologists, and even obesity medicine physicians should incorporate ApoB into their cardiovascular risk assessment toolkit. It is most valuable precisely in the metabolically complex patients that primary care sees every day.
FAQs
1. What is ApoB, and why does it matter more than LDL cholesterol?
Apolipoprotein B (ApoB) is a structural protein present on the surface of all atherogenic lipoproteins, including LDL, VLDL, IDL, and Lp(a). There is exactly one ApoB molecule per particle, making ApoB a direct measure of the total number of particles capable of entering the arterial wall and initiating atherosclerosis.
In contrast, LDL cholesterol (LDL-C) measures only the cholesterol content carried within these particles. When particles are small and dense (common in insulin resistance and metabolic syndrome), each carries less cholesterol, so LDL-C can appear normal or low while particle number remains high. Multiple studies and meta-analyses show ApoB is a superior predictor of atherosclerotic cardiovascular disease (ASCVD) events compared to LDL-C, particularly when the two markers are discordant (De Oliveira-Gomes et al., 2024; Galimberti et al., 2023).
2. What is a normal or optimal ApoB level?
There is no single universal cutoff, but targets generally align with LDL-C goals according to cardiovascular risk category. The 2026 ACC/AHA Dyslipidemia Guideline suggests the following approximate ApoB targets (in mg/dL):
- <90 mg/dL for lower or intermediate risk (primary prevention)
- <70 mg/dL for high risk
- <55 mg/dL for very high risk or secondary prevention
These levels correspond to reduced cumulative exposure of arteries to atherogenic particles. Many experts consider <80 mg/dL optimal for long-term prevention in metabolically healthy individuals. Treatment decisions should be individualized based on overall risk profile (2026 ACC/AHA Guideline).
3. Can I have a normal LDL cholesterol but still have high ApoB?
Yes, this phenomenon—known as discordance—is common, occurring in approximately 20–50% of individuals depending on the population studied. It is especially frequent in people with insulin resistance, type 2 diabetes, metabolic syndrome, high triglycerides, central obesity, or fatty liver disease.
In these conditions, the liver overproduces VLDL particles that are converted into smaller, denser LDL particles carrying less cholesterol each. Consequently, LDL-C may read as “normal” (<100 mg/dL or even lower), while ApoB remains elevated, reflecting a higher particle burden and greater ASCVD risk (Galimberti et al., 2023; Varvel et al., 2015).
4. Do I need to fast before an ApoB blood test?
No, fasting is not required for ApoB measurement. ApoB levels remain stable in both fasting and non-fasting states. However, if ApoB is ordered together with a standard lipid panel (which includes triglycerides for accurate calculation of LDL-C via the Friedewald or Martin-Hopkins equation), fasting for 8–12 hours is often still recommended for the triglyceride component (Mora et al., 2008; Cleveland Clinic, 2023).
5. Do statins reduce ApoB, or just LDL cholesterol?
Statins reduce both LDL-C and ApoB, but the magnitude of reduction can differ. Statins decrease hepatic production of ApoB-containing particles and upregulate LDL receptor clearance. However, they often enlarge remaining LDL particles, causing LDL-C to fall more than ApoB in some patients. This makes ApoB particularly useful for monitoring residual particle risk on statin therapy. Other agents such as ezetimibe, PCSK9 inhibitors, and bempedoic acid also effectively lower ApoB (De Oliveira-Gomes et al., 2024).
6. Is ApoB available on the NHS or standard health insurance?
Availability and coverage vary by country and insurance plan. In the UK (NHS), ApoB is not routinely offered but may be available in specialist lipid clinics for patients with diabetes, high triglycerides, familial hypercholesterolemia, or suspected discordance. In the United States, the 2026 ACC/AHA guideline supports its use (Class 2a), yet many insurers still classify it as advanced testing, often requiring out-of-pocket payment ($30–100 at direct labs). In India and many other countries, private laboratories offer ApoB affordably without special approval. Check with your local laboratory or clinician.
7. Will ApoB replace LDL cholesterol in routine blood tests?
ApoB is unlikely to fully replace LDL-C in the immediate future, as LDL-C remains a widely available, inexpensive first-line test. However, the 2026 ACC/AHA Dyslipidemia Guideline gives ApoB a Class 2a recommendation for assessing residual risk and guiding therapy intensification once LDL-C and non-HDL-C goals are achieved—particularly in patients with type 2 diabetes, elevated triglycerides (>200 mg/dL), cardiovascular-kidney-metabolic syndrome, or low achieved LDL-C (<70 mg/dL). Its role is expected to expand as evidence and laboratory access grow
Author’s Note (Clinician’s Perspective)
As clinicians, we are trained to trust established biomarkers—and for decades, LDL cholesterol has served us well as a practical and evidence-based tool for cardiovascular risk reduction. Statin trials built on LDL-C have unquestionably transformed outcomes. However, in day-to-day practice, a recurring pattern emerges: patients with “acceptable” LDL-C who nevertheless progress to premature atherosclerotic cardiovascular disease. This clinical discordance is not anecdotal—it reflects a limitation in what LDL-C actually captures.
ApoB offers a more physiologically aligned lens. Atherosclerosis is fundamentally a particle-driven process, where each ApoB-containing lipoprotein has the potential to enter and become retained within the arterial wall. In this context, measuring the number of atherogenic particles—rather than their cholesterol content—provides a closer approximation of cumulative vascular exposure. This distinction becomes particularly relevant in patients with insulin resistance, hypertriglyceridaemia, or central adiposity, where LDL-C may underestimate true risk.
From a practical standpoint, ApoB is not a replacement for the lipid panel, but a refinement tool—especially valuable in cases of suspected discordance or residual risk. It integrates seamlessly into existing workflows, does not require fasting, and can meaningfully influence treatment thresholds and intensity.
That said, clinical judgment remains paramount. Not every patient requires ApoB testing, and resource considerations must be acknowledged across different healthcare settings. However, for metabolically complex patients—the very population driving the global burden of cardiometabolic disease—ApoB provides clarity where traditional markers may fall short.
Incorporating ApoB into routine risk assessment is less about abandoning LDL-C and more about advancing precision in preventive cardiology.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Atherogenic Dyslipidemia Explained: The Role of ApoB in Hidden Cardiovascular Risk
Remnant Cholesterol: The Hidden Link Between Insulin Resistance, Type 2 Diabetes, and Heart Disease
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
Why Belly Fat Causes Insulin Resistance: Portal Theory Explained Simply
The Role of Cholesterol in Health and Disease: Beyond the "Bad" Label | DR T S DIDWAL
Lowering Cholesterol with Food: 4 Phases of Dietary Dyslipidemia Treatment | DR T S DIDWAL
References
De Oliveira-Gomes, D., Joshi, P. H., Peterson, E. D., Rohatgi, A., Khera, A., & Navar, A. M. (2024). Apolipoprotein B: Bridging the gap between evidence and clinical practice. Circulation, 150(1), 62–79. https://doi.org/10.1161/CIRCULATIONAHA.124.068885
Galimberti, F., Casula, M., & Olmastroni, E. (2023). Apolipoprotein B compared with low-density lipoprotein cholesterol in the atherosclerotic cardiovascular diseases risk assessment. Pharmacological Research, 195, Article 106873. https://doi.org/10.1016/j.phrs.2023.106873
Genedy, N., & Zouwail, S. (2025). ApoB/LDL-C discordance as a predictor of atherosclerotic cardiovascular disease in genetically confirmed heterozygous familial hypercholesterolemia: A hypothesis-generating cohort study. Journal of Clinical Lipidology. Advance online publication. https://doi.org/10.1016/j.jacl.2025.11.008
Mortensen, M. B. (2024). ApoB triumphs once more over LDL-C and non-HDL-C in risk prediction: Ready for guidelines? European Heart Journal, 45(27), 2419–2421. https://doi.org/10.1093/eurheartj/ehae257
Tsimikas, S., & Bittner, V. (2024). Particle number and characteristics of lipoprotein(a), LDL, and ApoB: Perspectives on contributions to ASCVD. Journal of the American College of Cardiology, 83(3), 396–400. https://doi.org/10.1016/j.jacc.2023.11.008
Blumenthal, R. S., Morris, P. B., Gaudino, M., Johnson, H. M., Anderson,, J. J., Shapiro, & Wilkins, J. T. (2026). 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of dyslipidemia: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology. Advance online publication. https://doi.org/10.1016/j.jacc.2025.11.016