Remnant Cholesterol: The Hidden Link Between Insulin Resistance, Type 2 Diabetes, and Heart Disease
Remnant cholesterol is a hidden cause of heart disease risk—even with normal LDL. Learn how it drives atherosclerosis and how to reduce it.
HEARTMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/2/202626 min read
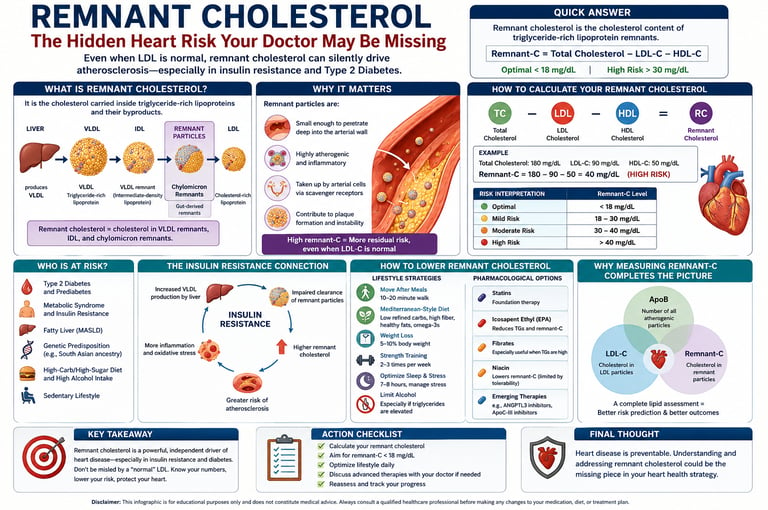
Remnant cholesterol is the cholesterol carried within triglyceride-rich lipoprotein remnants, including VLDL remnants, IDL, and chylomicron remnants. Elevated remnant cholesterol is increasingly recognized as an independent risk factor for cardiovascular disease because these particles can directly enter artery walls and promote plaque formation. It is calculated as Total Cholesterol − LDL-C − HDL-C and is often elevated in insulin resistance and Type 2 Diabetes.
Why Does Remnant Cholesterol Matter?
Can promote atherosclerosis even when LDL is normal
Commonly elevated in insulin resistance and Type 2 Diabetes
Contributes to residual cardiovascular risk
Reflects cholesterol in VLDL remnants, IDL, and chylomicron remnants
Can be calculated from a standard lipid panel
May identify hidden heart disease risk missed by LDL-C alone
Who Should Check Remnant Cholesterol?" Box
Potential candidates:
Type 2 diabetes
Prediabetes
Metabolic syndrome
NAFLD/MASLD
Elevated triglycerides
South Asians
Premature coronary disease
Why Your "Normal" Cholesterol May Not Protect You
Getting a lipid panel back that says “LDL: normal” feels like a win. You’ve eaten better, maybe lost some weight, and your doctor nods approvingly. But here’s the part that rarely gets said in a 10-minute visit: normal LDL doesn’t always mean your arteries are safe.
The missing piece is remnant cholesterol — the cholesterol tucked inside leftover particles from fat digestion. You can calculate it yourself: `Total Cholesterol − LDL-C − HDL-C`. If it’s above 30 mg/dL, your heart risk goes up, even if LDL looks perfect.
Why does it matter? Remnant particles slip into artery walls without needing to be oxidized first. That means they turn into plaque faster than LDL. And they hang around much longer after meals if you have insulin resistance, belly fat, or Type 2 Diabetes. So while you’re fasting for your lab test, your arteries may be exposed to high remnant levels for 12–16 hours a day.
This isn’t rare. In people with diabetes, remnant-C stays high even when blood sugar is controlled. It’s also why someone with an LDL of 82 can still have progressive plaque.
The good news: you can act. Cut back on refined carbs, walk 15 minutes after meals to activate muscle clearance, and shrink visceral fat. If remnant-C stays >30 mg/dL, ask your doctor about ApoB testing, fibrates, or prescription EPA.
Bottom line: LDL is only one chapter. If you have triglycerides >150, low HDL, or a waist >90 cm (men) / >80 cm (women), calculate your remnant-C today. It takes 10 seconds and could change your entire prevention plan.
Your heart deserves the full picture, not just the headline number. Talk to your clinician about your complete lipid risk — you might catch the danger hiding in plain sight.
What Is Remnant Cholesterol?
Most people know the cholesterol story in two acts: LDL ("bad") and HDL ("good"). But this binary misses a third, highly atherogenic chapter: remnant cholesterol.
Remnant cholesterol (remnant-C) refers to the cholesterol content inside triglyceride-rich lipoproteins and their metabolic byproducts, specifically:
VLDL remnants — lipoproteins produced by the liver that become progressively enriched with cholesterol as their triglyceride cargo is burned off during circulation
Intermediate-density lipoprotein (IDL) — a transitional particle sitting between VLDL and LDL, and distinctly atherogenic in its own right
Chylomicron remnants — gut-derived particles formed after dietary fat absorption, which accumulate in the bloodstream for hours after every meal, especially in insulin-resistant individuals
These are not hypothetical particles. They circulate in your blood every day, and in people with certain metabolic profiles, they accumulate to levels that directly injure artery walls.
How Remnant Cholesterol Fits Into the Lipid Picture
Understanding remnant cholesterol requires zooming out from LDL to see the full landscape of atherogenic lipids:
LDL-C (Low-Density Lipoprotein Cholesterol)
What it measures: The total mass (weight) of cholesterol carried specifically inside LDL particles.
Clinical role: This is the standard, primary target in medical guidelines. It plays a direct, causal role in building up plaque in the arteries (ASCVD
).
Non-HDL-C (Non-High-Density Lipoprotein Cholesterol)
What it measures: The total cholesterol mass found across all plaque-causing (atherogenic) lipoproteins combined.
Clinical role: A more powerful predictor of risk than traditional LDL-C, particularly for individuals dealing with metabolic disease or insulin resistance.
ApoB (Apolipoprotein B)
What it measures: The total number of plaque-causing particles. Because every single bad lipoprotein particle carries exactly one ApoB protein molecule, counting ApoB equals counting the particles.
Clinical role: The single best marker for understanding your total particle burden, capturing risk that standard cholesterol mass tests sometimes miss.
Remnant-C (Remnant Cholesterol)
What it measures: The specific cholesterol content trapped inside the leftover remnants of triglyceride-rich lipoproteins (TRLs).
Clinical role: A critical driver of "residual risk"—the heart risk that remains high even after you successfully lower your LDL-C, especially common in Type 2 diabetes and obesity.
Triglycerides
What it measures: The actual amount of fat (triglycerides) packed inside those triglyceride-rich lipoproteins.
Clinical role: Serves as a surrogate marker; a high number is a major red flag reflecting a heavy, overworked lipoprotein burden.
Each of these markers captures a different dimension of risk. Measuring only LDL is like checking only one room for a gas leak.
How to Calculate Your Remnant Cholesterol
One of the most practical aspects of remnant cholesterol assessment is that you already have the data you need — it is embedded in your standard lipid panel.
The Simple Formula
Remnant-C = Total Cholesterol − LDL-C − HDL-C
Example:
Total Cholesterol: 210 mg/dL
LDL-C: 110 mg/dL
HDL-C: 55 mg/dL
Remnant-C = 210 − 110 − 55 = 45 mg/dL ← Elevated
What Do the Numbers Mean?
Here is the breakdown of Remnant Cholesterol (Remnant-C) reference ranges rewritten into a structured formatting layout, making it much easier to interpret at a glance.
Optimal: Under 17–18 mg/dL
Interpretation: Excellent. Indicates low levels of residual triglyceride-rich remnants, minimizing this specific driver of arterial plaque buildup.
Borderline: 18–30 mg/dL
Interpretation: Watchful zone. Monitor this closely alongside other metabolic markers like fasting glucose, A1c, and waist circumference to watch for early signs of insulin resistance.
Elevated: Greater than 30 mg/dL
Interpretation: Meaningful increase in cardiovascular (ASCVD) risk. Remnants at this level are actively contributing to plaque formation, even if your standard LDL-C looks normal.
Significantly Elevated: Greater than 40 mg/dL
Interpretation: High risk. This tier strongly warrants a deeper clinical investigation and targeted intervention (such as intensive dietary changes, weight management, or medical therapy) to protect your arteries.
Why Remnant-C Matters: Remnant cholesterol particles are highly atherogenic (plaque-forming). Because they are large and packed with triglycerides, they can easily get trapped in the artery walls, triggering inflammation and accelerating heart disease independently of standard LDL levels
Important caveat: This calculation relies on accurate LDL-C measurement. It becomes less reliable when fasting triglycerides exceed 400 mg/dL, or in non-fasting samples. In complex cases, direct lipoprotein analysis (such as NMR spectroscopy) provides greater precision.
Your 3-Step Self-Assessment
Get a fasting lipid panel (standard blood test, available through your GP)
Apply the formula: Total Cholesterol − LDL-C − HDL-C
Flag for your doctor if: Remnant-C > 25 mg/dL AND you have triglycerides > 150 mg/dL, central obesity, or Type 2 Diabetes
Why Remnant Cholesterol Damages Arteries
Not all cholesterol-carrying particles are equally dangerous. What makes remnant lipoproteins distinctly harmful is a combination of their physical size, their cholesterol density, and — most critically — their behavior once they enter the arterial wall.
They Don't Need a "Trigger" to Cause Damage
Here is the key biological distinction that separates remnant cholesterol from LDL:
LDL particles must undergo oxidative modification before macrophages (immune cells patrolling the arterial wall) will engulf them. This oxidation step acts as a partial rate-limiter on atherosclerosis.
Remnant particles bypass this step entirely. Chylomicron remnants and VLDL remnants are taken up directly by arterial macrophages — no oxidation required. This means foam cell formation (the hallmark early lesion of atherosclerosis) proceeds faster and more efficiently with remnant particles than with LDL.
A landmark 2024 cohort study by Wadström et al., published in Arteriosclerosis, Thrombosis, and Vascular Biology, demonstrated that remnant cholesterol — not LDL-C — explained the peripheral artery disease risk associated with elevated ApoB levels. In other words, even when total atherogenic particle burden rises, it is the remnant fraction doing the vascular damage in peripheral arteries.
They Deliver More Cholesterol Per Particle
Each remnant particle carries substantially more cholesterol than a single LDL particle. As Baratta et al. (2023) highlight in the International Journal of Molecular Sciences, this amplifies the atherogenic signal considerably — fewer particles can deposit more cholesterol in the arterial wall.
They Trigger Vascular Inflammation
Beyond direct cholesterol deposition, remnant particles set off a cascade of vascular injury:
Endothelial dysfunction and reduced nitric oxide production
Release of pro-inflammatory cytokines (IL-6, TNF-α)
Activation of coagulation pathways
Increased arterial wall permeability
The ApoB Paradox Explained
Marotzmann et al. (2024) showed that the relationship between ApoB, LDL-C, and cardiovascular events differs meaningfully between patients with and without diabetes — precisely because insulin resistance alters the composition of circulating atherogenic particles. When metabolic dysfunction is present, remnant particles make up a larger fraction of total ApoB-carrying lipoproteins, meaning standard LDL assessment increasingly underestimates true risk.
The Insulin Resistance–Remnant Cholesterol Connection
If you want to understand why remnant cholesterol is so elevated in metabolic disease, you need to understand how insulin resistance rewires lipoprotein metabolism from the inside out. The relationship is not coincidental — it is mechanistic, bidirectional, and self-reinforcing.
Step 1: The Liver Overproduces VLDL
In states of insulin resistance, the liver loses its ability to suppress de novo lipogenesis appropriately. Elevated free fatty acid flux — driven by unrestrained lipolysis in visceral adipose tissue — floods the liver with raw material, driving overproduction of large, triglyceride-rich VLDL particles. Counterintuitively, hyperinsulinemia (high circulating insulin) promotes VLDL assembly and secretion even while peripheral tissues stop responding to insulin's signals.
Step 2: Clearance Mechanisms Break Down
Simultaneously, the enzyme responsible for clearing TRLs from circulation — lipoprotein lipase (LPL) — is increasingly inhibited. The culprit is ApoC-III, a protein that rises sharply in insulin-resistant states and directly blocks LPL activity.
Hepatic remnant clearance also falters. The LDL receptor-related protein (LRP1) and the LDL receptor itself become less efficient at capturing circulating remnants for degradation. The result: remnant particles linger in circulation far longer than they should, vastly extending their window of opportunity to penetrate artery walls.
Step 3: The Vicious Cycle Closes
Here is where the feedback loop becomes especially concerning. Elevated circulating remnants deposit ectopic fat in the liver, skeletal muscle, and pancreas. This ectopic lipid accumulation directly worsens insulin signaling — completing a vicious cycle where insulin resistance generates remnant excess, which in turn deepens insulin resistance.
A comprehensive 2026 narrative review by Natsir et al. in Therapeutics and Clinical Risk Management delineates this pathophysiology rigorously, establishing remnant cholesterol as an independent atherogenic lipoprotein in Type 2 Diabetes — not merely a proxy for elevated triglycerides.
Remnant Cholesterol and Type 2 Diabetes
For people living with Type 2 Diabetes, remnant cholesterol is not a secondary concern — it is arguably the central driver of their excess cardiovascular risk.
Why HbA1c Control Is Not Enough
One of the most important — and most underappreciated — clinical findings in this field is that remnant cholesterol remains elevated despite glycemic control. A patient can achieve a target HbA1c of 6.5–7.0% and still have a dangerously high remnant particle burden.
This explains a frustrating clinical reality: many patients with well-controlled diabetes continue to experience cardiovascular events. They are not failing treatment — they are receiving incomplete treatment.
As Natsir et al. (2026) emphasize, lipotoxicity persists independent of glucose normalization. Treating glucose without addressing atherogenic dyslipidemia is like fixing a roof leak without repairing the underlying structural damage.
The "Double Hit" in Type 2 Diabetes
People with T2DM experience a particularly severe post-meal vascular assault. After eating, two damaging processes occur simultaneously:
Postprandial hyperglycemia — glucose spikes reduce nitric oxide availability in blood vessel walls
Postprandial hyperlipidemia — remnant particles deliver cholesterol to already-inflamed endothelium
Each insult is harmful alone. Together, their combined effect on endothelial function is worse than either in isolation — a mechanism researchers have termed the "double hit" hypothesis. The clinical consequence is accelerated early atherosclerosis even in patients who appear well-controlled on standard metrics.
The LDL Illusion in Diabetes
In patients with atherogenic dyslipidemia, an unexpected artifact distorts standard lipid assessment. When triglycerides are elevated, triglyceride-rich particles exchange lipids with LDL, resulting in smaller, cholesterol-depleted LDL particles and an apparent lowering of measured LDL-C. The LDL number looks better. The actual atherogenic burden is worse.
This "LDL illusion" means that in metabolic disease specifically, LDL-C can actively mislead clinical decision-making.
The Postprandial Trap: Risk Between Your Meals
Here is a fact that reframes how we should think about cardiovascular risk: most people spend fewer than 8 hours per day in a true fasting state. After every fat-containing meal, the gut floods the bloodstream with chylomicrons — large, triglyceride-rich particles that are progressively metabolized into cholesterol-enriched remnants.
In healthy individuals, this postprandial lipemia clears within 4–6 hours.
In people with insulin resistance or Type 2 Diabetes, the same broken clearance machinery that prolongs VLDL remnant circulation also fails to efficiently clear chylomicron remnants. The result is a state of chronic postprandial lipemia — a persistent, meal-to-meal elevation of remnant particles that the arterial wall is exposed to for the majority of every waking day.
Why Fasting Lipid Panels Miss the Problem
Standard lipid panels are drawn in the fasting state for methodological reasons — but this creates a significant blind spot. A patient with fasting triglycerides of 160 mg/dL may have postprandial triglycerides exceeding 400–500 mg/dL for 8–10 hours after each meal. Their fasting panel looks merely "borderline." Their real daily vascular exposure is severe.
Non-fasting triglyceride measurements — increasingly recommended by European cardiovascular guidelines — capture this dynamic burden more accurately and have demonstrated stronger associations with ASCVD events than fasting measurements in several large population studies.
A 2024 Mendelian randomization study by Zhao et al. in Nature Communications provided compelling causal evidence that both elevated remnant cholesterol and elevated triglycerides independently drive cardiometabolic multimorbidity — strengthening the case that these are not just biomarkers, but active pathological agents.
Atherogenic Dyslipidemia: The Metabolic Triad
Remnant cholesterol does not exist in isolation. It is typically accompanied by a characteristic lipid pattern called atherogenic dyslipidemia — a triad that is extremely common in metabolic syndrome, Type 2 Diabetes, and central obesity, yet frequently missed by standard lipid assessment.
The Three Components
1. Elevated Triglycerides (≥ 150 mg/dL) Reflects increased triglyceride-rich lipoprotein burden. Directly associated with higher remnant particle exposure.
2. Low HDL Cholesterol Below 40 mg/dL in men, below 50 mg/dL in women. Indicates impaired reverse cholesterol transport and reduced vascular protection.
3. Small Dense LDL Particles More susceptible to oxidation, capable of greater arterial wall penetration, and more atherogenic per particle than large buoyant LDL — despite being captured in the same LDL-C number on a standard panel.
Why This Pattern Is Clinically Dangerous
The metabolic triad typically coexists with a normal or low LDL-C — which creates a false sense of security. Standard panels focus primarily on LDL-C, HDL-C, and total cholesterol. When these appear acceptable, clinicians and patients may conclude that lipid-related risk is managed. In reality, significant atherogenic burden may be hidden in an elevated remnant fraction.
A practical screening tool: if a patient has triglycerides above 150 mg/dL and low HDL, calculate their remnant-C immediately. A result above 25–30 mg/dL warrants serious clinical attention, regardless of LDL.
How to Assess Your Full Lipid Risk
Tier 1: Core Markers (Available on Any Standard Lipid Panel)
Fasting Triglycerides
How it is calculated: Direct laboratory measurement.
Clinical target: $< 150\text{ mg/dL}$.
Clinical role: Key indicator of the total burden of Triglyceride-Rich Lipoproteins (TRLs).
Non-HDL Cholesterol
How it is calculated: $\text{Total Cholesterol} - \text{HDL-C}$.
Clinical target: $< 130\text{ mg/dL}$ for the general population.
Clinical role: Measures the absolute total amount of cholesterol carried across all plaque-causing (Atherogenic) particles.
Remnant Cholesterol (Remnant-C)
How it is calculated: $\text{Total Cholesterol} - \text{LDL-C} - \text{HDL-C}$.
Clinical target: $< 17\text{--}18\text{ mg/dL}$ is considered optimal.
Clinical role: Pinpoints the specific cardiovascular risk driven by leftover TRL remnants.
TG/HDL Ratio
How it is calculated: $\text{Triglycerides} \div \text{HDL-C}$.
Clinical target: $< 3.0$ (lower is better).
Clinical role: Serves as a reliable, highly accessible surrogate marker for underlying insulin resistance.
Tier 2: Advanced Markers (Widely Available Add-On Tests)
Apolipoprotein B (ApoB)
What it measures: The literal count of all atherogenic particles.
Why it matters: Far superior to standard LDL-C for determining true particle burden, especially when particle sizes vary.
Fasting Insulin / HOMA-IR
What it measures: The severity of a patient's insulin resistance.
Why it matters: Evaluates the primary metabolic driver that causes remnant cholesterol to spike in the first place.
Lipoprotein(a) [Lp(a)]
What it measures: An independent, highly inflammatory lipoprotein particle.
Why it matters: Driven entirely by genetics, checking it at least once in a lifetime ensures a hidden, high-risk factor isn't missed.
Tier 3: Specialized Markers (Advanced/Niche Testing)
NMR Lipoprotein Analysis
What it shows: The exact number and physical size distribution of all lipoprotein fractions.
When to consider: Complex cases, patients with high triglycerides, or when there is a major mismatch (discordance) between a patient's ApoB and LDL-C levels.
Apolipoprotein C-III (ApoC-III)
What it shows: Levels of the protein that inhibits Lipoprotein Lipase (LPL), which rise during insulin resistance.
When to consider: For diagnosing and evaluating severe defects in how a patient clears TRLs from their blood.
Non-Fasting Lipid Panel
What it shows: Real-world, post-meal (postprandial) lipid and fat exposure.
When to consider: When you strongly suspect a patient experiences prolonged spikes in lipids after eating, despite normal fasting numbers
.
2026 Clinical Guideline Summary
Primary Targets: The 2026 ACC/AHA Dyslipidemia Guidelines continue to prioritize LDL-C and Non-HDL-C as the gold-standard primary treatment targets.
The Role of ApoB: Earns a solid Class IIa recommendation. It is heavily relied upon to uncover hidden cardiovascular risk in patients with Type 2 diabetes, elevated triglycerides ($> 200\text{ mg/dL}$), or those who have successfully hit low LDL-C targets but still suffer cardiac events.
The Role of Remnant-C: Does not currently hold a formal, primary treatment target in major guidelines, but is highly recognized as a valuable tool to guide clinical judgment and paint a complete metabolic picture
Evidence Summary: Key Studies at a Glance
Here is the recent scientific data on Remnant Cholesterol (Remnant-C)
2023
Baratta et al., 2023 (Int J Mol Sci)
Study Population: Review of Triglyceride-Rich Lipoprotein (TRL) data.
Key Finding: Remnant-C is causally linked to atherosclerotic cardiovascular disease (ASCVD). Unlike standard LDL, remnants can undergo direct uptake by macrophages without needing to be oxidized first.
2024
Wadström et al., 2024 (ATVB)
Study Population: Large Danish cohort.
Key Finding: Remnant-C—not LDL-C—is the specific marker that explains the Peripheral Artery Disease (PAD) risk conferred by elevated ApoB levels.
Marotzmann et al., 2024 (Atherosclerosis)
Study Population: Patients with and without Type 2 Diabetes (T2DM).
Key Finding: The standard association between ApoB and cardiovascular disease differs significantly between diabetic and non-diabetic populations.
Zhao et al., 2024 (Nature Communications)
Study Population: Mendelian randomization study of a large cohort.
Key Finding: Elevated Remnant-C and Triglycerides (TG) causally drive the development of cardiometabolic multimorbidity.
2025
Doi et al., 2025 (Curr Atheroscler Rep)
Study Population: Literature review.
Key Finding: Remnant-C shows a potent association with ASCVD; this residual cardiovascular risk persists aggressively even after successful LDL-C lowering therapy.
Journal of AHA, 2025 (JAHA.125.045376)
Study Population: Prospective cohort study.
Key Finding: Strongly reinforces the independent association between elevated Remnant-C and Major Adverse Cardiovascular Events (MACE).
2026
Natsir et al., 2026 (TCRM)
Study Population: Narrative review focusing on Type 2 Diabetes (T2DM).
Key Finding: Remnant-C acts as an independent atherogenic (plaque-forming) lipoprotein in T2DM patients, persisting stubbornly despite optimal glycemic (blood sugar) control.
Wulff et al., 2026 (Expert Opin Ther Targets)
Study Population: Clinical feasibility review.
Key Finding: Remnant-C is highly feasible as a direct therapeutic target; emerging pipeline drugs are showing strong clinical promise.
Feng et al., 2026 (Front Endocrinol)
Study Population: Cross-sectional study of middle-aged and older men.
Key Finding: Elevated Remnant-C-based lipid indicators are significantly associated with testosterone deficiency.
Zhang et al., 2026 (Diabetol Metab Syndr)
Study Population: Longitudinal data from the China Health and Retirement Longitudinal Study (CHARLS).
Key Finding: High Remnant-C levels are closely associated with a greater risk of developing new-onset chronic diseases, specifically diabetes and CVD.
Atherosclerosis, 2026 (DOI:10.1016/j.atherosclerosis.2026.120755)
Study Population: Clinical study.
Key Finding: Adds further weight to the growing clinical consensus supporting Remnant-C as an independent vascular risk driver.
How to Lower Remnant Cholesterol: Lifestyle Strategies
The good news: remnant cholesterol is highly responsive to lifestyle change — often more dramatically and rapidly than LDL-C. Here are the evidence-based strategies, ranked by impact.
1. Cut Refined Carbohydrates First (Not Just Fat)
This surprises many people. Dietary fat directly elevates chylomicrons post-meal, but refined carbohydrates chronically drive hepatic VLDL overproduction and raise fasting triglycerides.
Swapping white rice, bread, sugar-sweetened beverages, and processed snacks for whole grains, legumes, vegetables, and low-glycemic alternatives can reduce fasting triglycerides by 20–40% within 4–8 weeks — without any medication.
Nutritional patterns consistently shown to lower remnant-C include:
Low-glycemic index diets
Mediterranean-style eating (olive oil, vegetables, fish, legumes)
Very-low-carbohydrate / ketogenic diets (particularly effective for severe hypertriglyceridemia)
2. Take a 15-Minute Walk After Meals
This is one of the highest-impact, lowest-cost interventions available, and it is dramatically underutilized.
The mechanism: Skeletal muscle is the primary site of lipoprotein lipase (LPL) activity — the enzyme that clears triglyceride-rich remnants from the blood. A single session of moderate-intensity movement activates muscle LPL for up to 12–24 hours, dramatically blunting the postprandial triglyceride spike that follows a meal.
Even gentle walking for 15 minutes after eating has been shown to meaningfully reduce postprandial lipemia. For people with insulin resistance, this simple habit addresses one of the core physiological defects driving remnant accumulation.
3. Reduce Visceral Fat Specifically
Waist circumference is a powerful surrogate for remnant cholesterol burden. In South Asian populations (including Indian individuals), clinically significant visceral obesity begins at:
Waist ≥ 90 cm in men
Waist ≥ 80 cm in women
Visceral fat reduction — through caloric deficit, resistance training, and dietary quality improvement — enhances LPL activity, decreases hepatic VLDL production, and improves insulin sensitivity simultaneously. A 5–10% reduction in body weight can produce striking improvements in the full atherogenic dyslipidemia triad.
4. Implement Time-Restricted Eating
Eating within an 8–10-hour window (time-restricted eating, or TRE) reduces total daily remnant particle exposure time by naturally extending the overnight fast. It also improves insulin sensitivity independently of caloric restriction in several clinical trials. For someone who typically eats from 7 AM to 9 PM — a 14-hour eating window — compressing this to 10 AM to 6 PM meaningfully reduces the hours spent in a high-remnant postprandial state.
5. Add Resistance Training
Beyond aerobic exercise, resistance training (weight lifting, bodyweight exercises) increases total skeletal muscle mass — which permanently expands the body's LPL "capacity." More muscle mass means greater clearance of triglyceride-rich particles with every meal and every bout of activity.
6. Prioritize Sleep and Stress Management
Chronic sleep deprivation and psychological stress elevate cortisol and promote visceral fat accumulation, worsening insulin resistance and driving remnant overproduction. Seven to nine hours of quality sleep per night is not a luxury for cardiometabolic health — it is a biological requirement.
Pharmacological Options
When lifestyle changes are insufficient — or when remnant-C remains elevated despite optimal effort — pharmacological intervention is warranted. Options span from established therapies to exciting emerging drugs.
Statins: Effective for LDL, Limited for Remnants
Statins are the cornerstone of lipid-lowering therapy and remain the best-evidenced pharmacological intervention for ASCVD prevention. They primarily lower LDL-C by upregulating hepatic LDL receptor expression.
However, these same receptors also clear IDL and VLDL remnants, so statins do modestly reduce remnant cholesterol. The limitation: statin monotherapy often leaves substantial residual remnant burden in patients with atherogenic dyslipidemia. They are necessary but frequently insufficient in this population.
Fibrates: Targeted Triglyceride/Remnant Lowering
Fibrates (e.g., fenofibrate, bezafibrate) activate PPARα, a nuclear receptor that:
Upregulates LPL expression → accelerates TRL clearance
Reduces ApoC-III production → removes the LPL brake
Increases HDL cholesterol
Result: triglyceride reductions of 30–50%, with meaningful improvements in remnant-C. Fibrates are particularly valuable in patients with the metabolic triad (high TG, low HDL, normal LDL). Clinical guidelines support their use in combination with statins when TG remain elevated.
Prescription Omega-3s (EPA / Icosapent Ethyl)
High-dose prescription omega-3 fatty acids, specifically icosapent ethyl (Vascepa) — a purified EPA formulation — have demonstrated cardiovascular benefit beyond triglyceride lowering in the landmark REDUCE-IT trial. The mechanisms extend to anti-inflammatory, anti-thrombotic, and membrane-stabilizing effects on remnant-burdened endothelium. Effects include:
TG reduction of 20–30%
Significant reduction in major adverse cardiovascular events in high-risk patients
Note: standard fish oil supplements have not demonstrated the same cardiovascular benefit and are not equivalent to prescription-grade icosapent ethyl.
Emerging Therapies: The Exciting Frontier
ApoC-III inhibitors (volanesorsen, olezarumab/AKCEA-APOCIII-LRx) dramatically reduce the inhibition of LPL, producing TG reductions of 70–80% in patients with severe hypertriglyceridemia and familial chylomicronemia syndrome. They represent a mechanistically precise attack on the impaired clearance pathway that underlies remnant accumulation.
ANGPTL3 inhibitors (evinacumab) block angiopoietin-like protein 3, a key regulator of LPL and endothelial lipase activity. They achieve remarkable remnant particle lowering even in patients with genetic LDL receptor deficiency — a setting where conventional lipid therapies have limited effect on TRL metabolism.
As reviewed by Wulff et al. (2026) in Expert Opinion on Therapeutic Targets, remnant cholesterol is increasingly being considered as a feasible therapeutic target in its own right — not merely a secondary consideration.
Here is a streamlined, highly scannable breakdown of therapies targeting Triglycerides (TG) and Remnant Cholesterol, organized from standard foundational therapies to emerging cutting-edge treatments.
Established Foundational Therapies
Statins
Primary Mechanism: Increases LDL receptor expression on the liver.
TG Reduction: Modest ($10\text{--}20\%$).
Remnant-C Impact: Mild to moderate.
Clinical Status: Standard of care / fully established.
Fibrates
Primary Mechanism: Activates PPAR$\alpha$ (peroxisome proliferator-activated receptor alpha), which increases LPL (lipoprotein lipase) activity and decreases ApoC-III.
TG Reduction: Robust
Remnant-C Impact: Moderate to significant.
Clinical Status: Well-established.
Icosapent Ethyl (Pure EPA)
Primary Mechanism: Utilizes multiple anti-inflammatory, antioxidant, and plaque-stabilising pathways.
TG Reduction: Meaningful
Remnant-C Impact: Moderate.
Clinical Status: Established prescription therapy (frequently used for managing residual risk).
Advanced & Emerging Pipeline Therapies
ApoC-III Inhibitors
Primary Mechanism: Removes the biological "brake" on Lipoprotein Lipase (LPL), rapidly accelerating the body's ability to clear TRLs (triglyceride-rich lipoproteins) from the blood.
TG Reduction: Massive
Remnant-C Impact: Exceptionally high.
Clinical Status: Emerging breakthrough.
ANGPTL3 Inhibitors
Primary Mechanism: Increases both LPL and endothelial lipase activity by blocking angiopoietin-like 3 proteins.
TG Reduction: Potent.
Remnant-C Impact: High.
Clinical Status: Emerging / newly approved for specific high-risk genetic populations.
Common Myths and Mistakes
❌ Myth 1: "My LDL is fine, so my cholesterol is fine."
Reality: LDL-C is one dimension of atherogenic risk, not the complete picture. In patients with insulin resistance, metabolic syndrome, or elevated triglycerides, the atherogenic burden is substantially driven by remnant particles — which LDL-C does not capture. A patient can have an LDL of 70 mg/dL and a remnant-C of 50 mg/dL simultaneously.
❌ Myth 2: "Triglycerides are just a fuel marker, not a risk marker."
Reality: Triglycerides are a measure of TRL burden in the bloodstream. Elevated triglycerides directly reflect more remnant particle exposure to the arterial wall. Multiple Mendelian randomization studies confirm that elevated triglycerides causally increase cardiovascular risk — they are not merely a bystander.
❌ Myth 3: "My HbA1c is controlled, so my cardiovascular risk is controlled."
Reality: Glycemic control and lipid control are partially independent. Remnant cholesterol remains elevated in many patients with well-controlled HbA1c. Natsir et al. (2026) explicitly document that lipotoxicity — the cellular damage from excess lipid — persists independent of glucose normalization.
❌ Myth 4: "Eating fat causes high triglycerides and remnant cholesterol."
Reality: Dietary fat acutely raises chylomicrons post-meal, but the primary chronic driver of elevated fasting triglycerides and VLDL overproduction is excess refined carbohydrates and sugar — not dietary fat per se. For most people with atherogenic dyslipidemia, reducing carbohydrates is more impactful than reducing fat.
❌ Myth 5: "Fish oil supplements will fix this."
Reality: Over-the-counter fish oil supplements have not demonstrated consistent cardiovascular benefit in clinical trials. The cardiovascular benefit seen with icosapent ethyl (purified EPA) in REDUCE-IT appears to be product-specific and dose-specific. Standard fish oil supplements are not a reliable substitute.
❌ Myth 6: "This is only relevant for people with very high triglycerides."
Reality: Remnant cholesterol can be clinically elevated even with triglycerides in the 150–199 mg/dL range — a level often described as "borderline" and dismissed. In the context of other metabolic risk factors, borderline triglycerides with elevated remnant-C carry meaningful risk that warrants attention.
FAQs
1. What is remnant cholesterol in simple terms?
Remnant cholesterol is the cholesterol carried inside partially broken-down fat-transporting particles in your blood. Think of these particles as delivery trucks: they start out full of fat (triglycerides), and as the fat gets used up, the leftover "cargo" — the cholesterol — becomes proportionally more concentrated. These cholesterol-laden remnant trucks can directly clog your artery walls without needing any additional trigger.
2. What is a normal remnant cholesterol level?
Optimal remnant cholesterol is below 17–18 mg/dL. Levels above 30 mg/dL are associated with meaningfully increased cardiovascular risk, particularly in people with Type 2 Diabetes or metabolic syndrome. Calculate it from your standard lipid panel: Total Cholesterol − LDL-C − HDL-C.
3. Can you have high remnant cholesterol with normal LDL?
Yes — and this is precisely why remnant cholesterol matters. In patients with insulin resistance, atherogenic dyslipidemia can drive high remnant-C while LDL-C appears controlled or even low. This is the core of "residual cardiovascular risk" — ongoing vascular injury despite apparent LDL management.
4. How quickly can lifestyle changes lower remnant cholesterol?
Significant improvements in fasting triglycerides (a primary driver of remnant-C) can occur within 4–8 weeks of reducing refined carbohydrate intake, increasing physical activity, and reducing body weight. Postprandial remnant burden can improve even faster — a single bout of exercise can measurably reduce postprandial lipemia for up to 24 hours.
5. Is remnant cholesterol the same as VLDL cholesterol?
They overlap significantly but are not identical. VLDL cholesterol is one component of remnant cholesterol (alongside IDL and chylomicron remnants). In practice, calculated remnant-C from a standard lipid panel includes all of these fractions together. Some laboratories report VLDL-C directly, which approximates one portion of remnant burden.
6. Does remnant cholesterol matter if I'm on a statin?
Yes. Statins effectively lower LDL-C but only modestly reduce remnant cholesterol. For patients with high triglycerides, low HDL, central obesity, or Type 2 Diabetes who remain on statin therapy with apparently controlled LDL, elevated remnant-C may explain persistent atherosclerosis progression. This is a key argument for adding fibrates, omega-3s, or newer therapies in selected patients.
7. How does diet affect remnant cholesterol?
Dietary quality affects remnant-C through multiple pathways. Refined carbohydrates and sugar drive hepatic VLDL overproduction, raising fasting remnant-C. Dietary fat composition affects post-meal (chylomicron) remnant burden. Weight gain — particularly visceral fat accumulation — worsens insulin resistance and impairs LPL-mediated clearance. A Mediterranean-style or low-glycemic diet addresses multiple pathways simultaneously.
8. Should non-fasting remnant cholesterol be tested?
Non-fasting lipid testing captures postprandial remnant burden — which more closely reflects the daily vascular exposure most people experience. Several European cardiovascular guidelines have moved toward recommending non-fasting lipid panels for this reason. Non-fasting triglycerides > 175 mg/dL are associated with increased cardiovascular risk independent of fasting values.
9. Is remnant cholesterol linked to testosterone levels?
Emerging research is exploring this connection. A 2026 cross-sectional study by Feng et al. in Frontiers in Endocrinology found that remnant cholesterol–based lipid indicators were associated with testosterone deficiency in middle-aged and older men. The mechanisms likely involve insulin resistance and metabolic dysfunction, which independently affect both lipid metabolism and androgen production. This is an active area of research.
10. What is the difference between remnant cholesterol and non-HDL cholesterol?
Non-HDL cholesterol = Total Cholesterol − HDL-C. It captures the cholesterol content of all atherogenic lipoproteins, including LDL, VLDL, IDL, and chylomicron remnants. Remnant cholesterol = Total-C − LDL-C − HDL-C. It captures only the TRL remnant fraction, excluding LDL-C. Remnant-C is a subset of non-HDL-C and provides additional information about TRL-specific burden beyond what LDL-C measures.
11. Can remnant cholesterol cause problems in people without diabetes?
Yes. While remnant cholesterol is particularly elevated in insulin resistance and Type 2 Diabetes, it is a causal risk factor for ASCVD in the general population. Genetic studies (Mendelian randomization) confirm that lifelong exposure to elevated remnant-C raises cardiovascular risk regardless of diabetes status. Familial hypertriglyceridemia, even without metabolic syndrome, can drive a significantly elevated remnant burden.
12. How does remnant cholesterol relate to the development of new chronic diseases?
A 2026 analysis of the CHARLS longitudinal study by Zhang et al. found that elevated remnant cholesterol was independently associated with the risk of developing new-onset chronic diseases, including cardiovascular disease and Type 2 Diabetes, over time — suggesting it is not only a consequence of metabolic disease but potentially a contributor to its progression.
13. If I Already Measure ApoB, Do I Still Need Remnant Cholesterol?
ApoB and remnant cholesterol provide complementary information rather than competing measurements.
In many patients, ApoB alone provides excellent risk assessment. However, remnant cholesterol can add valuable insight when triglycerides are elevated, insulin resistance is present, or cardiovascular risk appears disproportionately high despite acceptable LDL-C and ApoB levels. This is particularly relevant in people with Type 2 Diabetes, metabolic syndrome, MASLD, and South Asian populations.
ApoB remains the preferred marker for overall atherogenic particle burden, while remnant cholesterol helps uncover residual cardiometabolic risk related to triglyceride-rich lipoproteins. When available, the two markers are best viewed as complementary rather than interchangeable.
Action Checklist
Use this checklist at your next medical appointment and in the coming weeks:
At Your Next Lab Visit
[ ] Request a fasting lipid panel if you have not had one in the past 12 months
[ ] Calculate your Remnant-C: Total-C − LDL-C − HDL-C
[ ] Check your TG/HDL ratio (flag if > 3.0)
[ ] Ask about ApoB testing if your TG > 150 mg/dL or you have T2DM / metabolic syndrome
[ ] Measure your waist circumference (flag if ≥ 90 cm men / ≥ 80 cm women, South Asian)
Starting This Week
[ ] Replace one refined carbohydrate per day with a whole-food alternative
[ ] Add a 15-minute walk after your largest meal
[ ] Compress your eating window to 10–12 hours (time-restricted eating)
[ ] Track waist circumference monthly alongside body weight
If Remnant-C Is Above 30 mg/dL
[ ] Discuss with your doctor whether fibrates or omega-3s are appropriate
[ ] Request assessment for insulin resistance (fasting insulin, HOMA-IR)
[ ] Consider non-fasting lipid testing to capture postprandial burden
[ ] Review statin adequacy — statin alone may be insufficient
Always work with a qualified healthcare professional before making changes to medications or supplements. This checklist is a guide for informed conversation, not self-diagnosis.
Clinical pearls
1. The "Hidden Burden" Pearl
Scientific Perspective: LDL-C measures the cholesterol mass in LDL particles, but in insulin-resistant states, Remnant-C (the cholesterol in VLDL and IDL) represents a significant portion of the total ApoB-carrying (atherogenic) particles. Standard panels often miss this "residual risk."
"Your 'bad' cholesterol (LDL) might look like it’s in the safe zone, but there’s a second type of 'hidden' bad cholesterol called remnants. It’s like checking the front door of your house but leaving the back door wide open."
2. The "Fast-Track" Foam Cell Pearl
Scientific Perspective: Unlike LDL, which generally requires oxidative modification to be taken up by macrophages, remnant lipoproteins can be internalized directly. This bypasses a major rate-limiting step in foam cell formation and accelerates arterial wall damage.
"Standard bad cholesterol has to 'spoil' (oxidize) before it gets stuck in your arteries. Remnant cholesterol is more aggressive—it can start building up blockages immediately, without needing that extra step."
3. The "Muscle as a Sink" Pearl
Scientific Perspective: Skeletal muscle is the primary site for Lipoprotein Lipase (LPL) activity. Resistance training and postprandial movement upregulate LPL, which is the "master switch" for clearing triglyceride-rich remnants from the blood.
"Your muscles act like a vacuum cleaner for the fats in your blood. Every time you lift weights or take a short walk after a meal, you’re turning that vacuum on to clear out the particles that cause heart attacks."
4. The "Post-Meal Reality" Pearl
Scientific Perspective: Most humans spend 16+ hours a day in a postprandial (fed) state. Fasting lipid panels only capture a brief, "clean" window. Remnant levels post-meal are often a superior predictor of cardiovascular events because they reflect the body's actual daily toxic exposure.
"A fasting blood test is like checking your heart health while you’re resting on the couch. But your heart lives in the 'real world' where you eat several times a day. We need to care about what your blood looks like after you eat, not just when you’re hungry."
5. The "Fuel vs. Freight" Pearl
Scientific Perspective: Triglycerides are a measure of energy (fuel), but Remnant Cholesterol measures the actual cargo (cholesterol) left behind in the arterial wall. In Type 2 Diabetes, the "freight" stays in circulation too long because the "unloading docks" (hepatic receptors) are dysfunctional.
"Triglycerides are just the fuel your body burns for energy. The real danger is the 'cargo'—the cholesterol—that falls off the truck and gets stuck in your artery walls. In people with high blood sugar, those trucks are broken and stay on the road way too long."
Conclusion
Remnant cholesterol is not a niche lipid curiosity. It is a mechanistically validated, clinically actionable driver of cardiovascular risk — one that is systematically underdiagnosed because it does not appear in the headline numbers of a standard lipid panel.
The core message of two decades of evolving lipoprotein science is this: a normal LDL does not equal low cardiovascular risk, particularly in people with insulin resistance, metabolic syndrome, central obesity, or Type 2 Diabetes. For these patients, the true atherogenic villain may be hiding in the remnant fraction — and it is calculable from any standard blood test today.
The path forward is not to abandon LDL as a target — the evidence for LDL lowering remains robust and foundational. Rather, it is to expand the framework. Integrate triglycerides, non-HDL cholesterol, ApoB, and remnant cholesterol into a multi-dimensional picture of cardiometabolic risk. Target insulin resistance as an upstream driver, not just a comorbidity. And recognize that glycemic control, while essential, is insufficient for fully managing cardiovascular risk in Type 2 Diabetes.
The tools to act on this knowledge — from a post-meal walk to a calculated remnant-C from an existing lipid panel — are available right now. The question is whether the clinical conversation has caught up to the science.
Related Articles
GLP-1 Receptor Agonists and Cardiovascular Protection: Evidence from CVOT Trials Explained
ApoB vs LDL Cholesterol: Which Is the Most Accurate Predictor of Heart Disease?
Atherogenic Dyslipidemia Explained: The Role of ApoB in Hidden Cardiovascular Risk
Visceral Fat and Cardiovascular Risk: The Hidden Driver of Atherosclerosis
The #1 Diet Strategy to Reduce Visceral Fat According to Latest Research
References
Baratta, F., Cocomello, N., Coronati, M., Ferro, D., Pastori, D., Angelico, F., & Del Ben, M. (2023). Cholesterol remnants, triglyceride-rich lipoproteins and cardiovascular risk. International Journal of Molecular Sciences, 24(5), Article 4268. https://doi.org/10.3390/ijms24054268
Bhatt, D. L., Steg, P. G., Miller, M., Brinton, E. A., Jacobson, T. A., Ketchum, S. B., Doyle, R. T., Jr., Juliano, R. A., Jiao, L., Granowitz, C., Tardif, J.-C., & Ballantyne, C. M. (2019). Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. New England Journal of Medicine, 380(1), 11–22. https://doi.org/10.1056/NEJMoa1812792
Doi, T., Langsted, A., & Nordestgaard, B. G. (2025). Remnant cholesterol: Should it be a target for prevention of ASCVD? Current Atherosclerosis Reports, 27, Article 44. https://doi.org/10.1007/s11883-025-01288-w
European Atherosclerosis Society Consensus Panel. (2020). Triglyceride-rich lipoproteins and cardiovascular risk: An consensus statement. European Heart Journal, 41(1), 99–130. https://doi.org/10.1093/eurheartj/ehz806
Feng, X., Zhang, G., Liu, Y., Zha, Z., Zhang, W., Zhuang, Q., Zhao, H., & Mei, Y. (2026). Association between remnant cholesterol–based lipid indicators and testosterone deficiency in middle-aged and older men: A cross-sectional study. Frontiers in Endocrinology, 17, Article 1782710. https://doi.org/10.3389/fendo.2026.1782710
Ginsberg, H. N. (2002). New perspectives on atherogenesis: Role of abnormal triglyceride-rich lipoprotein metabolism. Circulation, 106(16), 2137–2142. https://doi.org/10.1161/01.CIR.0000035280.54348.14
Journal of the American Heart Association. (2025). [Study on remnant cholesterol and major adverse cardiovascular events]. Journal of the American Heart Association, Advance online publication. https://doi.org/10.1161/JAHA.125.045376
Marotzmann, S., Laufs, U., & Dressel, A. (2024). Association of apolipoprotein B and LDL cholesterol with cardiovascular events in patients with and without diabetes. Atherosclerosis, 391, Article 117468. https://doi.org/10.1016/j.atherosclerosis.2024.117468
Natsir, R. M., Halimah, E., Diantini, A., & Levita, J. (2026). A narrative review of remnant cholesterol as an independent atherogenic lipoprotein in Type 2 Diabetes: Pathophysiology and clinical implications. Therapeutics and Clinical Risk Management, 22, 105–118. https://doi.org/10.2147/TCRM.S593168
Nordestgaard, B. G., & Varbo, A. (2014). Triglycerides and cardiovascular disease. The Lancet, 384(9943), 626–635. https://doi.org/10.1016/S0140-6736(14)61177-6
Remnant cholesterol as independent vascular risk driver. (2026). Atherosclerosis, Article 120755. Advance online publication. https://doi.org/10.1016/j.atherosclerosis.2026.120755
Wadström, B. N., Pedersen, K. M., Wulff, A. B., & Nordestgaard, B. G. (2024). Remnant cholesterol, not LDL cholesterol, explains peripheral artery disease risk conferred by apoB: A cohort study. Arteriosclerosis, Thrombosis, and Vascular Biology, 44(5), 1261–1272. https://doi.org/10.1161/ATVBAHA.123.320175
Wulff, A. B., Varbo, A., Nordestgaard, A. T., & Nordestgaard, B. G. (2026). Feasibility of remnant cholesterol as a therapeutic target for atherosclerotic cardiovascular disease. Expert Opinion on Therapeutic Targets, 30(3), 229–244. https://doi.org/10.1080/14728222.2026.2639678
Zhang, H., Tao, J., Liang, C., et al. (2026). Association between the remnant cholesterol and the risk of new-onset chronic diseases: Evidence from CHARLS. Diabetology & Metabolic Syndrome, 18, Article 51. https://doi.org/10.1186/s13098-026-02106-2
Zhao, Y., Zhuang, Z., Li, Y., et al. (2024). Elevated blood remnant cholesterol and triglycerides are causally related to the risks of cardiometabolic multimorbidity. Nature Communications, 15, Article 2451. https://doi.org/10.1038/s41467-024-46686-x
Last Updated: June 2026 | Author: Dr. T.S. Didwal, M.D. (Internal Medicine) | Category: Heart & Metabolism