Cellular Senescence: Why Your Cells Age and What It Means for Your Health
What is cellular senescence? Learn how aging cells affect your heart and brain, and discover emerging treatments like senolytics to improve your healthspan.
AGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/19/202616 min read
Aging rarely arrives all at once. It creeps in quietly — in the extra time it takes to recover from a workout, the stiffness that lingers in the knees each morning, the forgotten name hovering just beyond memory, the sudden fatigue after a poor night’s sleep. For decades, medicine treated these changes as inevitable consequences of time. But modern biology is revealing something far more unsettling — and far more hopeful. Deep inside our tissues, a hidden population of damaged cells may be actively accelerating the aging process itself.
These cells are known as senescent cells, often nicknamed “zombie cells.” They no longer divide or function normally, yet they refuse to die. Instead, they remain metabolically active, releasing a toxic stream of inflammatory chemicals that gradually damages surrounding healthy tissue — a process increasingly linked to cardiovascular disease, type 2 diabetes, neurodegeneration, frailty, and even cancer progression (Ajoolabady et al., 2025; Tenchov et al., 2024). Scientists now consider cellular senescence one of the central biological hallmarks of aging.
What makes this discovery revolutionary is that senescence may not simply mark aging — it may help drive it. Even more remarkably, emerging research for 2025–2026 suggests that these harmful cells might someday be selectively targeted, silenced, or removed through therapies known as senolytics and senomorphics (Martin et al., 2026; Kletsas, 2026). Yet the science is more nuanced than early headlines suggested. Some senescent cells also help suppress cancer, repair wounds, and coordinate tissue healing (Yamauchi & Takahashi, 2025). Aging, it turns out, is not merely wear and tear. It is a complex biological conversation — and scientists are finally beginning to understand its language.
Clinical Takeaways on Cellular Senescence
1. Cellular Senescence Is a Core Driver of Biological Aging
Senescent “zombie” cells are now recognised as a major hallmark of ageing, contributing to chronic inflammation, tissue dysfunction, frailty, and multimorbidity across organ systems.
2. Chronic Inflammation (“Inflammaging”) Connects Aging Diseases
The SASP inflammatory profile links cellular senescence to major age-related diseases including cardiovascular disease, Type 2 Diabetes, neurodegeneration, sarcopenia, osteoarthritis, and cancer progression.
3. Immune Aging Reduces Senescent Cell Clearance
Age-related dysfunction of CD8+ T cells weakens immune surveillance, allowing senescent cells to accumulate and amplify systemic inflammation and tissue degeneration.
4. Senescence Is Biologically Complex — Not Universally Harmful
Emerging 2025–2026 research shows some senescent cells support tumour suppression, wound healing, and tissue repair, highlighting the need for precision rather than indiscriminate anti-aging therapies.
5. Lifestyle Medicine Remains the Most Evidence-Based “Senolytic”
Regular exercise, metabolic health optimization, Mediterranean-style nutrition, quality sleep, stress reduction, and smoking avoidance remain the strongest clinically validated interventions to slow senescence accumulation.
6. Healthspan Is Becoming a Central Clinical Target
Modern longevity medicine is shifting focus from simply extending lifespan to preserving cognitive function, mobility, metabolic resilience, immune competence, and independence throughout aging.
What Exactly Is Cellular Senescence?
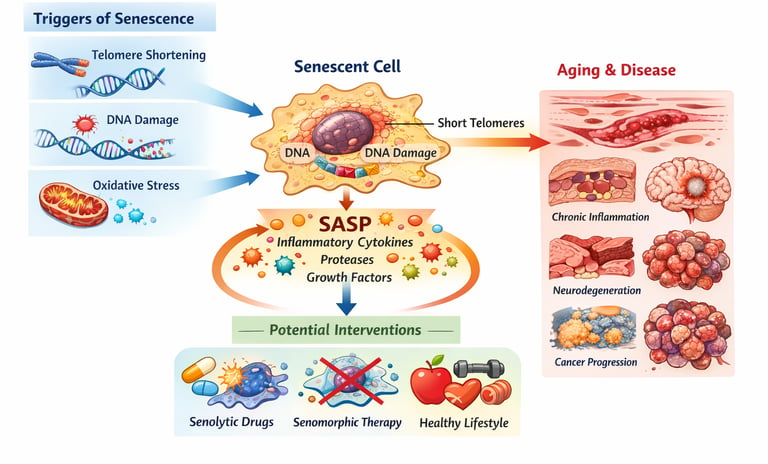
Every cell in your body carries a built-in division counter embedded in structures called telomeres — protective caps at the tips of chromosomes. Each time a cell divides to repair tissue or replace aging structures, these caps shorten slightly. After approximately 50–70 divisions — a threshold known as the Hayflick Limit — the telomere becomes critically short, and the cell triggers an internal alarm: no more division (Ajoolabady et al., 2025).
But rather than dying quietly through programmed cell death (apoptosis), many senescent cells choose a different path. They enter a state of permanent metabolic activity — alive, but no longer useful — while simultaneously broadcasting a cascade of inflammatory molecules to everything around them. Researchers call this the Senescence-Associated Secretory Phenotype, or SASP (Ajoolabady et al., 2025).
The SASP 'chemical soup' contains inflammatory cytokines such as IL-6 and TNF-α, growth factors that can paradoxically encourage tumour growth, and enzymes that degrade the surrounding tissue architecture. A handful of zombie cells in a blood vessel wall or in the pancreas can corrupt entire neighbourhoods of healthy tissue, spreading cellular dysfunction like a biological wildfire.
Key Definition: SASP (Senescence-Associated Secretory Phenotype)
The inflammatory cocktail secreted by senescent cells. It includes cytokines, growth factors, and tissue-degrading enzymes that damage neighbouring healthy cells and fuel chronic, low-grade inflammation — a process scientists call 'inflammaging.'
The Biological Complexity Behind the Science: Beyond Simple 'Zombie Cells'
For years, the narrative around cellular senescence was relatively straightforward: cells become senescent, accumulate, cause damage, and must be eliminated. A groundbreaking 2026 review in Nature Reviews Molecular Cell Biology by Martin and colleagues challenges that oversimplification head-on.
Martin et al. (2026) demonstrate that senescent cells are not a monolithic population. Their molecular signatures — the specific proteins, gene expression patterns, and secretory outputs — vary dramatically depending on the cell type, the trigger that induced senescence, and the tissue microenvironment. What acts as a harmful zombie cell in one organ may play a context-dependent repair role in another.
This biological complexity has enormous implications. It means that blanket strategies to eliminate all senescent cells may be too crude, risking the removal of cells that are transiently beneficial — for instance, during wound healing or embryonic development. The future of anti-senescence therapy will likely require cell-type-specific and context-aware approaches.
Similarly, Kletsas (2026), writing in FEBS Open Bio, highlights specific molecular signatures and structural remodelling patterns that distinguish harmful chronic senescence from transient, protective senescence. The distinction matters enormously for designing targeted therapies that preserve the good while eliminating the bad.
Why Senescence Begins: The Four Main Triggers
Multiple insults can push a healthy cell into senescence. Understanding the triggers helps explain why lifestyle choices matter so profoundly.
1. Telomere Shortening (Replicative Senescence)
The most classical pathway: cells that divide frequently — skin, gut lining, immune cells — exhaust their telomere reserves faster. This is the biological odometer described by the Hayflick Limit. Lifestyle factors such as chronic psychological stress, poor sleep, smoking, and a sedentary lifestyle measurably accelerate telomere attrition (Tenchov et al., 2024).
2. DNA Damage Response
Radiation, environmental toxins, chemotherapy, and the ordinary byproducts of metabolism can all damage the double helix. When the damage is too severe to repair, the cell permanently arrests — a protective response that prevents potentially cancerous replication, but at the cost of creating a lingering inflammatory cell (Ajoolabady et al., 2025).
3. Oxidative Stress and Mitochondrial Dysfunction
Free radicals generated during energy production damage cellular components, including DNA and mitochondrial membranes. As we age, our antioxidant defences decline, allowing oxidative stress to accumulate and drive stress-induced premature senescence — even in cells that have not yet reached their division limit (Ajoolabady et al., 2025).
4. Oncogene Activation
When a proto-oncogene mutates and fires inappropriately, cells can arrest themselves in senescence as an emergency brake to prevent malignant transformation. This is a profoundly important anti-cancer mechanism — which also explains why senescence is a double-edged sword (Yamauchi & Takahashi, 2025).
The Double-Edged Sword: Senescence as Friend and Foe
One of the most surprising findings in senescence biology is that the very process responsible for tissue dysfunction and aging is also one of your body's most powerful cancer-prevention tools. This paradox has been elegantly described by Yamauchi and Takahashi (2025) in The Journal of Biochemistry.
In early life and young tissues, senescence acts as a tumour suppressor: when cells detect DNA damage or oncogene activation that could become cancer, they permanently arrest before turning malignant. The immune system — particularly CD8+ cytotoxic T cells — then clears these arrested cells efficiently, maintaining tissue health.
The problem emerges across decades. As we age, our immune surveillance capacity declines, and the clearance of senescent cells becomes increasingly inefficient. Senescent cells accumulate. Their SASP begins to create a pro-tumorigenic tissue microenvironment — rich in growth factors and inflammatory signals — that paradoxically begins to promote the very cancer the cells were originally trying to prevent (Yamauchi & Takahashi, 2025).
Clinical Insight: The Immune Connection
He et al. (2026) specifically examined how CD8+ T cells — the immune system's primary 'garbage collectors' for senescent cells — become dysfunctional with age. Aged CD8+ T cells develop their own senescence markers, reducing the immune system's ability to patrol and clear zombie cells. This creates a vicious cycle: more senescent cells escape clearance, the inflammatory environment worsens, and immune function deteriorates further.
Immune Cell Senescence: How Your Defence System Ages
The senescence story is not limited to structural tissues like heart muscle or brain neurons. The immune system itself succumbs to senescence — a phenomenon that compounds every other age-related vulnerability.
He et al. (2026), publishing in Science China Life Sciences, provide a comprehensive analysis of CD8+ T cell senescence. These cytotoxic lymphocytes are essential for killing virally infected cells, clearing damaged tissue, and eliminating early cancer cells. With age, they accumulate specific senescence biomarkers, lose their killing efficiency, and begin producing pro-inflammatory cytokines that mirror the SASP of structural cells.
A complementary 2026 study by Ohyagi, Ito, and Yoshimura in Inflammation and Regeneration examines how T cell senescence in specific organs drives tissue-level aging. Their findings reveal that immune cell senescence is not uniform across the body — it occurs in organ-specific patterns that may explain why certain tissues age faster than others in the same individual. This adds another layer to the complexity identified by Martin et al. (2026): the immune microenvironment of a given organ shapes both how senescent cells behave and how efficiently they are cleared.
Together, these findings suggest that restoring immune surveillance capacity — alongside direct targeting of senescent structural cells — may be an essential component of comprehensive anti-aging strategies.
How Senescent Cells Drive Age-Related Diseases
The SASP is not an abstract laboratory curiosity — it has direct, measurable consequences across virtually every major organ system.
Cardiovascular Disease
Senescent cells accumulate in arterial walls, driving the chronic vascular inflammation that underpins atherosclerosis. The SASP degrades the extracellular matrix holding plaque stable, increasing the risk of rupture and acute cardiovascular events (Tenchov et al., 2024).
Neurodegeneration
In the brain, senescent microglia and astrocytes secrete toxic inflammatory molecules that damage neurons and have been implicated in the pathophysiology of Alzheimer's and Parkinson's diseases. The brain's unique immune environment makes senescent cell clearance particularly challenging (Ajoolabady et al., 2025).
Type 2 Diabetes
Senescence of pancreatic beta cells — the insulin-producing cells — reduces insulin secretion capacity. Simultaneously, SASP-driven inflammation in adipose tissue promotes systemic insulin resistance, creating a dual metabolic burden (Tenchov et al., 2024).
Musculoskeletal Decline
Senescent cells in joint cartilage contribute to osteoarthritis through SASP-mediated matrix degradation. In skeletal muscle, accumulation of senescent satellite cells impairs regenerative capacity, accelerating age-related muscle loss (sarcopenia) (Ajoolabady et al., 2025).
Immune Dysfunction and Infection Susceptibility
As described by He et al. (2026) and Ohyagi et al. (2026), immune senescence increases vulnerability to infections, reduces vaccine effectiveness, and diminishes cancer immunosurveillance — compounding the risks created by senescent structural cells.
Emerging Treatments: From Senolytics to Immunotherapy
The rapid growth of senescence science has launched an equally energetic therapeutic development pipeline. Three major categories of intervention are currently under investigation.
Senolytics: Targeted Elimination
Senolytic drugs are designed to selectively kill senescent cells while leaving healthy cells unharmed. They typically work by blocking the survival signals that keep senescent cells alive despite the damage that would normally trigger apoptosis. Early clinical trials with combinations such as dasatinib plus quercetin have shown reductions in senescent cell burden and improvements in physical function in specific patient populations. However, as Martin et al. (2026) and Kletsas (2026) caution, the biological heterogeneity of senescent cells means that a single senolytic agent is unlikely to be universally effective — and indiscriminate clearance risks eliminating transiently beneficial senescent populations.
Senomorphics: Silencing the SASP
Rather than killing senescent cells, senomorphic compounds suppress their harmful inflammatory secretions. This approach is conceptually attractive because it reduces the collateral damage of senescence without the risks of aggressive cell elimination. Compounds such as rapamycin (an mTOR inhibitor) and certain flavonoids have demonstrated senomorphic activity in preclinical models (Ajoolabady et al., 2025).
Immune Restoration Therapy
Given the central role of CD8+ T cell senescence in failed immune clearance, strategies to rejuvenate the immune surveillance system represent a third therapeutic avenue. These include checkpoint inhibitor approaches, adoptive cell therapies using ex vivo-expanded rejuvenated T cells, and metabolic reprogramming strategies to restore mitochondrial fitness in immune cells (He et al., 2026; Ohyagi et al., 2026).
Important Note
No senolytic or senomorphic drug is currently approved by the FDA or equivalent regulatory bodies for routine clinical use in aging or age-related disease outside of specific cancer indications. All are considered investigational. Consult your physician before considering any supplement or drug claimed to target cellular senescence.
Practical Applications: What You Can Do Today
While pharmaceutical interventions continue through clinical development, the strongest current evidence supports lifestyle-based strategies that meaningfully slow senescence accumulation. These are not consolation prizes — they represent powerful, synergistic biology.
1. Move — Consistently and Vigorously
Exercise is the single most robustly validated anti-senescence intervention available without a prescription. Aerobic exercise reduces oxidative stress, preserves telomere length, enhances mitochondrial efficiency, and — critically — has been shown to reduce circulating SASP markers. Aim for at least 150 minutes of moderate-intensity aerobic activity per week, incorporating resistance training twice weekly to protect muscle mass and insulin sensitivity.
2. Adopt a Mediterranean-Style Diet
Rich in polyphenols, omega-3 fatty acids, fibre, and antioxidants, the Mediterranean diet has been associated with longer telomere length and lower markers of inflammaging in population studies. Specific components — including quercetin (found in onions and apples), resveratrol (found in grapes), and spermidine (found in fermented foods and mushrooms) — are actively studied for senomorphic properties.
3. Prioritise Sleep Quality
Chronic sleep deprivation is a potent driver of oxidative stress and accelerates biological aging. During deep sleep, the glymphatic system clears metabolic waste from the brain — including senescence-associated inflammatory proteins. Target seven to nine hours of quality, uninterrupted sleep per night.
4. Manage Chronic Stress
Psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, generating cortisol and inflammatory mediators that accelerate telomere shortening and promote stress-induced premature senescence. Mind-body practices including mindfulness meditation, yoga, and breathwork have demonstrated measurable effects on telomere-associated biomarkers in controlled trials.
5. Protect Against Environmental Senescence Triggers
Limit UV radiation exposure (sunscreen and protective clothing), avoid cigarette smoke (active and passive), minimise processed food consumption (which drives glycation and oxidative stress), and reduce exposure to environmental pollutants where possible — all represent evidence-based strategies for reducing the cellular burden that drives premature senescence.
6. Optimise Metabolic Health
Insulin resistance and elevated blood glucose dramatically accelerate cellular senescence, particularly in pancreatic, vascular, and adipose tissue. Maintaining a healthy body weight, eating a low-glycaemic diet, and exercising regularly protect against metabolic drivers of senescence accumulation.
Frequently Asked Questions
1. Is cellular senescence the same as aging?
No — but the two are intimately connected. Cellular senescence is one of several core biological mechanisms that drive the aging process. Research by Tenchov et al. (2024) identifies nine distinct hallmarks of aging, of which cellular senescence is among the most impactful. Other hallmarks include mitochondrial dysfunction, stem cell exhaustion, and epigenetic alterations. Senescence does not cause all of aging, but it significantly accelerates it.
2. If senescent cells cause harm, why doesn't the body just destroy them?
It does — but imperfectly, and decreasingly so with age. The immune system, particularly CD8+ cytotoxic T cells, is responsible for patrolling tissues and eliminating senescent cells. In youth this system is highly efficient. However, as He et al. (2026) and Ohyagi et al. (2026) demonstrate, T cells themselves develop senescence markers with age, progressively losing their clearance efficiency. The result is a growing backlog of senescent cells that escape immune surveillance — precisely the therapeutic gap that researchers are working to close.
3. Can cellular senescence actually be reversed?
Partially, and under specific conditions. Senolytics can remove senescent cells, which represents a form of partial reversal by reducing the senescent burden. However, the question of whether a senescent cell itself can be 'un-senesced' and returned to normal function is more complex. Some research suggests limited epigenetic reprogramming may be possible, but this remains far from clinical application. What is clear is that preventing new senescence accumulation — through lifestyle and potentially emerging pharmacological strategies — is currently more achievable than reversing established senescence.
4. Is cellular senescence always harmful?
No — and this nuance is critical. As Yamauchi and Takahashi (2025) emphasise, senescence serves essential biological functions including tumour suppression, wound healing facilitation, and embryonic development. The problem is chronic, accumulated senescence in aged tissues where clearance mechanisms fail. Martin et al. (2026) go further, demonstrating that the same molecular event can have beneficial or harmful outcomes depending on cell type, tissue context, and duration. This complexity is precisely why indiscriminate senolytic strategies may carry risks alongside their benefits.
5. What is the SASP and why does it matter for my health?
SASP stands for Senescence-Associated Secretory Phenotype — the inflammatory signal cocktail secreted by senescent cells into surrounding tissues. It contains cytokines (inflammatory signalling proteins such as IL-6 and TNF-α), matrix-degrading enzymes, and growth factors. For your health, SASP is important because it explains how a relatively small number of senescent cells can cause disproportionately widespread damage: the secretions spread inflammation, degrade tissue structure, and can even induce senescence in neighbouring healthy cells — a phenomenon called 'paracrine senescence.' Chronic elevation of SASP markers correlates with increased risk of cardiovascular disease, diabetes, neurodegeneration, and cancer.
6. Are there any supplements proven to target cellular senescence?
Several natural compounds — including quercetin, fisetin, resveratrol, and spermidine — have demonstrated senolytic or senomorphic properties in cell culture and animal models, and are being investigated in human trials. However, no supplement is currently proven to meaningfully reduce senescent cell burden in humans through well-powered, peer-reviewed clinical trials. The concentrations required for biological effect typically exceed what standard dietary intake or off-the-shelf supplements reliably deliver. Approach commercially marketed 'anti-senescence' supplements with healthy scepticism, and discuss any supplementation with your doctor before starting.
7. How can I know if I have high levels of cellular senescence?
Currently, measuring cellular senescence reliably requires specialised laboratory analysis of tissue biopsies — techniques not available in routine clinical practice. Circulating biomarkers of senescence and SASP (such as plasma IL-6, p16 expression in peripheral blood cells, or GDF-15 levels) are active areas of research and show promise as non-invasive indicators, but are not yet standardised for clinical use. In practice, the best proxy measures are markers of biological age and inflammaging available through functional medicine panels: fasting insulin, HbA1c, high-sensitivity CRP, homocysteine, and telomere length testing (available commercially, though with variable accuracy). Discuss with a physician interested in longevity medicine for the most current options.
Clnical pearls
1. The Paradox of the "Emergency Brake"
Scientific Perspective: Cellular senescence is a highly evolved, cell-autonomous tumor-suppressor mechanism. When a cell experiences oncogene activation or severe DNA damage, it permanently arrests replication via pathways like $p16^{INK4a}/Rb$ or $p53/p21$ to prevent malignant transformation.
Patient-Friendly Perspective: Think of cellular senescence as your body's emergency brake. When a cell gets dangerously damaged and threatens to turn into cancer, the body forces it to stop dividing completely to protect you from tumors.
2. Chronicity Shifts the Balance from Protection to Pathogenesis
Scientific Perspective: While transient senescence assists in acute wound healing and embryogenesis, chronic accumulation of these cells over decades results in a persistent Senescence-Associated Secretory Phenotype (SASP). The continuous secretion of pro-inflammatory cytokines (like IL-6 and TNF-$\alpha$) and matrix metalloproteinases disrupts surrounding extracellular matrix architecture and drives tissue-level "inflammaging."
Patient-Friendly Perspective: In the short term, "zombie cells" can actually help heal wounds. The trouble starts as we age and these cells pile up. Because they refuse to die, they constantly leak a toxic, inflammatory chemical soup that slowly poisons and damages the healthy tissue around them.
3. The Heterogeneity Hurdle in Senotherapeutic Design
Scientific Perspective: Senescent cells do not possess a universal, monolithic molecular signature. Recent 2026 data shows their phenotypes, surface markers, and secretory outputs vary radically based on the cell type of origin and the initiating stressor. Consequently, broad-spectrum senolytic strategies risk off-target toxicity or the inadvertent deletion of transiently beneficial senescent cell populations.
Patient-Friendly Perspective: There isn't just one type of "zombie cell." New research shows these cells look and act very differently depending on where they are in the body. Because of this, scientists cannot just use a single, blunt drug to wipe them all out without accidentally killing off some "good" cells that are still helping the body repair itself.
4. The Vicious Cycle of Immunosenescence and Surveillance Failure
Scientific Perspective: Under physiological conditions, cytotoxic CD8+ T cells efficiently identify and clear senescent structural cells. However, as the immune system itself undergoes immunosenescence, aged CD8+ T cells exhibit compromised cytotoxic efficiency and begin contributing to the systemic SASP burden. This leads to a self-perpetuating cycle of failed clearance and accelerated tissue degradation.
Patient-Friendly Perspective: In your youth, your immune system acts like an efficient garbage truck, hunting down and destroying zombie cells. But as time goes on, the immune system's cells get old and "senescent" too. The garbage trucks break down, allowing the toxic zombie cells to multiply even faster.
5. Paracrine Senescence Spreads Organ-Specific Disease
Scientific Perspective: Through paracrine signaling, the SASP can actively induce "secondary senescence" in neighboring, healthy bystander cells. This local amplification loop directly drives the clinical progression of site-specific pathologies, including matrix degradation in osteoarthritis, endothelial dysfunction in atherosclerosis, and beta-cell exhaustion in Type 2 Diabetes.
Patient-Friendly Perspective: Zombie cells don't keep to themselves; they act like a biological wildfire. The toxic chemicals they secrete can actually "infect" neighboring healthy cells, turning them into zombies too. This chain reaction is what causes specific problems like stiff, aching joints, clogged arteries, and diabetes.
6. Lifestyle Interventions as Endogenous Senomorphic Therapies
Scientific Perspective: While targeted pharmaceutical senolytics (like dasatinib and quercetin) remain investigational, mechanical and metabolic stressors—such as progressive resistance exercise and caloric modulation—act as effective senomorphics. They downregulate SASP expression, mitigate oxidative stress, and stimulate autophagy, effectively preserving telomere length and enhancing endogenous immune clearance.
Patient-Friendly Perspective: While there isn't an approved anti-aging pill yet, everyday habits are incredibly powerful at silencing these zombie cells. Regular vigorous exercise, deep sleep, and a Mediterranean diet rich in antioxidants act like a mute button on the toxic chemical soup, while helping your immune system clean up the cellular trash.
Take Your Healthspan Into Your Own Hands
The science of cellular senescence is one of the fastest-moving fields in medicine. Stay ahead of the curve — and take action now with these evidence-based steps.
✅ Book a metabolic health review with your GP or a longevity-focused physician
✅ Request an inflammation panel (hs-CRP, IL-6, fasting insulin, HbA1c)
✅ Start your 'anti-senescence lifestyle' today: move, eat colourfully, sleep deeply, manage stress
✅ Share this article with someone whose healthspan matters to you
✅ Follow the references below to explore the primary science firsthand
Clinician’s Perspective: Why Cellular Senescence Matters in Modern Medicine
For clinicians, cellular senescence is rapidly evolving from a theoretical aging concept into a clinically relevant framework that may help explain why so many chronic diseases cluster together with advancing age. Conditions traditionally managed in isolation — including Type 2 Diabetes, Alzheimer's Disease, atherosclerotic cardiovascular disease, sarcopenia, frailty, osteoarthritis, and cancer — increasingly appear linked by a shared biology of chronic inflammation, mitochondrial dysfunction, immune exhaustion, and senescent cell accumulation.
What makes this field particularly important is its translational potential. Senescence biology offers a mechanistic bridge between preventive medicine, longevity science, metabolic health, and immunology. The SASP phenotype helps clinicians understand how a relatively small burden of dysfunctional cells can amplify systemic inflammation (“inflammaging”), impair tissue repair, worsen insulin resistance, destabilize vascular plaques, and accelerate multisystem decline.
However, clinicians should approach the field with scientific caution rather than commercial enthusiasm. Despite growing public interest in “anti-aging medicine,” no senolytic or senomorphic therapy currently has sufficient long-term evidence for routine clinical use outside research settings. Many supplements marketed online dramatically overstate human evidence. The current standard of care remains aggressive optimization of established lifestyle and metabolic interventions.
From a practical perspective, the most evidence-based anti-senescence strategy today remains:
exercise prescription,
metabolic risk reduction,
sleep optimization,
nutritional quality,
body composition management,
smoking cessation,
and inflammation control.
Importantly, senescence research reinforces a major shift occurring in internal medicine: the transition from disease-centered care toward healthspan-centered care. The goal is no longer merely extending survival, but preserving physiological resilience, cognitive function, mobility, immune competence, and independence across decades of aging.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Mitochondria, Motor Units, and Muscle Aging: A Complete Guide | DR T S DIDWAL
Can Aging Cells Cause Diabetes? The Science Behind SASP and Blood Sugar Dysfunction
Exercise and Longevity: The Science of Protecting Brain and Heart Health as You Age | DR T S DIDWAL
The Science of Healthy Brain Aging: Microglia, Metabolism & Cognitive Fitness | DR T S DIDWAL
The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It | DR T S DIDWAL
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
Waist-Calf Ratio: The Longevity Metric Most People Aren’t Tracking | DR T S DIDWAL
Blue Zones Secrets: The 4 Pillars of Longevity for a Longer, Healthier Lifepost | DR T S DIDWAL
Anabolic Resistance: Why Muscles Age—and How to Restore Their Growth Response | DR T S DIDWAL
References
Ajoolabady, A., Pratico, D., Bahijri, S., et al. (2025). Hallmarks and mechanisms of cellular senescence in aging and disease. Cell Death Discovery, 11, 364. https://doi.org/10.1038/s41420-025-02655-x
He, Z., Guo, F., Zhao, Q., & Lu, W. (2026). CD8+ T cell aging, senescence, and related disease. Science China Life Sciences. https://doi.org/10.1007/s11427-025-3101-7
Kletsas, D. (2026). Cellular senescence: Molecular signatures and cellular remodeling. FEBS Open Bio, 16, 818–820. https://doi.org/10.1002/2211-5463.70258
Martin, N., Li, H., Keyes, W. M., et al. (2026). Prevailing views of cell senescence overlook its biological complexity. Nature Reviews Molecular Cell Biology. https://doi.org/10.1038/s41580-026-00973-1
Ohyagi, M., Ito, M., & Yoshimura, A. (2026). Senescence of T cells and organ aging. Inflammation and Regeneration, 46, 19. https://doi.org/10.1186/s41232-026-00419-3
Tenchov, R., Sasso, J. M., Wang, X., & Zhou, Q. A. (2024). Aging hallmarks and progression and age-related diseases: A landscape view of research advancement. ACS Chemical Neuroscience, 15(1), 1–30. https://doi.org/10.1021/acschemneuro.3c00531
Yamauchi, S., & Takahashi, A. (2025). Cellular senescence: Mechanisms and relevance to cancer and aging. The Journal of Biochemistry, 177(3), 163–169. https://doi.org/10.1093/jb/mvae079