The Aging Muscle Paradox: How Senescent Cells Cause Insulin Resistance and The Strategies to Reverse It
Discover how senescent cells cause insulin resistance in aging muscle, and learn 7 evidence-based strategies — from exercise to emerging drugs — to reverse it.
AGING
Dr. T.S. Didwal, M.D.
5/26/202621 min read
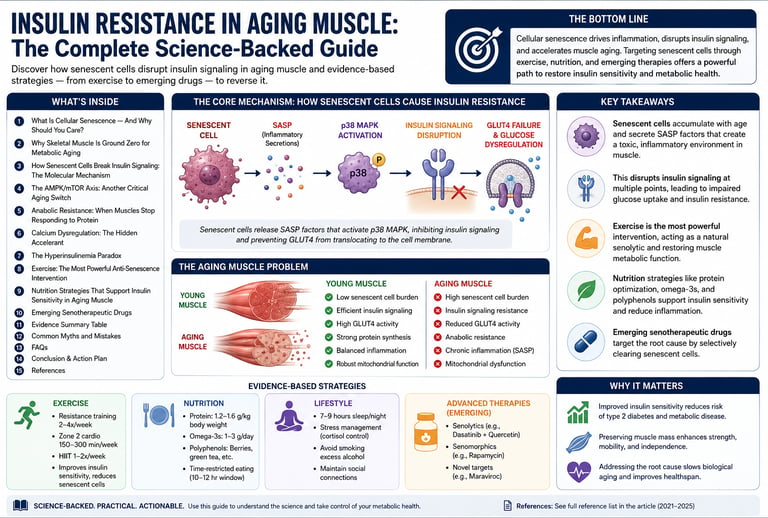
Insulin resistance in aging muscle is primarily driven by cellular senescence — the accumulation of dysfunctional "zombie cells" that secrete inflammatory factors (SASP). These factors activate p38 MAPK, which disrupts insulin signaling by impairing Akt phosphorylation and GLUT4 translocation to the muscle cell membrane.
Key mechanisms include:
- Senescence-driven chronic inflammation
- AMPK/mTOR imbalance
- Anabolic resistance
- Calcium dysregulation
Most effective evidence-based ways to reverse it:
1. Combined exercise (resistance + aerobic/HIIT) – acts as a natural senolytic, strongest intervention
2. Higher protein intake (1.6–2.2 g/kg/day)
3. Optimize Vitamin D and magnesium
4. Mediterranean diet rich in polyphenols
5. Emerging senolytics (dasatinib + quercetin, p38 MAPK inhibitors, Maraviroc)
Key takeaways
1. Cellular senescence drives muscle insulin resistance through SASP-mediated inflammatory signaling. Accumulation of senescent cells in skeletal muscle secretes a pro-inflammatory SASP that activates p38 MAPK, impairing downstream insulin signaling (specifically Akt phosphorylation and GLUT4 translocation), independent of primary receptor defects (Rana et al., 2025; Englund et al., 2021).
2. Skeletal muscle functions as the primary site of age-related metabolic dysfunction. As the largest insulin-sensitive tissue responsible for ~80% of postprandial glucose uptake, senescence-induced impairments in muscle lead to systemic glucose dysregulation, sarcopenia, and accelerated metabolic aging, positioning muscle as ground zero rather than a secondary victim (Rizvi & Rizzo, 2024).
3. Disruption of the AMPK/mTOR axis constitutes a parallel pathway to senescence-driven pathology. Age-related decline in AMPK activity reduces autophagy, mitochondrial biogenesis, and insulin sensitization, while dysregulated mTOR contributes to anabolic resistance; exercise potently restores this balance (Mingzheng & You, 2025).
4. Anabolic resistance and insulin resistance form a bidirectional vicious cycle. Elevated thresholds for muscle protein synthesis in aging, combined with impaired insulin-mediated amino acid uptake, exacerbate sarcopenia and further impair glucose disposal, necessitating higher per-meal protein doses (1.6–2.2 g/kg/day) to overcome (Pérez-Castillo et al., 2025).
5. Exercise represents the most potent senotherapeutic intervention currently available. Structured combined training (resistance + aerobic/HIIT) exerts direct senolytic and senomorphic effects via autophagy induction, AMPK activation, myokine release, and GLUT4 upregulation, significantly reducing senescent cell burden and restoring insulin sensitivity (Podraza-Farhanieh et al., 2025; Zhang et al., 2025).
6. Precision senotherapeutics targeting senescence and SASP offer promising disease-modifying potential. Compounds such as dasatinib + quercetin, p38 MAPK inhibitors, and repurposed agents like Maraviroc (via CCR5 targeting identified through multiomics) address root mechanisms, shifting the therapeutic paradigm from symptom management (e.g., hyperinsulinemia) toward clearance or suppression of dysfunctional cells (Li et al., 2025).
Introduction
You eat right, you stay reasonably active, but as the years pass, your blood sugar climbs and your muscles feel less responsive. You're told it's just "normal aging." But what if the real culprit isn't your diet, your genetics, or even your willpower — but a hidden army of dysfunctional cells quietly poisoning your muscles from the inside?
Insulin resistance in aging muscle is one of the most consequential — and least understood — metabolic changes in the human body. It accelerates the path to type 2 diabetes, erodes muscle mass, and speeds up the biological aging process itself. And according to a rapidly expanding body of research published between 2021 and 2025, the primary driver isn't what most people think.
The culprit is cellular senescence — and the inflammatory chaos these "zombie cells" create inside your skeletal muscle tissue.
This guide breaks down the cutting-edge science in plain language. You'll learn exactly what's happening inside aging muscle at the cellular level, why it matters for your metabolic health, and — most importantly — what you can do about it today, backed by the latest peer-reviewed evidence.
Here's what you'll discover:
What cellular senescence is and why it hijacks your insulin signaling
The molecular pathway (SASP → p38 MAPK → GLUT4 failure) that causes glucose dysregulation
How exercise acts as a natural "senolytic" agent
Emerging drug therapies targeting the root cause
Practical, evidence-based protocols to protect and restore your metabolic health
1. What Is Cellular Senescence — And Why Should You Care?
Imagine a factory worker who shows up every day, refuses to do any work, and actively throws wrenches into every other machine on the floor. That's a senescent cell.
Cellular senescence is a state of permanent growth arrest — cells that have stopped dividing but refuse to undergo programmed cell death (apoptosis). In small numbers and for short periods, senescent cells serve useful biological functions: they help wounds heal, suppress tumor formation, and signal for tissue repair. The problem arises when these cells accumulate faster than the body can clear them, which is exactly what happens with aging.
What Makes Senescent Cells Dangerous: The SASP
Senescent cells don't sit quietly. They secrete a toxic cocktail of inflammatory molecules known as the Senescence-Associated Secretory Phenotype (SASP). This includes:
Pro-inflammatory cytokines (IL-6, IL-8, TNF-α)
Matrix metalloproteinases that degrade surrounding tissue
Growth factors that dysregulate neighboring cells
Reactive oxygen species (ROS) that cause oxidative damage
Think of SASP as a chronic, low-grade inflammatory signal that never turns off. In the short term, it's a warning system. Chronically, it's a slow poison.
Key Point: Senescent cells in skeletal muscle accumulate progressively with age and are now recognized as primary drivers of age-related metabolic dysfunction, not merely innocent bystanders (Englund et al., 2021).
2. Why Skeletal Muscle Is Ground Zero for Metabolic Aging
Skeletal muscle is far more than a locomotion system. It is the largest insulin-sensitive organ in the human body, responsible for clearing approximately 80% of postprandial blood glucose. When muscle metabolism falters, the metabolic consequences ripple across virtually every organ system.
The Scale of the Problem
Consider these numbers:
Muscle mass declines at roughly 3–8% per decade after age 30
After age 60, the rate of decline accelerates
Individuals with significant sarcopenia face a 2–4× higher risk of developing type 2 diabetes
Approximately 40% of adults over 70 show measurable insulin resistance even without obesity
Crucially, as Rizvi and Rizzo (2024) highlight in Medicina, the convergence of reduced muscle mass and diminished insulin sensitivity in older adults — particularly those who are obese — creates a compounding metabolic crisis that standard glucose-lowering treatments are poorly equipped to address. Treating the blood sugar number without addressing the muscle biology is like mopping the floor while the tap is still running.
Sarcopenia vs. Metabolic Dysfunction: Which Comes First?
The old view framed sarcopenia (muscle mass loss) as the primary problem. Contemporary research reframes the story: the accumulation of senescent cells within muscle tissue transforms the microenvironment from anabolic to catabolic, and sarcopenia is largely a downstream consequence.
People who maintain robust metabolic health into their 80s and 90s tend to have lower senescent cell burdens — not necessarily superior genetics for muscle building. This reframing is therapeutically important: it shifts the target from "build more muscle" to "clear the cellular dysfunction driving muscle breakdown."
3. How Senescent Cells Break Insulin Signaling: The Molecular Mechanism
This is where the biology becomes both alarming and actionable.
The Normal Insulin Signaling Cascade
In a healthy muscle cell, insulin signaling works like a perfectly choreographed relay race:
Insulin binds to the insulin receptor on the muscle cell surface
The receptor activates IRS-1 (Insulin Receptor Substrate-1)
IRS-1 activates PI3K (phosphatidylinositol 3-kinase)
PI3K activates Akt (Protein Kinase B)
Activated Akt triggers GLUT4 translocation to the cell membrane
GLUT4 acts as the glucose doorway — glucose enters the cell and blood sugar normalizes
When this cascade functions optimally, muscles act as an efficient glucose buffer after every meal.
How Senescent Cells Sabotage This Pathway
Senescent cells release SASP factors that activate p38 Mitogen-Activated Protein Kinase (p38 MAPK) — a stress signaling molecule that acts like a molecular jamming device.
According to research published in the Journal of Receptors and Signal Transduction (Rana et al., 2025), when muscle cells were induced into senescence in culture, they displayed:
Significantly impaired Akt phosphorylation — the relay is broken midway
Reduced GLUT4 translocation to the cell surface — the glucose door stays shut
Measurable insulin resistance that could be partially reversed by p38 MAPK inhibition
This is a landmark finding. It tells us that the insulin resistance in aging muscle isn't primarily about damaged insulin receptors — it's about inflammatory crosstalk from neighboring senescent cells jamming the downstream signaling machinery.
The Inflammatory Crosstalk Model
Think of senescent cells as hostile neighbors blasting loud music. The noise (SASP) doesn't just bother their immediate neighbors — it disrupts the entire neighborhood's ability to function. In muscle tissue, healthy cells surrounded by senescent ones absorb this inflammatory signaling, progressively losing their own metabolic competence.
4. The AMPK/mTOR Axis: Another Critical Aging Switch
Insulin signaling isn't the only metabolic pathway aging muscle gets wrong. A 2025 study by Mingzheng and You, published in Molecular and Cellular Biochemistry, examines the critical role of the AMPK/mTOR balance in exercise-related adaptations in aging muscle.
Understanding AMPK and mTOR
AMPK (AMP-activated protein kinase): The cellular energy sensor — activated by low energy states, exercise, and caloric restriction. Promotes glucose uptake, fat oxidation, mitochondrial biogenesis, and autophagy (cellular cleanup).
mTOR (mechanistic Target of Rapamycin): The growth and anabolic signaling hub — promotes protein synthesis and cell growth. Activated by nutrients, insulin, and growth factors.
In youth, these two systems operate in elegant counterbalance. After exercise, AMPK surges, cleaning up cellular debris and enhancing insulin sensitivity. During recovery and feeding, mTOR rises, rebuilding muscle protein.
How Aging Disrupts the Balance
With aging:
Baseline AMPK activity declines, reducing the body's capacity for cellular housekeeping and insulin-sensitizing signaling
mTOR signaling becomes dysregulated — chronically elevated in some contexts (accelerating senescence) and paradoxically blunted in response to anabolic stimuli (contributing to anabolic resistance)
Mitochondrial efficiency drops, further impairing AMPK's ability to sense and respond to energy demands
The result is an aging muscle that is simultaneously resistant to anabolic signals (won't rebuild) and inefficient at glucose disposal (won't clear blood sugar). The AMPK/mTOR imbalance thus acts as a second, parallel pathway through which aging impairs muscle metabolic function — independent of, but synergistic with, senescence-driven SASP inflammation.
Clinical Insight: Exercise powerfully re-engages AMPK signaling and helps restore the AMPK/mTOR balance, offering one mechanistic explanation for why physical activity is metabolically restorative even in older adults (Mingzheng & You, 2025).
5. Anabolic Resistance: When Muscles Stop Responding to Protein
Even when older adults eat adequate protein, their muscles often fail to respond with the same efficiency as younger muscle tissue. This phenomenon — anabolic resistance — is a defining feature of aging muscle biology and has direct implications for insulin resistance.
What Is Anabolic Resistance?
In young individuals, a protein-rich meal triggers a robust muscle protein synthesis (MPS) response. Leucine and other essential amino acids activate mTORC1, driving new protein construction. In older adults, the threshold for triggering MPS is elevated, meaning:
Higher protein doses are required to achieve the same anabolic response
The duration of the anabolic window after meals is compressed
Oxidative disposal of amino acids increases, reducing their efficiency for muscle building
A comprehensive 2025 review in Nutrients by Pérez-Castillo and colleagues documents the nutritional and exercise strategies most effective for combating anabolic resistance in aging muscle. Their analysis highlights that the solution isn't simply eating more protein — it's combining optimal protein timing, leucine-enriched protein sources, and exercise stimuli to overcome the elevated anabolic threshold.
The Link to Insulin Resistance
Anabolic resistance and insulin resistance are deeply interconnected. Insulin is itself an anabolic signal for muscle — it promotes not just glucose uptake but also amino acid transport and protein synthesis. When insulin signaling fails (due to senescence-driven disruption), amino acid uptake into muscle is also impaired, compounding anabolic resistance. The two dysfunctions feed each other in a self-reinforcing cycle.
6. Calcium Dysregulation: The Hidden Accelerant
Most discussions of muscle aging focus on inflammation. But there's a less-appreciated mechanism quietly accelerating both senescence and insulin resistance: calcium dysregulation.
Calcium's Role in Healthy Muscle
Calcium is not just about muscle contraction. It's a master regulator of:
Gene expression and signaling cascades
Mitochondrial energy production
Redox (oxidative) balance
Autophagy activation
In healthy muscle, calcium is tightly compartmentalized. It surges during contraction and is rapidly pumped back into storage by SERCA (Sarco/Endoplasmic Reticulum Calcium ATPase) and managed by ryanodine receptors.
How Aging Disrupts Calcium Handling
Research by Terrell, Choi, and Choi (2023) in the International Journal of Molecular Sciences demonstrates that age-related changes in calcium-handling proteins create a state of chronic intracellular calcium dysregulation:
SERCA activity declines, leaving excess calcium in the cytoplasm
Ryanodine receptors become "leaky," releasing calcium inappropriately
Elevated intracellular calcium triggers oxidative stress and mitochondrial dysfunction
These conditions are powerful inducers of cellular senescence
In other words, calcium dysregulation is an upstream trigger — it helps create the senescent cells whose SASP then impairs insulin signaling. Addressing calcium homeostasis may therefore represent a preventive strategy, reducing the rate of senescent cell accumulation before it escalates to full metabolic dysfunction.
Calcium-Related Therapeutic Targets
Vitamin D optimization: Vitamin D receptors modulate calcium handling in muscle. Deficiency — extremely common in older adults — impairs SERCA function and worsens calcium dysregulation.
Magnesium adequacy: Magnesium is a cofactor for hundreds of enzymatic reactions, including those involved in calcium transport.
Exercise: Physical activity directly stimulates SERCA activity and improves calcium handling efficiency in muscle tissue.
Safety Note: Calcium supplementation alone is insufficient and may be counterproductive in isolation. Optimize total calcium metabolism through diet, Vitamin D, and physical activity first — discuss supplementation with your healthcare provider.
7. The Hyperinsulinemia Paradox
Here's one of the most counterintuitive findings in modern aging research: the very hormone that keeps you metabolically healthy in youth may accelerate your aging in middle age and beyond.
The Paradox Explained
In young, insulin-sensitive individuals, insulin is the ultimate anabolic hormone — driving growth, glucose clearance, and protein synthesis. But as cellular senescence accumulates:
Muscle becomes insulin resistant
The pancreas compensates by secreting more insulin (hyperinsulinemia)
Chronically elevated insulin accelerates cellular senescence and promotes inflammation
More senescence → more insulin resistance → more hyperinsulinemia → more aging
This feedback loop, documented by Kolb, Kempf, and Martin (2023) in Frontiers in Endocrinology, explains why simply managing blood glucose numbers with insulin-stimulating drugs may not address — and may inadvertently worsen — the underlying aging process.
What This Means Clinically
The therapeutic implication is profound: the goal should be to restore insulin sensitivity (so that lower insulin levels achieve the same glucose clearance) rather than simply adding more insulin signaling. This means addressing the root cause — cellular senescence — rather than patching the downstream manifestation.
8. Exercise: The Most Powerful Anti-Senescence Intervention
Before reaching for any pill or supplement, the evidence overwhelmingly points to one intervention as the single most powerful tool for combating insulin resistance in aging muscle: structured physical exercise.
Exercise as a Senolytic and Senomorphic Agent
A landmark 2025 study by Podraza-Farhanieh and colleagues in Molecular Metabolism demonstrated that physical training directly reduces cellular senescence burden in skeletal muscle while simultaneously restoring associated insulin resistance. This means exercise works at the root level — not just building muscle or burning calories, but actively clearing the dysfunctional cells causing the metabolic problem.
The mechanisms are multiple:
Autophagy activation: Exercise-induced cellular stress activates autophagy — the cell's self-cleaning system — which degrades and recycles senescent cell components and damaged organelles
Mitochondrial biogenesis: Exercise upregulates PGC-1α, driving new, healthy mitochondria production and improving energy metabolism
AMPK reactivation: Exercise powerfully engages AMPK signaling, restoring the metabolic balance disrupted by aging (Mingzheng & You, 2025)
GLUT4 upregulation: Regular physical activity increases the total number of GLUT4 transporters and their responsiveness to insulin and muscle contraction signals
Anti-inflammatory signaling: Contracting muscle releases myokines (including IL-6 in an acute, beneficial burst and irisin) that have systemic anti-inflammatory effects, counteracting SASP
What Type of Exercise Works Best?
A comprehensive 2025 systematic review in Frontiers in Physiology by Zhang and colleagues examined the effects of aerobic, resistance, interval, and combined training on glucose metabolism in older adults:
Exercise Type Primary Benefit Secondary Benefit Resistance Training Muscle mass preservation, GLUT4 upregulation Improved basal metabolic rate Aerobic Training Mitochondrial biogenesis, AMPK activation Fat oxidation, cardiovascular health High-Intensity Interval Training (HIIT) Maximum AMPK engagement, time-efficient Senolytic signaling, VO2max improvement Combined (Concurrent) Training Broadest metabolic benefits Addresses both senescence and anabolic resistance
The evidence-based recommendation: Combined training — incorporating both resistance and aerobic/interval elements — appears to offer the most comprehensive benefits for insulin resistance in aging muscle (Zhang et al., 2025).
Practical Exercise Protocol for Aging Muscle Metabolic Health
Resistance Training (2–3×/week):
Compound movements: squats, deadlifts, rows, presses
3–4 sets of 8–12 repetitions at 65–80% 1RM
Include unilateral exercises to address asymmetries
Aerobic/HIIT (2–3×/week):
Moderate-intensity continuous: 30–45 minutes at 60–70% max heart rate
Or HIIT: 8–10 × 1-minute high-intensity efforts with 1–2 minute recovery
Walking, cycling, swimming, rowing — choose what you'll sustain
Weekly Minimum:
150 minutes moderate-intensity OR 75 minutes vigorous-intensity aerobic activity
2 resistance training sessions
Aim to reduce prolonged sitting with movement breaks every 30–60 minutes
Start conservatively if sedentary, and consider working with a qualified exercise physiologist, particularly if managing diabetes or cardiovascular conditions.
9. Nutrition Strategies That Support Insulin Sensitivity in Aging Muscle
Exercise is the cornerstone, but nutrition powerfully modulates the cellular environment in which exercise works.
Protein: Quality, Quantity, and Timing Matter
Drawing on the anabolic resistance research (Pérez-Castillo et al., 2025), older adults likely need more protein than standard recommendations:
Target: 1.6–2.2 g protein per kg body weight per day (vs. the standard 0.8 g/kg RDA)
Per-meal dose: At least 30–40g of high-quality protein per meal to overcome the elevated anabolic threshold
Leucine emphasis: Prioritize leucine-rich sources (whey protein, eggs, meat, fish, legumes) — leucine is the primary mTORC1 trigger for muscle protein synthesis
Timing: Consuming protein within 1–2 hours post-exercise maximizes the synergistic anabolic effect
Anti-Senescence Nutritional Strategies
1. Quercetin
Anti-Aging Mechanism: Acts as a powerful senolytic (clears aged cells) and helps regulate the p38 MAPK pathway to reduce cellular stress.
Best Food Sources: Capers, red onions, apples, and berries.
2. Fisetin
Anti-Aging Mechanism: A potent natural senolytic compound proven in animal models to target and eliminate dysfunctional senescent cells.
Best Food Sources: Strawberries, apples, and persimmons.
3. Omega-3 Fatty Acids
Anti-Aging Mechanism: Fights the SASP (Senescence-Associated Secretory Phenotype) by lowering systemic inflammation, while actively supporting muscle protein synthesis.
Best Food Sources: Fatty fish (salmon, mackerel), flaxseeds, and walnuts.
4. Vitamin D
Anti-Aging Mechanism: Crucial for maintaining calcium homeostasis, preserving skeletal muscle function, and improving insulin sensitivity.
Best Food Sources: Sunlight exposure, oily fish, and fortified foods.
5. Magnesium
Anti-Aging Mechanism: Serves as an essential co-factor for calcium transport and plays a vital role in optimizing insulin receptor function.
Best Food Sources: Nuts, seeds, leafy green vegetables, and whole grains
.
6. Broad-Spectrum Polyphenols
Anti-Aging Mechanism: Delivers robust antioxidant defense, boosts mitochondrial health, and activates the body's longevity pathway, AMPK.
Best Food Sources: Berries, green tea, extra virgin olive oil, and dark chocolate.
Dietary Patterns With Evidence
Mediterranean Diet: Consistently associated with reduced insulin resistance, lower inflammatory markers, and better muscle mass preservation in aging adults
Time-Restricted Eating (TRF): Emerging evidence suggests compressing eating to an 8–10 hour window may enhance AMPK signaling, autophagy, and insulin sensitivity — though optimal protocols in older adults still require study
Avoid ultra-processed foods: These are independently associated with accelerated cellular senescence and metabolic dysfunction
⚠️ Dietary changes should be personalized. Those with kidney disease need careful guidance before increasing protein intake. Consult a registered dietitian.
10. Emerging Senotherapeutic Drugs
For many older adults, exercise and nutrition alone may not fully overcome decades of senescent cell accumulation. This is where pharmacological research is advancing rapidly.
Senolytics: Eliminating Senescent Cells
Senolytics are drugs that selectively induce apoptosis (programmed cell death) in senescent cells while leaving healthy cells unharmed. Current candidates in clinical investigation include:
Dasatinib + Quercetin (D+Q):
The most studied senolytic combination
Dasatinib (originally a leukemia drug) + quercetin (natural flavonoid)
Clinical trials showing reductions in senescent cell burden and related biomarkers
Typically used in intermittent pulsed dosing, not daily
Fisetin:
Natural senolytic found in fruits
Strong preclinical evidence; human trials underway
Potential safety advantage over pharmaceutical senolytics
Navitoclax (ABT-263):
BCL-2 inhibitor that targets anti-apoptotic proteins upregulated in senescent cells
Effective senolytic in animal models; thrombocytopenia is a limiting side effect
Senomorphics: Silencing the SASP
Senomorphics don't kill senescent cells — they suppress the toxic secretions that cause damage:
p38 MAPK Inhibitors:
Directly block the inflammatory signaling pathway identified by Rana et al. (2025) as responsible for GLUT4 suppression
Represent a highly targeted approach to restoring insulin signaling in aged muscle
Multiple compounds in clinical development
JAK Inhibitors:
Block JAK-STAT signaling, a major SASP amplification pathway
Ruxolitinib has shown senomorphic effects in early studies
The Maraviroc Discovery: A Precision Senotherapy Approach
One of the most exciting recent findings comes from a multiomics analysis published in Nature Communications (Li et al., 2025). Using comprehensive gene expression, proteomics, and metabolomic profiling of aging human skeletal muscle, researchers identified Maraviroc — a drug originally developed to block HIV entry into cells — as a potential senotherapeutic for sarcopenia.
The discovery emerged by identifying the specific molecular signature of senescent muscle cells (upregulated p16, p21, and dysregulated metabolic pathways) and screening approved drugs against this transcriptomic profile. Maraviroc targets CCR5, a receptor upregulated on senescent muscle cells, and appears capable of selectively reducing the senescence burden in muscle tissue.
This precision pharmacology approach — matching drug mechanisms to the specific molecular fingerprint of senescent cells in a given tissue — represents the future of senotherapy.
⚠️ Senotherapeutic drugs are investigational for aging and metabolic indications. Do not self-prescribe. Discuss participation in clinical trials with your healthcare provider if interested.
11. Evidence Summary Table
1. Top-Tier Interventions (Highest Evidence)
Combined Exercise Training
Key Mechanism: Acts as a natural senolytic (clears aged cells), activates AMPK pathways, increases GLUT4 transporters for glucose uptake, and triggers mitochondrial biogenesis (creation of new cellular energy factories).
Level of Evidence: Highest — Backed by multiple Randomized Controlled Trials (RCTs) and systematic reviews (2023–2025).
Practical Accessibility: ★★★★★ (Highly accessible to most individuals)
Optimized Protein Intake (1.6-2.2g/kg/day)
Key Mechanism: Overcomes age-related anabolic resistance (the body's decreased ability to utilize protein) and directly stimulates Muscle Protein Synthesis (MPS).
Level of Evidence: Strong — Supported by comprehensive meta-analyses.
Practical Accessibility: ★★★★★ (Easy to implement via diet and supplementation)
2. Strong to Moderate Evidence Interventions
Mediterranean Diet Pattern
Key Mechanism: Systemically reduces chronic inflammation and broadens overall metabolic health support.
Level of Evidence: Strong observational data, strongly supported by controlled clinical trials.
Practical Accessibility: ★★★★☆ (Requires consistent dietary habit shifts)
Vitamin D Optimization
Key Mechanism: Regulates calcium homeostasis and improves insulin receptor function.
Level of Evidence: Moderate — Supported by RCTs, though outcomes can vary by individual.
Practical Accessibility: ★★★★☆ (Accessible via sunlight, food, and low-cost supplements)
Dietary Polyphenols (Quercetin, Fisetin)
Key Mechanism: Provides natural senolytic action and suppresses the anti-SASP (inflammatory compounds secreted by aging cells).
Level of Evidence: Moderate preclinical data; early-stage human clinical trials are expanding.
Practical Accessibility: ★★★★☆ (Found readily in specific fruits, vegetables, and supplements)
Time-Restricted Eating
Key Mechanism: Activates the AMPK pathway, stimulates autophagy (cellular clean-up), and improves insulin sensitivity.
Level of Evidence: Moderate overall; clinical data specific to older adults are currently limited.
Practical Accessibility: ★★★☆☆ (Requires strict behavioral and scheduling compliance)
3. Emerging & Clinical Interventions (Lower Accessibility)
Dasatinib + Quercetin
Key Mechanism: Direct pharmaceutical/nutraceutical senolytic combo that aggressively reduces the body's overall cellular senescence burden.
Level of Evidence: Promising early-stage clinical trials.
Practical Accessibility: ★★☆☆☆ (Requires medical supervision; prescription-dependent)
p38 MAPK Inhibitors
Key Mechanism: Directly targets cellular stress pathways to restore healthy insulin signaling in muscle tissue.
Level of Evidence: Strong mechanistic data; active clinical translation is ongoing.
Practical Accessibility: ★★☆☆☆ (Experimental/Investigational)
Maraviroc (Sarcopenia Indication)
Key Mechanism: Targets CCR5 receptors on senescent muscle cells to combat age-related muscle wasting.
Level of Evidence: Supported by preclinical research and multiomics data; an emerging therapeutic candidate.
Practical Accessibility: ★★☆☆• (Off-label use or clinical trial setting only)
12. Common Myths and Mistakes
Myth 1: "Insulin resistance in aging is inevitable and irreversible." Reality: While aging creates biological headwinds, multiple interventions — particularly exercise and emerging senotherapeutics — can meaningfully restore insulin sensitivity even in older adults. The trajectory is modifiable, not fixed.
Myth 2: "Eating less protein is better for aging kidneys." Reality: In individuals with healthy kidney function, protein intakes of 1.6–2.2 g/kg/day are safe and necessary to overcome anabolic resistance. Protein restriction in aging accelerates muscle loss and worsens metabolic outcomes.
Myth 3: "Calcium supplements are the solution to calcium-related muscle aging." Reality: Calcium supplementation alone cannot correct the intracellular calcium signaling dysregulation that drives senescence. Calcium balance is managed through diet, Vitamin D, and exercise — with supplementation reserved for specific deficiencies under medical supervision.
Myth 4: "If my blood sugar is controlled, my muscle aging is being treated." Reality: Glucose control is important, but treating the blood sugar number while ignoring the underlying senescent cell burden is symptom management, not disease modification. The cellular fire driving metabolic dysfunction continues burning.
Myth 5: "HIIT is too dangerous for older adults." Reality: Appropriately scaled high-intensity interval training has been shown safe and highly effective for older adults, including those with metabolic disease, when properly supervised and introduced progressively.
Myth 6: "Supplements like quercetin will reverse cellular senescence on their own." Reality: While quercetin shows senolytic activity in preclinical and early clinical studies, it should be considered a complement to — not a replacement for — exercise and lifestyle optimization. Dose, bioavailability, and clinical efficacy thresholds in humans are still being established.
13. Frequently Asked Questions
Q: What is the simplest explanation of how aging causes insulin resistance in muscle? As muscles age, dysfunctional "zombie" cells (senescent cells) accumulate and release toxic inflammatory chemicals (SASP). These chemicals activate a stress pathway (p38 MAPK) that blocks the normal insulin signaling cascade, specifically preventing GLUT4 — the glucose transporter — from reaching the muscle cell surface. The result: glucose stays in the bloodstream even when insulin is present, causing insulin resistance.
Q: Can exercise alone reverse insulin resistance in aging muscle? Exercise is the single most evidence-based intervention available, and robust data (Podraza-Farhanieh et al., 2025; Zhang et al., 2025) shows it reduces senescent cell burden and restores insulin sensitivity. For many people, consistent structured exercise combined with appropriate nutrition can dramatically improve or even normalize insulin sensitivity. However, severely affected individuals or those with advanced metabolic disease may benefit from additional pharmacological approaches as they become available.
Q: How much protein should older adults eat to support muscle insulin sensitivity? Current evidence suggests older adults should target 1.6–2.2 grams of protein per kilogram of body weight per day, distributed across meals with at least 30–40g per meal, ideally from high-quality leucine-rich sources. This is significantly higher than the standard RDA of 0.8 g/kg, but necessary to overcome age-related anabolic resistance (Pérez-Castillo et al., 2025).
Q: What are senolytics and are any available now? Senolytics are drugs that selectively eliminate senescent cells. The most studied combination is dasatinib (a leukemia medication) plus quercetin (a plant flavonoid). While dasatinib requires a prescription and is investigational for aging indications, quercetin and fisetin are available as supplements. Clinical trials are ongoing — consult your doctor about eligibility.
Q: How does the AMPK/mTOR imbalance contribute to aging muscle problems? AMPK (the cellular energy sensor) declines with age, reducing the body's capacity for metabolic housekeeping, autophagy, and insulin sensitization. mTOR signaling becomes dysregulated. The net result is muscle that is simultaneously resistant to growth signals (anabolic resistance) and inefficient at glucose disposal. Exercise powerfully restores AMPK function and helps rebalance these pathways (Mingzheng & You, 2025).
Q: Is cellular senescence detectable with standard blood tests? Not yet with standard clinical tests. Assessment currently requires tissue biopsy or specialized blood tests measuring circulating senescent cells or biomarkers like p16 and p21. This is an active research area, with multiomics approaches (Li et al., 2025) advancing toward clinically accessible diagnostics.
Q: What role does Vitamin D play in muscle metabolic aging? Vitamin D is essential for normal calcium handling in muscle (a key upstream driver of senescence), insulin receptor function, and muscle protein synthesis. Deficiency — extremely common in adults over 50 — impairs all three. Optimizing Vitamin D status through sensible sun exposure, dietary sources, and supplementation (guided by 25-OH-D blood levels) is a low-risk, high-value component of any aging metabolic health strategy.
Q: Is type 2 diabetes in older adults primarily a muscle disease? Not exclusively, but the role of skeletal muscle is central and underappreciated. Given that muscle handles 80% of postprandial glucose disposal, senescence-driven insulin resistance in muscle tissue is a primary contributor to the glucose dysregulation that defines type 2 diabetes in aging. Liver, adipose tissue, and pancreatic beta-cell function also contribute (Rizvi & Rizzo, 2024).
Q: What is the Maraviroc discovery and why does it matter? Maraviroc is an HIV drug identified through multiomics analysis of aging muscle as a potential senotherapeutic for sarcopenia (Li et al., 2025). It targets the CCR5 receptor, upregulated on senescent muscle cells. This finding represents a precision medicine approach — matching existing approved drugs to specific molecular targets in senescent tissue — that could rapidly accelerate the development of senotherapeutics.
Q: Can a Mediterranean diet reduce cellular senescence in muscle? Directly, the evidence is still emerging. However, the Mediterranean diet's rich content of polyphenols (including quercetin and fisetin), omega-3 fatty acids, and anti-inflammatory compounds provides a dietary environment that reduces SASP-related inflammatory burden, supports mitochondrial health, and may reduce the rate of senescent cell accumulation. It's the most evidence-backed dietary pattern for aging metabolic health overall.
14. Conclusion and Action Plan
The science is clear: insulin resistance in aging muscle isn't just a glucose problem — it's a cellular biology problem. Senescent cells accumulating in skeletal muscle tissue disrupt insulin signaling through inflammatory cascades, calcium dysregulation, AMPK/mTOR imbalance, and anabolic resistance. These aren't separate aging phenomena; they're interconnected mechanisms driven by a common upstream source.
The good news is equally clear: this process is not fully inevitable, and meaningful reversal is possible.
Your Evidence-Based Action Plan
✅ Start exercising (or upgrade your current routine): Combine resistance training (2–3×/week) and aerobic/interval training (2–3×/week). This is your single highest-impact intervention.
✅ Optimize protein intake: Target 1.6–2.2 g/kg/day, distributed across meals, emphasizing leucine-rich sources.
✅ Check your Vitamin D: Ask your doctor to check your 25-OH-D level and optimize to the 40–60 ng/mL range.
✅ Adopt a Mediterranean-style eating pattern: High in polyphenols, omega-3s, vegetables, and lean protein. Minimize ultra-processed foods and refined carbohydrates.
✅ Reduce prolonged sitting: Movement breaks every 30–60 minutes can sustain AMPK activity between formal exercise sessions.
✅ Discuss senescence burden with your clinician: If you have prediabetes or type 2 diabetes, ask whether assessment tools or clinical trial options are appropriate for you.
✅ Stay informed: The senotherapeutic landscape is evolving rapidly. Dasatinib/quercetin combinations, p38 MAPK inhibitors, and agents like Maraviroc are progressing through clinical trials. The next 5–10 years may bring clinically available senolytic options.
The convergence of cellular biology, exercise science, and precision pharmacology is rewriting the story of metabolic aging. You are not condemned to a slow metabolic decline. You have more agency over this process than any previous generation of aging adults — but only if you act on the evidence.
⚠️ Medical Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making significant changes to your exercise, nutrition, or supplementation regimen, particularly if you have existing medical conditions.
Related Articles
VO2 Max & Longevity: The Ultimate Guide to Living Longer | DR T S DIDWAL
Why Exercise Is the Most Powerful Anti-Aging Therapy: A Research-Driven Guide | DR T S DIDWAL
References
Chaib, S., Palmer, A. K., Wyles, S. P., et al. (2025). Translating cellular senescence research into clinical practice for metabolic disease. Nature Reviews Endocrinology. Advance online publication. https://doi.org/10.1038/s41574-025-01187-9
Englund, D. A., Zhang, X., Aversa, Z., & LeBrasseur, N. K. (2021). Skeletal muscle aging, cellular senescence, and senotherapeutics: Current knowledge and future directions. Mechanisms of Ageing and Development, 200, Article 111595. https://doi.org/10.1016/j.mad.2021.111595
Kolb, H., Kempf, K., & Martin, S. (2023). Insulin and aging—a disappointing relationship. Frontiers in Endocrinology, 14, Article 1261298. https://doi.org/10.3389/fendo.2023.1261298
Li, Y., Li, C., Zhou, Q., et al. (2025). Multiomics and cellular senescence profiling of aging human skeletal muscle uncovers Maraviroc as a senotherapeutic approach for sarcopenia. Nature Communications, 16, Article 6207. https://doi.org/10.1038/s41467-025-61403-y
Mingzheng, X., & You, W. (2025). AMPK/mTOR balance during exercise: Implications for insulin resistance in aging muscle. Molecular and Cellular Biochemistry, 480(23), 5941–5953. https://doi.org/10.1007/s11010-025-05362-4
Pérez-Castillo, Í. M., Rueda, R., Pereira, S. L., Bouzamondo, H., López-Chicharro, J., Segura-Ortiz, F., & Atherton, P. J. (2025). Age-related anabolic resistance: Nutritional and exercise strategies, and potential relevance to life-long exercisers. Nutrients, 17(22), Article 3503. https://doi.org/10.3390/nu17223503
Podraza-Farhanieh, A., Spinelli, R., Zatterale, F., Nerstedt, A., Gogg, S., Blüher, M., & Smith, U. (2025). Physical training reduces cell senescence and associated insulin resistance in skeletal muscle. Molecular Metabolism, 95, Article 102130. https://doi.org/10.1016/j.molmet.2025.102130
Rana, K. S., Marwah, M. K., Raja, F. N. S., Dias, I., Hindalekar, Y. S., Al Tahan, M. A., & Bellary, S. (2025). The influence of senescent associated secretory phenotype on glucose homeostasis in C2C12 muscle cells: Insights into potential p38 inhibitor interventions. Journal of Receptors and Signal Transduction, 45(2), 118–127. https://doi.org/10.1080/10799893.2025.2475441
Rizvi, A. A., & Rizzo, M. (2024). Age-related changes in insulin resistance and muscle mass: Clinical implications in obese older adults. Medicina, 60(10), Article 1648. https://doi.org/10.3390/medicina60101648
Terrell, K., Choi, S., & Choi, S. (2023). Calcium's role and signaling in aging muscle, cellular senescence, and mineral interactions. International Journal of Molecular Sciences, 24(23), Article 17034. https://doi.org/10.3390/ijms242317034
Zhang, Q., Guo, Y., Zhang, H., Xu, W., & Yin, L. (2025). Effects of aerobic, resistance, interval, and combined training on glucose metabolism in older adults: Insights into type, dose, and mechanism. Frontiers in Physiology, 16, Article 1702669. https://doi.org/10.3389/fphys.2025.1702669