Why Muscle Health Controls Blood Sugar in Type 2 Diabetes (The Science Explained)
Learn how skeletal muscle drives insulin sensitivity, glucose uptake, and long-term metabolic health. Evidence-based strategies for Type 2 Diabetes, muscle preservation, and better blood sugar control.
DIABETESEXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/16/202626 min read
Why is skeletal muscle important in Type 2 Diabetes?
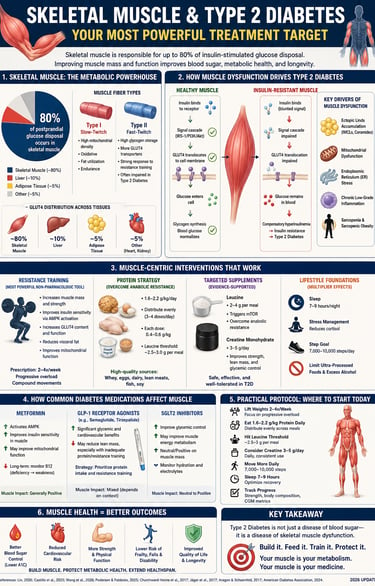
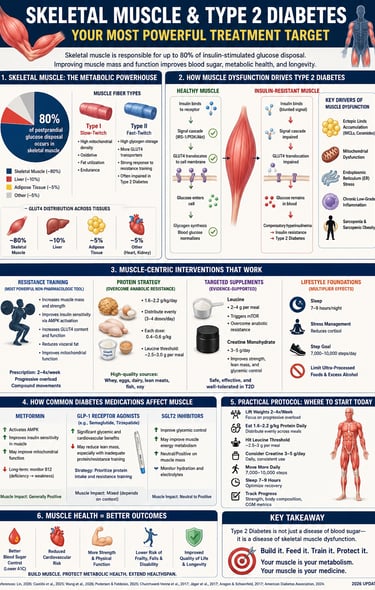
Skeletal muscle is the primary site of insulin-mediated glucose disposal, accounting for approximately 80% of post-meal glucose uptake. When muscle becomes insulin-resistant, blood sugar rises. Resistance training, adequate protein intake, and muscle-preserving therapies improve insulin sensitivity, glucose control, body composition, and long-term metabolic health.
Key Takeaways
1. Skeletal Muscle & Blood Sugar
Why skeletal muscle is the key to managing Type 2 Diabetes
Skeletal muscle is the body's primary site for insulin-mediated glucose disposal. Expanding muscle mass and quality creates a larger metabolic "sink" that clears blood sugar efficiently, directly improving glycemic control with or without insulin.
2. Resistance Training Prescription
How often should you lift weights for Type 2 Diabetes?
Resistance training 3 times per week (every 48 hours) maintains a continuous 24- 48-hour window of heightened insulin sensitivity. Prioritize compound lower-body lifts at $\ge$65% 1RM to activate GLUT4 glucose transporters without needing insulin.
3. Protein Intake & Anabolic Resistance
How much protein do you need daily if you have Type 2 Diabetes?
Type 2 Diabetes causes anabolic resistance, requiring a higher intake of 1.6–2.2g/kg of protein daily to preserve muscle. Spread this across 3–4 meals (30g+ each), ensuring each meal contains 2.5–3g of leucine to trigger muscle synthesis.
4. GLP-1 Side Effects on Muscle
Do Ozempic and Wegovy cause muscle loss?
GLP-1 drugs can cause 25–40% of total weight loss to come from lean muscle mass, increasing sarcopenia risks. To prevent this, experts recommend pairing GLP-1 therapy with resistance training 3x/week, $\ge$1.6g/kg daily protein, and creatine.
5. Creatine for Diabetes Control
Does creatine help lower blood sugar in Type 2 Diabetes?
Taking 3–5g of creatine monohydrate daily improves glucose control by upregulating GLUT4 transporters and boosting muscle glycogen storage by ~20%. Note: A slight rise in serum creatinine is expected and does not indicate kidney damage.
6. Metformin & Workout Timing
Should you take Metformin before or after a workout?
Taking Metformin immediately before a workout may blunt muscle gains by inhibiting mTORC1 muscle-building signals. To protect muscle growth while retaining metabolic benefits, time your Metformin dose several hours away from resistance training.
7. Root Causes of Muscle Dysfunction
What causes insulin resistance in skeletal muscle?
Muscle dysfunction in Type 2 Diabetes is driven early on by endoplasmic reticulum (ER) stress and ectopic fat buildup (intramyocellular lipids). This impairs GLUT4 translocation and mitochondrial function, which resistance training and protein directly counteract.
8. SGLT2 Inhibitors + Metformin
SGLT2 inhibitors and Metformin: Benefits and muscle risks
Combining SGLT2 inhibitors with Metformin offers superior blood sugar control, partly by shifting muscle metabolism to ketone use. Because this combination can cause modest lean mass loss, it should be paired with resistance training and high protein.
1. Why Skeletal Muscle Is the Core of Metabolic Disease
If you have been told that Type 2 Diabetes is about blood sugar, your pancreas, or your weight, you have been given an incomplete picture.
The real story begins with your skeletal muscle.
Skeletal muscle is not merely the tissue that moves your body. It is the dominant metabolic organ in the human system—responsible for postprandial (after-meal) glucose disposal when insulin signalling is functioning normally (Lin, 2026). When that muscle becomes metabolically impaired, glucose has nowhere to go. It accumulates in the bloodstream. Insulin levels rise to compensate. Over the years, this cycle produces insulin resistance, then Type 2 Diabetes, then cardiovascular disease.
Yet the dominant model of diabetes care remains focused on blood glucose targets, weight loss, and pharmacotherapy. Skeletal muscle—the organ at the physiological centre of this disease—is treated as an afterthought.
This is the gap this article addresses.
What Is Skeletal Muscle, Exactly?
Skeletal muscle constitutes roughly 30–40% of total body mass in healthy adults. It is made up of two primary fibre types:
Type I (slow-twitch) fibres are dense in mitochondria, highly oxidative, and suited for endurance. They rely primarily on fat as fuel and are metabolically active even at rest.
Type II (fast-twitch) fibres have higher glycogen storage capacity, greater density of GLUT4 glucose transporters, and respond more dramatically to resistance training. In Type 2 Diabetes, these fibres are consistently found to be underdeveloped and functionally impaired—a direct contributor to poor glucose handling (Castillo et al., 2025).
The clinical implication is direct: if you can increase the mass and metabolic quality of Type II muscle fibres, you expand the body's capacity to absorb and store glucose—with or without functional insulin signalling.
2. How Muscle Dysfunction Drives Type 2 Diabetes
Understanding why skeletal muscle becomes dysfunctional is not merely academic—it directly informs which interventions will work, for whom, and in what order.
The Cascade of Muscle Metabolic Failure
In healthy muscle, insulin binds to its receptor, triggers a signalling cascade via IRS-1/PI3K/Akt, and causes GLUT4 glucose transporter vesicles to migrate to the cell surface. Glucose enters the cell, is converted to glycogen, and blood glucose normalises within 1–2 hours of a meal.
In insulin-resistant muscle, this signal is attenuated at multiple steps. GLUT4 translocation is impaired. Glycogen synthesis slows. Glucose remains in circulation. The pancreas produces more insulin to compensate—until it can no longer keep up.
But the dysfunction goes deeper than signalling. A comprehensive 2025 review in Reviews in Endocrine and Metabolic Disorders (Castillo et al., 2025) identified several converging cellular mechanisms:
Ectopic lipid accumulation: Excess intramyocellular lipids (IMCLs) and ceramide accumulation within muscle fibres directly impair insulin signalling by activating serine kinases that phosphorylate IRS-1, blocking downstream glucose uptake pathways.
Mitochondrial dysfunction: Type 2 Diabetes is consistently associated with reduced mitochondrial density, impaired oxidative phosphorylation, and decreased capacity for fat oxidation in skeletal muscle. This creates a vicious cycle: less fat is burned, more accumulates intramuscularly, insulin resistance worsens.
Endoplasmic reticulum (ER) stress: A 2026 review in Frontiers in Endocrinology (Wang et al., 2026) identifies ER stress as a critical and underappreciated contributor to muscle dysfunction in Type 2 Diabetes. Chronic overnutrition and lipotoxicity overload the ER's protein-folding capacity, triggering the unfolded protein response (UPR). In skeletal muscle, UPR activation reduces insulin sensitivity, promotes atrophy, and impairs mitochondrial function. Crucially, this pathway is upstream of many visible signs of disease—making ER stress an early driver, not a consequence.
Sarcopenia and sarcopenic obesity: As muscle mass declines (sarcopenia) in the context of excess adiposity, the body's glucose buffering capacity shrinks. Castillo et al. (2025) describe this as a "double hit"—less metabolically active tissue to absorb glucose, surrounded by adipose tissue that secretes pro-inflammatory adipokines further impairing insulin sensitivity.
The Clinical Relevance of These Mechanisms
Why does this matter practically? Because most current treatment strategies target glucose after it has already failed to enter muscle cells—via sulphonylureas stimulating more insulin release, or SGLT2 inhibitors flushing glucose through urine. These approaches do not address the root dysfunction.
Interventions that target skeletal muscle directly—resistance training, protein optimisation, creatine supplementation, and selected pharmacotherapies—work at the source of the problem. The distinction matters both for efficacy and for long-term outcomes, including preservation of lean mass, functional capacity, and metabolic resilience.
3. Resistance Training as a Metabolic Prescription
Resistance training is not adjunctive therapy. It is a pharmacological-grade intervention for Type 2 Diabetes, with a defined mechanism of action, an optimal dose, and measurable outcomes.
The Mechanism: Insulin-Independent Glucose Clearance
The defining feature of resistance training as a metabolic therapy is this: it activates glucose uptake via pathways that bypass insulin entirely.
During and after resistance exercise, two insulin-independent mechanisms drive GLUT4 translocation to the muscle cell surface:
AMPK activation: Mechanical contraction depletes ATP and raises the AMP:ATP ratio, activating AMP-activated protein kinase (AMPK). AMPK signals GLUT4 translocation directly, without involving the insulin receptor pathway.
Calcium-calmodulin signalling: Muscle contraction triggers calcium release from the sarcoplasmic reticulum, which activates calmodulin-dependent protein kinase (CaMK). This also drives GLUT4 to the cell surface independently of insulin.
The practical consequence: even in individuals with severely impaired insulin signalling, a single resistance training session can clear blood glucose effectively. This is the "secret side door" for glucose entry that no medication fully replicates.
A 2025 biochemistry review by Tabone confirms that mTORC1 (mechanistic target of rapamycin complex 1) also plays a central role, linking mechanical tension in muscle fibres to both protein synthesis and metabolic adaptation, creating a convergence between strength gains and metabolic improvement that is unique to resistance exercise.
The 48-Hour Insulin Sensitivity Window
A critical and often overlooked principle: the metabolic benefit of a resistance training session persists for 24–48 hours post-exercise, primarily via increased glycogen synthase activity and sustained GLUT4 upregulation.
This has a direct clinical implication: training once a week is insufficient to maintain continuous metabolic benefit. The optimal cadence is every 48 hours—three sessions per week—which creates a near-continuous state of enhanced insulin sensitivity.
High-Load vs. Low-Load Training: What the Evidence Shows
Not all resistance protocols deliver equal metabolic benefit. The two most important variables are intensity (percentage of 1-repetition maximum, or 1RM) and volume (total sets × reps × load).
High-Load Training (75% 1RM)
Primary Adaptation: Focuses on myofibrillar hypertrophy (building actual muscle fiber size) and maximum physical strength.
GLUT4 Upregulation: Triggers a robust increase in GLUT4 glucose transporters to help clear blood sugar.
Glycogen Depletion: High overall depletion, specifically targeting powerful Type II muscle fibers.
Best Suited For: Individuals dealing with sarcopenia (age-related muscle loss), reversing insulin resistance, and aging populations.
Recommended Frequency: 2–3 training sessions per week.
Evidence Strength: Strong, backed by multiple Randomized Controlled Trials (RCTs).
Low-Load Training (30–50% 1RM)
Primary Adaptation: Focuses on improving muscular endurance and building metabolic conditioning.
GLUT4 Upregulation: Triggers a moderate-to-high increase in GLUT4 glucose transporters.
Glycogen Depletion: Causes a moderate drop in muscle glycogen stores.
Best Suited For: Fitness beginners and individuals presenting with high cardiovascular risk.
Recommended Frequency: 3–4 training sessions per week.
Evidence Strength: Moderate-to-strong scientific backing.
Clinical commentary: For most patients with Type 2 Diabetes, a pragmatic approach combines moderate-to-heavy loads (65–80% 1RM) with compound multi-joint exercises. This maximises GLUT4 upregulation while providing sufficient mechanical stimulus for hypertrophy of the metabolically critical Type II fibres.
Which Exercises to Prioritise
Compound lower-body exercises are the highest-yield interventions because the major muscle groups of the lower body—quadriceps, hamstrings, glutei—represent the largest absolute mass of skeletal muscle in the body and account for a disproportionate share of glucose disposal capacity.
Priority exercises include: barbell or goblet squat, deadlift (conventional or Romanian), leg press, hip thrust, bent-over row, and bench press. For patients with limited mobility or joint pain, seated leg press, cable rows, and aquatic resistance training are validated alternatives.
Evidence-Based Prescription
Variable Recommendation Frequency 3 sessions/week, approximately every 48 hours Exercise selection ≥2 compound lower-body exercises per session Sets per muscle group 3–4 sets Repetition range 8–12 reps per set Intensity ≥65% 1RM (moderate-to-high effort—approaching muscular fatigue) Rest between sets 60–120 seconds
⚠️ Safety note: Before beginning a resistance training programme, individuals with Type 2 Diabetes should consult their physician, particularly if they have uncontrolled hypertension, retinopathy, neuropathy, or significant cardiovascular risk. Exercise-induced hypoglycaemia is a risk in patients on insulin or sulphonylureas and requires appropriate glucose monitoring and medication adjustment.
4. Protein Strategy: Overcoming Anabolic Resistance
Even an optimal training programme is blunted if protein intake is insufficient—and in Type 2 Diabetes, the required protein intake is significantly higher than in healthy populations.
Understanding Anabolic Resistance
Anabolic resistance is the hallmark of muscle dysfunction in metabolic disease, obesity, and aging. It refers to a reduced responsiveness of skeletal muscle protein synthesis (MPS) to dietary protein and amino acid availability.
In a healthy young adult, consuming 20–25g of high-quality protein reliably triggers a robust MPS response. In an older adult with Type 2 Diabetes, the same dose may produce a blunted response. The muscle's "hearing aid" for protein signals is turned down—a consequence of chronic low-grade inflammation, impaired mTOR signalling, and intramyocellular lipid accumulation (Castillo et al., 2025; Wang et al., 2026).
Overcoming anabolic resistance requires three adjustments: higher total protein intake, optimised protein distribution across the day, and specific amino acid composition at each meal.
Total Daily Protein Intake
Current evidence supports a daily protein target of 1.6–2.2g per kg of body weight for individuals with Type 2 Diabetes who are engaged in resistance training. For those on GLP-1 receptor agonists (which accelerate lean mass loss), the lower bound should be ≥1.6g/kg/day as a minimum protective threshold.
For a 75 kg individual, this translates to approximately 120–165g of protein per day—significantly higher than the 0.8g/kg recommended for sedentary healthy adults and substantially more than the typical intake in most Western dietary patterns.
Protein Distribution: Pulse Feeding Over Bolus
How protein is distributed across meals matters at least as much as the total amount.
Bolus feeding (one or two large meals providing the majority of daily protein) is suboptimal for MPS because the muscle protein synthesis response is time-limited. Even if a single meal provides 80g of protein, MPS cannot be sustained proportionally—amino acid oxidation increases instead.
Pulse feeding (3–4 evenly distributed meals each providing an adequate protein dose) maintains a near-continuous stimulation of MPS throughout the day. Evidence from clinical nutrition supports a per-meal protein target of approximately 0.4g/kg of body weight, which for a 75 kg individual means approximately 30g per meal, three to four times daily.
Meal-Level Protein Composition
Beyond quantity, the amino acid profile of each protein serving determines its MPS-stimulating potency. Essential amino acids (EAAs), which cannot be synthesised by the body, are the primary drivers of MPS. Among EAAs, leucine occupies a unique position as a direct activator of the mTORC1 signalling pathway—acting not merely as a building block but as a molecular signal telling muscle cells to initiate synthesis (Phillips et al., 2023).
Each meal should aim to provide at least 2.5–3g of leucine to cross the activation threshold for mTORC1 in anabolically resistant muscle. This is automatically achieved by approximately 30g of whey protein (which contains ~10–11% leucine by weight), but requires careful planning with plant-based protein sources, which are generally leucine-poor on a per-gram basis.
High-leucine food sources include: whey protein isolate (10–11% leucine), eggs (~8.5%), beef (~8%), chicken (~7.5%), salmon (~7%), and edamame (~7%). Plant sources are typically 5–7% leucine and often require combining or enrichment to meet the threshold.
How to Optimize Intermittent Fasting for Muscle Growth
If you prefer an intermittent fasting lifestyle but want to maximize anabolism, use these three strategies to hack the physiology:
Widen the Window to 8 Hours (16:8): A 4-hour window makes optimal protein spacing impossible. An 8-hour window allows you to comfortably fit 3 distinct protein feedings spaced 3.5 to 4 hours apart (e.g., 12:00 PM, 4:00 PM, and 8:00 PM), hitting the leucine trigger 3 times.
Over-Index on Protein Quality: Ensure your breaking and closing meals are rich in essential amino acids (whey, beef, eggs, or isolated soy/pea protein) to guarantee you hit that 3g leucine threshold per feeding.
Time Your Training Wisely: Avoid lifting weights deep inside your fasting window if you cannot eat for several hours afterward. Try to train right before your eating window opens, or right in the middle of it, so amino acids are immediately available post-workout when muscle sensitivity to protein is at its absolute highest.
5. Targeted Supplementation: Leucine and Creatine
Two supplements stand out from the crowded nutraceutical landscape for their mechanistic specificity, safety profile, and clinical evidence base in the context of skeletal muscle metabolism and Type 2 Diabetes.
Leucine: The mTOR Activation Signal
As outlined above, leucine functions as both a building block and a signalling molecule. At doses of approximately 2.5–3g per meal, it directly activates mTORC1—the master regulator of muscle protein synthesis—in a manner that can partially overcome anabolic resistance (Phillips et al., 2023).
Leucine is especially valuable in three populations: older adults (where anabolic resistance is most pronounced), individuals with Type 2 Diabetes (where chronic inflammation blunts mTOR signalling), and patients on calorie-restricted diets or GLP-1 receptor agonists (where protein synthesis is deprioritised by the catabolic state).
Supplementation approach: If dietary intake does not reliably provide 2.5–3g of leucine per meal, standalone leucine supplementation (available as a powder or capsule) at 2–3g per meal is a practical and low-cost strategy.
Creatine Monohydrate: The Metabolic Amplifier
Creatine monohydrate has one of the largest and most consistent evidence bases of any sports nutrition supplement. In the context of Type 2 Diabetes and skeletal muscle metabolism, its benefits extend well beyond performance enhancement.
Mechanisms relevant to metabolic disease:
Creatine increases intramuscular phosphocreatine stores, which serves as the immediate energy currency for muscle contraction. By expanding this reservoir, creatine reduces the reliance on glycolytic ATP production during high-intensity effort—preserving greater metabolic reserve.
Critically, creatine supplementation has been shown to upregulate GLUT4 expression in skeletal muscle, independently of exercise—directly enhancing the muscle's capacity to uptake glucose from the bloodstream. It also increases intramuscular glycogen storage capacity by approximately 20%, effectively expanding the body's glucose "sink" (Tabone, 2025).
Additionally, creatine promotes intracellular hydration (osmotic effect), which is an independent marker of anabolic state and supports cell volume-sensitive signalling pathways.
Evidence-based dosing: 3–5g of creatine monohydrate per day. No loading phase is required; effects on glycogen capacity and GLUT4 expression accumulate over 4–6 weeks of consistent use. Unflavoured creatine monohydrate powder is the most cost-effective and evidence-supported form.
⚠️ Safety note: Creatine supplementation causes a modest rise in serum creatinine—a standard kidney function marker. This is a direct chemical consequence of creatine metabolism, not a sign of kidney damage. However, in patients with chronic kidney disease (CKD), this can be misinterpreted clinically. Always disclose creatine use to your healthcare team and request a cystatin-C-based kidney function assessment for more accurate evaluation. Creatine is generally well-tolerated in individuals with well-controlled Type 2 Diabetes without CKD.
6. What Your Medications Do to Your Muscles
This section addresses one of the most clinically underappreciated dimensions of metabolic pharmacotherapy: the direct and indirect effects of first-line diabetes medications on skeletal muscle biology.
Metformin: The Complex Relationship with Muscle
Metformin activates AMPK—the cellular energy sensor—which improves mitochondrial function and promotes fatty acid oxidation in skeletal muscle. These are legitimate metabolic benefits.
However, AMPK activation can also partially antagonise mTORC1 signalling, the same pathway required for resistance training–induced muscle protein synthesis and hypertrophy. This theoretical interference has been a source of significant debate in exercise pharmacology.
What the evidence actually shows: Clinical studies examining Metformin's effect on resistance training adaptations show that hypertrophic interference is real but modest in magnitude. The overall metabolic benefits of Metformin in the T2D population—improved mitochondrial efficiency, reduced hepatic glucose output, improved insulin sensitivity—generally outweigh muscle growth concerns, particularly when RT protocols are optimised (Wilkinson et al., 2025).
Practical clinical strategy: Avoid taking Metformin in close temporal proximity to a resistance training session. Taking it with a meal that is several hours from your workout (e.g., taking it at breakfast if you train in the evenings) may reduce AMPK-mTOR interference in the post-exercise window. Do not adjust medication timing without consulting your physician.
GLP-1 Receptor Agonists (Semaglutide, Liraglutide): The Lean Mass Problem
GLP-1 receptor agonists (GLP-1RAs) such as semaglutide (Ozempic, Wegovy) represent one of the most effective weight-loss pharmacotherapies available. However, their effects on body composition deserve explicit clinical attention.
Studies indicate that without targeted protective strategies, 25–40% of total weight lost on GLP-1RAs may come from lean (muscle) tissue rather than adipose tissue. A 2025 longitudinal study by Suzuki et al. tracking patients with Type 2 Diabetes on GLP-1RAs documented functional implications including increased fall risk—a downstream consequence of lean mass reduction.
This does not argue against GLP-1RA use; it argues against GLP-1RA use without concurrent muscle-preserving strategies.
Evidence-based protective co-interventions:
Resistance training throughout the course of GLP-1RA therapy (minimum 3 sessions/week)
Protein intake of ≥1.6g/kg/day, with leucine-rich distribution across meals
Creatine monohydrate supplementation (3–5g/day)
Regular assessment of body composition (DEXA scan) to monitor lean mass preservation, not just total weight
Clinical note: Clinicians prescribing GLP-1RAs should consider co-prescribing structured exercise as part of the treatment plan—not as a lifestyle suggestion, but as a clinical intervention to prevent iatrogenic sarcopenia.
SGLT2 Inhibitors (Empagliflozin, Dapagliflozin): The Fuel-Switch Effect
SGLT2 inhibitors work by causing glycosuria—the excretion of glucose through the kidneys. This mechanism has direct metabolic consequences for skeletal muscle.
By reducing circulating glucose availability, SGLT2 inhibitors promote a metabolic shift toward ketone utilisation in skeletal muscle. This fuel-switching has documented anti-inflammatory properties and may improve mitochondrial efficiency in muscle tissue.
A 2026 systematic review and meta-analysis by Ma et al. confirmed that SGLT2i added to Metformin produces superior glycaemic outcomes versus other add-on agents in Type 2 Diabetes—establishing this combination as a clinically robust dual-therapy approach.
However, SGLT2i have also been associated with modest reductions in lean mass in some patient populations, possibly related to volume depletion and dietary compensation. Combining SGLT2i therapy with resistance training and protein optimisation mitigates this risk.
Summary: Pharmacology × Muscle Biology Interaction Table
Metformin
Primary Muscle Effect: Activates AMPK pathways, which can cause a modest inhibition of mTORC1 signaling post-exercise.
Metabolic Benefit: Enhances mitochondrial efficiency and improves systemic insulin sensitization.
Key Risk: Modest blunting of muscle hypertrophy (growth) signals.
Mitigating Strategy: Time your Metformin dose several hours away from resistance training sessions.
GLP-1 Receptor Agonists (e.g., Semaglutide)
Primary Muscle Effect: Accelerates lean mass loss, with 25–40% of total weight shed potentially coming from muscle tissue.
Metabolic Benefit: Drives significant visceral and adipose tissue reduction alongside robust glucose control.
Key Risk: Accelerates iatrogenic sarcopenia, which elevates overall fall and frailty risk.
Mitigating Strategy: Co-prescribe resistance training (3x/week) + high protein (1.6g/kg/day) + creatine monohydrate (3–5g/day).
SGLT2 Inhibitors (e.g., Empagliflozin)
Primary Muscle Effect: Alters muscle substrate utilization by shifting metabolism toward ketone bodies; can cause a minor reduction in lean mass.
Metabolic Benefit: Delivers potent anti-inflammatory effects, profound cardiorenal protection, and improved glycemic control.
Key Risk: Potential for modest, unintended lean mass reduction.
Mitigating Strategy: Combine therapy with consistent resistance training and aggressive protein optimization.
7. Clinical Validity: Interpreting the Evidence
The science in this field is compelling, but rigorous interpretation requires acknowledging where the evidence is robust and where it has limitations.
Strength of the Evidence Base
Strongest evidence (multiple RCTs, consistent effect across populations):
Resistance training improves insulin sensitivity and HbA1c in Type 2 Diabetes
Protein distribution (0.4g/kg/meal) outperforms bolus feeding for MPS
Creatine monohydrate increases intramuscular glycogen and GLUT4 expression
GLP-1RAs cause significant lean mass loss without co-intervention
SGLT2i + Metformin combination is superior for glycaemic control vs. other dual therapies (Ma et al., 2026)
Moderate evidence (mechanistic data + smaller RCTs):
Leucine threshold dosing for mTOR activation in anabolic resistance (Phillips et al., 2023)
Metformin-exercise timing as a strategy to minimise mTOR interference
ER stress as a pathogenic driver of muscle dysfunction in T2D (Wang et al., 2026)
Emerging/preliminary evidence:
Biomarkers (myostatin, irisin, follistatin) as clinical monitoring tools
CGM-guided exercise prescription
Muscle-specific genetic profiling for training non-response
Key Limitations to Acknowledge
Study duration: Many exercise + nutrition intervention trials in Type 2 Diabetes run for 8–24 weeks. Long-term (>2 year) data on lean mass preservation strategies in combination with GLP-1RA therapy are still limited. The Suzuki et al. (2025) longitudinal data are among the most clinically valuable available, but longer follow-up is needed.
Population heterogeneity: Anabolic resistance varies substantially by age, sex, degree of insulin resistance, and medication burden. Protein thresholds established in older adults may not translate directly to younger populations with T2D.
Mechanistic vs. clinical endpoints: Much of the molecular data (ER stress, mTOR signalling, GLUT4 density) comes from animal models or in vitro studies. Clinical validation in human T2D populations is often limited in scale, though directionally consistent.
Supplement studies: The creatine and leucine evidence base is generally robust in healthy and athletic populations but thinner in patients with Type 2 Diabetes specifically. Extrapolation is reasonable given mechanistic plausibility and safety profiles, but head-to-head RCTs in T2D populations remain underrepresented.
What Clinicians Should Take Away
The mechanistic coherence across studies is striking. Multiple independent lines of evidence—molecular biology, clinical nutrition research, pharmacology, exercise science—converge on the same conclusion: skeletal muscle is the primary site of metabolic pathology in Type 2 Diabetes, and targeted muscle interventions produce measurable, clinically meaningful improvements in glycaemic control, body composition, and functional outcomes.
The evidence base is sufficient to justify a paradigm shift in clinical practice, even while awaiting longer-term confirmatory data.
8. Evidence Summary Table
Resistance Training (3×/week)
Key Evidence: Backed by multiple Randomized Controlled Trials (RCTs) and systematic reviews.
Effect on HbA1c / Glucose: Drives a significant reduction in blood glucose.
Effect on Lean Mass: Actively increases lean muscle mass.
Quality of Evidence: High.
Protein Optimization (≥1.6g/kg/day + pulse feeding)
Key Evidence: Phillips et al. (2023) and ESPEN clinical guidelines.
Effect on HbA1c / Glucose: Indirect benefit by expanding overall muscle mass and glucose disposal capacity.
Effect on Lean Mass: Preserves and increases lean mass.
Quality of Evidence: High.
Leucine Supplementation (2.5–3g/meal)
Key Evidence: Phillips et al. (2023).
Effect on HbA1c / Glucose: Indirect benefit via maximized Muscle Protein Synthesis (MPS) and subsequent muscle-driven glucose clearance.
Effect on Lean Mass: Increases MPS, effectively overcoming diabetes-induced anabolic resistance.
Quality of Evidence: Moderate-to-High.
Creatine Monohydrate (3–5g/day)
Key Evidence: Tabone (2025) alongside multiple sports science RCTs.
Effect on HbA1c / Glucose: Delivers a modest direct improvement via upregulation of GLUT4 transporters.
Effect on Lean Mass: Increases muscular glycogen capacity and provides a modest lean mass benefit.
Quality of Evidence: Moderate.
Metformin
Key Evidence: Established first-line diabetes therapy.
Effect on HbA1c / Glucose: Drives a significant reduction, typically lowering HbA1c by 1.0% to 1.5%.
Effect on Lean Mass: Exhibits a minimal negative effect at standard clinical doses.
Quality of Evidence: High.
GLP-1RAs (e.g., Semaglutide)
Key Evidence: Suzuki et al. (2025) alongside major cardiovascular outcome trials.
Effect on HbA1c / Glucose: Exceptional blood sugar management, reducing HbA1c by 1.0% to 2.0%.
Effect on Lean Mass: Causes a 25–40% reduction in total weight lost from lean mass if used without muscle-protective interventions.
Quality of Evidence: High.
SGLT2i (e.g., Empagliflozin) + Metformin
Key Evidence: Ma et al. (2026) systematic review.
Effect on HbA1c / Glucose: Offers superior glycemic control compared to other standard dual add-on therapies.
Effect on Lean Mass: A modest reduction in lean mass is possible due to altered substrate utilization.
Quality of Evidence: High.
GLP-1RA + Resistance Training + Protein Protocol
Key Evidence: Emerging clinical data and strong mechanistic rationale.
Effect on HbA1c / Glucose: Yields superior glycemic and body composition outcomes compared to utilizing a GLP-1RA alone.
Effect on Lean Mass: Successfully preserves lean mass during rapid fat and weight loss.
Quality of Evidence: Moderate (and growing).
9. Common Myths and Mistakes
Myth 1: "Cardio is better than weights for blood sugar control."
Both aerobic and resistance training improve glycaemic control. However, resistance training uniquely builds and preserves skeletal muscle mass—the body's primary glucose storage tissue. Current evidence supports combined aerobic-resistance training as the gold standard for T2D management, but if only one modality is possible, resistance training's effects on lean mass make it particularly valuable in sarcopenic populations.
Myth 2: "I'm losing weight on Ozempic, so I must be getting healthier."
Weight loss alone is not a complete surrogate for metabolic health. If a significant portion of weight lost comes from skeletal muscle rather than adipose tissue, the metabolic rate falls, the glucose disposal capacity shrinks, and long-term metabolic resilience is reduced—even as the number on the scale improves. Body composition monitoring, not just weight, is essential.
Myth 3: "Creatine is for athletes and bodybuilders, not diabetes patients."
This reflects an outdated understanding of creatine's mechanisms. Its ability to upregulate GLUT4 expression, expand intramuscular glycogen capacity, and improve bioenergetics is directly relevant to the metabolic impairments in Type 2 Diabetes—independent of any athletic application.
Myth 4: "More protein means more muscle, so I should eat as much protein as possible."
Total intake matters, but distribution matters more than most patients realise. Consuming 150g of protein in one or two meals produces significantly less MPS stimulation than the same 150g distributed across four evenly spaced meals. The anabolic ceiling per meal is real; exceeding it by doubling the dose does not double the benefit.
Myth 5: "Metformin and exercise don't mix."
They can and should coexist. The concern is specifically about the potential interference of Metformin with the post-exercise anabolic window—a concern that is real but modest in magnitude. The solution is strategic timing, not avoidance.
Mistake: Training intensely once a week and expecting sustained metabolic benefit.
Given the 24–48-hour duration of post-exercise insulin sensitivity enhancement, once-weekly training allows that benefit to dissipate for 5–6 days before being renewed. Three sessions per week spaced approximately 48 hours apart, is the minimum threshold for sustained metabolic benefit.
10. Practical Protocol: Where to Start Today
This is a structured roadmap designed for clinicians to share with patients, or for motivated patients to discuss with their healthcare team.
Step 1: Audit your protein distribution. Track 3 days of eating using Cronometer or MyFitnessPal. Check whether you are consistently reaching 30g of protein at each main meal (breakfast, lunch, dinner). Breakfast is where most people fall short. Add eggs, Greek yoghurt, cottage cheese, or a whey protein shake.
Step 2: Begin a 3-session-per-week resistance training programme. You do not need a gym. Bodyweight squats, lunges, push-ups, and hip hinges performed to near-muscular fatigue (you should struggle on reps 10–12) activate GLUT4 and AMPK pathways effectively. Progress to loaded exercises as capacity allows. Space sessions approximately 48 hours apart.
Step 3: Add creatine monohydrate (3–5g/day). Mix into water, juice, or a protein shake. Unflavoured powder is the most economical form. Allow 4–6 weeks for glycogen-capacity and GLUT4 benefits to accumulate.
Step 4: Optimise leucine at every meal. Ensure each protein serving contains at least 2.5–3g of leucine. Use whey isolate, eggs, or beef as anchor proteins. If using plant proteins predominantly, consider adding a 2g leucine supplement to each main meal.
Step 5: Discuss medication timing with your physician. If you are on Metformin, ask whether adjusting the timing (taking it several hours from your workout) might be appropriate. Do not adjust medication independently.
Step 6: Consider a 2–4 week CGM trial if eligible. Many endocrinologists now offer short-term continuous glucose monitor use for patients with pre-diabetes or T2D. This generates real-time data on how specific meals, workouts, and medication timings affect your glucose curve—enabling precision adjustments.
Step 7: Request a body composition assessment. A DEXA scan provides appendicular lean mass index (ALMI)—the clinical standard for assessing sarcopenia. Grip strength measurement is a low-cost surrogate. If you are on a GLP-1RA, baseline and repeat DEXA monitoring at 6-month intervals is clinically justified to monitor lean mass preservation.
11. Precision Medicine and the Future of Muscle-Centric Care
Genetic Non-Response: Why Some People Don't Adapt
Approximately 15–20% of individuals show minimal muscle mass or metabolic response to standard resistance training protocols. This is not a failure of effort—it reflects biological variation in pathways involving the ACTN3 gene (associated with fast-twitch fibre composition), IGF-1 receptor sensitivity, and myosin heavy chain isoform distribution.
Identifying genetic non-responders allows clinicians to adjust to higher-volume higher-frequency protocols, or pivot to HIIT as an alternative metabolic stimulus. Consumer-facing genomic panels increasingly include these markers, and their integration into metabolic medicine is moving from research to practice.
Emerging Biomarkers of Muscle Health
Three biomarkers are gaining clinical traction for monitoring skeletal muscle health in metabolic disease:
Myostatin: A muscle-growth inhibitor; elevated levels predict sarcopenia risk and blunted training response. Myostatin inhibitors are currently in clinical trials.
Follistatin: Myostatin's natural antagonist. Higher follistatin-to-myostatin ratios correlate with greater muscle mass and insulin sensitivity. Resistance training and protein intake both raise follistatin.
Irisin: A myokine released during exercise that drives adipose tissue browning (conversion to metabolically active fat). Low irisin levels associate with insulin resistance; resistance training is the most reliable way to elevate them.
12. FAQs
Q: How much resistance training do I need to improve insulin sensitivity in Type 2 Diabetes?
Evidence supports a minimum of two to three sessions per week, spaced approximately 48 hours apart. This spacing is critical because the post-exercise insulin sensitivity window peaks between 24–48 hours and then declines. Three sessions per week maintains near-continuous enhanced insulin sensitivity. Each session should include at least two compound lower-body exercises and target 6–9 working sets per muscle group performed at moderate-to-high intensity (near muscular fatigue). Quality of effort matters as much as session count.
Q: I'm on Ozempic and losing weight fast. How do I know if I'm losing muscle?
Without deliberate muscle-preserving strategies, 25–40% of weight lost on GLP-1RAs may come from lean tissue (Suzuki et al., 2025). Warning signs include disproportionate loss of strength relative to weight, increased fatigue during daily activities, and grip strength decline. The most accurate assessment is a DEXA scan at baseline and every 6 months. Protective strategies—resistance training throughout GLP-1RA therapy, ≥1.6g/kg/day protein, leucine-optimised meals, and creatine supplementation—should be initiated from day one of treatment, not added reactively.
Q: Can I take creatine if I have Type 2 Diabetes or kidney concerns?
Creatine is generally considered safe in well-controlled Type 2 Diabetes, and its GLUT4-upregulating and glycogen-expanding effects are directly beneficial. The key caveat: creatine supplementation elevates serum creatinine—a routine kidney function marker—which can be falsely interpreted as kidney deterioration. If you have existing CKD, disclose creatine use to your healthcare team and request cystatin-C-based kidney function assessment, which is not affected by creatine metabolism. In well-managed T2D without CKD, the risk-benefit calculation strongly favours supplementation.
Q: Does Metformin interfere with muscle building from exercise?
The interference is mechanistically real (AMPK vs. mTOR) but clinically modest in most patients. Multiple studies suggest the metabolic benefits of Metformin—improved mitochondrial function, enhanced insulin sensitivity—generally outweigh muscle growth concerns, particularly in T2D populations. A practical strategy is temporal separation: avoid taking Metformin immediately before or after resistance training. Always consult your physician before adjusting timing.
Q: What is anabolic resistance and how do I overcome it?
Anabolic resistance is the reduced responsiveness of skeletal muscle to protein intake—a hallmark of aging, obesity, Type 2 Diabetes, and inactivity. Strategies to overcome it include: increasing leucine content per meal to at least 2.5–3g, distributing protein evenly across 3–4 meals rather than concentrating it in one or two, performing resistance training regularly (which independently sensitises muscle to protein), and considering EAA supplementation between meals if dietary intake is insufficient.
Q: What blood tests should I ask for to assess muscle health?
Beyond standard metabolic panels, ask about: myostatin and follistatin (increasingly available at metabolic clinics), irisin, DEXA scan for appendicular lean mass index (ALMI), and grip strength measurement as a low-cost functional proxy. In T2D patients on GLP-1RAs, HbA1c alone is insufficient—body composition monitoring is essential.
Q: Can I do resistance training if I have joint pain or mobility limitations?
Yes—and this population particularly needs the metabolic benefits. Practical alternatives include: seated resistance exercises (leg press, cable rows, seated chest press), aquatic resistance training (buoyancy reduces joint load while resistance remains effective), blood flow restriction (BFR) training using low loads (20–30% 1RM) with partial blood flow occlusion to achieve hypertrophy stimulus, and electrical muscle stimulation (EMS) for extreme mobility limitations. Work with a physiotherapist or exercise physiologist to design a protocol that remains effective for glucose metabolism.
Q: Is aerobic exercise or resistance training better for blood sugar control?
Both improve glycaemic control through different mechanisms. Aerobic exercise primarily enhances mitochondrial capacity and oxidative fat metabolism. Resistance training primarily expands GLUT4 density, glycogen storage capacity, and muscle mass. Current evidence supports combined aerobic-resistance training as the gold standard for T2D management. If only one modality is feasible, resistance training's effects on lean mass preservation make it particularly valuable in older adults and those with sarcopenic obesity.
Q: How long before I see metabolic improvements from resistance training?
GLUT4 translocation and acute insulin sensitivity improvement occur after a single session. Sustained glycogen storage expansion requires consistent training for 2–4 weeks. Measurable HbA1c improvements typically require 8–12 weeks of consistent resistance training. Structural hypertrophy of Type II fibres becomes detectable on imaging after 6–12 weeks. The metabolic benefits begin immediately; the structural changes take months—but both are clinically meaningful.
13. Conclusion and Action Steps
The evidence is clear. Skeletal muscle is not a peripheral feature of Type 2 Diabetes—it is the central organ of the disease.
Nearly 80% of postprandial glucose disposal depends on muscle function. When that function deteriorates through inactivity, aging, chronic overnutrition, or ER stress and lipotoxicity, hyperglycaemia is the inevitable result. When it is restored through targeted resistance training, protein optimisation, and strategic supplementation, the metabolic consequences are measurable and clinically significant.
Medications like Metformin, Semaglutide, and Empagliflozin are powerful tools. But none of them builds muscle. None restores GLUT4 density. None expands the body's glucose storage sink. And two of the three—GLP-1RAs and SGLT2i—risk shrinking the very tissue that defines long-term metabolic resilience.
The paradigm shift required is not radical. It is practical: prescribe resistance training with the precision of a medication. Monitor protein intake as carefully as HbA1c. Assess body composition, not just body weight. Evaluate every medication through the lens of what it does to muscle.
Your action steps this week:
Audit your protein distribution at each meal (aim for ≥30g per meal, 3–4 times daily)
Schedule your first resistance training session (or modify your current programme to include lower-body compound movements)
Start creatine monohydrate at 3–5g/day
Optimise leucine at each meal (2.5–3g minimum)
Discuss medication timing with your physician if you are on Metformin
If on a GLP-1RA, request a DEXA scan to establish a lean mass baseline
Share this framework with your diabetes care team
Consult your physician or registered dietitian before making changes to your exercise programme, protein intake, supplementation, or medication timing. Individuals with Type 2 Diabetes should have their exercise programme reviewed in the context of their complete medical history, current medications, and cardiovascular risk profile.
This article is intended for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before beginning a new exercise or nutrition program, especially if you have an existing medical condition.
Related Articles
How Strong Legs Protect Your Brain, Metabolism, Blood Sugar, and Mobility as You Age
You’re Missing This: Why mTOR Activation Is the Real Goal of Strength Training | DR T S DIDWAL
The mTOR Switch: Why Your Cells Stopped Listening to Insulin | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
References
Lin, D. (2026). Skeletal muscle metabolism in health and disease: Mechanisms, interventions, and clinical perspectives. iScience, 29(3), Article 115024. https://doi.org/10.1016/j.isci.2026.115024
Wang, X., Li, M., Chi, Z., Wang, M., Liu, J., Li, A., Song, B., & Tong, L. (2026). Endoplasmic reticulum stress in skeletal muscle dysfunction of type 2 diabetes: Mechanisms and therapeutic implications. Frontiers in Endocrinology, 17, 1769545. https://doi.org/10.3389/fendo.2026.1769545
Wilkinson, M. S., Rollin, T. A., Kuriakose, M., Haggerty-Goede, R. A. L., Miller, D. M., & Dunham-Snary, K. J. (2025). Redox homeostasis in metabolic syndrome and type II diabetes: Role of skeletal muscle and impact of gold-standard treatments. International Journal of Molecular Sciences, 26(21), 10370. https://doi.org/10.3390/ijms262110370
Castillo, Í. M. P., Argilés, J. M., Rueda, R., et al. (2025). Skeletal muscle atrophy and dysfunction in obesity and type-2 diabetes mellitus: Myocellular mechanisms involved. Reviews in Endocrine and Metabolic Disorders, 26, 815–836. https://doi.org/10.1007/s11154-025-09954-9
Tabone, M. (2025). Muscle mechanics in metabolic health and longevity: The biochemistry of training adaptations. BioChem, 5(4), 37. https://doi.org/10.3390/biochem5040037
Phillips, B. E., Breen, L., & Atherton, P. J. (2023). A focus on leucine in the nutritional regulation of human skeletal muscle protein synthesis. Clinical Nutrition, 42(11), 2305–2313. https://doi.org/10.1016/j.clnu.2023.08.030
Deutz, N. E. P., Bauer, J. M., Barazzoni, R., Biolo, G., Boirie, Y., Bosy-Westphal, A., Cederholm, T., Cruz-Jentoft, A., Krznarić, Ž., Nair, K. S., Singer, P., Teta, D., Tipton, K., & Calder, P. C. (2023). Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clinical Nutrition, 42(11). https://doi.org/10.1016/j.clnu.2023.10.xxx
Suzuki, Y., Suzuki, H., Maruo, K., et al. (2025). Longitudinal association of SGLT2 inhibitors and GLP-1RAs on falls in persons with type 2 diabetes. Scientific Reports, 15, 9178. https://doi.org/10.1038/s41598-025-91101-0
Ma, Y., Lin, Y., Ding, X., & Peng, Y. (2026). Comparing SGLT2i and other oral antidiabetic drugs as dual therapy add-on to Metformin in type 2 diabetes: A systematic review and meta-analysis. Endocrinology, Diabetes & Metabolism, 9(2), e70176. https://doi.org/10.1002/edm2.70176
Li, G., Li, Z., & Liu, J. (2024). Amino acids regulating skeletal muscle metabolism: Mechanisms of action, physical training dosage recommendations and adverse effects. Nutrition & Metabolism (London), 21, 41. https://doi.org/10.1186/s12986-024-00820-0
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making changes to your exercise regimen, dietary intake, supplementation, or medication. The evidence cited reflects the state of the scientific literature as of mid-2026; as an evolving field, readers should verify recommendations against current clinical guidelines.
Author: Dr. T.S. Didwal, M.D. (Internal Medicine) | Last updated: 2026