The Diabetes Protein Guide: What to Eat, How Much You Need, and How It Affects Blood Sugar
Discover how much protein to eat with diabetes, which sources protect your heart and kidneys, and what 2025–2026 research reveals about blood sugar control.
DIABETESNUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/15/202625 min read

How Much Protein Do You Need If You Have Diabetes?
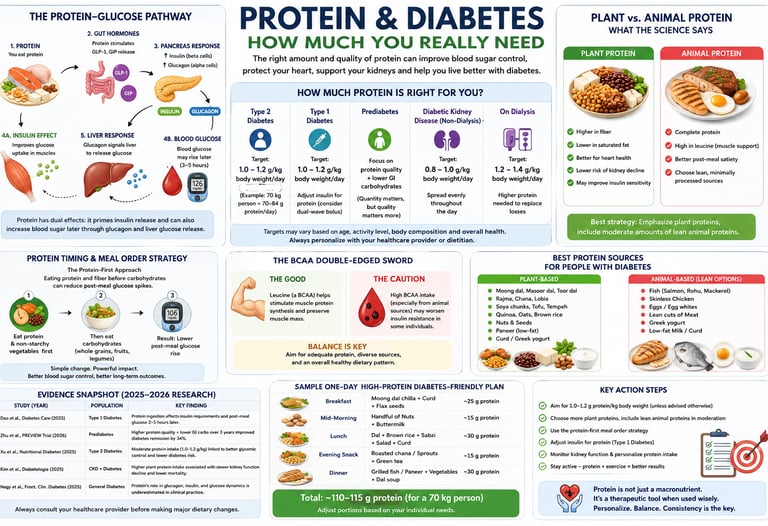
For most adults with Type 2 or Type 1 diabetes who have normal kidney function, the evidence-based recommendation is to consume 1.0 to 1.2 grams of protein per kilogram of body weight daily (roughly 70–84 grams of protein per day for a 70 kg / 154 lb person). If you live an active lifestyle or engage in regular strength training, your daily target increases to 1.2 to 1.6 grams per kilogram.
However, if you have Chronic Kidney Disease (CKD)—a common complication of diabetes—you must reduce your intake to a strict 0.6 to 0.8 grams per kilogram daily under medical supervision to slow kidney decline and prevent hyperfiltration damage.
Key takeaways
1. Protein is Not a "Free Food" for Blood Sugar
While carbohydrates cause immediate glucose spikes, dietary protein triggers glucagon release, prompting the liver to secrete stored glucose. Clinical data from a 2025 Frontiers review confirms that high-protein, low-carb meals cause a delayed, measurable rise in blood sugar 3 to 5 hours after eating, meaning protein must be factored into comprehensive glycemic management plans.
2. Clinical Protein Targets Vary by Diabetes Diagnosis
Medical consensus dictates that daily protein targets cannot be generalized. For standard Type 2 Diabetes, an intake of 1.0–1.2 g per kilogram of body weight optimizes muscle preservation and glycemic control. However, if Chronic Kidney Disease (CKD) is present, targets must be strictly restricted to 0.6–0.8 g/kg/day under the supervision of a renal dietitian to prevent organ hyperfiltration.
3. Type 1 Diabetes Regimens Require "Protein Counting"
Landmark 2025 research published in Diabetes Care proves that protein ingestion significantly alters postprandial insulin requirements. Individuals managing Type 1 Diabetes via continuous glucose monitors (CGMs) or insulin pumps frequently require a delayed, "dual-wave" or "square-wave" bolus to safely cover the slow, late glucose rise triggered by protein hours after consumption.
4. Plant Protein Is Superior to Red Meat for Insulin Sensitivity
In rigorous multi-cohort substitution models (Nutritional Diabetes, 2025), replacing equal calories of processed red meat with whole plant proteins—specifically legumes like lentils and chickpeas—dramatically improves baseline insulin sensitivity, lowers blood pressure, and reduces systemic inflammatory markers in Type 2 Diabetes.
5. Legumes are the Premier Whole-Food Protein Option
Legumes (dal, beans, peas) outperform animal proteins in metabolic trials because they deliver protein bundled with viscous soluble fiber and resistant starch. This natural matrix slows down gastric emptying, selectively feeds beneficial gut microbiota, and blunts post-meal glucose spikes, aligning perfectly with international diabetes nutritional guidelines.
6. The "Protein-First" Meal Order Flattens Glucose Spikes
Consuming your protein and vegetable portions 5 to 10 minutes before eating carbohydrates physically alters digestion kinetics. This precise eating sequence triggers early gut hormone release (specifically GLP-1), priming the pancreas to secrete insulin in advance and reducing subsequent post-meal glucose peaks by 20% to 30%.
7. Unused BCAAs Act as a Metabolic Block to Insulin
Mechanistic evidence (Frontiers in Nutrition, 2024) reveals a metabolic paradox: while Branched-Chain Amino Acids (BCAAs) found in whey and red meat support muscle synthesis when paired with resistance exercise, they are harmful when sedentary. In the context of low activity and excess calories, circulating BCAAs pile up in the blood, chronically activating mTOR and physically jamming the cellular signals that tell muscles to absorb glucose.
8. Combined Diet Quality Drives Prediabetes Remission
Long-term data from the landmark, multinational PREVIEW trial (2026) demonstrate that reversing prediabetes is not achieved by altering macronutrient quantities alone. A high-quality, moderate-to-high protein diet combined exclusively with low-glycemic index (low-GI) complex carbohydrates yields the highest rates of clinical prediabetes remission by simultaneously repairing pancreatic beta-cell secretion capacity and peripheral insulin sensitivity.
Introduction
If you have diabetes, you've probably spent a lot of time counting carbohydrates. But here's what most diabetes education misses: protein is not a "free" food, and the latest science is rewriting the rules around how it interacts with your blood sugar, insulin, and long-term health.
A landmark 2025 study in Diabetes Care confirmed that protein ingestion produces measurable effects on insulin requirements and glucose dynamics in people with type 1 diabetes—something many patients have never been told (Dao et al., 2025). Meanwhile, a 2026 multinational diabetes prevention trial found that the quality of dietary protein and carbohydrate, not just quantity, determines whether people with prediabetes can reverse course entirely (Zhu et al., 2026).
Whether you have type 1 diabetes, type 2 diabetes, prediabetes, or diabetic kidney disease, this guide gives you an evidence-based, fully personalized framework for using dietary protein as a therapeutic tool—not just a macronutrient afterthought.
In this guide, you'll learn:
How much protein is optimal for your specific type of diabetes
Why protein source (plant vs. animal) matters more than most people realize
How protein affects glucagon, insulin, and post-meal glucose spikes
The kidney safety question—answered with real data
Practical meal strategies grounded in the latest 2025–2026 research
1. Why Protein Matters for Blood Sugar Control
Most diabetes nutrition education begins and ends with carbohydrate counting. This approach is incomplete.
Protein interacts with glucose metabolism through several distinct pathways. When you eat protein, your gut releases hormones including GLP-1 (glucagon-like peptide-1), which primes your pancreas to release insulin before carbohydrates even enter your bloodstream. At the same time, protein stimulates glucagon release from the alpha cells of the pancreas—a hormone that signals the liver to release stored glucose.
This dual hormonal response means that:
High-protein meals without carbohydrates can still raise blood glucose, typically 3–5 hours later, due to glucagon-driven hepatic glucose release
Protein eaten before carbohydrates in a meal can meaningfully blunt the post-meal glucose spike
The source and speed of protein digestion influences how strongly these hormonal signals fire
A 2025 review in Frontiers in Clinical Diabetes and Healthcare by Nagy, Turner, and Riddell synthesized the mechanisms linking protein intake to glucagon, insulin, and glucose dynamics, concluding that protein's effect on diabetes management has been systematically underestimated in clinical practice (Nagy et al., 2025/2026).
The global diabetes burden makes this research urgent. Over 400 million people worldwide live with diabetes, including more than 77 million in India alone. Optimizing every dietary lever—including protein—is essential for reducing complications and improving quality of life.
2. How Much Protein Should You Eat with Diabetes?
There is no single protein target that works for every person with diabetes. The right amount depends on your type of diabetes, kidney function, body composition, and activity level.
Here are the evidence-based general targets:
For Type 2 Diabetes (without kidney disease)
Target: 1.0–1.2 g per kilogram of body weight per day
A large registry-based cohort study and meta-analysis published in Nutritional Diabetes (Xu et al., 2025) found that moderate protein intake—particularly when it replaces refined carbohydrates—is associated with lower type 2 diabetes risk and better glycemic control. Going well above 1.2 g/kg does not appear to provide additional metabolic benefit for most people, and extremely high intake from processed animal sources may be harmful.
Practical example: A 70 kg (154 lb) person with type 2 diabetes should aim for approximately 70–84 grams of protein per day.
For Type 1 Diabetes
Target: 1.0–1.2 g/kg/day, with insulin dose adjustment
People with type 1 diabetes need to account for protein in their bolus insulin calculations, not just carbohydrates. Research by Dao et al. (2025) showed that protein ingestion significantly affects post-meal glucose patterns in type 1 diabetes. Many individuals need a delayed or "dual-wave" insulin bolus to cover the slower glucose rise that protein triggers 2–5 hours after eating.
For Prediabetes
Target: Prioritize protein quality over strict quantity
The PREVIEW trial—a multinational randomised diabetes prevention trial—found that higher protein intake combined with lower-glycemic-index carbohydrates over 3 years significantly increased the likelihood of prediabetes remission compared with a moderate-protein, moderate-glycemic-index diet (Zhu et al., 2026). Protein quality and carbohydrate quality together drove the benefit, not protein quantity alone.
For Diabetes with Chronic Kidney Disease (CKD)
Target: 0.6–0.8 g/kg/day
This is covered in detail in the kidney disease section below.
For Physically Active People with Diabetes
Target: 1.2–1.6 g/kg/day
Higher protein intake is appropriate for people with diabetes who engage in regular resistance or endurance training. Distribute intake across meals and time at least one protein-containing snack or meal within 2 hours after exercise.
3. The Science: What Recent Studies Actually Show
Study 1: Protein and Type 1 Diabetes Glucose Control (Dao et al., 2025)
Published in Diabetes Care, this study specifically examined how protein ingestion affects insulin requirements and blood glucose patterns in people with type 1 diabetes.
Key finding: Protein does not just contribute calories—it alters the insulin dosing landscape. Protein-induced glucagon secretion can prevent hypoglycemia in some scenarios but complicate control in others. Individuals on insulin pumps or using CGM (continuous glucose monitors) are best positioned to observe and respond to these patterns in real time.
Clinical implication: Diabetes education programs should incorporate protein counting alongside carbohydrate counting, especially for those on intensive insulin regimens.
Study 2: Dietary Protein and Type 2 Diabetes Risk—Registry Cohort and Meta-Analysis (Xu et al., 2025)
Published in Nutritional Diabetes, this study combined data from a large registry-based cohort with a meta-analysis of prospective cohort studies.
Key finding: Moderate protein intake reduces type 2 diabetes risk when it displaces refined carbohydrates. Plant-based proteins—especially from legumes—provided superior protection compared to red and processed meats.
Clinical implication: Food source matters as much as grams of protein. A gram of protein from lentils and a gram from a processed sausage are not metabolically equivalent.
Study 3: Protein, Amino Acids, and T2D Mechanisms (Mensink, 2024)
This Frontiers in Nutrition review examined the biochemical pathways linking specific amino acids to insulin secretion and glucose homeostasis.
Key finding: Branched-chain amino acids (BCAAs) stimulate insulin secretion but can impair insulin signaling when chronically elevated in the context of high caloric intake and low physical activity. Fast-digesting proteins (whey) produce rapid insulin spikes; slow-digesting proteins (casein, legume proteins) produce more gradual responses.
Clinical implication: Protein processing and digestion speed influence glycemic management. Whole food proteins typically digest more slowly and produce gentler glycemic responses than protein powders and isolates.
Study 4: Whey vs. Pea Protein Insulinogenic Effects (Thondre et al., 2026)
Published in PLOS ONE, this randomized controlled trial in healthy participants compared the insulinogenic effects of whey protein and pea protein when co-ingested with glucose.
Key finding: Both whey and pea protein augmented the insulin response to glucose, but with different kinetics. Pea protein demonstrated a sustained insulinogenic effect consistent with its slower digestion profile, which may benefit post-meal glucose control.
Clinical implication: Plant-based protein sources like peas are not inferior to whey protein for metabolic purposes—and may offer advantages for people with diabetes who benefit from slower, steadier insulin release.
Study 5: Animal vs. Plant Protein and Cardiometabolic Risk (Namazi et al., 2025)
Published in the Journal of Diabetes and Metabolic Disorders, this study used isoenergetic substitution models—replacing one food with an equal number of calories from another—to precisely quantify the effect of protein source in people with type 2 diabetes.
Key finding: Replacing processed red meat with plant-based protein improved insulin sensitivity, reduced triglycerides, lowered blood pressure, reduced inflammatory markers, and improved cholesterol profiles. Among animal proteins, fish and poultry outperformed red meat. Whole-food legume proteins outperformed isolated plant protein supplements.
Study 6: Protein Restriction in Diabetic Kidney Disease (Liu et al., 2025)
This 10-year retrospective cohort study published in BMC Nutrition followed people with both type 2 diabetes and CKD.
Key finding: Long-term protein restriction to 0.6–0.8 g/kg/day slowed CKD progression, reduced proteinuria, improved blood pressure, and better-controlled blood glucose—without compromising nutritional status when plant-based proteins replaced higher quantities of animal proteins.
Study 7: PREVIEW Trial—Protein Quality and Prediabetes Remission (Zhu et al., 2026)
This landmark multinational randomized trial (Diabetologia, 2026) tested whether dietary protein content and carbohydrate glycemic index could prevent progression from prediabetes to type 2 diabetes over 3 years.
Key finding: A high-protein, low-GI diet led to significantly greater rates of prediabetes remission compared to a moderate-protein, moderate-GI diet. The effect was driven by improvements in both insulin secretion capacity and insulin sensitivity, emphasizing that combined dietary quality—protein and carbohydrates—is what moves the metabolic needle most.
General diabetes (normal kidney function): No specific protein gram target is mandated. Focus on overall healthy eating patterns. Individualize based on needs, preferences, and goals. For older adults: at least 0.8 g/kg body weight/day (or 15–20% of calories) to preserve lean muscle mass.
Diabetes with CKD (stage G3 or higher, non-dialysis): Protein intake of 0.8 g/kg/day (recommended daily allowance). Do not routinely restrict below 0.8 g/kg/day, as it does not improve blood glucose, cardiovascular risk, or GFR decline. Higher intakes (>1.3 g/kg/day or >20% of calories) should be avoided.
On dialysis: Consider 1.0–1.2 g/kg/day to prevent protein-energy wasting.
4. Plant vs. Animal Protein: Which Is Better for Diabetes?
This question has a nuanced, evidence-based answer: it depends on what you're replacing and which animal protein you're comparing.
When Plant Protein Wins
Legumes—lentils, chickpeas, black beans, kidney beans—don't just deliver protein. They come packaged with:
Viscous soluble fiber: Slows gastric emptying, blunts post-meal glucose spikes
Resistant starch: Acts as a prebiotic, improving gut microbiome diversity linked to insulin sensitivity
Magnesium and polyphenols: Independently associated with lower T2D risk
Lower saturated fat: Reduces cardiovascular risk, which is already elevated in people with diabetes
Multiple studies, including Namazi et al. (2025) and Xu et al. (2025), found that replacing red and processed meat with legumes improved blood glucose control, reduced cardiovascular risk markers, and lowered inflammatory markers.
When Quality Animal Protein Is Appropriate
Not all animal protein is equal. The research consistently distinguishes:
How Different Animal Proteins Affect Diabetes and Metabolism
Processed Red Meat (Bacon, Sausage, Deli Meats): Highly Harmful. Consistently linked to a significantly higher risk of type 2 diabetes, worsened insulin sensitivity, and increased markers of systemic inflammation.
Unprocessed Red Meat (Steak, Beef, Lamb): Neutral to Modestly Negative. While not as damaging as processed varieties, high intake can still modestly hinder insulin sensitivity and increase long-term cardiovascular risk.
Skinless Poultry (Chicken, Turkey): Neutral to Mildly Favorable. A clean source of lean protein that does not negatively impact glucose control, making it a reliable, blood-sugar-neutral option when baked or grilled.
Fatty Fish (Salmon, Sardines, Mackerel): Highly Favorable. Packed with potent omega-3 fatty acids that actively reduce systemic inflammation, protect blood vessels, and support overall insulin sensitivity.
Whole Eggs: Neutral to Mildly Favorable. When consumed as a whole food, eggs do not disrupt blood glucose and provide an excellent source of slow-digesting protein and vital micronutrients located in the yolk.
Fermented Dairy (Greek Yogurt, Cottage Cheese, Curd): Favorable. Rich in slow-digesting casein proteins, calcium, and gut-healthy probiotics that promote prolonged satiety and support a healthy metabolic profile.The Iso-Energetic Substitution Principle
The iso-energetic substitution models used by Namazi et al. (2025) show that it's not enough to just add plant protein—the benefit comes from replacing lower-quality protein sources with higher-quality ones, calorie for calorie. Simply adding legumes on top of an already high red-meat diet doesn't confer the same benefit.
Practical rule of thumb: Try replacing one serving of red or processed meat per week with a legume-based meal. Research suggests this single swap produces measurable improvements in insulin sensitivity within weeks.
5. Protein and Diabetic Kidney Disease
Approximately 30–40% of people with diabetes eventually develop chronic kidney disease (CKD). When kidney disease is present, protein management becomes a separate clinical equation.
Why Restrict Protein in CKD?
Healthy kidneys filter metabolic waste products produced when your body breaks down protein—primarily urea and creatinine. In early diabetic kidney disease, the kidneys enter a state of hyperfiltration: they work in overdrive to handle the increased metabolic load. High dietary protein accelerates this hyperfiltration, effectively wearing out the kidneys faster.
The Liu et al. (2025) 10-year cohort study demonstrated that restricting protein to 0.6–0.8 g/kg/day in people with type 2 diabetes and CKD:
Slowed progression to advanced CKD stages
Reduced proteinuria (protein in the urine, a marker of kidney damage)
Lowered blood pressure
Improved blood glucose control
Critically, this protective benefit was maintained without nutritional compromise—provided that plant-based proteins (which generate less nitrogen waste per gram than animal proteins) made up a significant portion of the diet.
Who Should Restrict Protein?
Do not self-restrict protein if you have diabetes and CKD. The appropriate target depends on your specific stage of kidney disease (eGFR level), whether you are on dialysis, your nutritional status, and other factors. Work with a renal dietitian for individualized guidance.
CKD Stages 1–2 (eGFR > 60): Standard diabetes protein targets may still apply
CKD Stages 3–4 (eGFR 15–59): Protein restriction (0.6–0.8 g/kg/day) is generally recommended
CKD Stage 5 / Dialysis: Higher protein intake is often required to compensate for dialysis-related losses—the restriction strategy reverses
Plant Protein Advantage in CKD
Plant proteins have a lower protein nitrogen appearance rate than animal proteins, meaning they produce less uremic waste per gram. This makes legumes, tofu, tempeh, and whole grains particularly valuable for people managing both diabetes and CKD.
6. Protein Timing and Meal Order Strategy
When you eat protein—and what you eat it with—can be as important as how much you eat.
Spreading Protein Throughout the Day
Research consistently shows that distributing protein evenly across 3–4 meals produces better outcomes than concentrating it in one sitting. Muscle protein synthesis—which matters for insulin sensitivity because muscle is the body's primary glucose disposal organ—is maximized when protein is spread across the day rather than consumed primarily at dinner, which is the pattern in most Western and South Asian diets.
Target: Aim for 20–30 g of protein per meal across 3 meals, rather than 10 g at breakfast, 15 g at lunch, and 50 g at dinner.
The "Protein-First" Eating Order
Several studies now support eating protein (and vegetables) before carbohydrates in the same meal. This works through two mechanisms:
GLP-1 stimulation: Protein in the gut triggers GLP-1 release, which primes pancreatic insulin secretion before carbohydrates arrive
Mechanical delay: Protein slows gastric emptying, spreading the carbohydrate load over a longer period
Practical strategy: Start your meal with a protein source (dal, paneer, fish, chicken, eggs) or a vegetable side before moving to rice, roti, or bread. Even a 10–15 minute head start makes a measurable difference in post-meal glucose readings.
Protein Timing for Type 1 Diabetes
For people with type 1 diabetes on insulin, protein timing carries additional complexity. A high-protein meal without carbohydrates may still require a bolus, but the insulin should be delayed and extended ("dual-wave" or "square-wave" bolus on an insulin pump) to match the slower, later glucose rise driven by glucagon.
Work with your diabetes care team to test and adjust your insulin strategy based on CGM feedback from protein-containing meals.
7. BCAAs: The Double-Edged Sword
Branched-chain amino acids—leucine, isoleucine, and valine—are found in high concentrations in whey protein, red meat, eggs, and dairy. They are the amino acids most responsible for stimulating muscle protein synthesis, which is why they're popular in fitness nutrition.
However, the Mensink (2024) review and other research highlight a concern specific to people with diabetes: chronically elevated circulating BCAAs are associated with insulin resistance, particularly in people who are sedentary or consuming excess calories.
The mechanism involves interference with the PI3K-Akt signaling pathway—essentially, high BCAA levels can "jam the signal" that tells muscle cells to take up glucose in response to insulin.
The BCAA Paradox, Explained
BCAAs + resistance exercise: Beneficial. The amino acids are taken up by muscle for repair and synthesis, BCAAs are cleared from circulation quickly, and insulin signaling remains intact.
BCAAs + excess calories + low activity: Potentially harmful. BCAAs accumulate in the bloodstream, activate mTOR chronically, and impair insulin signaling.
Practical takeaway: If you use whey protein supplements, pair them with resistance training—don't consume them as a passive calorie or protein supplement without the exercise to match. For people with type 2 diabetes who are sedentary, whole-food plant proteins (which have a more balanced amino acid profile and lower BCAA density) may be metabolically safer than whey-heavy supplement regimens.
8. Evidence Summary Table
Recent clinical trials, long-term cohorts, and expert consensuses have fundamentally shifted how we view protein in diabetes management. Here are the core breakthroughs and what they mean for your daily nutrition:
Protein Demands Delayed Insulin (Dao et al., 2025): A clinical study on Type 1 Diabetes proved that protein alters late-phase glucose dynamics. The Implication: Individuals using insulin must account for protein in their bolus calculations, often utilizing a "dual-wave" pump setting to manage a slow blood sugar rise hours after eating.
Legumes Outperform Red Meat (Xu et al., 2025): A massive registry cohort and meta-analysis confirmed that moderate protein intake lowers Type 2 Diabetes risk, but specifically noted that plant-based legumes offer far superior metabolic protection compared to red meat. The Implication: You should actively prioritize plant-based protein sources over animal ones.
Digestion Speed Matters for Insulin (Mensink, 2024): This mechanistic review revealed that fast-digesting proteins can cause sudden insulin spikes, while chronically elevated branched-chain amino acids (BCAAs) from sedentary overeating can "jam" insulin signaling pathways. The Implication: Focus on slow-digesting, whole-food proteins rather than highly processed protein isolates.
The "Swap, Don't Add" Rule (Namazi et al., 2025): An iso-energetic substitution study found that replacing red meat calories with plant protein calories dramatically improves blood pressure, cholesterol, and inflammatory markers in Type 2 Diabetes. The Implication: Do not just add plant proteins on top of your current diet; you must swap them out for lower-quality meats to see the cardiometabolic benefits.
Protein Restriction Protects Kidneys (Liu et al., 2025): A rigorous 10-year retrospective cohort study confirmed that restricting daily protein to 0.6–0.8 g per kilogram of body weight safely slows down the progression of Chronic Kidney Disease (CKD) and lowers proteinuria. The Implication: Dietary protein restriction is vital and metabolically safe if you have diabetic kidney disease.
Protein is "Pharmacologically Active" (Nagy et al., 2025/2026): This clinical review synthesized how protein actively forces the gut to release GLP-1 while simultaneously prompting the pancreas to secrete glucagon. The Implication: Protein is not a passive, "free" macronutrient—it functions as an active biological trigger that heavily drives glucose and hormone curves.
Pea Protein Matches Whey (Thondre et al., 2026): A randomized controlled trial comparing protein powders found that while both whey and pea protein stimulate a healthy insulin response, pea protein provides a more sustained, gradual effect. The Implication: Plant-based pea protein is a highly effective, metabolically steady alternative to dairy-based whey.
The Blueprint for Prediabetes Remission (Zhu et al., 2026): The multinational PREVIEW trial discovered that a diet pairing higher protein with strictly low-glycemic index (low-GI) carbohydrates optimizes prediabetes reversal over 3 years. The Implication: Reversing prediabetes requires managing both protein quality and carbohydrate quality together; one cannot fix a poor profile without the other.
Validation of Traditional Diets (Mohan et al., 2023): An expert medical consensus from India confirmed that traditional South Asian, legume-heavy eating patterns perfectly align with modern metabolic evidence. The Implication: Culturally familiar proteins—such as whole dals, chana, and traditional curd—are exceptional clinical tools for local diabetes management.
9. Common Myths and Mistakes
Myth 1: "Protein doesn't affect blood sugar, so I can eat as much as I want."
Reality: Protein stimulates glucagon secretion and triggers hepatic glucose release, particularly relevant in type 1 diabetes. High-protein meals without carbohydrates can cause a delayed glucose rise 3–5 hours after eating. No macronutrient is truly "free."
Myth 2: "More protein is always better for diabetes management."
Reality: The evidence supports moderate protein intake (1.0–1.2 g/kg/day for most people with T2D). Beyond this range, there is no demonstrated additional glycemic benefit, and high intake from animal sources may increase cardiovascular risk. For those with kidney disease, high protein is actively harmful.
Myth 3: "Plant proteins are incomplete and inferior."
Reality: While individual plant foods may lack one or more essential amino acids, a varied plant-based diet—eating a combination of legumes, grains, nuts, seeds, and vegetables across the day—provides all essential amino acids. The metabolic benefits of plant proteins (fiber, lower saturated fat, anti-inflammatory compounds) make them superior overall for people with diabetes and cardiovascular risk.
Myth 4: "Protein supplements are equivalent to whole food protein."
Reality: The PREVIEW trial (Zhu et al., 2026), Namazi et al. (2025), and Mohan et al. (2023) all highlight that whole food proteins outperform processed alternatives. A can of chickpeas delivers protein plus fiber, resistant starch, magnesium, and polyphenols. A protein powder delivers protein only—and often processed additives.
Myth 5: "Restricting protein will cause muscle loss."
Reality: In the context of diabetic kidney disease, moderate protein restriction (0.6–0.8 g/kg/day) does not cause muscle loss when nutritional status is monitored and protein quality is high. The Liu et al. (2025) 10-year study confirmed maintained nutritional status throughout. Adequate caloric intake and weight-bearing exercise are the primary protectors of muscle mass—not high protein intake alone.
Myth 6: "All animal proteins are the same."
Reality: Processed meats (bacon, sausage, deli meats) are consistently associated with worse outcomes in people with diabetes. Unprocessed lean meats, poultry, fish, eggs, and dairy occupy a very different risk category. Lumping all animal proteins together leads to both unnecessary restriction and inappropriate permissiveness.
10. Best Protein Sources for People with Diabetes
Tier 1: Prioritize
These provide protein bundled with fiber, minerals, and anti-inflammatory compounds:
Legumes: Lentils (dal), chickpeas (chana), black beans, kidney beans (rajma), soybeans, mung beans
Soy products: Tofu, tempeh, edamame
Whole grains: Quinoa, amaranth (complete protein profiles)
Nuts and seeds: Almonds, walnuts, chia seeds, flaxseeds, hemp seeds
Vegetables: Peas, broccoli, spinach (contribute meaningful protein at scale)
Tier 2: Include (Quality Animal Proteins)
Fatty fish: Salmon, sardines, mackerel, trout (omega-3s, anti-inflammatory)
Lean poultry: Skinless chicken or turkey breast
Eggs: Whole eggs (including the yolk—it carries most of the micronutrients)
Fermented dairy: Greek yogurt, cottage cheese, kefir (probiotics + slow-digesting casein)
Tier 3: Minimize or Avoid
Processed meats: Bacon, sausage, salami, deli meats, hot dogs
Fatty unprocessed red meat: Lamb, beef with visible fat
Ultra-processed protein products: Protein bars with added sugar, heavily processed meat substitutes
Fried animal proteins: The cooking method can negate protein quality benefits
11. Practical Meal Planning Guide
Sample Day: Type 2 Diabetes (70 kg person, target 70–84 g protein/day)
Breakfast (~20–25 g protein)
Moong dal chilla (2 pieces) with a small bowl of low-fat curd
Or: 2-egg omelette with spinach and 1 slice of whole grain toast
Mid-morning snack (~10 g protein)
A small handful of mixed nuts (almonds + walnuts)
Or: 100 g Greek yogurt with a few berries
Lunch (~25–30 g protein)
1 cup cooked rajma or chana curry
Small portion of brown rice or 1–2 rotis
Salad or sabzi on the side
Eat the dal/sabzi before the rice/roti
Dinner (~20–25 g protein)
Grilled fish (100–120 g) or paneer (75–100 g) in a low-oil preparation
Roasted or steamed vegetables
Small portion of quinoa or dal
Protein-First Meal Template
For every main meal, use this ordering framework:
Start with protein + vegetables (eat for 5–10 minutes)
Then eat complex carbohydrates (rice, roti, bread, fruit)
Finish with any dessert or sweeter items
This simple reordering consistently reduces post-meal glucose peaks by 20–30% in research studies.
Checklist: Optimizing Your Protein for Diabetes
[ ] Calculate your daily protein target (weight in kg × 1.0 for T2D; × 0.6–0.8 for CKD)
[ ] Distribute protein across 3–4 meals rather than one large serving
[ ] Replace at least one red meat serving per week with a legume-based dish
[ ] Eat protein before carbohydrates at main meals
[ ] Choose whole food proteins over supplements wherever possible
[ ] If using whey protein, pair it with resistance exercise
[ ] If you have T1D, discuss protein counting with your diabetes educator
[ ] Get kidney function (eGFR, urine albumin-to-creatinine ratio) checked before significantly increasing protein intake
12. FAQs
Q: How much protein should I eat daily if I have diabetes?
For most people with type 2 diabetes, 1.0–1.2 grams per kilogram of body weight per day is the evidence-based target. If you have chronic kidney disease alongside diabetes, this drops to 0.6–0.8 g/kg/day. People with type 1 diabetes should work with a diabetes educator to factor protein into insulin dosing calculations. Your individual target depends on body composition, kidney function, activity level, and blood glucose control.
Q: Is plant-based protein better than animal protein for managing diabetes?
In most direct comparisons, yes. Plant proteins—especially legumes—are associated with better insulin sensitivity, lower cardiovascular risk, and improved cholesterol profiles compared to red and processed meats. However, quality animal proteins like fish, eggs, and poultry are also appropriate. The biggest benefit comes from replacing processed and red meats with plant sources, not just adding plants on top.
Q: Does protein raise blood sugar?
Protein raises blood sugar more slowly and less dramatically than carbohydrates, but it is not neutral. Protein stimulates glucagon secretion, which prompts the liver to release glucose. In type 1 diabetes especially, a high-protein meal can cause a delayed glucose rise 3–5 hours later. For type 2 diabetes, the effect is typically more modest but still present and measurable with CGM.
Q: Can protein help prevent hypoglycemia (low blood sugar)?
Protein-triggered glucagon release can help counteract falling blood sugar in some circumstances, but this effect is unpredictable and should not replace standard hypoglycemia treatment (fast-acting glucose). If you experience frequent hypoglycemia, discuss the role of protein and meal timing with your healthcare provider.
Q: Should I take protein supplements or powders if I have diabetes?
Whole food protein sources are superior to supplements for people with diabetes based on the current evidence. Whole foods provide fiber, minerals, vitamins, and anti-inflammatory compounds that protein powders don't. Unless you have a specific nutritional gap that can't be addressed through food (confirmed by a dietitian), focus on food-first protein strategies.
Q: Is high protein intake dangerous for my kidneys?
For people with normal kidney function, moderate protein intake (up to 1.2 g/kg/day) does not appear to harm kidney health. However, people with existing CKD—common in long-standing diabetes—should restrict protein to prevent accelerated kidney damage. Never increase protein substantially without first checking your kidney function (eGFR and urine albumin).
Q: How does protein affect insulin resistance?
Adequate protein intake combined with muscle-building resistance exercise improves insulin sensitivity by increasing muscle mass—the body's primary glucose disposal organ. However, high BCAA intake from whey or red meat in the context of excess calories and low activity can impair insulin signaling. Protein quality, source, and the exercise context together determine whether protein helps or hinders insulin sensitivity.
Q: Can protein help with weight loss when I have diabetes?
Yes. Protein increases satiety more than carbohydrates or fat, reduces total calorie intake, and preserves muscle mass during weight loss. Maintaining muscle is particularly important for people with diabetes because muscle drives glucose uptake. A moderate protein intake (1.0–1.2 g/kg/day) during a caloric deficit is associated with better body composition outcomes than low-protein weight loss diets.
Q: What is the best protein for type 1 diabetes?
There is no single "best" protein for type 1 diabetes. The key considerations are: accounting for protein in insulin dosing calculations, choosing slow-digesting proteins (legumes, casein-rich dairy, fish) that produce gentler and more predictable glucose patterns, spreading protein across meals, and tracking individual responses using CGM.
Q: How much protein do I need after exercise with diabetes?
People with diabetes who exercise regularly benefit from 20–30 g of high-quality protein within 2 hours post-exercise to support muscle protein synthesis and recovery. This can come from a serving of Greek yogurt, a small portion of cooked dal with paneer, a boiled egg with a handful of nuts, or a legume-based snack. Coordinate post-exercise nutrition with your diabetes care team if you're adjusting insulin around exercise.
Q: What about protein needs for older adults with diabetes?
Sarcopenia (age-related muscle loss) is a significant concern in older adults with diabetes, as reduced muscle mass worsens insulin resistance and increases fall risk. Older adults with diabetes generally benefit from protein intake at the higher end of the range (1.2 g/kg/day) unless kidney disease is present. Prioritize protein distribution across all three meals to maximize muscle protein synthesis with each eating occasion.
Q: Are traditional Indian protein foods (dal, paneer, curd) good for diabetes?
Yes—several of them are among the best choices in the world for people with diabetes. Dal (lentils, mung, chana, rajma) provides protein + fiber + resistant starch, making it genuinely superior to meat for glycemic management. Paneer is a reasonable protein source but is higher in saturated fat, so portion size matters. Curd (especially low-fat) provides protein, probiotics, and calcium. The Mohan et al. (2023) Indian expert consensus specifically endorses traditional legume-based diets as ideal for diabetes management in South Asian contexts.
13. Conclusion and Action Steps
The latest 2025–2026 research makes one thing clear: protein is an active participant in your diabetes management, not a passive bystander. How much you eat, where it comes from, when you eat it, and what it replaces all carry measurable metabolic consequences.
The most consistent finding across every study reviewed here is the superiority of whole food plant proteins—particularly legumes—for people with diabetes. This isn't about eliminating animal foods. It's about building a diet where protein works with your metabolism, not against it.
Start with these six evidence-based actions:
Calculate your protein target using your body weight and health status (1.0–1.2 g/kg for T2D; 0.6–0.8 g/kg for CKD). Don't guess—know your number.
Get your kidney function tested before making any significant protein changes. Ask your doctor for eGFR and urine albumin-to-creatinine ratio (ACR).
Replace one red or processed meat serving per week with a legume dish. This single swap has outsized cardiometabolic benefits.
Eat protein before carbohydrates at meals. Start with dal, sabzi, fish, or eggs before moving to rice or roti.
Spread protein across all three meals rather than concentrating it at dinner.
Consult a registered dietitian with diabetes expertise to personalize your protein strategy, especially if you have T1D, CKD, or are on insulin.
Author's Note (Clinician's Perspective)
As a physician in internal medicine, one of the most common misconceptions I encounter in diabetes care is the belief that only carbohydrates matter. Many patients become highly focused on counting carbs while paying little attention to protein quality, meal composition, and meal timing. Yet the emerging science reviewed in this article shows that protein is far more than a passive nutrient—it actively influences insulin secretion, glucagon release, satiety, muscle preservation, kidney health, and long-term metabolic outcomes.
I recall a 58-year-old gentleman with type 2 diabetes, obesity, hypertension, and early fatty liver disease who came to clinic frustrated by persistently elevated blood glucose levels despite carefully reducing sugar and refined carbohydrates. His diet was relatively low in protein and heavily dependent on refined grains. Breakfast often consisted of toast and tea, lunch centered around rice, and dinner was largely carbohydrate-based with minimal legumes or other quality protein sources.
Rather than focusing exclusively on further carbohydrate restriction, we worked on improving protein quality and distribution throughout the day. He began including lentils, chickpeas, Greek yogurt, and occasionally fish in his meals. We also adopted a "protein-first" meal strategy, encouraging him to eat protein-rich foods and vegetables before consuming rice or bread. In addition, he started a simple resistance-training program three times per week.
Over the following several months, he reported improved satiety, fewer cravings, and better energy levels. His continuous glucose readings showed lower post-meal glucose excursions, he lost a meaningful amount of weight, and his HbA1c improved substantially. Equally important, these changes were sustainable because they were based on food quality and meal structure rather than extreme dietary restriction.
Cases like this reinforce an important lesson: diabetes management is not simply about eating less sugar. The quality, quantity, timing, and source of dietary protein can significantly influence metabolic health. While no single dietary strategy works for everyone, the evidence increasingly supports a pattern centered on whole-food protein sources—particularly legumes, nuts, seeds, dairy, fish, and other minimally processed foods—combined with regular physical activity and individualized medical care.
My goal as a clinician is not only to help patients lower glucose numbers but also to preserve muscle mass, protect kidney function, reduce cardiovascular risk, and improve quality of life. When used thoughtfully, protein becomes an important therapeutic tool that supports all of these objectives.
Note: This article is for educational purposes. It reflects peer-reviewed research from 2023–2026 but does not constitute individualized medical advice. Always consult your physician or registered dietitian before making significant dietary changes, particularly if you have kidney disease, take insulin, or have multiple health conditions.
Related Articles
Low Carb or Low Fat: What the Latest Research Says About Blood Sugar Control
You’re Missing This: Why mTOR Activation Is the Real Goal of Strength Training | DR T S DIDWAL
The mTOR Switch: Why Your Cells Stopped Listening to Insulin | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
References
Dao, G. M., Kowalski, G. M., Bruce, C. R., O'Neal, D. N., Smart, C. E., Zaharieva, D. P., Hennessy, D. T., Zhao, S., & Morrison, D. J. (2025). The glycemic impact of protein ingestion in people with type 1 diabetes. Diabetes Care, 48(4), 509–518. https://doi.org/10.2337/dci24-0096
Liu, D., Li, Q., Jia, R., He, W., Zhao, X., Pan, M., Chen, X., Wang, Y., Zhu, Y., Hou, H., Xie, J., & Wang, W. (2025). Type 2 diabetes mellitus with chronic kidney disease benefits from long-term restriction of dietary protein intake: A 10-year retrospective cohort study. BMC Nutrition, 11(1), 131. https://doi.org/10.1186/s40795-025-01119-w
Mensink, M. (2024). Dietary protein, amino acids and type 2 diabetes mellitus: A short review. Frontiers in Nutrition, 11, 1445981. https://doi.org/10.3389/fnut.2024.1445981
Mohan, V., Misra, A., Bhansali, A., Singh, A. K., Makkar, B., Krishnan, D., Chadha, M., Shah, P., Samaddar, R., Saraogi, R. K., Tiwaskar, M., Saboo, B., Baruah, M. P., Chowdhury, S., Jaggi, S., & Shivaswamy, V. (2023). Role and significance of dietary protein in the management of type 2 diabetes and its complications in India: An expert opinion. Journal of the Association of Physicians of India, 71(12), 36–46. https://doi.org/10.59556/japi.71.0339
Nagy, S., Turner, L. V., & Riddell, M. C. (2025/2026). Effects of protein intake on glucagon, insulin, and glucose dynamics: Implications for diabetes. Frontiers in Clinical Diabetes and Healthcare, 6, 1712506. https://doi.org/10.3389/fcdhc.2025.1712506
Namazi, N., Anjom-Shoae, J., Darbandi, M., et al. (2025). Dietary intake of total, animal, and vegetable protein and cardiometabolic risk factors in patients with type 2 diabetes: Using iso-energetic substitution models. Journal of Diabetes and Metabolic Disorders, 24, 60. https://doi.org/10.1007/s40200-025-01571-2
Thondre, P. S., Young, E., Pledger, S., Kefyalew, S., Hatami, I., Perreau, C., Guérin-Deremaux, L., Lefranc-Millot, C., & Tammam, J. (2026). A randomized controlled trial in healthy participants to compare the insulinogenic effects of whey protein and pea protein co-ingested with glucose. PLOS ONE, 21(1), e0340386. https://doi.org/10.1371/journal.pone.0340386
Xu, M., Zheng, J., Ying, T., et al. (2025). Dietary protein and risk of type 2 diabetes: Findings from a registry-based cohort study and a meta-analysis of prospective cohort studies. Nutritional Diabetes, 15, 25. https://doi.org/10.1038/s41387-025-00380-z
Zhu, R., Guo, J., Huttunen-Lenz, M., et al. (2026). Long-term effects of dietary protein and carbohydrate quality on prediabetes remission: Results from the PREVIEW randomised multinational diabetes prevention trial. Diabetologia, 69, 81–92. https://doi.org/10.1007/s00125-025-06560-x
American Diabetes Association Professional Practice Committee. (2026). 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes—2026. Diabetes Care, 49(Suppl. 1), S246–S263. https://doi.org/10.2337/dc26-S011 (Section on Nutrition)