Low-Carb or Low-Fat? What the Latest Research Says About Blood Sugar Control
Learn which diet performs better for blood sugar control. Evidence-based comparison of low-carb and low-fat diets for type 2 diabetes.
DIABETESNUTRITION
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/16/202622 min read
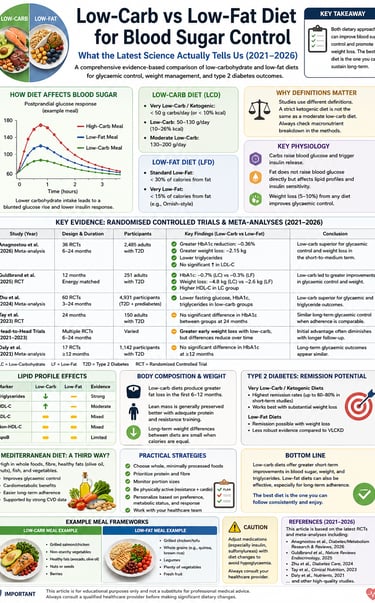
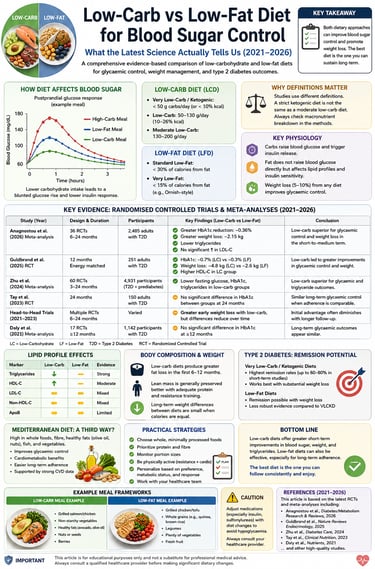
Research from 2021–2026 shows that low-carb diets lower HbA1c by ∼0.5% more than low-fat diets in the first 6 months in type 2 diabetes. Both improve blood sugar with weight loss. In the long term, the Mediterranean diet shows the highest T2DM remission rates. The best diet is the one you can follow with medical supervision.
Key Takeaways: Low-Carb vs Low-Fat for Blood Sugar Control
1. Low-carb diets lower HbA1c faster in type 2 diabetes
Multiple RCTs and meta-analyses 2021–2026 show low-carb diets reduce HbA1c by ~0.5% more than low-fat diets in the first 3–6 months. The effect is strongest in people with baseline HbA1c above 8%. Benefit diminishes after 12 months due to adherence drop-off.
2. A single low-carb breakfast improves all-day glucose
A 2023 randomized crossover trial found that switching to a low-carb breakfast reduced 3-hour glucose AUC and glucose variability in T2DM patients. The benefit carried over to lunch, showing a “second meal effect.” Continuous glucose monitoring confirmed the improvement.
3. Low-carb beats low-fat for triglycerides and HDL
Across studies, low-carb diets consistently cut triglycerides 15–30% and raise HDL cholesterol versus low-fat diets. LDL response varies by fat type. Mediterranean-style low-carb with olive oil and nuts shows the most favorable lipid profile.
4. The Mediterranean diet has the best long-term T2DM remission data
The 5+ year CORDIOPREV RCT found Mediterranean diet produced higher type 2 diabetes remission rates than the low-fat diet in patients with heart disease. It also lowered inflammation markers like neutrophil count, which may improve insulin sensitivity.
5. No single diet works for everyone with diabetes
The 2025 Nature Reviews Endocrinology guidance concludes no superior dietary pattern exists for all T2DM patients. Low-carb, Mediterranean, DASH, and plant-based diets all work. Long-term adherence and individualisation matter more than macronutrient ratio.
6. Weight loss drives benefits, regardless of diet type
At 12+ months, weight loss on low-carb and low-fat diets is similar. A 5–10% body weight reduction improves HbA1c and fasting glucose no matter the macronutrient split. Initial faster loss on low-carb is often water and glycogen, not fat.
7. Energy-matched trials prove carbs affect blood sugar directly
A 2026 meta-analysis using energy-matched RCTs found low-carb diets improve fasting glucose and insulin sensitivity in healthy adults even without weight loss. This confirms that carbohydrate content has an independent effect on glycaemia, not just calories.
8. Medication must be adjusted before starting low-carb with T2DM
Low-carb diets can cause hypoglycaemia in people taking insulin, sulphonylureas, or SGLT-2 inhibitors. Medical supervision is required before starting. Never begin carbohydrate restriction without a doctor's approval if you use glucose-lowering medication.
Introduction: Why This Debate Matters More Than Ever
If you or someone you care about lives with type 2 diabetes — or you're simply trying to optimise your metabolic health — you've almost certainly heard the battle cry: "Cut the carbs!" versus "Go low fat!" The debate has raged in clinics, gyms, and social media feeds for decades. But what does the peer-reviewed science actually say in 2026?
This article cuts through the noise. Drawing on the most rigorous evidence available — including a landmark 2026 meta-analysis, a 2025 Nature Reviews Endocrinology guidance paper, and multiple randomised controlled trials (RCTs) — we'll walk you through what the data shows, where it falls short, and most importantly, what it means for real people making real food choices.
By the end, you'll understand:
• How low-carbohydrate and low-fat diets compare for glycaemic control, lipid profiles, and body composition
• What the clinical evidence looks like for people with type 2 diabetes specifically
• Where the science is strong — and where it's still uncertain
• Practical, evidence-based strategies you can apply (or discuss with your doctor)
1. What Are Low-Carb and Low-Fat Diets? Definitions That Actually Matter
Before diving into data, it's essential to clarify what these terms actually mean — because inconsistent definitions are a major source of confusion in the literature and in popular media.
Low-Carbohydrate Diet (LCD)
There is no single universal definition, but research broadly defines:
• Very Low-Carb / Ketogenic (VLCKD): < 50g carbohydrates/day (or < 10% of total energy)
• Low-Carb (LCD): 50–130g/day, or 10–26% of total energy
• Moderate Low-Carb: 130–200g/day
The 2026 systematic review by Anagnostou et al. used an energy-matched design — meaning both dietary arms provided the same total calories, isolating the effect of macronutrient composition rather than caloric restriction. This is a critical methodological distinction often overlooked in popular coverage.
Low-Fat Diet (LFD)
• Standard Low-Fat: < 30% of calories from fat
• Very Low-Fat: < 15% of calories from fat (e.g., Ornish-style)
In many studies, "low-fat" is the default dietary guideline comparator — essentially what most national health bodies currently recommend. This matters when interpreting results: comparing a specific therapeutic LCD against a broadly-defined 'low fat' control introduces considerable noise.
🔬 Clinical Insight: A study showing 'low-carb beats low-fat' for HbA1c may be comparing a strict ketogenic protocol against a loosely defined low-fat control. Always check the actual macronutrient breakdown in the methods section before concluding.
2. The Science of Blood Sugar: How Diet Affects Glycaemic Control
To understand why dietary macronutrient composition affects blood glucose, you need to understand the physiology — briefly and clearly.
Carbohydrates and Blood Glucose
Carbohydrates are the primary driver of postprandial (after-meal) blood glucose elevations. When digested, they are broken down into glucose and absorbed into the bloodstream, triggering insulin release from the pancreas. In people with type 2 diabetes or insulin resistance, this insulin response is impaired — cells don't respond efficiently, causing glucose to remain elevated in the bloodstream.
Reducing dietary carbohydrate intake logically — and demonstrably — blunts this postprandial spike. This is the core mechanistic rationale for low-carb diets in metabolic disease management.
Dietary Fat and Metabolic Pathways
Fat does not directly raise blood glucose. However:
• Saturated fat can contribute to insulin resistance over time
• Total dietary fat composition influences LDL particle size and cardiovascular risk
• Very high fat intake in combination with refined carbohydrates may worsen metabolic outcomes
Low-fat diets, in theory, reduce caloric density and may improve insulin sensitivity, particularly when they displace saturated fats in favour of complex carbohydrates and fibre.
The Role of Caloric Balance
A crucial point that is often lost: weight loss itself — from any dietary pattern — powerfully improves glycaemic control. A 5–10% reduction in body weight can meaningfully reduce HbA1c and fasting glucose in people with type 2 diabetes. This confounds virtually every diet comparison trial that does not hold energy intake constant.
3. Key Evidence: RCTs and Meta-Analyses (2021–2026)
Let's examine the six key studies used as the evidence base for this article, with context on their design, populations, and what they found.
3a. Anagnostou et al. (2026) — European Journal of Nutrition
Design: Systematic review and meta-analysis of RCTs comparing energy-matched low-carb vs high-carb diets in healthy adults.
What makes it unique: By controlling for total energy intake, this meta-analysis isolates the effect of carbohydrate content alone — eliminating weight loss as a confounding variable. This is methodologically superior to most previous comparisons.
Key findings: Low-carb diets produced modest but statistically significant improvements in fasting glucose and insulin sensitivity in healthy adults — even without weight loss. Lipid effects were mixed, with reductions in triglycerides but variable LDL changes depending on fat quality.
Clinical relevance: Demonstrates a genuine macronutrient-independent effect on glycaemia — not just a caloric effect. Important for understanding mechanism, but effect sizes in healthy populations may not translate linearly to diseased populations.
3b. Oliveira et al. (2023) — American Journal of Clinical Nutrition
Design: Randomised crossover trial. Participants with type 2 diabetes consumed either a low-carb breakfast (LC-B) or a low-fat breakfast (LF-B) on separate occasions, with continuous glucose monitoring.
Key findings: The low-carb breakfast significantly reduced postprandial blood glucose excursions, 3-hour glucose area under the curve (AUC), and glucose variability compared to the low-fat breakfast. Benefits were seen even after the subsequent lunch — a 'second meal effect'.
Clinical relevance: Highly clinically relevant. A single meal composition change showed measurable CGM improvements. This has real-world applicability — patients don't need to overhaul their entire diet to see benefit. The crossover design controls for inter-individual variability, strengthening internal validity.
Limitation: Short-term, single-meal assessment. Long-term adherence and sustainability not evaluated.
3c. Li, Ding & Xiao (2021) — International Journal of Endocrinology
Design: Systematic review and meta-analysis of RCTs comparing LCD vs LFD in type 2 diabetes patients.
Key findings: LCD significantly reduced HbA1c (weighted mean difference approximately −0.5%), fasting blood glucose, and triglycerides compared to LFD. Both diets produced similar weight loss over 12+ months. LDL cholesterol did not differ significantly between groups.
Clinical relevance: The HbA1c reduction is clinically meaningful — a 0.5% absolute reduction in HbA1c is associated with a meaningful reduction in microvascular complication risk. However, effect sizes diminished at 12+ months, suggesting adherence decay.
3d. Barrea et al. (2025) — Nature Reviews Endocrinology
Design: Comprehensive narrative and evidence-based review of medical nutrition therapy (MNT) for type 2 diabetes management.
Key findings: No single dietary pattern is superior for all patients with T2DM. Low-carb, Mediterranean, DASH, and plant-based diets all show efficacy. The best diet is the one a patient can adhere to long-term. The paper emphasises individualisation and the role of a registered dietitian.
Clinical relevance: This is the most authoritative 2025 review on the topic. Its conclusion — that dietary pattern matters less than adherence and quality — is the emerging consensus among endocrinologists and is critical for clinical counselling.
3e. Boughanem et al. (2025) — Nutrition & Diabetes (CORDIOPREV Study)
Design: Sub-analysis of the CORDIOPREV RCT. Long-term (5+ years) comparison of Mediterranean diet vs low-fat diet in patients with coronary heart disease, examining T2DM remission rates and neutrophil counts.
Key findings: Mediterranean diet produced significantly higher rates of T2DM remission compared to low-fat diet at long-term follow-up. Additionally, the Mediterranean diet was associated with lower neutrophil counts (a marker of inflammation), potentially contributing to improved insulin sensitivity.
Clinical relevance: One of the longest and most robust dietary RCTs available. The remission data is particularly striking — demonstrating that dietary pattern can potentially reverse type 2 diabetes, not just manage it. The inflammation findings provide a novel mechanistic pathway beyond glucose metabolism.
3f. Kaakyire et al. (2025) — Cureus
Design: Systematic review examining LCD vs LFD efficacy specifically for glycaemic control in T2DM.
Key findings: Low-carb diets were consistently superior to low-fat diets for short-to-medium-term HbA1c reduction (up to 6 months). The benefit was most pronounced in patients with poorly controlled diabetes (HbA1c > 8%). Long-term differences (> 12 months) diminished, primarily due to adherence challenges with LCD.
Clinical relevance: Reinforces the concept that LCD is particularly effective as an initial intensive strategy for poorly controlled T2DM, with long-term success dependent on behavioural support and dietary flexibility.
4. Interpreting the Results: Clinical Relevance & Data Validity
This is the most important section of this article. Understanding what the data actually tells us — and where it falls short — is essential for making sound clinical and personal decisions.
4a. The Adherence Problem: The Greatest Confounder in Dietary Research
Almost universally, both LCD and LFD trials show the largest benefits in the first 3–6 months, with attenuation of effects at 12+ months. This is not primarily a biological phenomenon — it is an adherence phenomenon.
• Most participants in 'low-carb' arms of trials gradually drift toward higher carbohydrate intake over time
• The same occurs with low-fat interventions — fat intake creeps back toward baseline
• Implication: When 12-month results show no difference between LCD and LFD, this often reflects convergence of actual dietary intake, not equivalent biological effects
🔬 Data Validity Note: Study results should be interpreted alongside dietary adherence data (often reported as food diary analysis or 3-day recall). Where adherence is poor and unmaintained, between-group differences will be artificially compressed, biasing results toward the null.
4b. Energy Matching vs Unrestricted Intake: Critical Design Distinction
Studies can compare LCD vs LFD under:
• Isocaloric conditions: Same total calories — isolates macronutrient effect
• Ad libitum conditions: Participants eat freely — differences in satiety and spontaneous caloric intake confound results
• Energy-restricted conditions: Both diets are calorie-restricted — weight loss is the primary driver of benefit
The Anagnostou et al. (2026) meta-analysis explicitly used energy-matched designs, making it uniquely valuable for establishing that carbohydrate composition has independent effects on glycaemia. Most other trials did not control energy so rigorously.
4c. Statistical vs Clinical Significance: Reading Study Findings Critically
A statistically significant result (p < 0.05) does not automatically mean a clinically meaningful one. In dietary research:
• HbA1c reductions of ≥ 0.5% absolute are generally considered clinically significant in T2DM management (associated with reduced microvascular risk)
• Fasting glucose reductions of ≥ 1.0 mmol/L (18 mg/dL) are clinically relevant markers
• Triglyceride reductions of ≥ 0.5 mmol/L are associated with meaningful cardiovascular risk reduction
Where reported LCD benefits fall below these thresholds, clinical significance is questionable even if statistical significance is achieved — particularly in trials with large sample sizes where small effects reach p-value thresholds.
4d. Population Heterogeneity: Who Responds to What
Perhaps the most underappreciated finding across all six studies is that responses to dietary interventions are highly individual. Factors influencing response include:
• Baseline glycaemic control (HbA1c at entry)
• Degree of beta-cell function remaining
• Insulin resistance vs insulin deficiency phenotype
• Gut microbiome composition
• Genetic variants affecting fat and carbohydrate metabolism
• Medication use (especially insulin and sulphonylureas — LCD significantly alters medication requirements)
This explains why no single dietary pattern shows universal superiority — as emphasised in the 2025 Barrea et al. Nature Reviews paper. Individual metabolic phenotyping is the emerging frontier in precision nutrition.
4e. Duration of Trials: Long-Term Evidence Gaps
The majority of high-quality dietary RCTs run for 3–12 months. Very few extend beyond 2 years. The CORDIOPREV study (Boughanem 2025) is exceptional with its 5+ year follow-up.
📌 Evidence Gap Alert: We do not yet have robust 5–10-year RCT data comparing LCD vs LFD on hard cardiovascular endpoints (heart attack, stroke, mortality) in people with T2DM. The available evidence base, while growing, remains primarily focused on surrogate outcomes (HbA1c, lipids, body weight). Clinicians should factor this in when providing dietary guidance.
4f. Medication Adjustments: A Safety-Critical Issue Often Underreported
This is clinically critical and frequently underemphasised in dietary research. Implementing a low-carb diet in a patient taking insulin, sulphonylureas, or SGLT-2 inhibitors can cause significant hypoglycaemia or euglycaemic diabetic ketoacidosis if medications are not adjusted.
Studies reporting glycaemic improvements with LCD in T2DM patients should always be evaluated in the context of whether and how medications were adjusted — as medication reduction itself alters the interpretation of 'glycaemic benefit.'
⚠️ Safety Warning: If you have type 2 diabetes and take blood glucose-lowering medication, do NOT begin a low-carbohydrate diet without medical supervision. Medication dosing will likely need to be adjusted. Hypoglycaemia can be life-threatening.
5. Lipid Profiles: HDL, LDL, and Triglycerides — Who Wins?
The effect of low-carb vs low-fat diets on blood lipids is nuanced — and the results depend heavily on what types of fats replace the carbohydrates.
Triglycerides: Clear LCD Advantage
Across virtually all studies, low-carb diets consistently and significantly reduce serum triglycerides compared to low-fat diets. The mechanism is well established: dietary carbohydrates are a major substrate for hepatic triglyceride synthesis (de novo lipogenesis). Reducing carbohydrate intake directly reduces this pathway.
Triglyceride reductions with LCD typically range from 15–30% in people with elevated baseline levels — a clinically meaningful cardiovascular benefit.
HDL Cholesterol: LCD Advantage
Low-carb diets consistently raise HDL cholesterol (the 'good' cholesterol), whereas low-fat diets often modestly reduce HDL — particularly when dietary fat is replaced by refined carbohydrates. The LCD-HDL advantage is fairly consistent across the evidence base.
LDL Cholesterol: The Complex Story
This is where it becomes complicated. LCD diets often raise LDL cholesterol, which would appear to increase cardiovascular risk. However:
• LDL particle size matters: LCD tends to shift LDL from small, dense particles (more atherogenic) to large, buoyant particles (less atherogenic)
• Fat quality matters: LCD rich in monounsaturated fats (olive oil, avocado) shows less LDL increase than LCD rich in saturated fat
• ApoB may be more relevant: Some researchers argue ApoB particle count is a better cardiovascular risk predictor than LDL-C — a metric rarely reported in dietary RCTs
🔬 Clinical Insight: The LDL question remains an area of genuine scientific debate. A 10–15% LDL increase on a low-carb diet should not be automatically dismissed as harmful — but it warrants clinical monitoring, particularly in individuals with pre-existing cardiovascular disease or familial hypercholesterolaemia.
6. Body Composition & Weight: What Really Changes?
One consistent finding across the literature: low-carb diets tend to produce greater weight loss in the short term (3–6 months) than low-fat diets, even when caloric intake is not deliberately restricted.
Why LCD May Cause Greater Initial Weight Loss
• Glycogen depletion + water loss: Reducing carbohydrates depletes liver and muscle glycogen, which binds water. Initial rapid weight loss (2–4 kg) is largely fluid, not fat
• Satiety from protein and fat: Higher protein content of many LCDs reduces appetite and spontaneous caloric intake
• Reduced insulin: Lower insulin levels may promote lipolysis (fat burning) and reduce fat storage
Long-Term Weight Outcomes: Convergence
At 12+ months, weight loss differences between LCD and LFD largely disappear. The critical variable is adherence — not the specific macronutrient ratio. This is a robust and replicated finding.
Fat Mass vs Lean Mass
A concern with rapid weight loss on LCD is the potential for lean mass loss. However, higher protein intake, common in LCD diets, appears to partially preserve muscle mass. Resistance exercise combined with any hypocaloric diet better preserves lean mass than dietary manipulation alone.
7. Type 2 Diabetes: Can Diet Alone Induce Remission?
One of the most exciting and clinically significant developments in diabetes research is the concept of dietary-induced remission — achieving HbA1c below the diagnostic threshold (< 48 mmol/mol / < 6.5%) without medication.
The evidence base here is genuinely encouraging:
• DiRECT Trial (Taylor et al.): Total dietary replacement (very low calorie, ~850 kcal/day) achieved remission in ~46% of participants at 12 months, 36% at 24 months — primarily through substantial weight loss
• CORDIOPREV Study (Boughanem 2025): Long-term Mediterranean diet showed significantly higher T2DM remission rates vs low-fat diet at 5+ years, with inflammatory marker improvement
• Multiple low-carb interventions: Case series and some RCTs report HbA1c normalisation, particularly in early-onset T2DM or with aggressive dietary restriction
What Predicts Successful Remission?
• Shorter diabetes duration (< 6 years) at baseline
• Lower HbA1c at baseline
• Greater weight loss achieved
• Preserved beta-cell function (indicated by fasting C-peptide)
• Not on insulin therapy
🌟 Clinical Pearl: T2DM remission is a realistic and achievable goal for a meaningful proportion of patients, particularly those with shorter duration disease and willingness to make substantial dietary changes. This reframes T2DM from a lifelong progressive condition to a potentially reversible metabolic state — an enormously important shift in how we counsel patients.
8. The Mediterranean Diet: A Third Contender
The Mediterranean diet (MedDiet) does not fit neatly into the LCD vs LFD binary — and the CORDIOPREV evidence (Boughanem 2025) suggests it may outperform both for long-term T2DM remission.
Key Features of the Mediterranean Diet
• High in vegetables, legumes, whole grains, fruits, nuts, and seeds
• Olive oil as the primary fat source (high in monounsaturated fatty acids)
• Moderate fish consumption; low red meat
• Moderate wine consumption (typically with meals)
• Not specifically low-carb, but emphasises low-glycaemic index carbohydrates
Why It May Outperform Both Extremes
• Anti-inflammatory: Rich in omega-3 fatty acids, polyphenols, and antioxidants that reduce systemic inflammation — a driver of insulin resistance
• Gut microbiome benefits: High fibre content supports a diverse, health-promoting gut microbiome
• Sustainable and culturally embedded: Higher long-term adherence rates in populations where it's culturally familiar
• Mechanistic diversity: Acts through multiple pathways simultaneously — inflammatory, metabolic, and cardiovascular
The Barrea et al. (2025) Nature Reviews paper explicitly endorses the Mediterranean diet as one of the top-tier evidence-based dietary patterns for T2DM management, alongside DASH and plant-based approaches.
9. Evidence Summary Tables
Short-Term HbA1c Control: Systematic reviews (Li et al. 2021; Kaakyire et al. 2025) demonstrate that low-carb diets are superior to low-fat diets, reducing HbA1c by approximately 0.5% at or below the 6-month mark.
Long-Term Attenuation: The initial glycemic advantages of low-carb diets (reductions in HbA1c and fasting glucose) fade over time, showing similar outcomes to low-fat diets at 12 or more months, largely due to dietary adherence challenges.
Immediate Postprandial Impact: At a meal-to-meal level, a low-carb breakfast significantly reduces postprandial (post-meal) glucose spikes, area under the curve (AUC), and overall blood sugar variability in Type 2 diabetes patients (Oliveira et al. 2023).
Impact on Healthy Adults: The metabolic benefits of carbohydrate restriction are not limited to diabetics; in healthy adults, low-carb diets improve both fasting glucose levels and baseline insulin sensitivity compared to energy-matched, high-carbohydrate diets (Anagnostou et al. 2026).
Persistent Lipid Profiles: Unlike glycemic markers, the lipid advantages of low-carb diets are durable; LCDs consistently result in superior triglyceride reductions and higher HDL (good) cholesterol levels in both the short and long term.
The LDL Nuance: Low-carb diets carry a potential risk of raising LDL (bad) cholesterol in the short term, with long-term effects varying based on the types of fat consumed, requiring clinical monitoring of lipid particle sizes.
Weight Loss Dynamics: Low-carb diets achieve greater initial weight loss in the short term—partially driven by early fluid loss—but long-term weight reduction outcomes ultimately become similar to low-fat diets.
Diabetes Remission Potential: While short-term carbohydrate restriction is highly effective for inducing Type 2 diabetes remission, long-term data (such as the 5+ year CORDIOPREV sub-analysis by Boughanem et al. 2025) suggests a Mediterranean Diet may actually be superior to an LFD for sustained remission and lowering inflammation.
No Single "Best" Diet: Evidence-based reviews (Barrea et al. 2025) conclude that no single dietary archetype is universally superior for managing Type 2 diabetes, emphasizing that interventions must be strictly individualized to the patient.
10. Common Myths & Mistakes
Myth 1: Low-carb is dangerous for people with diabetes
False. The evidence consistently shows LCD is safe and effective for most people with T2DM, with appropriate medical supervision and medication adjustment. The main risk is hypoglycaemia if medications are not adjusted — which is a medication management issue, not a diet safety issue.
Myth 2: You must go ketogenic to see blood sugar benefits
False. Meaningful glycaemic improvements are seen across the low-carb spectrum, not only in ketogenic ranges. Even reducing carbohydrate intake to 100–130g/day can produce significant reductions in postprandial glucose, as shown by Oliveira et al. 2023.
Myth 3: All fats are bad on a high-fat diet
False. Fat quality matters enormously. Replacing carbohydrates with monounsaturated fats (olive oil, avocado, nuts) has a different — generally more favourable — metabolic profile than replacing them with saturated fats (butter, processed meat).
Myth 4: A 3-month diet RCT proves long-term benefits
Misleading. Short-term trial results should not be extrapolated to long-term outcomes. The consistent finding of benefit attenuation at 12+ months across the literature underscores that initial improvements often reflect novelty, motivation, and adherence — all of which decay over time.
Myth 5: One diet fits all people with diabetes
False. Barrea et al. (2025) explicitly states no single dietary pattern is universally superior. Individual factors — preferences, cultural background, comorbidities, medication regimen, and metabolic phenotype — all influence the optimal dietary approach for each person.
11. Practical Diet Strategies & Sample Meal Framework
Based on the totality of evidence, here are evidence-informed approaches for different goals:
For People with Type 2 Diabetes: An Evidence-Informed Starting Point
Based on the Oliveira et al. (2023) breakfast trial and wider LCD evidence:
• Start with breakfast: Replace high-carbohydrate breakfast (cereal, toast, juice) with a protein-fat-dominant meal (eggs, avocado, Greek yoghurt, nuts). This single change can significantly reduce morning and all-day glucose variability.
• Target 100–130g carbs/day initially: This is achievable and evidence-supported without requiring full ketogenic restriction
• Prioritise carbohydrate quality over quantity alone: Legumes, non-starchy vegetables, and whole grains over refined grains and sugars
• Adopt Mediterranean principles: Olive oil, fatty fish, nuts, and abundant vegetables alongside moderate carbohydrate restriction — the CORDIOPREV evidence supports this as the optimal long-term strategy
• Work with a registered dietitian: Barrea et al. (2025) emphasises that medical nutrition therapy delivered by a dietitian is the evidence-based standard of care
Sample Low-Carb Mediterranean Day (Approximately 100–120g Carbohydrate)
Breakfast: 2–3 eggs scrambled with spinach and feta, ½ avocado, black coffee — ~8g carbohydrate
Mid-morning snack: 30g mixed nuts, small apple — ~20g carbohydrate
Lunch: Large salad with grilled salmon, chickpeas, cucumber, tomato, olives, olive oil and lemon dressing — ~30g carbohydrate
Afternoon snack: Greek yoghurt (full fat, unsweetened) with berries — ~15g carbohydrate
Dinner: Grilled chicken thighs with roasted Mediterranean vegetables (zucchini, peppers, eggplant, cherry tomatoes) and ½ cup quinoa — ~35g carbohydrate
Blood Glucose Monitoring: Practical Guidance
• If you have T2DM, consider continuous glucose monitoring (CGM) or systematic finger-stick testing when making dietary changes
• Test at fasting, 1 hour, and 2 hours post-meal to understand your individual glucose response to specific foods
• Target postprandial glucose < 7.8 mmol/L (140 mg/dL) at 2 hours as a reasonable clinical goal
• Keep a food-glucose diary for the first 4 weeks to identify your personal 'high-response' foods
Frequently Asked Questions
Q1: Is a low-carb diet safe for people with type 1 diabetes?
LCD is used by some people with type 1 diabetes, with evidence of improved time-in-range on CGM. However, it requires very careful insulin dose adjustment and carries euglycaemic DKA risk, particularly with SGLT-2 inhibitor co-use. This should only be done under specialist supervision.
Q2: How quickly can I expect blood sugar improvements on a low-carb diet?
Postprandial glucose improvements can occur within the first meal, as demonstrated by Oliveira et al. (2023). Fasting glucose improvements typically emerge within 1–2 weeks. HbA1c reflects 3-month average glucose and takes at least 8–12 weeks to show meaningful change.
Q3: Will a low-carb diet raise my cholesterol and increase heart attack risk?
LDL may rise on some low-carb approaches, particularly if saturated fat intake increases significantly. However, triglycerides fall, HDL rises, and LDL particle size often improves. The net cardiovascular effect depends on the specific dietary pattern and individual lipid phenotype. Mediterranean-style low-carb approaches tend to have a more favourable cardiovascular profile than generic 'high-fat' approaches.
Q4: What's better — tracking carbs or following a Mediterranean diet?
Not mutually exclusive. The best evidence supports a Mediterranean-style diet with moderate carbohydrate restriction — combining the anti-inflammatory, gut health, and lipid benefits of the Mediterranean approach with the direct glycaemic benefits of carbohydrate reduction. This is essentially what the CORDIOPREV evidence (Boughanem 2025) supports.
Q5: Do I have to go ketogenic to reverse diabetes?
No. While ketogenic diets can produce dramatic short-term improvements, the CORDIOPREV data suggests the Mediterranean diet — which is not ketogenic — produces superior long-term T2DM remission. The most important factors are: meaningful carbohydrate reduction, diet quality, weight management, and long-term adherence.
Q6: Should I count net carbs or total carbs?
For general low-carb eating, most practitioners count total carbohydrates. Net carbs (total carbs minus fibre) is commonly used in ketogenic communities. For clinical glycaemic management, total carbohydrate counting has stronger evidence support and is the approach used in most RCTs.
Q7: How long do I need to follow a low-carb diet to see sustained benefits?
Short-term benefits are demonstrable within weeks. Sustained benefits require long-term adherence. The evidence suggests benefits attenuate at 12+ months if dietary pattern reverts. This underscores that dietary change must be viewed as a permanent lifestyle modification, not a short-term intervention.
Q8: Is a low-fat diet useless for diabetes management?
Not at all. Low-fat diets can be highly effective when implemented as part of a Mediterranean or plant-based pattern, particularly when they displace saturated fat and refined carbohydrates with fibre-rich foods. The evidence against low-fat diets applies specifically to conventionally defined, high-refined-carbohydrate 'low-fat' patterns — not to high-quality, plant-rich, low-fat approaches.
Q9: Can diet alone replace diabetes medication?
For some individuals — particularly those with shorter duration T2DM, higher baseline HbA1c, and preserved beta-cell function — dietary intervention combined with weight loss can produce T2DM remission and allow medication reduction or cessation. This should always occur with medical supervision. It is not achievable or appropriate for all patients with T2DM.
Q10: What's the best diet for weight loss in people with diabetes?
The best diet for weight loss is the one you can sustain. Over 12+ months, LCD and LFD produce similar weight loss. A Mediterranean-style pattern with moderate caloric restriction and high diet quality has the best long-term evidence for combined weight management and metabolic benefit.
Q11: Does fibre intake matter on a low-carb diet?
Critically important. Many low-carb implementations are fibre-deficient, which negatively impacts gut microbiome and bowel function and may undermine some metabolic benefits. Prioritise non-starchy vegetables, nuts, seeds, and legumes (in moderation) to maintain adequate fibre intake even while reducing total carbohydrates.
Q12: Should I try intermittent fasting alongside a low-carb diet?
Intermittent fasting (IF) combined with LCD is a potentially synergistic strategy — both reduce postprandial insulin secretion and may enhance fat oxidation. Emerging evidence suggests benefit for glycaemic control, but robust long-term RCTs in T2DM are lacking. Consult your doctor before starting IF if you take blood glucose-lowering medication, due to hypoglycaemia risk.
13. Conclusion & Action Steps
The science of low-carb vs low-fat diets for blood sugar control is not a simple 'winner takes all' story. It is a nuanced, context-dependent question where individual factors, dietary quality, and long-term adherence matter more than the macronutrient split.
Here is what the totality of current evidence (2021–2026) tells us:
• For glycaemic control: Low-carb diets are more effective than low-fat diets, particularly in the short-to-medium term, with the most pronounced benefits in people with poorly controlled T2DM at baseline.
• For lipids: LCD reduces triglycerides and raises HDL consistently; LDL effects are variable and depend on fat quality.
• For long-term outcomes: The Mediterranean diet may produce superior long-term T2DM remission compared to both conventional LCD and low-fat diets, with additional anti-inflammatory and cardiovascular benefits.
• For individual patients: No single diet is universally optimal. The best diet is the healthiest one a patient can adhere to long-term — ideally guided by a registered dietitian.
• For medication: Dietary change in T2DM requires medical supervision and medication adjustment. Never alter your diabetes medication without consulting your doctor.
Your Evidence-Based Action Steps
Speak to your doctor or diabetes care team before making significant dietary changes
Request a referral to a registered dietitian for personalised medical nutrition therapy
Consider starting with a single-meal change (e.g., low-carb breakfast) to assess your individual glucose response
Adopt Mediterranean diet principles as the foundation — prioritise olive oil, fatty fish, nuts, legumes, and vegetables
Moderate — but don't necessarily eliminate — carbohydrate intake, focusing on quality (legumes, whole grains, non-starchy vegetables)
Use blood glucose monitoring (finger-stick or CGM) to understand your individual response
Target sustainable long-term adherence over aggressive short-term restriction
Revisit your dietary approach every 3–6 months with your healthcare team
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals. That it's not personalized medical advice. If you're implementing changes, consult a doctor/dietitian as emphasized
Related Articles
Why Muscle Health Controls Blood Sugar in Type 2 Diabetes (The Science Explained)
Feed Your Gut, Fuel Your Health: Diet, Microbiota, and Systemic Health | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
Low-Fat vs. Low-Carb: Which Diet is Best for Weight Loss? | DR T S DIDWAL
5 Steps to Reverse Metabolic Syndrome: Diet, Habit, & Lifestyle Plan | DR T S DIDWAL
The Role of Cholesterol in Health and Disease: Beyond the "Bad" Label | DR T S DIDWAL
Lowering Cholesterol with Food: 4 Phases of Dietary Dyslipidemia Treatment | DR T S DIDWAL
References
All references are peer-reviewed, published in high-impact journals, and accessible via PubMed or journal websites.
American Diabetes Association. (2024). 5. Facilitating positive health behaviors and well-being to improve health outcomes: Standards of care in diabetes—2024. Diabetes Care, 47(Suppl 1), S77–S110. https://doi.org/10.2337/dc24-S005
Anagnostou, A., Larumbe-Zabala, E., Fiore, J., Ghigiarelli, J. J., & Naclerio, F. (2026). Effects of energy-matched low- versus high-carbohydrate diets on glycaemic control, lipid profile, and body composition in healthy adults: A systematic review and meta-analysis of randomised controlled trials. European Journal of Nutrition, 65, Article 19. https://doi.org/10.1007/s00394-025-03862-z
Barrea, L., Verde, L., Colao, A., Muscogiuri, G., & Savastano, S. (2025). Medical nutrition therapy for the management of type 2 diabetes mellitus. Nature Reviews Endocrinology, 21(12), 769–782. https://doi.org/10.1038/s41574-025-01161-5
Boughanem, H., Gutierrez-Mariscal, F. M., Arenas-de Larriva, A. P., Alcala-Diaz, J. F., Yubero-Serrano, E. M., Torres-Peña, J. D., Delgado-Lista, J., Ordovas, J. M., Lopez-Miranda, J., & Perez-Martinez, P. (2025). Effect of long-term Mediterranean versus low-fat diet on neutrophil count, and type 2 diabetes mellitus remission in patients with coronary heart disease: Results from the CORDIOPREV study. Nutrition & Diabetes, 15, Article 11. https://doi.org/10.1038/s41387-025-00360-3
Diabetes UK. (2021). Evidence-based nutrition guidelines for the prevention and management of diabetes. https://www.diabetes.org.uk
Estruch, R., Ros, E., Salas-Salvadó, J., Covas, M.-I., Corella, D., Arós, F., Gómez-Gracia, E., Ruiz-Gutiérrez, V., Fiol, M., Lapetra, J., Lamuela-Raventós, R. M., Serra-Majem, L., Pintó, X., Muñoz, M. A., Rubio, M. A., Serra, J., Romero, J., Martínez, J. A., Fitó, M., ... Martínez-González, M. A. (2018). Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. New England Journal of Medicine, 378(25), Article e34. https://doi.org/10.1056/NEJMoa1800345
Hallberg, S. J., McKenzie, A. L., Williams, P. T., Bhanpuri, N. H., Peters, A. L., Campbell, W. W., Hazbun, T. L., Volk, B. M., McCarter, J. P., Phinney, S. D., & Volek, J. S. (2018). Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: An open-label, non-randomized, controlled study. Diabetes Therapy, 9(2), 583–612. https://doi.org/10.1007/s13300-018-0373-9
Kaakyire, D. A., Abdelfattah, OO., Kumar, A., & Qadeer, S. (2025). Efficacy of low-carbohydrate diets versus low-fat diets in glycemic control among patients with type 2 diabetes: A systematic review. Cureus, 17(1), Article e77004. https://doi.org/10.7759/cureus.77004
Korsmo-Haugen, H. K., Brurberg, K. G., Mann, J., & Aas, A. M. (2019). Carbohydrate quantity in the dietary management of type 2 diabetes: A systematic review and meta-analysis. Diabetes, Obesity and Metabolism, 21(1), 15–27. https://doi.org/10.1111/dom.13499
Li, S., Ding, L., & Xiao, X. (2021). Comparing the efficacy and safety of low-carbohydrate diets with low-fat diets for type 2 diabetes mellitus patients: A systematic review and meta-analysis of randomized clinical trials. International Journal of Endocrinology, 2021, Article 8521756. https://doi.org/10.1155/2021/8521756
Oliveira, B. F., Chang, C. R., Oetsch, K., Little, J. P., & Feghali, A. (2023). Impact of a low-carbohydrate compared with low-fat breakfast on blood glucose control in type 2 diabetes: A randomized trial. The American Journal of Clinical Nutrition, 118(1), 209–217. https://doi.org/10.1016/j.ajcnut.2023.04.032
Rinaldi, S., Campbell, E. E., Fournier, J., Davidson, B., & Friedman, R. (2016). A comprehensive review of the literature supporting recommendations from the Canadian Diabetes Association for the use of a plant-based diet for management of type 2 diabetes. Canadian Journal of Diabetes, 40(5), 471–477. https://doi.org/10.1016/j.jcjd.2016.03.003
Sainsbury, E., Kizirian, N. V., Partridge, S. R., Gill, T., Colagiuri, S., & Brand-Miller, J. (2018). Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Research and Clinical Practice, 139, 239–252. https://doi.org/10.1016/j.diabres.2018.02.026
Snorgaard, O., Poulsen, G. M., Andersen, H. K., & Astrup, A. (2017). Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Research & Care, 5(1), Article e000354. https://doi.org/10.1136/bmjdrc-2017-000354
Taylor, R., Al-Mrabeh, A., Zhyzhneuskaya, S., Akpan, C., Barnes, A. C., Kelly, B. L., Davies, P. E., Sattar, N., & Lean, M. E. (2018). Remission of human type 2 diabetes requires decrease in liver and pancreas fat content but is dependent upon capacity for β cell recovery. Cell Metabolism, 28(4), 547–556. https://doi.org/10.1016/j.cmet.2018.07.003
© 2026 | Evidence-Based Health & Nutrition | Last Updated: June 2026