How Strong Legs Protect Your Brain, Metabolism, Blood Sugar, and Mobility as You Age
Learn why strong legs are linked to better metabolism, healthier aging, reduced fall risk, improved brain health, and longer lif
EXERCISEAGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/17/202625 min read
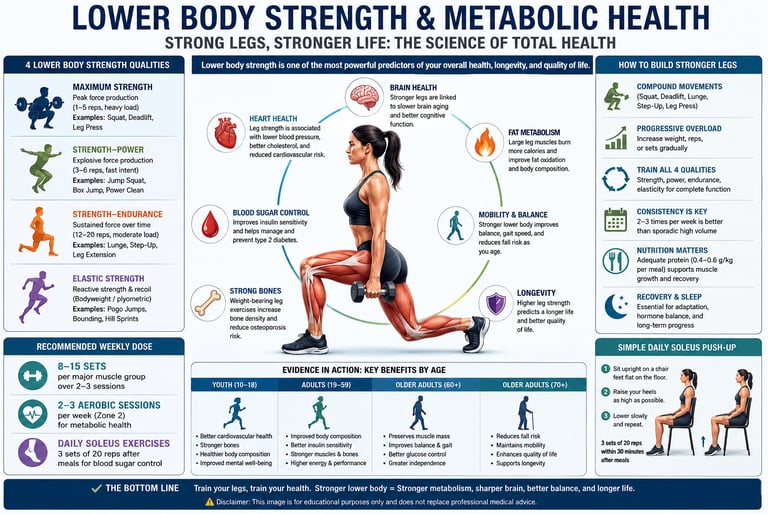
Lower body strength is a powerful biomarker of whole-body health. Evidence from landmark 2025–2026 studies shows stronger legs predict better cardiovascular markers, glucose control, brain aging, balance, and survival. Moderate resistance training of 8–15 sets/muscle/week plus aerobic exercise improves fat oxidation, insulin sensitivity, and mobility in all ages.
Key takeaways,
1. Leg Strength as a Whole-Body Health Biomarker
Lower body strength is a direct indicator of biological age and overall longevity. Stronger glutes, quads, and hamstrings predict superior cardiovascular health, better blood glucose control, higher bone mineral density, and lower mortality rates. This biological pattern remains consistent across all age groups, from youth to older adults.
2. Muscle Quality vs. Muscle Quantity for Fat Burning
When it comes to boosting your metabolic rate and burning fat, muscle quality matters more than sheer muscle mass. Maximal Fat Oxidation (MFO) depends heavily on your VO2 max and mitochondrial density. Implementing a hybrid training split—combining 2–3 strength sessions with 2 aerobic sessions weekly—is the fastest way to optimize fat metabolism.
3. The Optimal Training Volume for Strength and Hypertrophy
According to a massive network meta-analysis of 151 randomized controlled trials (RCTs), the training sweet spot is 8 to 15 sets per muscle group per week.
8–15 Sets: Maximizes strength, lean muscle mass, and physical function.
4–7 Sets: Generates significant health and fitness improvements over a sedentary baseline.
>20 Sets: Triggers diminishing returns and increases workout burnout and dropout risks.
4. Metabolic Signaling: Why Training Intensity Trumps Duration
To trigger beneficial biochemical changes, workout intensity is more effective than long session durations. Creating localized metabolic stress in the lower body releases powerful myokines (such as IL-6, irisin, and BDNF). These signaling proteins directly improve liver glucose uptake, accelerate mitochondrial biogenesis, and enhance brain health. High-intensity lower body circuits can match or beat long, moderate-intensity cardio sessions for metabolic health.
5. The Neuroprotective Link Between Leg Strength and Brain Age
Data from the Baltimore Longitudinal Study of Aging highlights a direct connection between physical frailty and cognitive decline. The combination of low leg strength and an accelerated Brain-Predicted Age (BPA) jointly predicts rapid mobility decline and elevated fall risks. Heavy lower-body training acts as a neuroprotective intervention that preserves both walking speed and cognitive reserve.
6. The Calf and Soleus Muscles: Secrets to Balance and Blood Sugar Control
The lower leg plays a massive role in both mobility and metabolic health:
Calf Strength: Maximal calf capacity directly dictates static balance, dynamic stability, and walking velocity.
Soleus Push-Ups: Performing seated soleus raises immediately after eating activates a specialized metabolic pump. This blunts post-meal glucose spikes and improves blood sugar control without requiring a gym setup.
7. The 4 Essential Strength Qualities for Functional Fitness
A well-rounded longevity workout plan should target four distinct lower-body strength qualities rather than focusing solely on maximum weight:
Maximum Strength: Heavy compound movements (e.g., heavy squats).
Strength-Power: Explosive velocity training (e.g., box jumps).
Strength-Endurance: High-repetition structural capacity (e.g., high-rep lunges).
Elastic Strength: Fast, reactive plyometrics (e.g., reactive bounds).
8. Accessible Training for Age-Related Muscle Loss (Sarcopenia)
Resistance training is highly effective at any age, regardless of equipment access. Clinical trials on sarcopenic adults over age 60 demonstrate robust improvements in physical function from low-to-moderate training volumes. Additionally, research shows that velocity-based training (VBT) allows women to rapidly develop relative power. For individuals with limited mobility, simply performing 3 sets of 20 seated soleus raises post-meal offers a highly effective strategy for glycemic control.
Introduction: Why Your Legs Hold the Key to Whole-Body Health
You might think of leg day as optional—something to squeeze in when you have time. The science says otherwise. A rapidly expanding body of high-quality research now positions lower body strength as one of the powerful, measurable biomarkers of overall human health—predicting cardiovascular risk, metabolic flexibility, brain aging, balance, gait, and survival itself.
Latest landmark studies have confirmed what clinicians on the front line were beginning to suspect: skeletal muscle—especially the large muscle groups of the hips, thighs, and calves—functions as a metabolic organ, a neurological mirror, and a longevity engine, all at once. Whether you are 22 or 82, the strength in your lower limbs tells a story about every organ system in your body.
This comprehensive, evidence-based guide synthesises peer-reviewed studies published in top-tier journals. Each section decodes the underlying biology, critically evaluates the data, discusses clinical relevance, and ends with actionable takeaways.
What You Will Learn in This Guide
• How lower body strength drives fat oxidation and metabolic flexibility
• Why leg strength predicts brain aging and mobility decline
• The difference between muscle mass quantity and muscle quality—and which matters more
• How to train for balance, gait speed, glycaemic control, and power
• Sex-specific adaptations to velocity-based strength training
• Evidence-based training volumes, loads, and frequencies for all ages
• 10 common myths about lower body training—busted
• A practical 4-week starter programme grounded in the latest evidence
1. The Metabolic Science: How Leg Muscles Burn Fat
Local Metabolic Stress as a Systemic Signal
A 2025 paper by Curovic, published in Frontiers in Physiology, challenged the longstanding assumption that training volume is the primary driver of health adaptation. The hypothesis: local metabolic stress—the accumulation of lactate, inorganic phosphate, and hydrogen ions during intense contraction—may be a more potent systemic signal than total sets or repetitions.
When large lower-body muscles work under high metabolic demand, they release myokines—cytokine-like proteins including IL-6, irisin, BDNF, and FGF-21. These molecules circulate systemically, improving mitochondrial biogenesis in distant tissues, enhancing hepatic glucose uptake, reducing visceral fat, and even crossing the blood-brain barrier to support neuroplasticity.
Clinical Relevance and Validity of the Data
Clinical Insight — Metabolic Stress
Validity: Curovic's paper is a hypothesis-driven mechanistic review, not an RCT. The myokine cascade it describes is well-supported by independent in vitro and in vivo data; however, direct causation from condensed training protocols to superior systemic outcomes has not yet been confirmed in large human RCTs.
Clinical Relevance: The practical implication is significant. Short, high-intensity lower-body training bouts (e.g., 20-minute metabolic circuits) may provide metabolic benefits comparable to 60-minute moderate-load sessions. This is directly relevant for adherence in clinical populations with time constraints.
Key Takeaway: Prioritise training intensity over session length when optimising lower body workouts for metabolic health. Working your legs hard and briefly may trigger systemic benefits that rival longer, gentler sessions.
2. Lower Body Strength as a Whole-Body Health Predictor in Youth
The Meta-Analytic Evidence
Moreno-Gonzalez et al. (2025) published a systematic review and meta-analysis in Sports Medicine and Health Science examining lower body muscular strength as a predictor of health indicators across the youth population. Pooling data from dozens of studies, the investigators found consistent, statistically significant associations between leg strength and:
• Favourable cardiovascular markers (lower resting blood pressure, better lipid profiles)
• Improved glycaemic regulation and insulin sensitivity
• Higher bone mineral density
• Better psychological well-being and lower depressive symptom scores
• Reduced prevalence of overweight and obesity
• Superior physical function and lower injury risk
What Does This Mean Clinically?
The meta-analytic design confers relatively high evidence quality, though the authors note substantial heterogeneity across included studies in how 'leg strength' was measured—some used isokinetic dynamometry, others used standing broad jump or vertical jump, and others used leg press 1-RM. This measurement heterogeneity limits precise pooled effect sizes but does not undermine the direction of association, which is consistent across methods.
Clinical Relevance — Youth Strength
Strength screening at school or paediatric clinical visits (using simple field tests like the standing long jump) could serve as a low-cost, non-invasive biomarker of cardiometabolic risk.
Intervention implication: Structured lower-body resistance training in schools may be more impactful for long-term public health than additional cardiovascular exercise alone.
3. Muscle Quality vs. Quantity: What Actually Drives Fat Oxidation?
The Opazo-Díaz Study (2025)
Published in the Journal of the International Society of Sports Nutrition, this study by Opazo-Díaz and colleagues addressed a deceptively simple question: does having more lean mass automatically mean you burn more fat? The answer is nuanced, and clinically important.
The researchers found that maximal fat oxidation (MFO—the peak rate at which the body oxidises fat as fuel) was more closely associated with cardiorespiratory fitness (VO₂max) than with absolute lean mass. In a mediation analysis, VO₂max accounted for a substantial portion of the variance in MFO that lean mass alone could not explain. In other words, two people with identical lean body mass can have vastly different fat-burning capacities depending on their aerobic fitness level.
The Biology Behind the Finding
High cardiorespiratory fitness signals dense mitochondrial networks within skeletal muscle fibres, particularly type I and IIA fibres. More mitochondria per unit of muscle tissue means greater oxidative enzyme activity (citrate synthase, beta-hydroxyacyl-CoA dehydrogenase), a larger capacity to uptake and oxidise fatty acids, and superior metabolic flexibility—the ability to shift fuel use between fat and carbohydrate based on demand.
Clinical Relevance — Muscle Quality
You cannot reliably improve fat oxidation by simply adding muscle mass without also improving aerobic fitness. Resistance training alone, while valuable for metabolic rate, glycaemic control, and insulin signalling, does not maximally upregulate the oxidative machinery within muscle.
Implication for programme design: Hybrid training models that combine 2–3 strength sessions per week with 2 aerobic sessions (zone 2 cycling, brisk walking, swimming) are superior for fat metabolism compared to resistance-only or cardio-only approaches.
4. Resistance Training Volume and Older Adults: The Dose-Response Evidence
Network Meta-Analysis by Radaelli et al. (2025)
This is arguably the most clinically actionable study in the synthesis. Published in Sports Medicine, the authors pooled data from 151 randomised controlled trials involving older adults (mean age ≥60) to identify the optimal resistance training volume for physical function, lean body mass, and lower-body muscle hypertrophy and strength.
Optimal Performance (Moderate Volume): Performing 8–15 sets per muscle group per week yields the best overall results, offering the highest gains in hypertrophy (muscle growth), optimal strength increases, and the greatest improvements in physical functions like chair-rise time, stair-climb speed, and gait velocity.
The Sweet Spot vs. Excess (High Volume): Pushing past 20 sets per muscle group per week triggers diminishing returns. It offers no extra strength benefits compared to moderate volume, slightly worse hypertrophy outcomes, and comes with a higher risk of workout burnout or dropout.
Efficiency of Lower Effort (Low Volume): Even a low commitment of 4–7 sets per muscle group per week is highly effective. While muscle growth is modest, it still delivers moderate strength gains and significant functional physical improvements over doing nothing
Complementary Evidence — Sarcopenia
Yan et al. (2025) in Aging Clinical and Experimental Research conducted a systematic review and meta-analysis specifically in older adults diagnosed with sarcopenia. Their findings aligned closely with Radaelli: progressive resistance training significantly improved muscle strength, physical function, and lean mass in sarcopenic populations, with multi-joint lower-body exercises (squats, leg press, leg extension) producing the largest effect sizes.
Clinical Relevance — Older Adults
The 151-RCT network meta-analysis is the highest-quality evidence synthesis available on this topic. Its conclusions carry substantial clinical weight.
For geriatric clinicians: even frail or pre-sarcopenic patients can safely begin at low volumes (2 sets, 2×/week) and progress. The barrier to entry is lower than most patients believe.
For exercise physiologists: 8–15 sets/muscle/week, delivered across 2–3 sessions, is the evidence-based sweet spot. Beyond this, patient burden increases without proportional benefit.
Consistency over volume: Patients who sustain moderate-volume programmes for 12+ months outperform those who start high-volume programmes and quit at 8 weeks.
5. Leg Strength, Brain-Predicted Age, and Mobility Decline
The Baltimore Longitudinal Study Finding
Vaughan et al. (2025), writing in The Journals of Gerontology, analysed data from the Baltimore Longitudinal Study of Aging—one of the longest-running longitudinal ageing cohorts in the world. Using advanced neuroimaging (machine-learning-derived brain-predicted age, or BPA) and validated measures of leg strength, the researchers asked: which predicts mobility decline more powerfully—brain ageing or leg weakness?
The answer: both, and together they are more predictive than either alone. Individuals whose BPA exceeded their chronological age AND who had low leg strength showed accelerated mobility decline, reduced gait speed, and increased fall risk over follow-up. Conversely, participants with biologically younger brains and strong legs maintained mobility across the study period.
The Bidirectional Neuromuscular Relationship
This bidirectional relationship is biologically coherent. Strong, frequently activated leg muscles send trophic signals (via BDNF, IGF-1) to the motor cortex and cerebellum, maintaining synaptic density and grey matter volume. Meanwhile, a functionally intact corticospinal tract efficiently recruits motor units in leg muscles, preserving force production. When either side of this loop degrades, the other follows.
Clinical Relevance — Brain-Predicted Age
Validity: Longitudinal cohort studies demonstrate association, not causation, but the biological plausibility is strong and consistent across multiple independent cohorts.
Clinical screening: A simple clinical measure of leg strength (e.g., 30-second chair-stand test, handgrip as a proxy) may serve as an early flag for accelerated neurological ageing—well before imaging is warranted.
Therapeutic implication: Resistance training for leg strength should be positioned as a neuroprotective intervention, not merely a musculoskeletal one. This reframing is especially important for patients with early cognitive decline.
6. The Neuromuscular Activation Blueprint: Strength and Running Economy
Zhang et al. (2026) — iScience
Published in iScience, this study used integrated electromyography (iEMG) to map the relationship between lower-limb strength and neuromuscular activation patterns during running. The researchers found that stronger runners exhibited lower co-activation ratios—meaning agonist and antagonist muscles fired more efficiently, with less energy wasted on counterproductive simultaneous contractions.
Greater lower-limb strength was also associated with higher peak muscle activation during push-off, improved force transmission through the kinetic chain, and reduced compensatory activation of proximal muscles (hip flexors, lumbar erectors)—all hallmarks of superior running economy.
Why This Matters Beyond Running
Running is simply a proxy for functional movement quality. The neuromuscular co-activation patterns measured during running reflect the same mechanisms that govern stair climbing, rising from a chair, navigating uneven terrain, and catching oneself during a stumble. In other words, stronger legs are more neurologically efficient legs—and that efficiency protects function across all daily activities.
Clinical Relevance — Neuromuscular Efficiency
The iEMG methodology provides direct, objective evidence of neuromuscular efficiency changes—not just self-reported outcomes. This strengthens the mechanistic argument.
For rehabilitation: Patients recovering from lower-limb injury often present with abnormal co-activation patterns even after pain resolves. Strength training that restores co-activation efficiency should be part of return-to-function protocols.
7. Balance, Gait Velocity, and Fall Prevention in Older Adults
Warneke et al. (2026) and Raudonis et al. (2025)
Two complementary studies address the critical clinical problem of falls in older adults. Warneke et al. (2026), published in Frontiers in Aging, directly measured the association between maximal lower leg strength (calf and ankle musculature) and static balance, dynamic balance, and gait velocity in a sample of older community-dwelling adults.
Their findings were unambiguous: greater lower leg maximal strength was significantly associated with better static balance (single-leg stance time), superior dynamic balance (Timed Up and Go performance), and faster comfortable gait velocity. The association was held after adjusting for age, sex, and BMI.
Raudonis et al. (2025), in Sensors, provided essential normative benchmarking data by quantifying gender- and age-related decline in lower-limb standing muscle strength across a wide age range. Their data revealed that strength decline follows a predictable trajectory that accelerates after age 60—but with substantial individual variation, suggesting that targeted intervention can meaningfully shift an individual above population norms.
The Fall Prevention Case
Falls are the leading cause of injury-related death in adults over 65, and the evidence linking lower limb weakness to fall risk is among the strongest in gerontological research. The Warneke et al. data add granularity by specifically implicating calf and ankle musculature—muscles that are frequently undertrained in standard resistance programmes that emphasise quads and glutes.
Clinical Relevance — Balance and Falls
Warneke et al.'s cross-sectional design, while not proving causation, is supported by a large body of RCT evidence showing that calf-strengthening exercises reduce fall rates. The two bodies of evidence together are clinically compelling.
Programme implication: Calf raises (both seated and standing), ankle dorsiflexion strengthening, and single-leg stance training should be non-negotiable components of fall-prevention programmes—not afterthoughts.
The normative benchmarking from Raudonis et al. is clinically useful: clinicians can now compare a patient's lower-limb strength against age- and sex-matched norms to identify those at highest risk before a fall occurs.
8. Glycaemic Control Without the Gym: Soleus Push-Ups and Non-Weight-Bearing Exercise
Vaishya et al. (2026) — Diabetes & Metabolic Syndrome
One of the most practically significant studies reviewed here comes from Vaishya et al. (2026), published in Diabetes & Metabolic Syndrome: Clinical Research & Reviews. The paper systematically reviewed evidence on non-weight-bearing lower-limb resistance activities—specifically soleus push-ups, calf raises in a seated position, and lower-limb muscle stretching—and their impact on glycaemic control and metabolic-circulatory outcomes.
The soleus muscle, though small relative to the quadriceps or glutes, is metabolically extraordinary. It is predominantly composed of slow-twitch, oxidative fibres that can sustain near-continuous activation for hours without fatigue. When the soleus contracts repetitively (as in standing or seated calf raises), it dramatically increases local glucose and lipid uptake, reducing postprandial blood glucose spikes and improving peripheral insulin sensitivity—even in the absence of whole-body exercise.
The Clinical and Public Health Implications
For patients with type 2 diabetes, obesity, mobility limitations, or post-surgical restrictions, the idea that seated lower-limb exercises performed at a desk or bedside can meaningfully improve metabolic outcomes is transformative. The evidence suggests that 3–4 sets of 10–25 repetitions of soleus push-ups, performed after meals, can blunt postprandial glucose excursions comparably to a short walk.
Clinical Relevance — Glycaemic Control
Validity: The paper is a systematic review, not a primary RCT. The underlying mechanistic evidence (soleus GLUT-4 translocation, oxidative fibre glucose uptake) is robust; head-to-head RCT data comparing soleus exercises to pharmacological glucose lowering are limited.
High practical utility: For bedbound, wheelchair-using, or post-operative patients, this represents a genuinely accessible metabolic intervention with negligible adverse effect risk.
Prescriptive guidance: 3 sets of 20 seated soleus push-ups performed within 30 minutes of a main meal is an evidence-informed starting point. Resistance can be progressively added via ankle weights.
Caution: Patients on sulfonylureas or insulin should monitor glucose if adding significant lower-limb exercise, as hypoglycaemia risk may increase.
9. Velocity-Based Strength Training: Sex-Specific Adaptations
Guo et al. (2026) — Frontiers in Physiology
Velocity-based training (VBT) is an emerging modality in which load prescription is guided by real-time bar velocity feedback rather than a percentage of estimated 1-RM. Guo et al. (2026), published in Frontiers in Physiology, conducted a comparative study of sex-specific adaptations to an 8-week VBT programme targeting the lower limbs.
Key findings: Both men and women showed significant improvements in maximal strength (1-RM squat), peak power output, and muscle thickness (rectus femoris and vastus lateralis via ultrasound). However, men demonstrated greater absolute gains in maximal strength, while women showed proportionally larger gains in relative power output and responded equally well to VBT-guided load prescription. Importantly, the velocity-based approach reduced the overtraining risk inherent in fixed-percentage programmes, as loads were automatically adjusted on days when neuromuscular readiness was lower.
Why Sex-Specific Data Matters Clinically
Most resistance training guidelines are derived from predominantly male cohorts. The Guo et al. data support using VBT as a sex-neutral, auto-regulating tool that respects daily fluctuations in hormonal milieu (particularly relevant across the menstrual cycle in pre-menopausal women) without requiring complex periodisation adjustments.
Clinical Relevance — VBT
The RCT design, use of objective ultrasound measurement for hypertrophy, and sex-stratified analysis represent meaningful methodological strengths.
VBT technology (velocity transducers, linear position transducers) is becoming increasingly accessible. However, low-tech proxies (RPE, bar speed estimation by trained coaches) can approximate VBT principles without specialist equipment.
Clinical populations with hormonal variability (perimenopausal women, men on testosterone therapy, endocrine disorders) may particularly benefit from auto-regulating, velocity-guided load prescription.
10. Classifying Lower Body Strength Qualities: A Data-Driven Framework
Geneau et al. (2025) — International Journal of Sports Science & Coaching
Geneau and colleagues applied data-driven statistical clustering to a battery of lower-body strength tests, identifying four distinct, partially independent strength qualities:
• Maximum Strength — Peak force production capacity (1-RM squat, isometric leg press)
• Strength-Power — Rapid force production (countermovement jump, horizontal jump)
• Strength-Endurance — Sustained force over repetitions (rep-max at 60% 1-RM)
• Elastic Strength — Recoil force during stretch-shortening cycles (reactive jump, sprint acceleration)
The key clinical insight from this classification: elite performance in one quality does not guarantee competence in others. An individual who deadlifts 200 kg (exceptional maximum strength) may have poor elastic strength and high fall risk if their reactive neuromuscular system is undertrained. Conversely, a ballet dancer with excellent elastic and endurance strength may be at risk of bone stress injury due to inadequate maximal strength.
Here is the training design framework
Maximum Strength (High Load, Low Reps)
Protocol: 1–5 repetitions at 85–95% of your 1-Repetition Maximum (1-RM).
Exercises: Squats, Deadlifts, Leg Presses.
Primary Health Benefit: Maximizes muscle mass, builds bone mineral density, and elevates your Basal Metabolic Rate (BMR).
Strength-Power (Explosive Intent, Moderate Reps)
Protocol: 3–6 repetitions at 60–80% 1-RM, performed with maximal explosive speed.
Exercises: Jump Squats, Power Cleans, Box Jumps.
Primary Health Benefit: Crucial for fall prevention and maintaining athletic function.
Strength-Endurance (High Reps, Lower Load)
Protocol: 12–20 repetitions at 50–65% 1-RM.
Exercises: Lunges, Step-Ups, Leg Extensions.
Primary Health Benefit: Enhances overall metabolic health and improves blood sugar (glycaemic) control.
Elastic Strength (Bodyweight & Reactive)
Protocol: Bodyweight-only, focused on quick, springy, reactive movements.
Exercises: Pogo Jumps, Bounding, Hill Sprints.
Primary Health Benefit: Preserves joint mobility and protects walking (gait) quality.
11. Evidence Summary: 10 Studies at a Glance
Level 1 Evidence (Highest Weight: Meta-Analyses & Systematic Reviews)
Radaelli 2025 (Network Meta-Analysis of 151 RCTs): Confirms that 8–15 sets per week is the optimal training volume for maximizing physical function and muscle mass in older adults.
Moreno-Gonzalez 2025 (Systematic Review & Meta-Analysis): Demonstrates that leg strength is a powerful health marker in youth, directly predicting six different health domains.
Yan 2025 (Systematic Review & Meta-Analysis): Proves that resistance training (RT) successfully improves strength, physical function, and muscle mass in older adults suffering from sarcopenia (age-related muscle loss).
Vaishya 2026 (Systematic Review): Highlights that targeting the calf muscle via soleus exercises significantly improves blood sugar (glycaemic) control in individuals with diabetes or metabolic syndrome.
Level 2 Evidence (Randomized Controlled Trials & Prospective Cohorts)
Vaughan 2025 (Longitudinal Cohort Study): Finds that leg strength combined with Brain-Predicted Age (BPA) jointly predict future mobility in older adults, using data from the Baltimore Longitudinal Study of Aging.
Guo 2026 (8-week RCT): Shows that Velocity-Based Training (VBT) effectively improves both strength and power, though notable differences in adaptation exist between sexes.
Level 3 Evidence (Cross-Sectional & Observational Studies)
Opazo-Díaz 2025 (Mediation Analysis): Discovers that cardiovascular fitness (VO₂max) plays a critical role in driving Maximal Fat Oxidation (MFO)—meaning lean muscle mass alone isn't the only factor in fat burning.
Geneau 2025 (Data-Driven Classification): Establishes that lower-body strength in athletes and adults is made up of 4 distinct, independent strength qualities (Maximum, Power, Endurance, and Elastic).
Raudonis 2025 (Normative Study): Provides clear age and sex-specific benchmarks mapping out how lower limb strength naturally declines from ages 20 to over 80.
Warneke 2026 (Cross-Sectional): Identifies a direct link between calf strength, balance, and overall walking (gait) velocity in older adults.
Zhang 2026 (iEMG Study): Shows that dedicated strength training directly improves neuromuscular efficiency (how effectively the brain recruits muscle fibers) in runners.
Level 5 Evidence (Expert & Mechanistic Insight)
Curovic 2025 (Mechanistic Review): Outlines the underlying biology of training, showing that metabolic stress inside a muscle acts as a trigger to release systemic myokines (health-promoting signaling proteins).
12. Common Myths About Lower Body Training—Debunked
Myth 1: “Soreness means your workout worked.”
Reality: DOMS (delayed-onset muscle soreness) reflects muscle damage, not hypertrophy. Van Every et al. (2025) confirmed that mechanical tension and protein synthesis—not damage—drive muscle growth. You can build significant muscle without chronic soreness by managing volume and progression intelligently.
Myth 2: “Cardio is the only way to lose body fat.”
Reality: Resistance training improves insulin sensitivity, increases resting metabolic rate, and—when combined with aerobic exercise—enhances maximal fat oxidation capacity (Opazo-Díaz et al., 2025). Hybrid programmes outperform single-modality approaches for fat loss.
Myth 3: “Only young people benefit from resistance training.”
Reality: The Radaelli et al. (2025) network meta-analysis of 151 RCTs and Yan et al. (2025) in sarcopenic adults demonstrate robust adaptations to resistance training well into the eighth and ninth decades of life.
Myth 4: “You need heavy weights to see results.”
Reality: Moderate loads (60–75% 1-RM) with appropriate volume produce equivalent hypertrophy to heavy loads (>80% 1-RM) when sets are taken close to failure (Van Every et al., 2025). The load matters less than the effort.
Myth 5: “Soleus exercises are only for runners.”
Reality: The soleus is a primary glucose disposal tissue due to its oxidative fibre composition. Seated soleus exercises meaningfully improve postprandial glycaemic control in sedentary and diabetic populations (Vaishya et al., 2026).
Myth 6: “More volume always equals better results.”
Reality: Radaelli et al. (2025) showed diminishing returns above 15 sets/muscle/week in older adults, with higher dropout rates at very high volumes. In clinical populations, sustainability beats maximalism.
Myth 7: “Big muscles mean a healthy metabolism.”
Reality: Opazo-Díaz et al. (2025) demonstrated that cardiorespiratory fitness—not lean mass alone—determines fat oxidation capacity. Muscle quality (mitochondrial density, oxidative capacity) outweighs muscle quantity for metabolic health.
Myth 8: “Leg training is only important for athletes.”
Reality: Leg strength predicts cardiovascular health, mental well-being, bone density, brain-predicted age, fall risk, and gait velocity across all ages (Moreno-Gonzalez et al., 2025; Vaughan et al., 2025; Warneke et al., 2026). It is a universal health priority.
Myth 9: “Women should avoid heavy leg training to avoid ‘bulking up.’”
Reality: Guo et al. (2026) confirmed that women respond to lower-limb strength training with significant strength and power gains, not disproportionate hypertrophy. Hormonal differences (lower testosterone) naturally limit the degree of muscle mass gain in women compared to men.
Myth 10: “One type of leg strength is enough.”
Reality: Geneau et al. (2025) identified four distinct, partially independent lower-body strength qualities. Training only maximum strength, for example, does not adequately develop elastic strength or strength-endurance, leaving functional gaps that increase injury and fall risk.
13. Your Evidence-Based Lower Body Training Blueprint
4-Week Starter Programme (All Fitness Levels)
The following programme synthesises findings from Radaelli et al. (2025), Geneau et al. (2025), Guo et al. (2026), and Warneke et al. (2026). It is designed to address all four strength qualities while remaining sustainable for both beginners and returning exercisers. Consult your healthcare provider before beginning if you have existing musculoskeletal, cardiovascular, or metabolic conditions.
Monday: Maximum Strength Focus
Target: Muscle mass, bone density, and basal metabolic rate.
Exercises: Goblet Squat, Leg Press, Romanian Deadlift, and Calf Raise.
Prescription: 3 sets × 5–6 repetitions at RPE 8 (Rating of Perceived Exertion; leaving ~2 reps in reserve).
Rest Period: 2–3 minutes between sets to maximize recovery.
Tuesday: Aerobic Engine & Metabolic Health
Target: Glycaemic control and cardiovascular base.
Activity: 30 minutes of brisk walking or cycling maintained in Zone 2 Heart Rate.
Targeted Extra: 3 sets × 20 bodyweight seated soleus push-ups performed post-meal to actively lower blood sugar spikes.
Rest Period: Continuous movement.
Wednesday: Strength-Endurance Focus
Target: Metabolic conditioning and tissue capacity.
Exercises: Step-Up, Walking Lunge, Leg Extension, and Seated Calf Raise.
Prescription: 3 sets × 15 repetitions at RPE 7 (challenging but moderate effort).
Rest Period: 60–90 seconds between sets to maintain metabolic stress.
Thursday: Active Recovery
Target: Tissue healing and flushing metabolic waste.
Routine: 15-minute gentle walk, followed by hip flexor stretches, calf stretches, and dedicated foam rolling.
Friday: Power & Elastic Strength
Target: Fall prevention, athletic function, and gait quality.
Exercises & Prescription:
Jumps & Bounds: Box Jumps (or Squat Jumps), Lateral Bounds, and Pogo Hops $\rightarrow$ 3 sets × 5 reps.
Sprints: Hill Sprints $\rightarrow$ 6 rounds × 20 meters.
Rest Period: 2 minutes between sets to ensure full central nervous system recovery.
Saturday: Balance & Gait Preservation
Target: Neuromuscular efficiency and stability.
Routine: 3 total rounds of: Single-leg stance (30 seconds per side), Tandem walk, Backward walk, and Heel-toe walk.
Rest Period: 30 seconds between tasks.
Sunday: Rest Day
Target: Complete systemic recovery.
Prescription: Full passive rest or gentle, non-strenuous yoga.
Progression Rule: Over the 4-week cycle, progress gradually by adding either one additional repetition or a small load increment to your lifting days every 1–2 weeks.
Daily Protein Targets
To support muscle repair, adaptation, and combat age-related muscle loss, aim for these specific nutritional benchmarks:
General Adults (Ages 18–60): Consume 1.6 to 2.2 grams of protein per kilogram of body weight daily.
Older Adults (Ages 60+): Consume 0.4 to 0.6 grams of protein per kilogram of body weight per meal to successfully trigger muscle protein synthesis and overcome anabolic resistance.
Post-Workout Window: Consume 20 to 40 grams of high-quality protein within 2 hours of completing any resistance training session.
Key Progression Principles
• Progressive overload: add 2.5–5 kg or 1–2 reps every 1–2 weeks on major lifts
• Consistent effort: 2–3 sessions per week outperform sporadic 5-session weeks
• Track the basics: weight lifted, reps completed, and a simple RPE rating
• Deload every 4–6 weeks: reduce volume by 40–50% for one week to allow full recovery
14. FAQs: Your Lower Body Strength Questions Answered
Q1. How much lower body exercise do I need per week for metabolic health?
Current evidence (Radaelli et al., 2025) supports 8–15 working sets per major muscle group per week across 2–3 sessions. For glycaemic control specifically, daily low-intensity activity (including seated soleus exercises) provides additional metabolic benefit independent of structured training sessions.
Q2. Can I improve leg strength if I have knee pain?
Yes, with appropriate modifications. Non-weight-bearing exercises (seated leg press, leg extension, seated calf raises, soleus push-ups) allow meaningful strength stimulus with reduced knee joint load. Always consult a physiotherapist for individualised assessment before progressing to weight-bearing exercises.
Q3. Does leg strength training help with weight loss?
Resistance training for leg strength improves insulin sensitivity, increases resting metabolic rate modestly, and—when combined with aerobic exercise—maximises fat oxidation capacity (Opazo-Díaz et al., 2025). It is an essential complement to dietary strategies for sustainable fat loss, primarily by preserving lean mass during a calorie deficit.
Q4. What is the best test to measure lower body strength at home?
The 30-second Chair Stand Test (count how many times you can fully stand from and return to a chair in 30 seconds) is a validated, equipment-free test with published age- and sex-specific norms. The single-leg stance test (time how long you can stand on one leg with eyes open) is a complementary balance measure.
Q5. At what age does lower body strength start to decline significantly?
Raudonis et al. (2025) normative data indicate that lower-limb standing strength begins to decline in the 40s, with the rate of decline accelerating markedly after age 60. However, the decline is not inevitable—regular resistance training can preserve and even increase lower-body strength well into the eighth decade.
Q6. Are soleus push-ups effective for diabetes management?
The emerging evidence from Vaishya et al. (2026) is promising. The soleus muscle’s predominantly oxidative fibre composition makes it uniquely effective at glucose uptake during low-intensity, sustained contraction. Performing 3 sets of 20 repetitions after meals appears to blunt postprandial glucose spikes. This should complement, not replace, prescribed diabetes management.
Q7. Should men and women train legs differently?
The fundamental training principles are the same for both sexes. Guo et al. (2026) confirmed similar absolute improvements from VBT protocols, though men gain more absolute strength and women gain proportionally more in relative power. Women may benefit from auto-regulating training loads across the menstrual cycle, as hormonal fluctuations affect recovery capacity.
Q8. How long does it take to see results from lower body strength training?
Neural adaptations (improved motor unit recruitment, coordination) begin within 2–4 weeks and produce early strength gains before significant hypertrophy occurs. Measurable muscle hypertrophy typically becomes evident after 6–8 weeks of consistent progressive overload. Functional improvements (balance, gait velocity) may be observable within 4–6 weeks in deconditioned older adults.
Q9. Does leg training really improve brain health?
The Vaughan et al. (2025) data from the Baltimore Longitudinal Study of Aging, combined with the established BDNF-exercise literature, provide strong evidence for a bidirectional neuromuscular–neurological relationship. Regular lower-limb resistance training appears to support motor cortex integrity, slow brain-predicted aging, and reduce mobility decline. It is not a cure for neurodegeneration, but it is one of the most effective modifiable protective factors.
Q10. Can I build lower body strength just by walking?
Walking provides a cardiovascular and mild muscular endurance stimulus, but it is insufficient to produce progressive strength gains in most adults above beginner fitness levels. To build meaningful lower-body strength, exercises that progressively overload the major lower-limb muscles (squats, deadlifts, leg press, lunges, step-ups) are required.
Q11. How important is calf strength for older adults?
Warneke et al. (2026) demonstrated that maximal lower leg (calf and ankle) strength is a significant independent predictor of static balance, dynamic balance, and gait velocity in older adults. Calf strength is often overlooked in standard resistance programmes—it should be specifically trained through standing and seated calf raises, and ankle strengthening exercises.
Q12. What is the minimum effective dose of resistance training for metabolic benefit
Even 2 weekly resistance training sessions targeting major lower-body muscle groups (at 8–12 sets total per session) produce clinically meaningful improvements in insulin sensitivity, lean mass, and physical function. For those unable to perform structured sessions, daily soleus push-ups and calf raises provide a genuine metabolic benefit with negligible time investment.
15. Conclusion and Action Steps
Lower body strength is not a performance metric—it is a health vital sign. The convergence of evidence from ten landmark studies published between 2025 and 2026 leaves little doubt: the strength in your legs predicts the health of your heart, the efficiency of your metabolism, the sharpness of your brain, the steadiness of your balance, and the trajectory of your aging.
The biological mechanisms are clear and mutually reinforcing. Large lower-limb muscles act as metabolic organs, releasing myokines that improve systemic insulin sensitivity and fat oxidation. The neuromuscular loop between the motor cortex and leg musculature sustains both brain health and mobility. The soleus’s unique oxidative fibre composition makes even seated lower-leg exercises a meaningful metabolic intervention. And the four distinct strength qualities—maximum, power, endurance, elastic—each contribute uniquely to functional health and longevity.
The practical prescription is neither extreme nor complicated: train your lower body 2–3 times per week with progressive overload, include aerobic conditioning to ensure your muscle tissue is metabolically active, eat adequate protein, balance your sessions across strength qualities, and add daily soleus exercises after meals if metabolic health is a priority.
Your 5 Evidence-Based Action Steps
1. Strength train your lower body 2–3 times per week at 8–15 sets per major muscle group. Prioritise squats, deadlifts, lunges, step-ups, and calf raises.
2. Add 2 aerobic sessions per week (zone 2 intensity) to improve the metabolic quality of your muscle tissue and maximise fat oxidation.
3. Perform 3 sets of 20 seated soleus push-ups after your two largest meals each day—especially if you have elevated blood glucose or a sedentary occupation.
4. Include balance and elastic strength work (single-leg stance, pogo hops, lateral bounds) at least once per week to protect against falls and preserve mobility.
5. Eat 0.4–0.6 g of high-quality protein per kg body weight per meal to support muscle protein synthesis—especially important after age 60.
⚠️ Medical Disclaimer: This article is intended for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before starting or modifying an exercise programme, particularly if you have existing health conditions including cardiovascular disease, diabetes, hypertension, osteoporosis, or musculoskeletal disorders.
Related Articles
The Science of Strength Training: How Building Muscle Improves Fat Loss, Heart Health, and Longevity
Reversing Type 2 Diabetes: Skeletal Muscle as a Master Regulator of Metabolic Health | DR T S DIDWAL
How to Build a Disease-Proof Body: Master Calories, Exercise & Longevity | DR T S DIDWAL
Lower Blood Pressure Naturally: Evidence-Based Exercise Guide for Metabolic Syndrome | DR T S DIDWAL
Exercise vs. Diet Alone: Which is Best for Body Composition? | DR T S DIDWAL
Cardiorespiratory Fitness: The Most Important Predictor of Health and Longevity You Can Improve
References
1. Curovic, I. (2025). The role of resistance exercise-induced local metabolic stress in mediating systemic health and functional adaptations: Could condensed training volume unlock greater benefits beyond time efficiency? Frontiers in Physiology, 16, Article 1549609. https://doi.org/10.3389/fphys.2025.1549609
2. Geneau, M. C., Gastin, P. B., Robertson, S., & James, L. P. (2025). Classification of lower body strength qualities: A data-driven approach. International Journal of Sports Science & Coaching, 20(2), 788–811. https://doi.org/10.1177/17479541251314131
3. Guo, L., Suo, L., Xue, W., Yang, J., Lv, X., Qi, H., Hao, M., Zhao, L., Yang, X., & Han, W. (2026). The effect of velocity-based strength training on lower limb maximal strength, power, and muscle thickness: A comparative study of sex-specific adaptations. Frontiers in Physiology, 17, Article 1787790. https://doi.org/10.3389/fphys.2026.1787790
4. Moreno-Gonzalez, L., Alonso-Callejo, A., Felipe, J. L., Manzano-Carrasco, S., Gallardo, L., & Garcia-Unanue, J. (2025). Lower body muscular strength as a predictor of health indicators in youth population: A systematic review and meta-analysis. Sports Medicine and Health Science. https://doi.org/10.1016/j.smhs.2025.06.004
5. Opazo-Díaz, E., Corral-Pérez, J., Pérez-Bey, A., Marín-Galindo, A., Montes-de-Oca-García, A., Rebollo-Ramos, M., … Ponce-González, J. G. (2025). Is lean mass quantity or quality the determinant of maximal fat oxidation capacity? The potential mediating role of cardiorespiratory fitness. Journal of the International Society of Sports Nutrition, 22(1). https://doi.org/10.1080/15502783.2025.2455011
6. Radaelli, R., Rech, A., Molinari, T., Markarian, A. M., Petropoulou, M., Granacher, U., Hortobágyi, T., & Lopez, P. (2025). Effects of resistance training volume on physical function, lean body mass and lower-body muscle hypertrophy and strength in older adults: A systematic review and network meta-analysis of 151 randomised trials. Sports Medicine, 55(1), 167–192. https://doi.org/10.1007/s40279-024-02123-z
7. Raudonis, V., Staneikaite, V., Kubiliūtė, U., Kubilius, R., Grube, S., Neidhardt, M., Schlaefer, A., & Tankevičius, G. (2025). Gender and age-related decline in lower limb standing muscle strength: Benchmarking for rehabilitation assessment. Sensors, 26(1), 69. https://doi.org/10.3390/s26010069
8. Vaishya, R., Vaish, A., Gopinathan, P., & Misra, A. (2026). Non-weight-bearing lower-limb simple resistance activities, soleus push-ups, and muscle stretching: Impact on glycemic control and metabolic–circulatory outcomes. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 20(2), Article 103375. https://doi.org/10.1016/j.dsx.2026.103375
9. Van Every, D. W., Lees, M. J., Wilson, B., Nippard, J., & Phillips, S. M. (2025). Load-induced human skeletal muscle hypertrophy: Mechanisms, myths, and misconceptions. Journal of Sport and Health Science, in press, Article 101104. https://doi.org/10.1016/j.jshs.2025.101104
10. Vaughan, B. A., Muniz-Terrera, G., Simon, J. E., Grooms, D. R., Clark, B. C., Davatzikos, C., Erus, G., Tian, Q., Ferrucci, L., Resnick, S. M., & Simonsick, E. M. (2025). The predictive power of brain-predicted age and leg strength on mobility decline in aging: Findings from the Baltimore Longitudinal Study of Aging. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 80(12), glaf222. https://doi.org/10.1093/gerona/glaf222
11. Warneke, K., Stotz, A., Konrad, A., & Zech, A. (2026). Association between maximal lower leg strength and static and dynamic balance as well as gait velocity in older adults. Frontiers in Aging, 7, Article 1736517. https://doi.org/10.3389/fragi.2026.1736517
12. Yan, R., Chen, Y., Zhang, R. et al. (2025). Optimal resistance training prescriptions to improve muscle strength, physical function, and muscle mass in older adults diagnosed with sarcopenia: A systematic review and meta-analysis. Aging Clinical and Experimental Research, 37, 320. https://doi.org/10.1007/s40520-025-03235-w
13. Zhang, Q., Van Hooren, B., Girard, O., Trowell, D., Jiang, S., Zeng, W., Chen, S., Zhang, Q., & Li, F. (2026). Exploring the relationship between lower-limb strength and neuromuscular activation in running: Insights from integrated EMG. iScience, 29(2), Article 115232. https://doi.org/10.1016/j.isci.2026.115232
Dr. T.S. Didwal, M.D. (Internal Medicine) | Evidence-Based Health & Nutrition
Published June 2026 | © All rights reserved