Reversing Type 2 Diabetes: Skeletal Muscle as a Master Regulator of Metabolic Health
Stop just managing diabetes—start reversing it. Discover how lifting weights transforms your muscles into endocrine powerhouses that lower blood sugar and "cool down" systemic inflammation
DIABETES
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/30/202620 min read
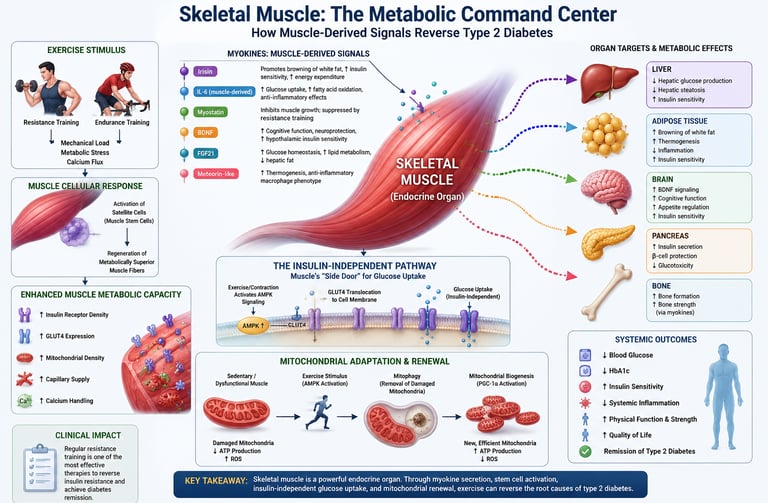
For decades, type 2 diabetes was framed as a progressive, one-way decline managed but rarely reversed. That narrative is changing. Skeletal muscle is not just for movement; it is a powerful endocrine organ that secretes more than 600 signaling molecules, or myokines, which talk directly to the liver, pancreas, fat, and brain to improve glucose control and calm inflammation (Iglesias, 2025).
When we contract a muscle against resistance, we activate a metabolic “side door.” AMPK-mediated GLUT4 translocation pulls glucose from blood into muscle cells even when insulin signaling is impaired, offering immediate relief to high blood sugar (Masuda & Matsuzaka, 2025). The benefits persist for 24–48 hours as muscles replenish glycogen stores, creating a sustained glucose sink.
Resistance training does more than move glucose today; it rebuilds the machinery for tomorrow. Loading activates dormant satellite cells, producing muscle with higher insulin receptor density, greater GLUT4 expression, and healthier mitochondria (Fukada & Nakamura, 2021). It also renews mitochondrial networks and reduces oxidative stress, a key driver of insulin resistance (Wilkinson et al., 2025).
The clinical impact is concrete. Meta-analysis of middle-aged and older adults shows resistance training lowers HbA1c by 0.5–0.8%, reduces CRP and TNF-α, decreases visceral fat, and increases lean mass—effects comparable to some medications, without pharmacologic side effects (Wang et al., 2025).
This is not lifestyle advice tacked onto prescriptions. It is physiology. Two to three sessions weekly at 60–80% of one-rep max can meaningfully shift the trajectory of type 2 diabetes (Zierath et al., 2025). Muscle is not passive. When we train it, it fights back. For patients and clinicians alike, that makes resistance training a first-line therapy, not a footnote.
Can Resistance Training Help Achieve Diabetes Remission?
While resistance training alone does not guarantee diabetes remission, growing evidence suggests it can be a powerful contributor to remission when combined with weight loss, nutritional therapy, and sustained lifestyle change. Diabetes remission is generally defined as maintaining an HbA1c below 6.5% for at least three months without glucose-lowering medications. By increasing muscle mass, improving insulin sensitivity, reducing visceral fat, and enhancing glucose disposal, resistance training directly targets several biological mechanisms underlying type 2 diabetes. For many individuals, exercise serves not merely as symptom management but as a cornerstone of metabolic recovery and long-term disease remission.
Clinical Pearl: The goal is not simply lower blood sugar—it is restoring metabolic health. Resistance training helps rebuild the body's largest glucose-regulating organ: skeletal muscle.
Key takeaways
Muscle is an endocrine organ: Active skeletal muscle secretes 600+ myokines that lower blood sugar, reduce inflammation, and improve insulin sensitivity (Iglesias, 2025).
Resistance training lowers HbA1c 0.5–0.8%: Meta-analysis shows 2–3 sessions/week deliver reductions equal to some diabetes drugs, with no side effects (Wang et al., 2025).
Exercise bypasses insulin resistance: Muscle contraction activates AMPK, moving GLUT4 to the cell surface so glucose enters without insulin (Masuda & Matsuzaka, 2025).
Glucose control lasts 24–48 hours post-workout: Muscles keep pulling in blood sugar to rebuild glycogen after resistance exercise, even when insulin signaling is impaired.
New muscle is metabolically better: Resistance training activates satellite cells, creating muscle with higher insulin receptor density and more mitochondria (Fukada & Nakamura, 2021).
Reduces systemic inflammation: Resistance training significantly lowers CRP, TNF-α, and chronic IL-6 — key drivers of insulin resistance (Wang et al., 2025).
Minimum effective dose is 2x per week: 2–3 resistance sessions weekly at 60–80% 1RM for 8–12 weeks improves HbA1c, fasting glucose, and visceral fat.
Targets visceral fat directly: Resistance training reduces dangerous organ fat that drives insulin resistance, while increasing lean mass for glucose disposal (Wang et al., 2025).
It’s not too late to start: Adults and older adults see significant metabolic benefits; satellite cells respond to resistance training at any age (Wang et al., 2025).
Protein amplifies results: 1.6–2.2 g/kg bodyweight daily optimizes muscle protein synthesis and metabolic adaptations from training.
Skeletal Muscle as an Endocrine Organ
The idea that muscles do more than move your body has transformed metabolic medicine over the last decade.
Skeletal muscle comprises roughly 40% of total body mass and accounts for 70–80% of insulin-stimulated glucose disposal. But a landmark 2025 review in the Journal of Clinical Medicine confirmed something even more remarkable: muscle tissue actively participates in endocrine regulation, producing a vast array of peptides, cytokines, and metabolites that act on distant organs (Iglesias, 2025).
These muscle-derived signaling molecules—called myokines—are secreted in response to mechanical loading, metabolic stress, and calcium flux during contraction. They constitute a molecular language between your muscles and the rest of your body, continuously broadcasting information about energy status and physical demand.
Key Myokines and Their Metabolic Roles
Here is a breakdown of the key myokines, their roles, and the metabolic impact of muscle loss, rewritten into clear, scannable points:
Irisin: Promotes the "browning" of white fat, which increases resting energy expenditure and directly improves insulin sensitivity. It is released during both resistance and endurance training.
IL-6 (Muscle-Derived): Enhances glucose uptake and boosts fatty acid oxidation (fat burning) during active exercise. This healthy, acute release contrasts sharply with the chronic, inflammatory IL-6 secreted by fat tissue in obesity.
Myostatin: Acts as a natural brake to limit muscle growth. Resistance training actively suppresses myostatin expression, lifting the brake to create a metabolically favorable, muscle-building environment.
BDNF (Brain-Derived Neurotrophic Factor): Supports cognitive function and protects brain neurons. Emerging data suggests it may also improve insulin sensitivity within the hypothalamus (the brain's metabolic control center).
FGF21 (Fibroblast Growth Factor 21): Optimizes glucose balance, improves lipid (fat) metabolism, and actively reduces fat accumulation in the liver.
Meteorin-Like: Stimulates calorie-burning thermogenesis in fat tissue and shifts immune cells toward an anti-inflammatory state, effectively cooling systemic metabolic inflammation.
The Stem Cell Science: How Exercise Rejuvenates Muscle
Within each muscle fiber lie dormant repair units called satellite cells (muscle stem cells). In sedentary individuals—and especially in people with metabolic disease—these cells enter deep quiescence, reducing regenerative capacity and contributing to progressive muscle wasting.
A pivotal 2021 study by Fukada and Nakamura, published in Endocrinology and Metabolism, demonstrated that resistance exercise activates these dormant satellite cells through specific molecular signaling cascades, including Notch and Wnt pathways. The resulting muscle regeneration produces tissue with qualitatively superior metabolic properties.
Why New Muscle Is Metabolically Superior
Muscle fiber regenerated through exercise-induced satellite cell activation has measurably better characteristics for glucose management:
Higher insulin receptor density — more "docking ports" for insulin on the cell surface
Enhanced GLUT4 expression — greater baseline capacity for glucose transport
Improved mitochondrial density — more efficient energy production and less lipotoxic metabolite accumulation
Greater capillary supply — faster delivery of glucose and insulin to the fiber
Better calcium signaling — improved muscle contraction and metabolic coordination
A 2025 review in Frontiers in Cell and Developmental Biology further characterized these regenerative mechanisms, showing that exercise-induced satellite cell proliferation is impaired in chronic metabolic disease, making targeted resistance training even more critical to restore this capacity (Jin et al., 2025).
Clinical Insight
Muscle stem cell activation doesn't just add size—it fundamentally upgrades metabolic hardware. In people with type 2 diabetes, where existing muscle is metabolically dysfunctional, this regenerative process may be even more therapeutic than in healthy individuals.
The Insulin-Independent Pathway: Muscle's "Side Door" for Glucose
One of the most clinically significant discoveries in exercise metabolism is that working muscle can import glucose from the bloodstream through a pathway that completely bypasses the insulin receptor.
In type 2 diabetes, the main insulin-dependent glucose uptake pathway is impaired. Insulin binds its receptor, but the downstream signaling cascade—involving IRS-1, PI3K, Akt, and ultimately GLUT4 translocation—is disrupted at multiple points. This is the essence of insulin resistance.
How Exercise Bypasses Insulin Resistance
Here is the breakdown of how exercise bypasses insulin resistance, organized into clear, scannable points:
The "Side Door" Mechanism for Glucose Clearance
Bypassing the Blockage: In type 2 diabetes, the standard "front door" for clearing blood sugar is broken because insulin signaling is blocked. However, muscle contraction creates an entirely independent pathway to pull sugar out of the bloodstream.
The Power of AMPK: Physical movement activates a cellular energy sensor called AMPK (AMP-activated protein kinase). AMPK acts as an alternative manager, signaling the cell to absorb fuel without needing insulin's permission.
The 4-Step Cellular Process
Step 1: Energy Depletion (Mechanical Loading): As you lift weights or exercise, your muscles rapidly burn through their immediate energy stores (ATP). This sudden energy drain triggers the activation of AMPK.
Step 2: Mobilizing the Transporters (GLUT4 Translocation): Once active, AMPK bypasses the faulty insulin pathways and directly signals GLUT4 (glucose transport proteins) inside the cell to move up to the cell's outer surface.
Step 3: Rapid Blood Sugar Absorption: With GLUT4 transporters successfully docked on the muscle cell membrane, they act like open channels, rapidly pulling glucose out of your blood to fuel the working muscle.
Step 4: The 48-Hour "Glucose Sink": After your workout ends, your muscles need to rebuild their stored energy (glycogen). This recovery process keeps the "side door" open, maintaining lowered blood sugar levels for 24 to 48 hours after a single exercise session.
What the Latest Science Shows
A Thousand Molecular Changes: A landmark 2025 study mapping muscle tissue found that a single bout of exercise triggers over 1,000 distinct molecular changes (phosphorylation events), explaining why exercise is such a powerful metabolic medicine.
Highly Personalized Responses: This same mapping research revealed that exactly how efficiently this "side door" opens varies from person to person, depending on the unique chemical environment inside their individual muscles.
Mitochondrial Renewal: Clearing the Metabolic Engines
In type 2 diabetes, skeletal muscle mitochondria are characteristically dysfunctional—fewer in number, structurally abnormal, and producing excessive reactive oxygen species (ROS). This mitochondrial dysfunction directly impairs insulin signaling and accelerates metabolic deterioration.
A 2025 paper in the International Journal of Molecular Sciences specifically examined redox homeostasis in metabolic syndrome and type 2 diabetes, demonstrating that oxidative stress in skeletal muscle mitochondria is a primary driver of insulin resistance—not merely a byproduct of it (Wilkinson et al., 2025).
Exercise-Induced Mitochondrial Biogenesis
Resistance training activates PGC-1α, the master regulator of mitochondrial biogenesis. Through this pathway, exercise literally triggers the creation of new, functionally superior mitochondria while clearing damaged ones via mitophagy (selective autophagy of defective organelles).
The metabolic effects of this renewal are significant:
Greater capacity to oxidize both glucose and fatty acids, reducing toxic lipid intermediates that impair insulin signaling
Reduced ROS production per unit of energy output, lowering chronic oxidative stress
Improved calcium handling within the cell, which coordinates metabolic and contractile function
Enhanced coupling efficiency—more ATP produced per molecule of glucose or fat consumed
Cooling Metabolic Fire: Exercise and Systemic Inflammation
Type 2 diabetes is now understood to be as much an inflammatory disease as a metabolic one. Chronic low-grade inflammation—driven by dysfunctional adipose tissue, gut dysbiosis, and immune dysregulation—directly impairs insulin receptor signaling in muscle and other tissues.
Skeletal muscle, when exercised regularly, actively counteracts this inflammatory milieu through two mechanisms: direct anti-inflammatory myokine secretion and long-term reductions in adipose-derived inflammatory signals as body composition improves.
The Evidence: What Resistance Training Does to Inflammatory Markers
A comprehensive meta-analysis by Wang, Fan, and Wang (2025) in Diabetes Research and Clinical Practice synthesized data from multiple randomized controlled trials examining resistance training in middle-aged and older adults with type 2 diabetes. The inflammatory findings were striking:
C-Reactive Protein (CRP) drops significantly: This is the primary clinical marker of systemic inflammation. Lowering it directly reduces your overall cardiovascular risk and helps restore baseline insulin sensitivity. (Evidence Quality: Strong)
TNF-α is heavily suppressed: Tumor Necrosis Factor-alpha (TNF-α) is a major culprit that actively destroys your insulin receptors. By suppressing it, your existing insulin immediately becomes more effective. (Evidence Quality: Strong)
Resting IL-6 levels are reduced: While muscles release a healthy spike of interleukin-6 (IL-6) during a workout to burn fat, regular training drastically lowers your baseline, resting levels of the damaging, inflammatory IL-6 secreted by fat tissue. (Evidence Quality: Strong)
IL-10 receives a powerful boost: Interleukin-10 (IL-10) is one of your body’s premier anti-inflammatory defenders. Boosting it helps protect your pancreas and immune system from metabolic stress. (Evidence Quality: Moderate)
Adiponectin levels increase: This protective hormone acts like a cellular cleaner. Higher levels directly stimulate your cells to absorb glucose and oxidize (burn) floating fatty acids. (Evidence Quality: Moderate)Critically, the 2025 review by Zierath and colleagues in the Journal of Sport and Health Science confirmed that these inflammatory improvements arise from multiple interconnected pathways—not a single mechanism—making the effect robust and difficult to reproduce pharmacologically (Zierath et al., 2025).
Meta-Analysis Evidence: Quantified Clinical Benefits
Understanding biological mechanisms is compelling—but the clinical question matters most: how much does resistance training actually improve outcomes in people with type 2 diabetes? The evidence is now both substantial and precise.
Here is the breakdown of the clinical, quantified benefits of resistance training for managing and reversing type 2 diabetes:
The Quantified Benefits of Muscle Training
While understanding cellular pathways is fascinating, what matters most is the real-world clinical impact. When you look at the data from large-scale clinical trials on adults with type 2 diabetes, resistance training delivers powerful, measurable improvements across every major marker of metabolic health:
HbA1c drops by 0.5% to 0.8%: Your HbA1c is your 3-month blood sugar average. In medicine, any drop greater than 0.5% is considered a major clinical milestone. Resistance training hits this threshold natively, often matching or exceeding the impact of common first-line diabetes medications.
Fasting Blood Glucose falls significantly: Regular training fundamentally improves your basal (resting) metabolic rate. This means your body handles blood sugar more efficiently even while you sleep, leading to noticeably lower numbers on your morning finger-prick or continuous glucose monitor (CGM).
Insulin Sensitivity improves drastically: Training makes your cells highly responsive to your hormones. As a result, your pancreas doesn't have to pump out massive, exhausting amounts of insulin just to manage a standard meal.
Lean Muscle Mass increases measurably: By building physical tissue, you are quite literally building a larger permanent "metabolic sink" to absorb circulating blood sugar throughout the day.
Muscle Strength sees substantial gains: Beyond looking or feeling stronger, increased physical strength is heavily correlated in long-term medical data with a lower risk of all-cause mortality in diabetic patients.
Visceral Fat drops noticeably: Visceral fat is the dangerous, inflammatory fat wrapped around your deep internal organs (like your liver and pancreas). Reducing it removes the primary physiological block that causes insulin resistance in the first place.
C-Reactive Protein (CRP) declines significantly: Lowering this key inflammatory marker directly defuses systemic irritation, providing massive protection for your blood vessels and heart.
A key finding from the meta-analysis: benefits were observed across diverse populations, varied training protocols, and different study durations—suggesting the metabolic response to resistance training is consistent and broadly applicable, not limited to specific subgroups.
How much can resistance training lower HbA1c? Meta-analysis data from 2025 shows resistance training reduces HbA1c by 0.5–0.8% on average in people with type 2 diabetes—a clinically significant reduction equivalent to some glucose-lowering medications, achieved without pharmacological side effects.
Evidence-Based Resistance Training Protocol
Although training programs should be individualized, research consistently identifies several key principles that improve blood sugar control, insulin sensitivity, and overall metabolic health in people with type 2 diabetes.
Core Training Recommendations
Frequency: Train 2–3 times per week on non-consecutive days.
Intensity: Use weights equivalent to 60–80% of your one-repetition maximum (1RM)—challenging enough to stimulate muscle growth while maintaining good technique.
Exercise Selection: Perform 8–10 exercises that collectively target all major muscle groups.
Training Volume: Complete 2–3 sets per exercise.
Repetition Range: Aim for 8–12 repetitions per set, finishing each set close to muscular fatigue.
Rest Intervals: Rest approximately 60–90 seconds between sets.
Progressive Overload: Gradually increase resistance, repetitions, or training volume as strength improves.
Time to Benefit: Most studies report meaningful improvements in HbA1c and insulin sensitivity after 8–12 weeks of consistent training.
Protein Intake: To maximize muscle adaptation, consume approximately 1.6–2.2 g of protein per kilogram of body weight daily.
Recommended Foundation Exercises
Exercises that engage large muscle groups produce the greatest metabolic benefits because they increase glucose uptake and energy expenditure.
Consider prioritizing:
Squats or Leg Presses – recruit the body's largest muscle groups and create substantial glycogen demand.
Deadlifts or Romanian Deadlifts – activate the posterior chain, including the glutes, hamstrings, and lower back.
Seated Rows or Lat Pulldowns – train large upper-back muscles and enhance overall muscle mass.
Chest Presses (machine, dumbbell, or barbell) – develop upper-body pushing strength.
Overhead Presses – engage the shoulders and upper body while improving functional strength.
Hip-Hinge Movements – target the glutes and hamstrings, which are among the body's most metabolically active muscles.
Safety Considerations
Individuals taking insulin or sulfonylurea medications should be aware that exercise can increase the risk of hypoglycemia during and after training sessions. Blood glucose should be monitored before exercise and, when appropriate, for several hours afterward. As fitness and insulin sensitivity improve, medication requirements may change, making regular communication with a healthcare professional essential.
Common Myths About Resistance Training and Type 2 Diabetes
Myth: "Cardio is better than weight training for blood sugar control."
Reality: Both aerobic and resistance exercise improve insulin sensitivity, but they do so through different biological pathways. Aerobic exercise enhances cardiovascular fitness and glucose utilization, while resistance training builds skeletal muscle—the body's largest site for glucose disposal. It also stimulates the release of beneficial myokines and improves long-term metabolic capacity. Research shows that resistance training alone can produce clinically meaningful reductions in HbA1c. For optimal metabolic health, combining both forms of exercise is ideal.
Myth: "I'm too old to benefit from strength training."
Reality: Age does not eliminate the body's ability to adapt. Studies involving middle-aged and older adults consistently demonstrate improvements in muscle mass, strength, insulin sensitivity, and glycemic control following resistance training. Although older adults may require a more gradual progression, muscle stem cells and adaptive pathways remain responsive throughout life.
Myth: "You need a gym to get meaningful results."
Reality: Effective resistance training does not require expensive equipment. Bodyweight exercises, resistance bands, and simple home-based programs can all improve strength and metabolic health. The key principle is progressive overload—gradually increasing the challenge placed on the muscles over time.
Myth: "Exercise is only a supplement to medication."
Reality: Resistance training is far more than a lifestyle add-on. It directly targets several root causes of type 2 diabetes, including insulin resistance, chronic inflammation, mitochondrial dysfunction, and loss of muscle mass. Through mechanisms such as satellite cell activation, mitochondrial biogenesis, myokine secretion, and insulin-independent glucose uptake, exercise produces metabolic effects that complement—and sometimes reduce the need for—pharmacological therapy under medical supervision.
Myth: "Only cardio lowers blood sugar."
Reality: Resistance training can lower blood glucose as effectively as aerobic exercise. Muscle contractions activate an insulin-independent pathway that moves GLUT4 transporters to the muscle cell surface, allowing glucose to enter cells even when insulin signaling is impaired. In addition, muscles continue drawing glucose from the bloodstream for up to 24–48 hours after training as they replenish glycogen stores.
Frequently Asked Questions
How quickly will resistance training lower my blood sugar?
A single bout of resistance exercise can lower blood glucose for up to 24–48 hours, as muscle draws on blood glucose to replenish glycogen stores. Improvements in insulin sensitivity begin within 2–4 weeks of regular training. Meaningful reductions in HbA1c—the 3-month average blood sugar marker—typically appear after 8–12 weeks of consistent training, with studies showing 0.5–0.8% reductions in people with type 2 diabetes.
Can I still benefit if I'm already on diabetes medications?
Absolutely—and the combination can be particularly powerful. Resistance training works through mechanisms that are entirely distinct from most diabetes medications. Many people find that, under medical supervision, medication requirements decrease as metabolic fitness improves. Never adjust medication independently; always work with your prescribing physician.
What's the minimum effective "dose" of resistance training for blood sugar benefits?
Research consistently shows that 2 sessions per week of 30–45 minutes produces clinically meaningful improvements. Three sessions per week is optimal for most outcomes. More frequent training doesn't necessarily produce proportionally better results and may impair recovery—an important consideration for people managing metabolic disease.
Should I check my blood glucose before exercising?
For people managing diabetes with insulin or sulfonylureas, yes. A pre-exercise glucose below 5.5 mmol/L (100 mg/dL) warrants a carbohydrate snack before training. Above 16 mmol/L (290 mg/dL) warrants postponing exercise until glucose is better controlled. For people managing diabetes through diet and lifestyle alone, monitoring is still advisable when establishing a new exercise routine. Your diabetes care team can help establish personalized glucose targets for exercise.
Is there a difference between machine-based and free-weight resistance training for metabolic outcomes?
From a metabolic standpoint, both modalities produce equivalent improvements in insulin sensitivity and glucose control when matched for intensity and volume. Free weights recruit additional stabilizer muscles and may provide marginally greater overall muscle activation, but machines are safer for beginners and allow precise loading. The best choice is the one you'll perform consistently and safely.
How does protein intake affect the metabolic benefits of resistance training?
Adequate protein intake (1.6–2.2 g per kg of body weight daily) is essential to maximize the anabolic response to resistance training—particularly important for people with type 2 diabetes who often have impaired muscle protein synthesis. Distributing protein across 3–4 meals (20–40 g per meal) is more effective than consuming it in fewer, larger doses. Leucine-rich sources such as eggs, dairy, fish, and poultry are particularly effective at stimulating muscle protein synthesis.
Can resistance training specifically target visceral fat—the dangerous fat around organs?
Yes. The Wang et al. 2025 meta-analysis confirmed that resistance training produces favorable shifts in body composition, including reductions in visceral adipose tissue. This matters enormously because visceral fat is the primary driver of ectopic fat deposition in liver and muscle, which directly causes insulin resistance. Resistance training's reduction of visceral fat may be as important as its direct effects on glucose metabolism.
What role does sleep play in maximizing the metabolic benefits of exercise?
Sleep is when the cellular adaptations triggered by resistance training actually occur—muscle protein synthesis, mitochondrial biogenesis, and satellite cell activation all peak during deep sleep. Inadequate sleep (under 7 hours) independently causes insulin resistance and impairs the anabolic response to exercise. Treating sleep as part of the metabolic intervention—not an afterthought—significantly amplifies the benefits of your training program.
Clinical pearls
Pearl 1: Bypassing the Insulin Receptor (The AMPK Pathway)
Scientific Perspective: In the insulin-resistant state, the proximal insulin signaling cascade (IRS-1/PI3K/Akt) is profoundly impaired. However, mechanical muscular contraction activates AMPK (AMP-activated protein kinase) via an elevated intracellular $AMP: ATP$ ratio. AMPK acts as an alternate master switch, independently stimulating GLUT4 vesicle translocation to the sarcolemma. This clears circulating glucose via an insulin-independent pathway.
When you have type 2 diabetes, the front door your cells use to absorb blood sugar is jammed shut. But when you lift weights, your muscles open up a metabolic 'side door.' This side door doesn't need insulin to work—it pulls sugar straight out of your blood simply because the muscle is working."
Pearl 2: Rejuvenating the Hardware (Satellite Cell Activation)
Scientific Perspective: Chronic hyperglycemia and lipotoxicity induce a state of deep, dysfunctional quiescence in skeletal muscle satellite cells (stem cells). Resistance training under progressive overload induces mechanical tension and localized micro-trauma, forcing these dormant satellite cells to proliferate and fuse with existing fibers. The resulting regenerated myofibers exhibit qualitatively superior metabolic architecture, including higher insulin receptor density and enhanced mitochondrial coupling efficiency.
Over time, sitting too much and having high blood sugar actually damages your muscle tissue, making it sluggish and resistant to hormones. Lifting weights wakes up dormant stem cells inside your arms and legs. It literally forces your body to grow brand-new, high-quality muscle fibers that act like pristine, highly sensitive sponges for blood sugar."
Pearl 3: The 48-Hour Post-Exercise "Glucose Sink"
Scientific Perspective: The metabolic benefit of a single bout of resistance training extends far beyond the acute exercise window. Depletion of intracellular glycogen stores triggers a prolonged upregulation of glycogen synthase activity. To replenish these stores, the muscle tissue acts as a high-capacity, insulin-independent glucose sink, maintaining elevated glucose clearance rates for 24 to 48 hours post-exercise.
You aren't just lowering your blood sugar while you are exercising. A solid 45-minute weight session leaves your muscles hungry for fuel. To rebuild their energy reserves, your muscles will continuously suck sugar out of your bloodstream for up to two full days after your workout—even while you are resting or sleeping."
Pearl 4: Defusing the "Metabolic Fire" (Myokine Immunomodulation)
Scientific Perspective: Visceral adipose tissue in metabolic syndrome chronically secretes pro-inflammatory adipokines (e.g., $TNF-\alpha$, systemic $IL-6$). This drives low-grade chronic inflammation that disrupts insulin receptor substrate signaling. Conversely, contracting skeletal muscle functions as an endocrine organ, releasing acute, anti-inflammatory myokines (such as muscle-derived $IL-6$ and Meteorin-like). These molecules actively polarize macrophages from a pro-inflammatory M1 phenotype to an anti-inflammatory M2 phenotype, cooling systemic inflammation.
Type 2 diabetes is like a slow, quiet fire burning inside your body, driven by toxic belly fat that interferes with your hormones. When you exercise your muscles, they release protective chemical messengers that act like a built-in fire extinguisher. They travel through your body, cool down that inflammation, and help your organs heal."
Pearl 5: Reversing Sarcopenic Obesity (The True Target)
Scientific Perspective: Body weight is a blunt and frequently misleading metric in metabolic medicine. A patient can remain weight-stable while undergoing a catastrophic shift in body composition: losing metabolically active lean mass (sarcopenia) and gaining ectopic, visceral fat. Resistance training targets the root pathophysiology of type 2 diabetes by shifting the skeletal muscle-to-visceral fat ratio, expanding the body’s primary glucose disposal site while shrinking the tissue driving insulin resistance.
Ignore the bathroom scale for a moment. You can weigh the same but be radically healthier if you swap a few pounds of dangerous belly fat for a few pounds of active muscle. Muscle is your body's main engine for burning sugar; losing muscle as you age is a metabolic emergency. We need to focus on building your strength, not just shrinking your weight."
Pearl 6: Dosing Exercise as a Precision Medicine
Scientific Perspective: To optimize myokine secretion and GLUT4 expression, resistance training must be dosed with clinical intention. Compound, multi-joint movements (e.g., leg presses, rows) should be prioritized because recruiting a larger aggregate muscle mass creates a larger absolute glucose sink. The protocol must utilize progressive overload—gradually increasing mechanical tension—to continuously stimulate satellite cell differentiation and mitochondrial biogenesis.
We need to treat exercise exactly like a prescription medication, with a specific dose and schedule. Walking is great for your heart, but to fix your metabolism, we need to challenge your largest muscle groups—like your legs and back. By gradually lifting a little more over time, you keep forcing your body to upgrade its metabolic machinery."
Here is the practical pathway to begin your metabolic transformation,
Starting a resistance program to reverse insulin resistance isn't just about fitness—it's a targeted medical intervention. To safely and effectively unlock the metabolic power of your muscles, treat your routine as a prescription using this 6-step framework:
Step 1: Secure Medical Clearance: Schedule a quick chat with your primary care doctor to discuss your new exercise plan. Feel free to bring this research with you—most physicians are incredibly supportive of evidence-based lifestyle changes that reduce reliance on medication.
Step 2: Schedule 3 Non-Negotiable Sessions: Look at your calendar and block out three 45-minute time slots for this week. Treat these blocks as critical medical appointments that cannot be canceled or pushed aside.
Step 3: Master the "Compound" Basics: Focus your energy on multi-joint movements like squats, rows, chest presses, and deadlifts. These exercises recruit the largest amounts of muscle tissue at once, creating the biggest possible "sink" to absorb blood sugar. Always prioritize learning perfect form before you start adding heavy weights.
Step 4: Track Your Internal Data: Don't obsess over the bathroom scale. Instead, focus on the metrics that actually define your metabolic health: watch your morning fasting glucose trend downward, note your rising daily energy levels, and get your HbA1c retested at the 3-month mark.
Step 5: Fuel with Adequate Protein: To assist your body in repairing fibers and triggering satellite cell activation, aim to eat 1.6 to 2.2 grams of protein per kilogram of body weight daily. Spread this intake relatively evenly across your meals to maximize absorption.
Step 6: Commit Intently to a 12-Week Block: True cellular upgrades, mitochondrial renewal, and vascular improvements take time. Commit to standard consistency for 12 full weeks before you step back to analyze your results. While you will likely feel a massive boost in energy and focus within the first 14 days, the real biological magic happens over months, not weeks.
Medical Disclaimer
The information in this article, including the research findings, is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Before starting any new strength training exercise program, you must consult with a qualified healthcare professional, especially if you have existing health conditions (such as cardiovascular disease, uncontrolled hypertension, or advanced metabolic disease). Exercise carries inherent risks, and you assume full responsibility for your actions. This article does not establish a doctor-patient relationship.
Related Articles
Is a Functional Cure for Diabetes Within Reach? The Science of Beta-Cell Restoration | DR T S DIDWAL
Dietary Protein and Glycemic Control: Evidence from the Latest Diabetes Research | DR T S DIDWAL
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
What’s New in the 2025 Blood Pressure Guidelines? A Complete Scientific Breakdown | DR T S DIDWAL
Manage Diabetes Naturally: How Beta-Glucans Control Blood Sugar | DR T S DIDWAL
Exercise as Metabolic Medicine: Latest Research on Glucose and Heart Health| DR T S DIDWAL
References
Castillo, Í. M. P., Argilés, J. M., Rueda, R., et al. (2025). Skeletal muscle atrophy and dysfunction in obesity and type-2 diabetes mellitus: Myocellular mechanisms involved. Reviews in Endocrine and Metabolic Disorders, 26, 815–836. https://doi.org/10.1007/s11154-025-09954-9
Fukada, S.-I., & Nakamura, A. (2021). Exercise/resistance training and muscle stem cells. Endocrinology and Metabolism, 36(4), 737–744. https://doi.org/10.3803/EnM.2021.401
Iglesias, P. (2025). Muscle in endocrinology: From skeletal muscle hormone regulation to myokine secretion and its implications in endocrine-metabolic diseases. Journal of Clinical Medicine, 14(13), 4490. https://doi.org/10.3390/jcm14134490
Jin, J. B., Robinson, A., Soukup, T., Black, E., Abit, A., Hammer, S. M., Han, A., Lucas, E., Kim, Y., & Bae, J. (2025). Metabolic and molecular regulation in skeletal muscle dysfunction and regeneration. Frontiers in Cell and Developmental Biology, 13, Article 1651553. https://doi.org/10.3389/fcell.2025.1651553
Levate, G., & Stimson, R. H. (2025). Molecular signatures of skeletal muscle insulin resistance: Bringing personalised diabetes treatment a step closer. Signal Transduction and Targeted Therapy, 10, Article 320. https://doi.org/10.1038/s41392-025-02412-7
Masuda, S., & Matsuzaka, T. (2025). Insulin resistance and exercise-induced insulin sensitization in skeletal muscle: Insights from personalized phosphoproteomics. Journal of Diabetes Investigation, 16, Article e70113. https://doi.org/10.1111/jdi.70113
Wang, J., Fan, S., & Wang, J. (2025). Resistance training enhances metabolic and muscular health and reduces systemic inflammation in middle-aged and older adults with type 2 diabetes: A meta-analysis. Diabetes Research and Clinical Practice, 229, Article 112941. https://doi.org/10.1016/j.diabres.2025.112941
Wilkinson, M. S., Rollin, T. A., Kuriakose, M., Haggerty-Goede, R. A. L., Miller, D. M., & Dunham-Snary, K. J. (2025). Redox homeostasis in metabolic syndrome and type II diabetes: Role of skeletal muscle and impact of gold-standard treatments. International Journal of Molecular Sciences, 26(21), 10370. https://doi.org/10.3390/ijms262110370
Zierath, J. R., Brady, A. J., Macgregor, K. A., Ortiz de Zevallos, J., & Stocks, B. (2025). Unlocking the secrets of exercise: A pathway to enhanced insulin sensitivity and skeletal muscle health in type 2 diabetes. Journal of Sport and Health Science, 14, Article 100980. https://doi.org/10.1016/j.jshs.2024.100980