Aerobic vs Anaerobic Threshold: The Complete Science-Based Guide to Endurance, Fat Burning, and Performance
Learn the difference between aerobic and anaerobic thresholds, how they affect performance, fat metabolism, and how to train smarter using Zone 2 and lactate science.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/4/202613 min read
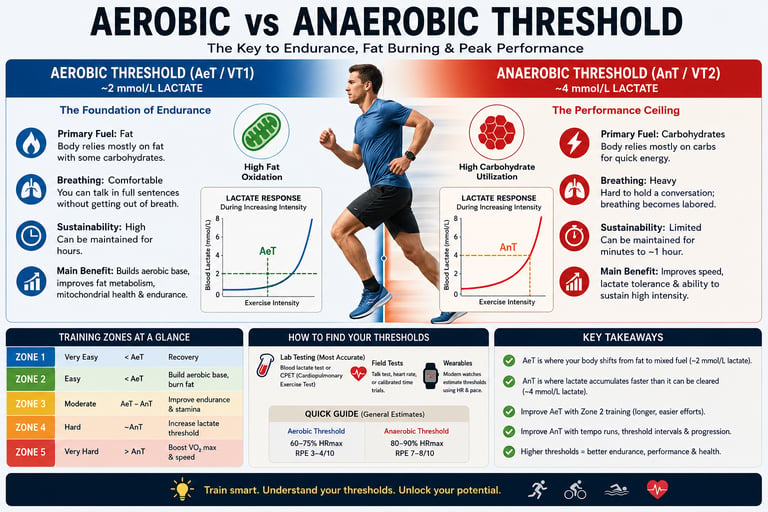
The aerobic threshold (AeT) is the exercise intensity where your body primarily burns fat and exercise feels comfortable enough to hold a conversation. The anaerobic threshold (AnT) is a higher intensity where lactate accumulates faster than it can be cleared, breathing becomes difficult, carbohydrates become the main fuel, and fatigue develops much more rapidly
Key Takeaways: Aerobic vs. Anaerobic Threshold
Your aerobic threshold is your body's fat-burning engine.
Exercising at or below your aerobic threshold (often called Zone 2) helps your body burn more fat, improves mitochondrial function (your cells' energy factories), and supports better blood sugar control and long-term heart health.Your anaerobic threshold determines how hard you can exercise before fatigue sets in.
As you approach this higher intensity, your muscles rely more on carbohydrates, breathing becomes difficult, and fatigue develops quickly. Raising this threshold helps you run, cycle, or walk faster for longer.Training below your aerobic threshold builds the foundation for fitness and longevity.
Regular Zone 2 exercise increases endurance, strengthens the heart, improves insulin sensitivity, and enhances your body's ability to use oxygen efficiently.Lactate is not harmful—it's an important fuel source.
Contrary to popular belief, lactate does not cause muscle soreness. Instead, it serves as a valuable energy source for muscles and the brain. Fatigue during intense exercise is more closely related to increasing acidity than to lactate itself.Your metabolic thresholds often predict real-world fitness better than VO₂ max alone.
While VO₂ max measures your maximum aerobic capacity, your aerobic and anaerobic thresholds show how much of that capacity you can actually sustain during daily activities, sports, or endurance events.Improving your aerobic threshold can benefit people with diabetes, obesity, and heart disease.
Conditions such as insulin resistance and type 2 diabetes often reduce your body's ability to burn fat efficiently. Consistent aerobic training can improve metabolic flexibility, glucose control, and cardiovascular health.Most workouts should be easy—not exhausting.
Research consistently shows that spending about 80% of your training at an easy, conversational pace and 20% at higher intensities produces better improvements in endurance, performance, and recovery than exercising hard every day.You don't need expensive laboratory tests to train effectively.
A simple talk test works surprisingly well: if you can comfortably speak in full sentences, you're likely training near your aerobic threshold. If you can only say a few words before needing a breath, you're close to your anaerobic threshold. This makes threshold-based training practical for almost everyone
Whether you're training for a marathon, trying to improve cardiovascular fitness, managing type 2 diabetes, or simply looking to exercise more effectively, understanding your aerobic threshold (AeT) and anaerobic threshold (AnT) may be one of the most powerful steps you can take.
Most people focus on calories burned, heart rate zones, or VO₂ max. Yet research increasingly shows that metabolic thresholds often provide a more practical measure of real-world performance, endurance, and even long-term health.
What Is the Aerobic Threshold?
The aerobic threshold (AeT) is the exercise intensity at which blood lactate first begins to rise above resting levels, typically around 2 mmol/L.
At intensities below this threshold:
Fat serves as the primary fuel source
Oxygen delivery adequately meets energy demands
Lactate production and clearance remain balanced
Exercise can be sustained for long periods
In practical terms, the aerobic threshold represents your body's highest sustainable "easy" pace.
Most people experience aerobic-threshold exercise as:
Comfortable breathing
Conversational pace
Steady energy levels
Minimal fatigue accumulation
This intensity generally corresponds to Zone 2 training, which has become increasingly popular because of its effects on mitochondrial health and metabolic flexibility.
What Is the Anaerobic Threshold?
The anaerobic threshold (AnT) represents a higher exercise intensity where lactate accumulates faster than it can be removed.
Although often associated with approximately 4 mmol/L lactate, the exact value varies considerably between individuals.
At intensities above this threshold:
Carbohydrate becomes the dominant fuel source
Lactate accumulation accelerates
Muscle acidity rises
Fatigue develops rapidly
Performance becomes time-limited
The anaerobic threshold is often called:
Lactate Threshold 2 (LT2)
Ventilatory Threshold 2 (VT2)
Onset of Blood Lactate Accumulation (OBLA)
Maximal Lactate Steady State (MLSS)
Think of the anaerobic threshold as your body's performance ceiling.
Aerobic vs Anaerobic Threshold: Key Differences
1. Blood Lactate Concentration
Aerobic Threshold (AeT): Typically sits around 2 mmol/L. This represents the first initial, subtle rise in blood lactate above a person's resting baseline.
Anaerobic Threshold (AnT): Generally approaches 4 mmol/L, though this value is highly variable between individuals. This marks the maximal lactate steady state where production still matches clearance.
2. Primary Fuel Substrate
Aerobic Threshold (AeT): Relies on a balanced combination of fats and carbohydrates. This intensity maximizes the rate of fat oxidation within the working muscles.
Anaerobic Threshold (AnT): Relies almost exclusively on carbohydrates. The body shifts heavily toward rapid glycolytic pathways to meet high energy demands.
3. Physical Sustainability
Aerobic Threshold (AeT): Highly sustainable. An individual can maintain this level of effort for multiple hours, limited primarily by hydration, glycogen stores, and mental fatigue.
Anaerobic Threshold (AnT): Strictly limited duration. This intensity can only be sustained from a few minutes up to approximately one hour before metabolic accumulation forces a slowdown.
4. Breathing Mechanics and Ventilation
Aerobic Threshold (AeT): Comfortable, steady, and rhythmic. The respiratory system can easily meet the body's demands without a noticeable spike in breathing rate.
Anaerobic Threshold (AnT): Heavy, rapid, and labored. Breathing increases sharply as the lungs work to buffer metabolic acidosis and clear accumulating carbon dioxide.
5. The Talk Test Field Surrogate
Aerobic Threshold (AeT): Full conversation is entirely possible. A person can speak in continuous, unbroken sentences without needing to pause mid-phrase for a breath.
Anaerobic Threshold (AnT): Communication is limited to short, broken phrases. An individual can generally manage only 3 to 4 words at a time before needing to inhale.
6. Target Training Zone
Aerobic Threshold (AeT): Corresponds to Zone 2. This is the foundational intensity used to build an extensive base of systemic cardiovascular endurance.
Anaerobic Threshold (AnT): Corresponds to Zone 4. This represents high-intensity, demanding work that targets systemic performance ceilings.
7. Core Physiological Adaptation
Aerobic Threshold (AeT): Drives mitochondrial biogenesis, enhances the efficiency of fat oxidation, and increases the structural density of capillary networks in slow-twitch muscle fibers.
Anaerobic Threshold (AnT): Improves systemic lactate tolerance, optimizes cellular buffering capacity, and trains the body to clear metabolic waste products under stress.
8. Primary Clinical Significance
Aerobic Threshold (AeT): Serves as a vital indicator of foundational metabolic health, insulin sensitivity, mitochondrial function, and overall metabolic flexibility.
Anaerobic Threshold (AnT): Acts as a critical predictor of peak functional capacity, athletic endurance potential, and cardiopulmonary prognosis in clinical populations.
The Physiology Behind Thresholds
Mitochondria: The Engine of Endurance
Mitochondria convert oxygen and nutrients into ATP, the body's energy currency.
Individuals with:
Higher mitochondrial density
Better capillary networks
Greater oxygen extraction
typically have higher aerobic thresholds and better endurance.
According to recent exercise physiology research, Zone 2 training stimulates mitochondrial biogenesis, helping muscles become more efficient at producing energy.
Lactate Is Not the Enemy
One of the biggest misconceptions in exercise science is that lactate causes fatigue.
Modern research demonstrates that lactate:
Serves as a valuable fuel source
Functions as a signaling molecule
Supports energy transfer between tissues
The body's ability to produce, transport, and recycle lactate largely determines where your thresholds occur.
Ventilatory Thresholds
Changes in breathing closely mirror metabolic thresholds.
Ventilatory Threshold 1 (VT1)
Closely corresponds to the aerobic threshold.
Signs include:
Slight increase in breathing rate
Comfortable conversation remains possible
Ventilatory Threshold 2 (VT2)
Closely corresponds to the anaerobic threshold.
Signs include:
Rapid breathing
Inability to speak comfortably
Significant effort perception
Why Thresholds Matter More Than VO₂ Max
VO₂ max measures the maximum amount of oxygen your body can utilize.
However, performance depends on how much of that capacity you can sustain.
For example:
Two athletes may have identical VO₂ max values
One can sustain 90% of VO₂ max
Another can sustain only 70%
The athlete with the higher threshold typically performs better.
This explains why threshold training is often more predictive of endurance performance than VO₂ max alone.
Thresholds and Metabolic Health
Thresholds are not just athletic metrics.
They are powerful indicators of health.
Research shows individuals with:
Obesity
Insulin resistance
Type 2 diabetes
Metabolic syndrome
often exhibit lower aerobic thresholds.
This reflects:
Reduced fat oxidation
Impaired mitochondrial function
Decreased metabolic flexibility
Improving aerobic threshold through structured Zone 2 training can significantly improve:
Insulin sensitivity
Blood glucose control
Body composition
Cardiovascular function
How Are Thresholds Measured?
Laboratory Testing
The gold-standard methods include:
Blood Lactate Testing
Small blood samples are taken during progressively harder exercise.
Benefits:
Highly accurate
Direct measurement
Limitations:
Requires specialized equipment
Cardiopulmonary Exercise Testing (CPET)
Measures:
Oxygen consumption
Carbon dioxide production
Ventilatory thresholds
CPET is widely used in sports medicine and cardiology.
Field Methods
The Talk Test
Aerobic Threshold:
You can comfortably hold a conversation.
Anaerobic Threshold:
Conversation becomes difficult.
Heart Rate Monitoring
Approximate ranges:
Aerobic threshold: 60–75% HRmax
Anaerobic threshold: 80–90% HRmax
Wearable Devices
Many modern smartwatches estimate thresholds using:
Heart rate variability
Running pace
Power output
How to Improve Your Aerobic Threshold
Zone 2 Training
Zone 2 remains the most effective method for increasing aerobic threshold.
Benefits include:
Increased mitochondrial density
Enhanced fat burning
Improved endurance
Better metabolic health
Sample Zone 2 Session
10-minute warm-up
45–90 minutes at conversational pace
5-minute cool-down
Weekly Recommendation
Most individuals benefit from:
3–5 Zone 2 sessions weekly
150–300 minutes total aerobic work
How to Improve Your Anaerobic Threshold
Improving the anaerobic threshold requires higher-intensity training.
Tempo Training
Example:
20–40 minutes at comfortably hard intensity
Benefits:
Improved lactate clearance
Increased sustainable speed
Threshold Intervals
Example:
4 × 10 minutes at threshold effort
2–3 minutes recovery
Benefits:
Increased tolerance to high workloads
Enhanced endurance performance
Training Zones Explained
1. Zone 1: Recovery
Intensity Profile: Very easy and light effort.
Primary Purpose: Promotes active recovery, stimulates gentle blood flow to flushing metabolic waste, and allows for psychological relaxation without adding any meaningful structural or physical stress to the body.
2. Zone 2: Easy Aerobic
Intensity Profile: Easy and conversational pace.
Primary Purpose: Explicitly targets raising the Aerobic Threshold. This zone stimulates mitochondrial biogenesis, enhances the efficiency of fat oxidation, and builds the baseline capillary network required for long-term endurance and metabolic flexibility.
3. Zone 3: Moderate
Intensity Profile: "Comfortably hard" or steady-state tempo effort.
Primary Purpose: Has limited direct use in polarized training models. While it accumulates substantial volume, it creates high autonomic nervous system stress and glycogen depletion without providing the maximal metabolic adaptations of Zone 2 or the high-intensity performance benefits of Zone 4.
4. Zone 4: Threshold
Intensity Profile: Hard, sustainable, and controlled discomfort.
Primary Purpose: Directly targets raising the Anaerobic Threshold. Training at this exact boundary teaches the body to optimize its lactate clearance kinetics, improves cellular buffering capacity, and extends the duration a person can sustain high-intensity efforts before hitting exhaustion.
5. Zone 5: Very Hard
Intensity Profile: Max or near-maximal short-burst efforts.
Primary Purpose: Specifically focused on VO2max development. This high-intensity stimulus challenges central cardiac output, maximizes stroke volume, and forces neuromuscular adaptations that expand the raw maximum capacity of the entire cardiopulmonary system.
Evidence Summary
1. Clinical Risk Prediction & Heart Failure
Study: Ryuzaki et al. (2023)
Core Finding: The anaerobic threshold (AT) is a powerful predictor of clinical outcomes and mortality risk in heart failure patients.
The Details: During cardiopulmonary exercise testing (CPET), the anaerobic threshold represents the point where the cardiorespiratory system can no longer deliver enough oxygen to the muscles to sustain purely aerobic metabolism, causing lactic acid to begin accumulating. In heart failure patients, a low AT indicates advanced cardiac dysfunction, poor skeletal muscle perfusion, and altered fatty acid metabolism (often linked to underlying carnitine deficiencies) (Ito et al., 2023). Because AT measures functional capacity under stress rather than just a resting state, it serves as a highly accurate baseline for predicting hospitalization and overall survival rates.
2. High-Intensity Interval Training vs. Ventilatory Thresholds
Study: Drwal & Maciejczyk (2025)
Core Finding: Aerobic Interval Training (AIT) significantly improves the second ventilatory threshold (VT2) and overall aerobic power.
The Details: In comparative trials tracking aerobic capacity, 6 weeks of Aerobic Interval Training (AIT) was proven to be uniquely effective at increasing oxygen uptake specifically at the VT2 level (Drwal, 2025).
What is VT2? It is the point of uncompensated metabolic acidosis—the intensity at which hyperventilation occurs because the body can no longer buffer accumulating blood lactate.
The Contrast: While higher-intensity Sprint Interval Training (SIT) or heavy strength training can successfully boost maximal oxygen uptake (VO2max) and raw peak power, they fail to move the VT2 milestone. AIT specifically adapts the body's cardiovascular system and blood flow mechanics to delay hyperventilation, meaning an individual can sustain submaximal, high-intensity efforts for a longer duration before hitting physical exhaustion.
3. The Irreplaceability of Base Training Volume
Study: Ambaum & Hoppe (2025)
Core Finding: High aerobic volume remains completely non-negotiable and essential for long-term endurance development.
The Details: Despite the popularity of short, time-efficient interval methods, systematic evaluations of energy pathways confirm that structural endurance cannot be built on high intensity alone. Large volumes of lower-intensity, steady-state training induce critical micro-adaptations that intervals cannot replicate as effectively—such as increased mitochondrial density, capillary network expansion in skeletal muscle, and improved stroke volume of the heart (Ambaum, 2025). Furthermore, having a deeply developed aerobic base drastically accelerates post-exercise recovery by speeding up the replenishment of cellular energy stores (phosphocreatine resynthesis) between high-intensity bursts.
4. Physiological Adaptability of Thresholds
Study: Armstrong & Welsman (2020)
Core Finding: Metabolic and physiological thresholds are highly plastic and adapt significantly when exposed to structured training stimuli.
The Details: This research counters the idea that an individual's aerobic and anaerobic thresholds are hardcoded biological limits. Somatic and cardiovascular systems exhibit high trainability across different age groups and maturity levels (Beyer et al., 2020). When exposed to consistent progressive overload, the point at which an individual begins to accumulate lactate or experience rapid breathing shifts upward toward a higher percentage of their total VO2max. This means that a trained athlete can work at an energy output that would trigger immediate, uncompensated fatigue in an untrained individual.
5. Systemic Cardiovascular Differentiation
Study: Patel et al. (2017)
Core Finding: Aerobic and anaerobic exercises generate entirely distinct structural and functional adaptations within the cardiovascular system.
The Details: The heart and blood vessels respond to the unique mechanical stress imposed by different types of training:
Aerobic Exercise (Volume Overload): Activities like distance running or cycling require sustained cardiac output. This triggers eccentric left ventricular hypertrophy—meaning the heart chambers actually stretch and expand in volume to pump more blood per beat (improving stroke volume), while blood vessels become more compliant and expand their capillary networks.
Anaerobic Exercise (Pressure Overload): Short-burst, high-resistance activities (like heavy lifting or sprinting) subject the heart to intense, acute pressure spikes. This triggers concentric left ventricular hypertrophy, where the muscular walls of the heart thicken to force blood out against high vascular resistance, altering myocardial stiffness and arterial characteristics in a completely different manner.
Common Myths and Mistakes
Myth #1: Anaerobic Means No Oxygen
False.
Your body continues using oxygen even during intense exercise.
Myth #2: Lactate Causes Muscle Soreness
False.
Delayed-onset muscle soreness is primarily related to microscopic muscle damage and inflammation.
Myth #3: The Anaerobic Threshold Is Always 4 mmol/L
False.
Threshold values vary substantially among individuals.
Myth #4: Harder Training Is Always Better
False.
Most endurance adaptations occur through large volumes of lower-intensity training.
Myth #5: Zone 2 Is Too Easy to Be Effective
False.
Zone 2 stimulates many of the mitochondrial adaptations associated with improved endurance and metabolic health.
Frequently Asked Questions
Q1. What is the difference between the aerobic and anaerobic threshold?
The aerobic threshold (AeT) is the point at which lactate first rises above resting baseline (~2 mmol/L), marking a shift from predominantly fat-based to mixed fuel utilization. The anaerobic threshold (AnT) is the higher-intensity inflection point (~4 mmol/L, variable) beyond which lactate accumulates faster than it can be cleared, and exercise becomes unsustainable within minutes. Put simply: AeT = you can go all day; AnT = you have minutes to hours at most.
Q2. How do I know if I'm training at the right threshold?
The most accessible field test for the AeT is the talk test: if you can speak in complete, comfortable sentences, you're likely below or at AeT. For the AnT, "comfortably hard" — where you can manage a few words but not a conversation — is a reasonable proxy. For precision, laboratory lactate profiling or CPET is the gold standard.
Q3. Can I improve both thresholds simultaneously?
Yes — but different training stimuli drive each adaptation. Zone 2 training (long, slow, aerobic work) primarily improves the AeT, while threshold intervals and tempo running raise the AnT. Most well-designed programs include both within a periodized framework, prioritizing AeT base-building before adding AnT-specific work.
Q4. Is the 'anaerobic threshold' the same as 'lactic acid threshold'?
Nearly — but with an important clarification. What is commonly called the "lactic acid threshold" more accurately refers to the blood lactate threshold (lactate is the measurable form in the body). The terms LT1, LT2, OBLA, and anaerobic threshold are related but not always identical — context and testing methodology matter.
Q5. Why do elite athletes have higher thresholds than recreational athletes?
Elite endurance athletes typically have both a higher AeT (more efficient fat metabolism and greater mitochondrial density) and a higher AnT relative to their VO₂ max (often 85–90% vs. 60–70% in recreational athletes). This is the product of years of high-volume aerobic training and targeted threshold work — not genetics alone.
Q6. Are thresholds important for non-athletes or patients?
Absolutely — and arguably even more so. The anaerobic threshold identified during CPET carries independent prognostic value for cardiovascular mortality and surgical risk. For patients with heart failure, COPD, cancer, or metabolic syndrome, threshold-guided exercise prescription is both safer and more effective than generic recommendations.
Q7. How often should I get my thresholds tested?
For competitive athletes: every 8–12 weeks (corresponding to training blocks). For recreational athletes: once or twice per year. For patients in cardiac rehab or with chronic disease: frequency should be determined by a physician or exercise physiologist based on clinical status and program goals.
Author’s Note
This article was written with a dual purpose: to bridge the gap between exercise physiology and clinical medicine, and to make complex metabolic concepts accessible without compromising scientific accuracy. As clinicians, we are often trained to view exercise through broad guidelines—“moderate intensity,” “150 minutes per week”—yet physiology is far more nuanced. Aerobic and anaerobic thresholds offer a precision-based framework that aligns far more closely with how the human body actually responds to stress, adapts to training, and progresses toward health or disease.
In both athletic and patient populations, I have consistently observed that outcomes improve when training is guided by physiology rather than arbitrary zones or generalized prescriptions. A patient with insulin resistance struggling with fatigue, or an athlete plateauing despite high training volume, often shares a common issue: a mismatch between training intensity and underlying metabolic capacity. Understanding thresholds allows us to correct that mismatch.
At the same time, it is important to acknowledge that these concepts—while grounded in robust evidence—are not absolute. Threshold values vary between individuals, testing methods differ, and real-world application requires clinical judgment and contextual interpretation. This article is not intended to replace individualized assessment, but rather to provide a scientifically grounded lens through which both clinicians and readers can better understand performance, fatigue, and metabolic health.
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
Related Articles
Exercise Is Metabolic Medicine: The Hidden Benefits Most People Never Learn About | DR T S DIDWAL
Lactate Threshold Explained: Boost Stamina, Burn Fat, and Train Smarter
HIIT for Athletes: Boost VO₂ Max, Lactate Threshold, and Peak Performance – Science-Based Guide
HIIT vs Moderate Cardio: Which Improves Cardiovascular Fitness Faster?
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanis
References
Armstrong, N., & Welsman, J. (2020). The development of aerobic and anaerobic fitness with reference to youth athletes. Journal of Science in Sport and Exercise, 2, 275–286. https://doi.org/10.1007/s42978-020-00070-5
Aerobic VS anaerobic exercise on body composition and hormonal adaptations in athletes and non-athletes: A randomized controlled trial. (2025). Journal of Coaching and Sports Science. https://doi.org/10.58524/JCSS.V4I1.553
Ambaum, C., & Hoppe, M. W. (2025). Evaluation of methods to quantify aerobic-anaerobic energy contributions during sports and exercise — a systematic review and best-evidence synthesis. Frontiers in Sports and Active Living, 7, 1650741. https://doi.org/10.3389/fspor.2025.1650741
Chamari, K., & Padulo, J. (2015). 'Aerobic' and 'anaerobic' terms used in exercise physiology: A critical terminology reflection. Sports Medicine – Open, 1(1), 9. https://doi.org/10.1186/s40798-015-0012-1
Drwal, A., & Maciejczyk, M. (2025). Strength training vs. aerobic interval training: Effects on anaerobic capacity, aerobic power and second ventilatory threshold in men. Applied Sciences, 15(14), 7953. https://doi.org/10.3390/app15147953
Patel, H., Alkhawam, H., Madanieh, R., Shah, N., Kosmas, C. E., & Vittorio, T. J. (2017). Aerobic vs anaerobic exercise training effects on the cardiovascular system. World Journal of Cardiology, 9(2), 134–138. https://doi.org/10.4330/wjc.v9.i2.134
Ryuzaki, T., Shiraishi, Y., Miura, K., Ikura, H., Seki, Y., Azuma, K., Sato, K., Fukuda, K., & Katsumata, Y. (2023). Real-time estimation of anaerobic threshold during exercise using electrocardiogram in heart failure patients. Journal of Clinical Medicine, 12(16), 5225. https://doi.org/10.3390/jcm12165225