HIIT vs Moderate Cardio: Which Improves Cardiovascular Fitness Faster?
Which is better for your heart—HIIT or steady cardio? This science-backed guide compares fitness, fat loss, and cardiovascular outcomes across populations.
EXERCISEHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/1/202617 min read
HIIT improves cardiovascular fitness (VO₂ max) faster than moderate cardio, making it the most time-efficient option for heart health.
Both HIIT and moderate exercise reduce heart disease risk, but HIIT may deliver stronger benefits for vascular function and arterial stiffness.
Moderate-intensity exercise is easier to sustain long-term, especially for beginners, older adults, and those with chronic conditions.
HIIT is safe and effective even in heart patients when performed under medical supervision and proper guidance.
The best approach is a combination of both—use moderate cardio as a foundation and HIIT to accelerate cardiovascular gains.
“The Dual-Intensity Cardiovascular Model (DICM)”
MICT = Base conditioning
HIIT = Adaptive stimulus
Clinician’s Perspective: Translating HIIT vs. MICT Into Cardiovascular Practice
Cardiorespiratory fitness is the primary therapeutic target.
Improvements in VO₂ max remain one of the strongest predictors of reduced cardiovascular and all-cause mortality. Across multiple randomized trials, HIIT consistently produces greater gains in VO₂ max compared to MICT, making it a potent tool for risk modification in both primary and secondary prevention.Time efficiency is not a trivial advantage—it is a clinical lever.
Lack of time is the most commonly cited barrier to exercise adherence. HIIT directly addresses this barrier, delivering comparable or superior cardiometabolic benefits in 40–60% less time (Guo et al., 2023). For busy or non-adherent patients, this can determine whether exercise is prescribed and followed.HIIT is no longer contraindicated in stable cardiac disease.
Contemporary evidence demonstrates that, under supervision, HIIT is safe and effective in patients with coronary artery disease, with superior improvements in functional capacity compared to MICT (Gonçalves et al., 2025). This represents a paradigm shift in cardiac rehabilitation.Vascular biology responds powerfully to intensity.
HIIT induces greater improvements in endothelial function, arterial compliance, and autonomic balance—key upstream drivers of atherosclerosis and hypertension (Luo et al., 2024; K B et al., 2024). These effects may translate into earlier reversal of subclinical disease.However, adherence remains the Achilles’ heel.
While physiologically superior, HIIT may not be sustainable for all patients. MICT retains a critical role due to its simplicity, tolerability, and higher long-term adherence rates—particularly in older adults and those with multimorbidity.The optimal prescription is not binary—it is integrative.
The most effective strategy is a hybrid model, combining MICT as a foundational aerobic base with periodic HIIT sessions to maximise cardiovascular adaptation.Exercise prescription must be individualised, not ideological.
Patient phenotype, comorbidities, baseline fitness, and preferences should guide intensity selection—not trends.
Bottom line: The future of preventive cardiology is not choosing between HIIT and MICT—but prescribing the right intensity, to the right patient, at the right time.
The Intensity Question That Could Redefine Cardiovascular Prevention
What if the difference between preventing heart disease and merely managing it came down not to whether you exercise, but how hard you exercise?
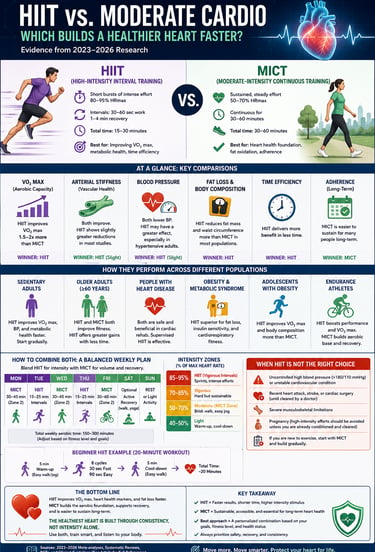
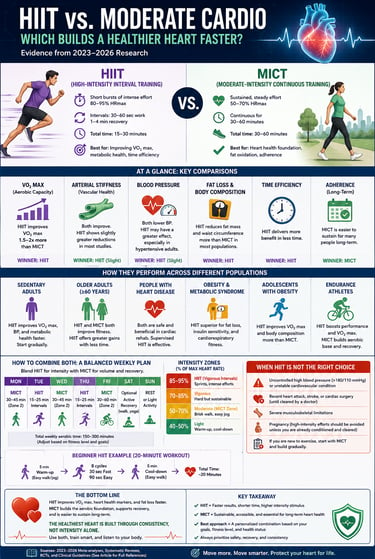
For decades, moderate-intensity continuous training (MICT) — sustained aerobic activity at 50–70% of maximum heart rate — has been the foundation of cardiovascular prevention guidelines. Yet emerging research suggests high-intensity interval training (HIIT) — short bursts of vigorous effort (80–95% max heart rate) alternated with recovery — may deliver superior cardiovascular adaptations in a fraction of the time.
At the heart of this debate is cardiorespiratory fitness, particularly VO₂ max (or VO₂ peak), one of the strongest independent predictors of cardiovascular and all-cause mortality. Multiple randomized trials and meta-analyses show HIIT consistently produces greater gains in VO₂ max compared with MICT across diverse groups: sedentary adults, individuals with obesity, and even patients with stable coronary artery disease (Gonçalves et al., 2025; Su et al., 2024). HIIT also appears to offer stronger benefits for vascular biology, including improved endothelial function, reduced arterial stiffness, and better autonomic balance — key mechanisms in atherosclerosis and heart failure (Luo et al., 2024; K B et al., 2024).
However, intensity has trade-offs. Questions remain about long-term adherence, safety in high-risk patients, and whether HIIT’s physiological advantages translate into better real-world outcomes.
This evidence-based guide examines the comparative effects of HIIT versus MICT on fitness, vascular health, fat loss, and clinical populations — separating science from hype. The goal is not to declare a winner, but to help clinicians and patients choose the right intensity for the right person at the right time.
What Exactly Are HIIT and MICT?
Before comparing them, it helps to understand what each training style actually involves.
High-Intensity Interval Training (HIIT) involves alternating short periods of vigorous effort (typically 80–95% of maximum heart rate) with recovery intervals. A session might look like 30–60 seconds of near-maximal effort, followed by 1–2 minutes of rest or light activity, repeated 6–10 times. Total workout time: often just 20–30 minutes.
Moderate-Intensity Continuous Training (MICT) involves sustained aerobic activity at 50–70% of maximum heart rate for a longer duration — typically 30–60 minutes. Think: a 45-minute brisk walk, a steady swim, or a light jog.
Both are aerobic. Both are proven to be healthy. The key differences lie in intensity, duration, and the specific physiological adaptations they trigger — and that is where things get scientifically interesting.
HIIT vs. MICT for Heart Disease Patients: Long-Term Evidence
For people already living with coronary artery disease (CAD), exercise prescription must be both effective and safe. A landmark randomized controlled trial by Gonçalves et al. (2025) enrolled CAD patients and assigned them to either HIIT or MICT protocols, tracking outcomes at 6 and 12 months.
The results were compelling: both training modalities produced significant improvements in cardiorespiratory fitness, quality of life, and cardiovascular risk markers. However, HIIT consistently showed greater gains in peak oxygen uptake (VO₂ peak) — a key measure of heart-lung efficiency — at both the 6-month and 12-month checkpoints. Importantly, HIIT was found to be safe and well-tolerated in this medically supervised context (Gonçalves et al., 2025).
Practical takeaway for heart patients: HIIT is not just for the fit and young. With appropriate medical supervision and individualised programming, it can be a powerful tool even in cardiac rehabilitation settings. However, never begin a HIIT programme without clearance from your cardiologist.
Arterial Stiffness: A Hidden Cardiovascular Threat
Most people have never heard of arterial stiffness — but your doctor likely pays close attention to it. When arteries lose their elasticity, the heart must work harder to pump blood, raising risk for hypertension, stroke, and heart failure.
A meta-analysis by Luo et al. (2024), published in Frontiers in Cardiovascular Medicine, synthesised evidence from multiple studies on how HIIT affects arterial stiffness in individuals at cardiovascular risk. The analysis found that HIIT significantly reduced arterial stiffness compared to sedentary controls, with effects broadly comparable to — and in some protocols exceeding — MICT.
The mechanism? HIIT's repeated cycles of high cardiac output stress followed by rapid recovery appear to train the vascular walls to become more elastic and responsive over time (Luo et al., 2024).
Why this matters: Reducing arterial stiffness is one of the most underappreciated benefits of exercise. Both HIIT and MICT help — but for people at cardiovascular risk, HIIT may offer a more time-efficient route to meaningful vascular benefit.
What About Sedentary Adults? HIIT vs. MICT Head-to-Head
Most of us are not athletes. Many of us spend large parts of the day sitting. So what happens when sedentary adults start either HIIT or MICT from scratch?
A 2025 comparative study by Aniya et al., published in the Journal of Heart Valve Disease, examined cardiovascular function in sedentary adults randomised to HIIT or MICT programmes. Both groups improved heart rate variability, resting heart rate, blood pressure, and exercise capacity. However, the HIIT group showed greater improvements in cardiac output and stroke volume — two fundamental measures of how efficiently the heart pumps blood (Aniya et al., 2025).
Notably, even short HIIT sessions — as brief as 20 minutes — produced significant cardiovascular improvements in previously sedentary participants. This challenges the common excuse that "I don't have time to exercise."
Practical insight: If you are sedentary and starting from scratch, both approaches work. But if your schedule is tight, a well-designed HIIT programme may give you more cardiovascular bang for your workout buck.
Obesity, Adolescents, and Heart Health: A Special Case
The global rise in childhood and adolescent obesity is one of the most pressing public health issues of our time. How does exercise intensity affect cardiovascular risk in young people with obesity?
Su et al. (2024), in a randomised controlled trial published in the European Journal of Sport Science, studied adolescent boys with obesity assigned to HIIT or MICT protocols. The results were revealing: HIIT produced greater improvements in cardiopulmonary function, including VO₂ peak and ventilatory threshold, compared to MICT. Additionally, HIIT more effectively improved cardiac autonomic function — which governs the heart's ability to respond to physical and emotional stress — and vascular function markers (Su et al., 2024).
These findings suggest that HIIT may be particularly powerful for reversing the cardiovascular damage associated with adolescent obesity — potentially offering a more effective intervention window before these risks solidify into adult disease.
For parents and healthcare providers: Age-appropriate HIIT programmes for teens with obesity are not only safe — they may be more effective than standard aerobic exercise at reducing long-term cardiovascular risk.
Fat Loss and Cardiorespiratory Fitness: The Metabolism Story
One of the most popular reasons people choose HIIT is fat loss. But is the evidence solid?
A systematic review and meta-analysis by Guo et al. (2023), published in the International Journal of Environmental Research and Public Health, analysed the effects of HIIT versus MICT on fat loss and cardiorespiratory fitness in young and middle-aged adults across multiple randomised controlled trials.
The findings: HIIT and MICT produced similar overall fat loss, but HIIT demonstrated a significant edge in improving cardiorespiratory fitness (measured as VO₂ max) and in considerably less total exercise time (Guo et al., 2023). HIIT also appeared to preserve or build lean muscle mass more effectively than steady-state cardio.
The mechanism behind HIIT's metabolic power involves the "afterburn effect" (excess post-exercise oxygen consumption, or EPOC) — your body continues burning calories at an elevated rate for hours after a HIIT session, something MICT does not trigger to the same degree.
Bottom line: For people looking to lose fat while improving heart health simultaneously, HIIT is a strong dual-purpose tool. That said, adherence matters — and for many people, MICT is simply more enjoyable and easier to sustain.
Vascular Function in Overweight and Obese Adults
Beyond the heart muscle itself, blood vessel health — specifically endothelial function (the health of the inner lining of blood vessels) — is a cornerstone of cardiovascular wellness.
A comprehensive systematic review by K B et al. (2024), published in the International Journal of Obesity, examined the effects of HIIT versus MICT on vascular function specifically in individuals with overweight and obesity. The review concluded that both training types significantly improved endothelial function and reduced markers of vascular inflammation. However, HIIT tended to produce more pronounced improvements in flow-mediated dilation — a gold-standard measure of blood vessel flexibility and health (K B et al., 2024).
This is clinically significant: poor endothelial function is an early, reversible sign of atherosclerosis (artery hardening). Improving it through exercise can delay or even prevent the progression to more serious cardiovascular disease.
Key message: If you are overweight or obese and concerned about heart disease risk, both HIIT and MICT improve your blood vessel health — but HIIT may push the needle further, faster.
What About Competitive and Endurance Athletes?
HIIT versus MICT is not just a question for clinical populations. A 2026 systematic review by Marmondi et al., published in the International Journal of Sports Science & Coaching, examined physiological, biochemical, physical, and biomechanical adaptations in endurance runners comparing HIIT and MICT.
The review found that HIIT outperformed MICT in improving VO₂ max, running economy, and lactate threshold in trained athletes — key indicators of competitive endurance performance. Importantly, biomechanical adaptations (stride efficiency, ground contact time) were also more robust following HIIT protocols (Marmondi et al., 2026).
However, the authors cautioned against exclusive reliance on HIIT for endurance athletes, noting that the combination of both HIIT and MICT — often called polarised or pyramidal training — may offer the best long-term outcomes for serious runners.
Side-by-Side Comparison: HIIT vs. MICT at a Glance
1. Cardiorespiratory Fitness (VO₂ Max)
HIIT: Superior. It is more effective at increasing the heart’s "pumping capacity" and the muscles' ability to use oxygen. It acts as a "turbocharger" for your aerobic engine.
MICT: Effective. It builds a solid aerobic base and improves endurance, but typically results in smaller gains in peak oxygen uptake compared to HIIT.
2. Arterial Stiffness & Vascular Health
HIIT: Strong Evidence. The rapid "on-off" nature of intervals creates a pulsatile blood flow that physically stretches the artery walls, making them more elastic and reducing stiffness.
MICT: Moderate Evidence. It maintains vessel health and promotes blood flow, but lacks the high-intensity "shear stress" required for rapid arterial remodeling.
3. Fat Loss & Metabolism
HIIT: Time-Efficient. While it burns fewer calories during the short workout, it triggers a significant "afterburn effect" (EPOC), keeping the metabolism elevated for hours after.
MICT: High Volume. It burns more calories during the actual session because the duration is longer, making it excellent for steady, daily energy expenditure.
4. Cardiac Autonomic Function (HRV)
HIIT: Greater Impact. It specifically trains the "vagus nerve," which helps the heart switch from a high-stress state to a relaxed state quickly. This is especially effective in teens and young adults.
MICT: Stabilizing. It helps lower the resting heart rate and provides a consistent, calming effect on the nervous system.
5. Practicality & Feasibility
HIIT: High Efficiency. Ideal for busy schedules, as most benefits are achieved in 20 minutes or less. However, it requires a higher "mental effort" to push through the intensity.
MICT: High Accessibility. Easy to start with no special equipment (e.g., walking). It is generally perceived as more "pleasant," which often leads to better long-term habit formation.
6. Safety & Clinical Use
HIIT: Safe with Supervision. Research shows it is safe even for heart disease (CAD) patients, but because it spikes blood pressure and heart rate, it requires medical clearance and structured programming.
MICT: The Gold Standard. This is the safest starting point for those with uncontrolled hypertension, joint issues, or severe deconditioning.
Practical Applications: How to Use This Research in Real Life
1. Start Where You Are
If you are completely new to exercise, start with MICT. A 30-minute brisk walk 5 days a week is still one of the most evidence-supported interventions in all of medicine. Build your aerobic base before introducing intervals.
2. Introduce HIIT Gradually
After 4–6 weeks of consistent moderate exercise, you can begin incorporating 1–2 HIIT sessions per week. A simple beginner HIIT protocol: 20 seconds of brisk effort (fast walk, light jog, cycling) followed by 40 seconds of easy movement, repeated 8–10 times.
3. Heart Patients: Supervised HIIT is Safe
If you have been diagnosed with CAD or other cardiovascular conditions, speak with your cardiologist or cardiac rehabilitation specialist. The evidence from Gonçalves et al. (2025) shows HIIT can be safely and effectively incorporated into cardiac rehab — but individual medical screening is non-negotiable.
4. For Weight Management, Combine Both
Use MICT for your longer weekend sessions (45–60 minutes of sustained cardio) and HIIT for weekday sessions when time is tight. This combination maximises both fat oxidation and cardiovascular adaptation.
5. Adolescents with Obesity: Make It Fun
For teens, the packaging matters. HIIT can be delivered through sports drills, circuit training, or even dance workouts — the physiological benefits are the same whether it feels like "training" or play (Su et al., 2024).
6. Track Your Resting Heart Rate
A simple, free way to monitor your cardiovascular progress at home is your resting heart rate. As your fitness improves through either HIIT or MICT, your resting heart rate should drop over weeks and months. Normal range: 60–100 bpm; trained athletes often see 40–60 bpm.
7. Respect Recovery
HIIT taxes the nervous system significantly. Never perform HIIT on consecutive days. Alternate with MICT, yoga, or rest days to allow full physiological recovery.
When NOT to Choose HIIT
HIIT is powerful — but it is not for everyone, at every time:
Uncontrolled hypertension: High-intensity effort can spike blood pressure dangerously. Get BP under control first.
Recent cardiac event: MICT with medical supervision is the starting point after a heart attack or cardiac procedure.
Joint pain or orthopaedic issues: HIIT's high-impact nature may aggravate knees, hips, or ankles. Low-impact MICT (swimming, cycling) is more appropriate.
Severe deconditioning: If you are extremely unfit, start with MICT exclusively until your baseline fitness improves.
Pregnancy: Moderate exercise is generally recommended; intense intervals should only be undertaken with explicit obstetric guidance.
The Verdict: Which Is Better?
The honest answer is: it depends on your goal, your current fitness level, and your health status.
For maximum cardiovascular improvement in the shortest time, HIIT wins on most metrics — from VO₂ max and arterial stiffness to vascular function and cardiac autonomic tone.
For accessibility, safety, long-term adherence, and general health maintenance, MICT remains the most broadly applicable and evidence-backed recommendation — especially for beginners and those with significant health challenges.
The best exercise programme is almost certainly one that combines both — using MICT as your foundation and HIIT as your accelerator.
And above all: the exercise you will actually do consistently is better than the perfect programme you abandon after two weeks.
Frequently Asked Questions (FAQs)
How many HIIT sessions per week are best for heart health?
Most evidence supports 2–3 HIIT sessions per week, with at least 48 hours of recovery between them to allow adaptation and prevent overtraining. Balance these with 2–3 days of MICT for a well-rounded program (Gonçalves et al., 2025; Guo et al., 2023).
Is HIIT safe for patients with coronary artery disease (CAD)?
Yes — when performed under medical supervision in cardiac rehabilitation. Trials such as Gonçalves et al. (2025) show HIIT is safe and often produces greater improvements in cardiorespiratory fitness than MICT. Always obtain cardiologist clearance first.
Does HIIT reduce arterial stiffness more effectively than moderate exercise?
HIIT can be more effective. Its pulsatile blood flow creates greater shear stress on artery walls, improving elasticity and reducing stiffness — a key factor in lowering hypertension and stroke risk (Luo et al., 2024).
Is HIIT better than walking (MICT) for fat loss?
Both produce similar overall fat loss, but HIIT is more time-efficient thanks to the “afterburn” effect (elevated calorie burn post-workout). HIIT also preserves lean muscle better and improves VO₂ max more in less time (Guo et al., 2023).
Which is better for obese adolescents — HIIT or MICT?
HIIT often shows superior results for improving VO₂ peak, vascular function, and cardiac autonomic control in teens with obesity, while remaining engaging through sports-like formats (Su et al., 2024). Age-appropriate, supervised programs work best.
Clinical pearls
1. The "Safety Paradox" of Intensity
Scientific Perspective: High-Intensity Interval Training (HIIT) increases the sheer stress on the vascular endothelium, which, despite appearing risky, actually triggers superior adaptive remodeling of the arterial walls compared to steady-state exercise.
Pushing your heart for short bursts feels intense, but it’s actually "training" your blood vessels to be more flexible. Think of it like stretching a rubber band so it doesn't get brittle; short bursts of hard work keep your pipes from getting stiff.
2. VO₂ Peak: The Ultimate Longevity Metric
Scientific Perspective: VO₂ peak is one of the strongest independent predictors of all-cause mortality. Clinical data (Gonçalves et al., 2025) suggests HIIT is more effective at increasing peak oxygen uptake than MICT, even in patients with existing coronary artery disease.
Your VO₂ peak is basically your body’s "engine size." A bigger engine handles hills, stairs, and stress more easily. While walking is great, HIIT is like giving your heart an engine upgrade, helping you live longer and feel less tired during daily tasks.
3. The Endothelial "Washout" Effect
Scientific Perspective: HIIT enhances flow-mediated dilation (FMD)—a measure of nitric oxide bioavailability. The rapid fluctuations in heart rate during interval training create a cyclic "pulsatile" blood flow that cleanses the inner lining of the arteries more effectively than constant flow.
Imagine a garden hose. A steady stream of water (MICT) is good, but pulsing the water on and off (HIIT) creates more pressure to clear out debris. HIIT helps "scrub" the inside of your arteries to keep them clear and healthy.
4. Reversing the "Sedentary Heart"
Scientific Perspective: Chronic physical inactivity leads to cardiac atrophy and increased left ventricular stiffness. Research (Aniya et al., 2025) shows that HIIT can significantly increase stroke volume—the amount of blood pumped per beat—reversing the structural stiffening caused by years of sitting.
Sitting all day makes your heart a bit smaller and "stiffer." You don't need hours of cardio to fix this. Just 20 minutes of intervals can teach your heart how to pump more blood with every single beat, making it a much more efficient pump.
5. Autonomic Resilience and HRV
Scientific Perspective: HIIT provides a unique stimulus to the autonomic nervous system, increasing parasympathetic tone (the "rest and digest" system). This is reflected in improved Heart Rate Variability (HRV), which reduces the risk of sudden cardiac events.
Your heart needs to be able to "react" to stress and then "calm down" quickly. HIIT trains your nervous system to flip the switch from high-stress to total relaxation. This makes you more resilient to both physical exercise and emotional stress.
Call to Action: Take the First Step Today
Your heart beats 100,000 times every day — it deserves your attention.
Whether you are just starting your fitness journey, managing a chronic condition, or looking to optimise your training, the evidence is clear: structured exercise — whether HIIT or MICT — is one of the most powerful medicines available to you, with no prescription required.
Here is your challenge:
Ready to put the science into practice? Follow this simple blueprint to jumpstart your cardiovascular health this week:
The Commitment: Complete 3 exercise sessions. Whether it’s a walk, a bike ride, or a swim, aim for just 20–30 minutes per session.
The HIIT Trial: Replace one of those sessions with this 12-minute "Power Interval" protocol:
30 Seconds: Brisk effort (High intensity – you should be breathless).
60 Seconds: Easy recovery (Slow pace to catch your breath).
Repeat: 8 times.
The Vital Stat: Track your Resting Heart Rate (RHR) every Monday morning before getting out of bed. As your heart becomes more efficient, this number will gradually trend downward.
The Accountability Move: Send this guide to a friend who says they "don't have time." If they have 12 minutes, they have enough time to protect their heart.
The Safety First Rule: If you have a known heart condition, hypertension, or joint issues, consult your doctor or physiotherapist to tailor these intensity levels to your specific needs.
Why These Steps Matter
Consistency beats Intensity: Three sessions build the habit; the intervals build the power.
Efficiency: The 12-minute protocol targets arterial stiffness and VO2 max more effectively than a standard 30-minute stroll.
Measurable Progress: Tracking RHR gives you tangible proof that your "pump" is getting stronger, providing a massive boost to long-term motivation."The best investment you can make is in your own health." — Start today, not Monday.
Author’s Note
This article was developed with a clinician’s intent: to bridge the gap between exercise science and real-world cardiovascular care. While the debate between high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) is often framed in absolute terms, the clinical reality is far more nuanced.
As a physician, I do not view exercise modalities as competing ideologies, but as therapeutic tools—each with specific indications, benefits, and limitations. The evidence presented here is drawn from randomized controlled trials, systematic reviews, and meta-analyses across diverse populations, including patients with coronary artery disease, individuals with obesity, sedentary adults, and trained athletes. The goal is not to promote one approach over another, but to empower informed, individualized decision-making grounded in science.
It is important to emphasize that physiological superiority does not always translate into real-world effectiveness. Adherence, safety, patient preference, and clinical context ultimately determine outcomes. For many patients, especially those new to exercise or managing chronic disease, moderate-intensity activity remains the most accessible and sustainable starting point. For others, particularly those seeking time-efficient and potent cardiovascular adaptations, HIIT offers a powerful alternative when appropriately prescribed.
Readers should not interpret this article as a substitute for personalized medical advice. Exercise prescriptions, particularly at higher intensities, should be tailored to individual health status and undertaken with appropriate medical guidance when necessary.
If this article achieves one objective, it is this: to shift the conversation from “Which is better?” to “What is best for this patient, at this moment?”
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
Related Articles
Want Faster Fat Loss? Here's What Science Says About HIIT vs. MICT
HIIT for Athletes: Boost VO₂ Max, Lactate Threshold, and Peak Performance – Science-Based Guide
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
References
Aniya, A. K. D. B., Ninama, K. R., Patel, N. M., & Patel, K. B. B. (2025). Comparative effects of high-intensity interval training and moderate-intensity continuous training on cardiovascular function in sedentary adults. Journal of Heart Valve Disease, 30(7), 26–30.
Gonçalves, C., Bravo, J., Abreu, A., et al. (2025). Comparing high-intensity versus moderate-intensity exercise training in coronary artery disease patients: A randomized controlled trial with 6- and 12-month follow-up. Journal of Public Health (Berlin), 33, 2571–2589. https://doi.org/10.1007/s10389-024-02224-z
Guo, Z., Li, M., Cai, J., Gong, W., Liu, Y., & Liu, Z. (2023). Effect of high-intensity interval training vs. moderate-intensity continuous training on fat loss and cardiorespiratory fitness in the young and middle-aged: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 20(6), 4741. https://doi.org/10.3390/ijerph20064741
K B, S., Vaishali, K., Kadavigere, R., Sukumar, S., K N, S., Pullinger, S. A., & Bommasamudram, T. (2024). Effects of high-intensity interval training versus moderate-intensity continuous training on vascular function among individuals with overweight and obesity: A systematic review. International Journal of Obesity, 48(11), 1517–1533. https://doi.org/10.1038/s41366-024-01586-4
Luo, P., Wu, R., Gao, W., Yan, W., Wang, R., & Ye, Y. (2024). Effects of high-intensity interval exercise on arterial stiffness in individuals at risk for cardiovascular disease: A meta-analysis. Frontiers in Cardiovascular Medicine, 11, 1376861. https://doi.org/10.3389/fcvm.2024.1376861
Marmondi, F., Panascì, M., Filipas, L., Faelli, E. L., & Bonato, M. (2026). High-intensity interval vs moderate-intensity continuous training in endurance runners: A systematic review of physiological, biochemical, physical, and biomechanical adaptations. International Journal of Sports Science & Coaching. Advance online publication. https://doi.org/10.1177/17479541251375315
Su, Z.-Y., Yu, W.-L., Yan, Z.-W., Ding, D.-D., Fang, C.-C., Luo, Q.-L., Liu, X., & Cao, L.-Z. (2024). Comparison of high-intensity interval training and moderate-intensity continuous training on cardiopulmonary function, cardiac autonomic function and vascular function in adolescent boys with obesity: A randomized controlled trial. European Journal of Sport Science, 24, 1871–1882. https://doi.org/10.1002/ejsc.12207