HIIT for Athletes: Boost VO₂ Max, Lactate Threshold & Peak Performance (Science-Based Guide)
Want to improve VO₂ max and delay fatigue? Learn how HIIT boosts athletic performance with proven science, optimal protocols, and real results.
EXERCISE
Dr. T.S. Didwal, M.D.(Internal Medicine)
7/4/202615 min read
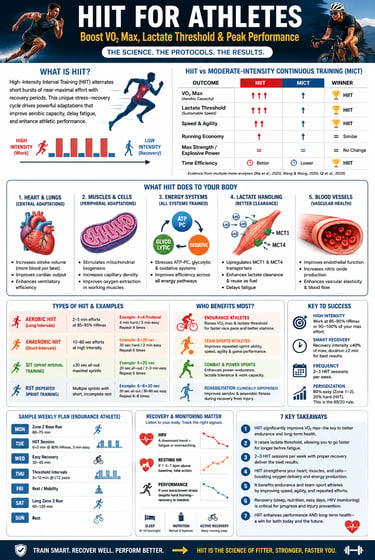
HIIT (High-Intensity Interval Training) is one of the most effective training methods for athletes because it improves VO₂ max, raises the lactate threshold, enhances endurance, and delays fatigue in less time than traditional steady-state cardio. Research shows that performing 2–3 HIIT sessions per week for 4–8 weeks can significantly improve aerobic fitness, speed, and repeated-sprint performance while supporting long-term cardiovascular health when adequate recovery is included.
Key Takeaways
HIIT significantly improves VO₂ max—the body's maximum ability to use oxygen.
A higher VO₂ max means your heart, lungs, and muscles can deliver and use more oxygen during exercise, helping you perform harder for longer while also supporting long-term cardiovascular health (Ma et al., 2023; Qi et al., 2026).HIIT raises your lactate threshold, allowing you to sustain faster speeds before fatigue sets in.
Rather than simply producing less lactate, your body becomes better at clearing and reusing it as fuel through improved buffering capacity and increased monocarboxylate transporter (MCT1 and MCT4) activity. This allows intense exercise to feel easier and be sustained for longer periods (Wang & Wang, 2024; Frontiers in Physiology, 2024).The biggest performance gains come from smart programming—not simply exercising harder.
Research suggests that 2–3 HIIT sessions per week, with carefully planned recovery intervals and training blocks lasting approximately 3–6 or 6–9 weeks, produce the greatest improvements in endurance and athletic performance while minimizing the risk of overtraining (Ma et al., 2023; Wang & Wang, 2024).HIIT strengthens both your heart and your muscles at the cellular level.
It increases stroke volume (the amount of blood pumped with each heartbeat), stimulates mitochondrial biogenesis (the creation of new energy-producing mitochondria), improves muscle capillary density, and enhances oxygen delivery and utilization in working muscles (Ma et al., 2023; PMC, 2024).HIIT is especially effective for endurance and team-sport athletes.
Studies consistently show improvements in VO₂ max, speed, agility, and repeated-sprint ability, making HIIT highly beneficial for runners, cyclists, footballers, basketball players, and other athletes performing repeated high-intensity efforts (Qi et al., 2026; Yuan et al., 2024).Recovery is part of the training—not a break from it.
Adequate sleep, proper nutrition, active recovery, and monitoring markers such as resting heart rate and heart rate variability (HRV) help your body adapt to training, reduce injury risk, and maximize performance gains while preventing overtraining (Ma et al., 2023; Wang & Wang, 2024).HIIT benefits both athletic performance and long-term health.
Beyond improving fitness, HIIT enhances vascular function, insulin sensitivity, cardiorespiratory fitness, and overall metabolic health. Because higher aerobic fitness and VO₂ max are strongly associated with lower risks of cardiovascular disease and premature death, a well-designed HIIT program can improve both athletic performance and lifelong health (Ma et al., 2023; Qi et al., 2026).
What Is HIIT — And Why Should Every Athlete Care?
High-Intensity Interval Training (HIIT) has evolved from a niche conditioning method into one of the most powerful, evidence-based tools in modern sports performance. For decades, athletes and coaches relied heavily on moderate-intensity continuous training (MICT) to build endurance. But a growing body of research now shows that strategically applied bursts of high-intensity work can produce equal—or even superior—adaptations in far less time. This is not just about training harder; it is about triggering a distinct physiological response that reshapes how the body delivers and utilizes oxygen.
At the center of this transformation lies VO₂ max—the gold-standard marker of aerobic capacity—and lactate threshold, the true determinant of sustainable race pace. HIIT uniquely targets both. Repeatedly pushing athletes to intensities near or above their anaerobic threshold, it stimulates central cardiovascular adaptations, such as increased stroke volume, alongside peripheral changes, including mitochondrial biogenesis and improved oxygen extraction (Ma et al., 2023). Even in elite athletes, where physiological ceilings are notoriously difficult to shift, HIIT has demonstrated meaningful improvements in VO₂ max with moderate-to-large effect sizes (Qi et al., 2026).
What makes HIIT particularly compelling is its dual impact: it raises the ceiling (VO₂ max) while simultaneously allowing athletes to operate closer to that ceiling for longer durations by improving lactate clearance and buffering capacity (Wang & Wang, 2024). In an era where marginal gains determine podium finishes, HIIT is no longer optional—it is foundational.
The Physiology: What HIIT Actually Does to Your Body
Understanding why HIIT works so well begins inside your cells. When you push past your anaerobic threshold, a chain reaction unfolds:
Centrally (Heart and Lungs): Your heart adapts by increasing stroke volume — the amount of blood ejected per beat. This means your cardiac output climbs, delivering more oxygen-rich blood per minute. Simultaneously, ventilatory efficiency (VE) improves, making each breath more productive.
Peripherally (Muscles and Mitochondria): Skeletal muscle undergoes remarkable remodeling. Capillary density increases, bringing oxygen closer to working muscle fibers. Most critically, mitochondrial biogenesis accelerates — your cells literally build more mitochondria, the power plants responsible for aerobic energy production. Research confirms that HIIT triggers superior mitochondrial volume density compared to MICT, with distinct changes in mitochondrial network arrangement within myofibers — an adaptation directly tied to enhanced energy metabolism (PMC, 2024).
Energy Systems: HIIT uniquely stresses all three energy pathways — the phosphocreatine (ATP-PC) system during intense efforts, the glycolytic system during sustained high-intensity work, and the oxidative system during recovery. This tri-system challenge is what makes HIIT such a potent stimulus.
VO₂ Max: The Number That Defines Your Aerobic Ceiling
VO₂ max — the maximum volume of oxygen your body can consume per minute per kilogram of body weight — is widely regarded as the gold standard of aerobic fitness. It predicts endurance performance with extraordinary accuracy and is strongly correlated with long-term cardiovascular health and even longevity.
So the key question is: Can HIIT move this number — especially in athletes who are already highly trained?
The evidence is emphatic: Yes.
A landmark 2023 meta-analysis by Ma et al., published in Heliyon, specifically examined VO₂ max responses to HIIT in elite athletes — a population notoriously difficult to improve because they already train near their physiological ceilings. The study included 176 high-level athletes across sports, including kayaking, tennis, taekwondo, triathlons, and cycling. The findings were striking: HIIT significantly increased VO₂ max compared to conventional training (effect size: 0.58; 95% CI: 0.30–0.87, p = 0.03). Critically, the analysis identified that positive training effects were most pronounced when recovery intervals lasted ≥2 minutes and recovery phase intensity stayed ≤40% of maximum effort (Ma et al., 2023).
This is not just a statistically significant result — it is a physiologically meaningful one. For elite athletes, even small gains in VO₂ max can translate to race-winning margins.
More recently, a 2026 systematic review and meta-analysis by Qi et al. in BMC Sports Science, Medicine and Rehabilitation, screening 4,289 titles and including 18 eligible studies, confirmed these findings in trained athletes broadly. HIIT produced a standardized mean difference (SMD) of 1.11 for VO₂ max improvement (95% CI: 0.48–1.74; heterogeneity p < 0.1) — a large effect size by any standard. The same review found that HIIT also significantly improved speed (MD: −0.72) and agility (MD: −0.93), though it did not significantly impact maximal heart rate, jump performance, or explosive power — pointing to HIIT's specific advantage in cardiopulmonary endurance rather than raw strength output (Qi et al., 2026).
The Mechanism Behind VO₂ Max Gains: HIIT improves VO₂ max through two interlocking pathways: (1) increased stroke volume enlarges oxygen delivery, and (2) a widened arteriovenous oxygen difference (a-vO₂ diff) reflects superior extraction of that oxygen at the muscle level. In combination, these adaptations essentially shift your body's oxygen utilization ceiling upward.
HIIT vs. MICT: A Head-to-Head Comparison in Athletes
One of the most important questions in contemporary sports science is not just "does HIIT work?" but "how does HIIT compare to the training athletes are already doing?"
Wang & Wang (2024), publishing in the European Journal of Applied Physiology, conducted a rigorous meta-analysis comparing HIIT and MICT across five major databases to specifically examine aerobic endurance performance parameters in athletes. Their findings offer nuanced, timing-sensitive guidance:
VO₂ max: Both 1–3 week and 4–9 week HIIT blocks were significantly superior to MICT for improving VO₂ max (p < 0.05). However, HIIT spanning 10 weeks or more lost this advantage, suggesting that periodically rotating training stimuli is important.
Anaerobic Threshold (AT): HIIT at 1–3 weeks was significantly more effective than MICT at improving the anaerobic threshold. This early advantage makes HIIT particularly valuable during preseason conditioning blocks.
Ventilatory Efficiency (VE): Six to ten weeks of HIIT outperformed MICT in improving minute ventilation.
Running Economy (RE): Interestingly, HIIT and MICT produced similar improvements in running economy — reinforcing the idea that movement efficiency is more influenced by training volume and technique than by intensity alone.
Hemoglobin (Hb): Within three weeks, MICT outperformed HIIT in improving hemoglobin levels — an important consideration for altitude camps or early-season aerobic base building (Wang & Wang, 2024).
The takeaway for athletes and coaches: HIIT is not a replacement for MICT — it is a strategic, time-sensitive complement. The two modalities serve different phases of the training year, and the smartest programs deploy both intentionally.
Lactate Threshold: The Real Race-Day Performance Marker
While VO₂ max defines your aerobic ceiling, lactate threshold defines how close to that ceiling you can race sustainably. Many coaches and athletes focus so heavily on VO₂ max that they overlook this arguably more trainable — and more performance-predictive — variable.
Understanding Lactate Dynamics: Lactate is not the villain it was once believed to be. It is a metabolic fuel and a valuable signaling molecule. The problem arises when its production overwhelms clearance capacity, causing accumulation and the familiar "burning" sensation that forces you to slow down.
There are two key thresholds to understand:
LT1 (Aerobic Threshold): The intensity at which lactate begins to rise above resting levels — the upper edge of comfortable aerobic effort.
LT2 (Anaerobic Threshold / Lactate Threshold 2): The intensity above which lactate accumulates exponentially — the edge of sustainable race pace for most athletes.
How HIIT Shifts the Threshold: HIIT drives lactate threshold upward through two key biochemical adaptations: (1) improved buffering capacity — your muscles become better at neutralizing hydrogen ions that accumulate alongside lactate, and (2) upregulation of monocarboxylate transporters (MCT1 and MCT4) — specialized proteins that shuttle lactate out of fatiguing muscles and into tissues where it can be oxidized as fuel. Research has confirmed that HIIT interventions significantly improve blood lactate clearance — with HIIT-trained subjects showing faster lactate removal at 15 and 30 minutes post-exercise compared to MICT-trained counterparts (Frontiers in Physiology, 2024).
Practical Protocols for Threshold Improvement:
Tempo Intervals: 10–20 minute efforts at LT2 pace with 3–5 minutes recovery — directly stresses the threshold zone.
Cruise Intervals: 4–6 × 5 minutes at threshold pace — trains lactate clearance while maintaining high cardiac output.
Types of HIIT: Matching the Method to the Athlete
Not all HIIT is created equal. Protocol selection should be driven by sport demands, training phase, and the specific physiological variable being targeted.
Aerobic HIIT (Long Intervals — 2–5 minutes): These longer intervals maximally stress VO₂ max by keeping the cardiovascular system near its upper limit for sustained periods. The famous Norwegian 4×4 protocol (4 minutes at 90–95% HRmax, 3 minutes active recovery, repeated 4 times) is the most rigorously validated example in the scientific literature. This is the preferred modality for endurance athletes — runners, cyclists, triathletes.
Anaerobic HIIT (Short Intervals — 10–60 seconds): Short, intense efforts develop glycolytic capacity and neuromuscular power. These are particularly valuable for team-sport athletes who need to generate high outputs repeatedly.
Sprint Interval Training (SIT — ≤30 seconds maximal sprints): SIT uses all-out efforts to generate a massive mitochondrial stimulus. A network meta-analysis comparing HIIT, SIT, and Repeated Sprint Training (RST) across 51 eligible studies involving 1,261 athletes found that RST demonstrated the highest probabilistic efficacy for VO₂ max improvement, followed by HIIT and SIT. Optimal SIT protocols involved sprints of ≤30 seconds with recovery periods under 97 seconds at 3 sessions per week over 3–6 weeks (BMC Sports Sci, 2025).
Repeated Sprint Training (RST): RST — multiple sprint repetitions with short, incomplete recovery — is the bread and butter of team-sport conditioning. A PLOS ONE meta-analysis found HIIT significantly improved VO₂ max, Yo-Yo Intermittent Recovery Test performance, and repeated-sprint ability in male team-sport athletes, confirming its value across football, basketball, and hockey contexts (Yuan et al., 2024).
Sport-Specific Applications: HIIT Across the Athletic Spectrum
Endurance Sports (Marathon, Cycling, Triathlon): In endurance athletes, HIIT's primary value lies in pushing both the VO₂ max ceiling and the lactate threshold upward. The combined effect: athletes can sustain higher absolute speeds at race pace. Research from Harinaracim & Sathya (2025) comparing HIIT and conventional endurance training in elite athletes confirmed meaningful improvements in endurance performance markers, with HIIT demonstrating particular advantages in time-trial performance and aerobic power output (Harinaracim & Sathya, 2025).
Team Sports (Football, Basketball, Hockey): These athletes need VO₂ max for repeated-effort recovery AND anaerobic capacity for explosive actions. HIIT's ability to simultaneously improve both systems makes it ideal. Small-sided games (SSGs) — a sport-specific form of HIIT — integrate cardiovascular training, tactical skill, and agility into a single session, making them extremely time-efficient for team-sport settings.
Combat and Power-Endurance Sports (Boxing, Wrestling, MMA): These athletes live at the intersection of glycolytic power and lactate tolerance. High-intensity rounds demand enormous lactate buffering capacity. HIIT protocols that simulate work-rest ratios of actual competition (e.g., 3 minutes hard : 1 minute rest for boxing) develop sport-specific tolerance more effectively than generic conditioning.
Designing an Evidence-Based HIIT Program
The most important lesson from the research is that protocol details matter enormously. Randomly "going hard" is not HIIT — it is exhausting yourself. Effective HIIT is precise.
Key variables to control:
Intensity: 85–95% of HRmax or 90–100% of VO₂ max velocity
Work Duration: 30 seconds to 5 minutes per interval, depending on the goal
Recovery Duration: Generally 1:1 to 1:2 work-to-rest ratios; recovery intensity ≤40% of maximum
Session Volume: 4–8 intervals per session
Weekly Frequency: 2–3 sessions per week of high-intensity work
Periodization — The 80/20 Model: The polarised training model, supported by extensive elite athlete data, recommends spending approximately 80% of total training volume at low intensity (Zone 1–2) and 20% at high intensity. This ratio avoids the "moderate-intensity trap" that leaves athletes chronically fatigued without the specific adaptations of either end of the spectrum.
Sample Weekly Structure (Endurance Athlete):
Monday: Zone 2 base run (60–75 minutes)
Tuesday: HIIT — 6×3 minutes at 90% HRmax, 3 minutes active recovery
Wednesday: Easy recovery ride or run (30–45 minutes)
Thursday: Threshold intervals — 3×10 minutes at LT2 pace
Friday: Rest or mobility
Saturday: Long Zone 2 run (90–120 minutes)
Sunday: Rest
Recovery and Overtraining: The Other Half of the Equation
HIIT's power is matched by its demand. Without adequate recovery, HIIT does not produce supercompensation — it produces breakdown.
Biomarkers to Monitor:
Heart Rate Variability (HRV): A declining HRV trend over multiple days signals insufficient recovery and impending overtraining.
Resting Heart Rate: Elevated resting HR (>5–7 bpm above baseline) indicates sympathetic nervous system stress.
Performance Decline: Objective power or pace data is the most reliable overtraining marker — if you are training hard but getting slower, something is wrong.
Recovery Optimization:
Nutrition: Post-HIIT carbohydrate replacement (1.0–1.2 g/kg body weight in the first 30–60 minutes) restores glycogen and supports adaptation.
Sleep: 8–10 hours for athletes in heavy training blocks; the majority of training adaptation occurs during slow-wave sleep.
Active Recovery: Low-intensity movement (Zone 1 cycling, walking) on recovery days accelerates lactate clearance and maintains blood flow without adding training stress.
Practical Applications: What You Can Start Doing Today
The research is clear. Here is how to bring it into your training — whether you are an athlete, a coach, or a sports medicine professional advising patients:
For Endurance Athletes: Begin with the Norwegian 4×4 protocol twice per week for 6–8 weeks. Monitor VO₂ max every 4 weeks using a time-trial test (e.g., 3,000 m run test). Expect meaningful VO₂ max improvements within 4–6 weeks.
For Team-Sport Athletes: Incorporate 2 RST sessions per week (6–8 × 30-second sprints at maximum effort, 2–4 minutes recovery) during the preseason. Track Yo-Yo Intermittent Recovery Test scores at 4-week intervals.
For Combat Sports Athletes: Design HIIT protocols that mirror your competition's work-to-rest ratio. Use lactate testing (if available) to assess threshold shifts across a training block.
For Coaches and Clinicians: Screen athletes for cardiovascular risk before initiating high-intensity programs. Use HRV monitoring and objective performance tracking to individualize load. Remember that 6–9 week HIIT blocks appear optimal for VO₂ max and ventilatory improvements — rotating to MICT or deload blocks beyond this window maintains gains while reducing injury risk (Wang & Wang, 2024).
Track What Matters: The three most important metrics to monitor in any HIIT program are: (1) VO₂ max or its field-test proxy, (2) lactate threshold pace or power, and (3) daily HRV. Together, these three numbers paint a complete picture of adaptation vs. fatigue.
Frequently Asked Questions (FAQs)
Q1. How quickly can HIIT improve my VO₂ max?
Most studies show measurable VO₂ max improvements within 4–6 weeks of structured HIIT, with 3 sessions per week. Elite athletes may need longer blocks (6–9 weeks) to see significant gains given their already high baseline fitness.
Q2. Is HIIT safe for all athletes, including those recovering from injury?
HIIT can be safe and beneficial even during rehabilitation, but it must be carefully supervised. Research in young football players returning from injury showed HIIT was slightly more effective than MICT for improving aerobic and anaerobic fitness during rehabilitation — but proper medical clearance and progressive overload are essential.
Q3. How is HIIT different from Sprint Interval Training (SIT)?
HIIT typically involves efforts of 30 seconds to 5 minutes at 85–95% HRmax. SIT uses shorter, all-out maximal efforts (≤30 seconds) with longer relative recovery. Both improve VO₂ max, but SIT generates a particularly intense mitochondrial stimulus. Your choice depends on your sport's energy demands and current fitness level.
Q4. Can I do HIIT every day?
No, and the research is clear on this. High-intensity work should represent no more than 20% of your total training volume (the 80/20 rule). Most athletes should limit HIIT to 2–3 sessions per week, with adequate Zone 1–2 work and recovery days between sessions.
Q5. Does HIIT improve lactate threshold, or just VO₂ max?
Both. HIIT improves lactate dynamics by increasing MCT1 and MCT4 transporter density (improving lactate clearance) and enhancing muscle buffering capacity. Studies show HIIT-trained athletes clear lactate significantly faster post-exercise compared to MICT-trained athletes — a critical advantage in race or game situations.
Q6. Should female athletes train differently with HIIT?
The evidence is still evolving, but current meta-analyses show both male and female athletes benefit meaningfully from HIIT. Some research suggests female athletes may demonstrate slightly different hormonal recovery profiles, particularly around menstrual cycle phases — so monitoring fatigue markers is especially important. Individualization is key.
Q7. What is the best HIIT protocol for team-sport athletes like footballers or basketball players?
For team sports, Repeated Sprint Training (RST) and small-sided games represent the most sport-specific HIIT modalities. Research confirms that HIIT significantly improves VO₂ max, Yo-Yo Intermittent Recovery Test performance, and repeated-sprint ability in male team-sport athletes. A practical starting point: 3 sessions/week of 6–8 × 30-second maximal sprints with 2–3 minutes recovery over a 3-week block.
Call to Action: Take the Next Step in Your Performance Journey
If you have read this far, you understand one thing clearly: training smarter — not just harder — is what separates good athletes from great ones.
Here is how to move forward today:
Start Your HIIT Self-Assessment: Before changing your training, establish your baseline. Run a 3,000 m time trial or perform a submaximal step test to estimate your current VO₂ max. Record your resting HR and download a free HRV app. These three numbers will become your performance compass.
Build Your 6-Week HIIT Block: Use the weekly programming framework above. Commit to 2–3 HIIT sessions per week, log every session, and retest your time trial at week 4 and week 6. The data will tell its own story.
Dive Deeper: This blog post is a companion to Chapter 17 of our comprehensive performance physiology book. The full chapter includes detailed physiology diagrams, protocol comparison tables, and case studies from elite endurance and team-sport athletes. [Link to Book/Chapter]
Join the Conversation: Have you tried a structured HIIT block? What protocol worked best for you — or what questions do you still have? Drop your experience in the comments below.
Author’s Note
This chapter reflects an intersection I have spent years navigating—where clinical medicine meets human performance. As a physician trained in internal medicine and deeply engaged with exercise physiology research, I have always been struck by a simple but powerful truth: the same biological systems that determine disease risk also define athletic potential. Nowhere is this more evident than in the study of high-intensity interval training (HIIT).
What makes HIIT fascinating is not just its efficiency, but its physiological precision. It challenges the heart, lungs, vasculature, skeletal muscle, and cellular metabolism in a way that few other training modalities can. Yet, like any powerful intervention, its benefits are dose-dependent and context-specific. In clinical practice, I have seen both sides—remarkable improvements in cardiometabolic health and performance when applied correctly, and burnout, injury, or overtraining when misused.
This article was written with a clear intention: to move beyond oversimplified fitness narratives and present HIIT as it truly is—a scientifically grounded, clinically relevant, and highly adaptable training tool. Every concept discussed here is anchored in peer-reviewed research, but equally important, translated into practical application for athletes, coaches, and healthcare professiona
Related Articles
The Physiology of HIIT: Mitochondria, Oxygen & Energy Systems
VO₂ Max vs Lactate Threshold Explained: What Truly Determines Your Fitness
HIIT vs Moderate Cardio: Which Improves Cardiovascular Fitness Faster?
Is Your Heart at Risk? How the TG/HDL Ratio Can Warn You Early | DR T S DIDWAL
How Exercise Boosts Nitric Oxide and Blood Flow: The Endothelial Shear Stress Mechanism
Exercise and Vascular Health: How Nitric Oxide and Endothelial Function Keep Your Arteries Young
Medical Disclaimer: This article is intended for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for consultation with a qualified healthcare professional. Always discuss exercise programmes and cardiac risk assessment with your doctor, particularly if you have existing cardiovascular disease or significant risk factors.
References
Ma, X., Cao, Z., Zhu, Z., Chen, X., Wen, D., & Cao, Z. (2023). VO₂max (VO₂peak) in elite athletes under high-intensity interval training: A meta-analysis. Heliyon, 9(6), Article e16663. https://doi.org/10.1016/j.heliyon.2023.e16663
Wang, Z., & Wang, J. (2024). The effects of high-intensity interval training versus moderate-intensity continuous training on athletes' aerobic endurance performance parameters. European Journal of Applied Physiology, 124, 2235–2249. https://doi.org/10.1007/s00421-024-05532-0
Qi, K., Tan, L., Xu, Q., et al. (2026). Effects of high-intensity interval training on aerobic capacity and athletic performance in trained athletes: A systematic review and meta-analysis. BMC Sports Science, Medicine and Rehabilitation, 18, 41. https://doi.org/10.1186/s13102-025-01479-7
Harinaracim, M., & Sathya, E. (2025). The impact of high-intensity interval training (HIIT) on endurance performance in elite athletes: A comparative analysis. International Journal of Sports, Health and Physical Education, 7(1), 25–29. https://www.physicaleducationjournal.in/archives/2025/vol7issue1/PartA/6-2-5-344.pdf
Yuan, Y., Soh, K. G., Qi, F., Bashir, M., & Zhao, N. (2024). Effects of high-intensity interval training on selected indicators of physical fitness among male team-sport athletes: A systematic review and meta-analysis. PLOS ONE. https://doi.org/10.1371/journal.pone.0310955