The New Era of Fatty Liver Disease: What Every Patient Should Know About New Treatments
Can MASLD be reversed? Explore the newest evidence on fatty liver disease, including breakthrough treatments, non-invasive diagnosis, lifestyle changes, and expert clinical insights.
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/29/202631 min read
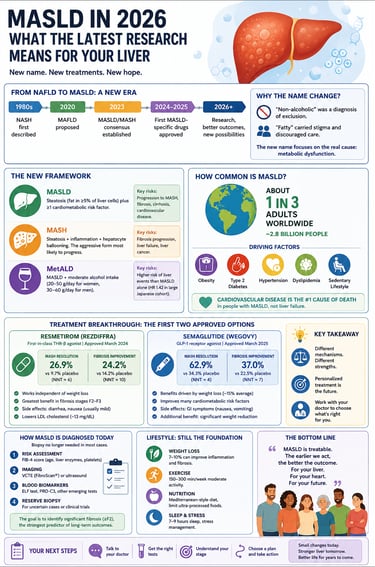
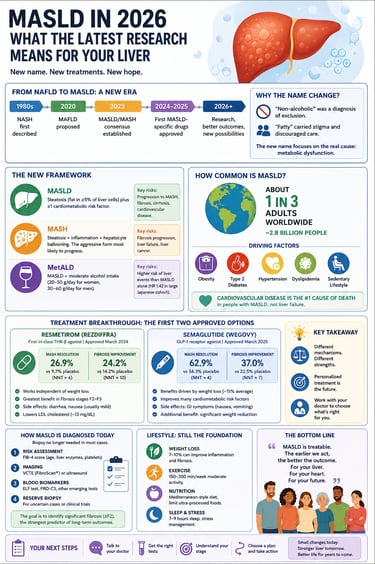
MASLD (metabolic dysfunction-associated steatotic liver disease) is the new name for most cases previously called NAFLD. It occurs when excess fat accumulates in the liver in people with metabolic risk factors such as obesity, diabetes, high blood pressure, or abnormal cholesterol. About 1 in 3 adults worldwide has MASLD, and the main long-term risk is often heart disease rather than liver failure.
Key takeaways
The Name Change Reflects Biology, Not Just Semantics: The shift from NAFLD to MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease) replaces a diagnosis of exclusion ("non-alcoholic") with affirmative cardiometabolic criteria. The newly defined MetALD category reveals that even modest alcohol intake combined with metabolic risk factors increases liver-related events by 42% (hazard ratio 1.42).
MASLD is a Global Epidemic and a Cardiovascular Threat: Affecting 1 in 3 adults worldwide, MASLD prevalence is projected to exceed 55% by 2040. Crucially, cardiovascular disease—not liver failure—is the leading cause of death across the MASLD spectrum until a patient develops advanced cirrhosis.
Fibrosis Stage, Not Fat Percentage, Dictates Your Risk: The actual amount of fat in the liver does not predict long-term health outcomes. Long-term risk is entirely driven by scarring (fibrosis); a patient with stage F4 fibrosis (cirrhosis) faces a 32-fold jump in liver-related events compared to someone at stage F0–F1.
"Burned-Out MASLD" is a Dangerous Diagnostic Trap: A counterintuitive drop in liver fat on a follow-up scan can actually signal that the disease has progressed to an advanced stage where heavily scarred tissue can no longer store fat. A fat reduction is only positive if fibrosis markers are actively improving alongside it.
The Diagnostic Framework Has Shifted Away From Biopsies: Driven by biopsy limitations (sampling errors and procedural risks), modern guidelines mandate a stepwise, non-invasive approach. Doctors now utilize the free, blood-test-based FIB-4 index as a first-line screen, reserving specialized elastography (FibroScan), MRI-PDFF, and biopsies only for indeterminate or high-risk cases.
Resmetirom (Rezdiffra) Heals the Liver from the Inside Out: Approved in 2024, this daily oral pill acts as a liver-targeted thyroid hormone receptor-beta (THR-β) agonist, treating a state of localized "liver hypothyroidism." It rapidly clears liver fat and resolves MASH in 25–30% of patients, while also lowering LDL cholesterol, though it does not improve blood sugar.
Semaglutide (Wegovy) Delivers Massive, Weight-Driven Resolution: Approved for MASH in late 2025 based on the landmark ESSENCE trial, this weekly injection resolves MASH in 62.9% of patients and improves fibrosis in 36.8%. Its liver benefits scale directly with weight loss, pushing resolution rates above 71% for those who lose more than 7% of their body weight.
Lifestyle is still the Foundation, but Drugs Bridge the Compliance Gap: Achieving a 10% body weight loss through diet and exercise resolves MASH in 90% of cases and reverses scarring in 50%—outperforming any drug. However, because long-term lifestyle changes are notoriously difficult to sustain, these new therapies provide a critical, life-saving safety net for the vast majority of patients.
If you've been told you have a "fatty liver," or your latest bloodwork flagged elevated liver enzymes, you've probably searched for answers and found a confusing tangle of acronyms — NAFLD, NASH, MAFLD, MASLD, MASH. The terminology changed in 2023, the diagnostic criteria changed with it, and in the two years since, the treatment landscape has changed faster than almost any other area of liver medicine in decades.
This article exists because most of what's written about metabolic dysfunction-associated steatotic liver disease (MASLD) is either outdated (written before the 2024 approval of the first MASLD-specific drug, or before the 2025 approval of the second one), too technical to be useful to a patient, or too vague to help you understand what your own test results actually mean.
We're going to do something different here: walk through what recent peer-reviewed research — published in Cellular & Molecular Immunology, Nature Reviews Drug Discovery, Scientific Reports, Molecular Biomedicine, and the Journal of Gastroenterology, among others — actually found, and then spend real time on what those findings mean clinically. Not just "the drug worked," but: how much did it work, in whom, with what tradeoffs, and how does a clinician (or a well-informed patient) actually use that information.
What Is MASLD, and Why Did the Name Change?
If you were diagnosed before 2023, you were probably told you had "non-alcoholic fatty liver disease" (NAFLD) or, if it had progressed, "non-alcoholic steatohepatitis" (NASH). In June 2023, a multisociety panel of international liver specialists formally retired those names.
The reasoning was twofold. First, "non-alcoholic" is a diagnosis of exclusion — it tells you what the disease isn't caused by, not what it is caused by. Second, the word "fatty" carried stigma that researchers found was discouraging people from seeking care.
The new framework, in plain terms:
MASLD (metabolic dysfunction-associated steatotic liver disease): fat buildup in the liver (steatosis, affecting at least 5% of liver cells) plus at least one cardiometabolic risk factor — things like elevated waist circumference, high blood pressure, prediabetes or diabetes, elevated triglycerides, or low HDL cholesterol.
MASH (metabolic dysfunction-associated steatohepatitis): the more aggressive form, where steatosis is joined by inflammation and a specific kind of cell injury called hepatocyte ballooning. This is the stage most likely to progress to scarring.
MetALD: a newly defined middle category for people who have MASLD's metabolic risk factors and drink more alcohol than the MASLD threshold allows (20–50 g/day for women, 30–60 g/day for men) but less than what defines alcohol-associated liver disease.
This isn't just semantics. Research published in 2026 in the Journal of Gastroenterology — the evidence-based guideline update from the Japanese Society of Gastroenterology and Japan Society of Hepatology — found that MetALD carries a meaningfully higher risk of liver-related events than MASLD alone (hazard ratio 1.42 in one large Japanese cohort of roughly 760,000 people), even though the alcohol involved falls below what's traditionally considered "heavy drinking." That distinction changes how a doctor counsels you about alcohol, and it didn't exist in the old framework.
If you were diagnosed under the old NAFLD/NASH system, nothing about your actual disease changed — the diagnostic criteria are designed to capture essentially the same population, and the evidence base built up over decades of NAFLD research still applies directly to MASLD. You haven't been "re-diagnosed" with something new; the label was updated to better reflect the biology.
How Common Is This, Really?
This is, by a wide margin, the most common chronic liver disease on the planet, and it's getting more common.
Global prevalence is approximately 30% of adults — roughly 1 in 3 people — according to a 2023 systematic review covering data through 2019, with regional variation from about 25% in Western Europe up to over 44% in Latin America.
Between 1990 and 2021, the global affected population more than doubled to an estimated 1.3 billion people, and forecasting models project prevalence will exceed 55% by 2040 if current trends continue.
In Japan specifically, prevalence has risen from roughly 22% in the mid-2000s to nearly 30% by 2016, and is forecast to climb from 33.7% in 2020 to 44.8% by 2040 — driven in part by an aging population and a notable subgroup of "lean MASLD" patients (people with the disease despite a normal body weight), who make up about 20.7% of Japan's MASLD population.
Among people who are overweight or obese, prevalence climbs to 70–75%. Among people with type 2 diabetes, it's roughly 69%.
Only an estimated 5% of people with MASLD progress to MASH, but that minority carries almost all of the disease's serious risk.
The clinically important point most people miss: MASLD is not primarily a liver disease in terms of what kills people. Cardiovascular disease — heart attacks and strokes — is the leading cause of death across the entire MASLD spectrum, until a person develops cirrhosis, at which point liver-specific complications take over as the dominant risk. A 2026 meta-analysis covering roughly 5.8 million participants found MASLD was associated with a 45% increase in cardiovascular disease risk (hazard ratio 1.45). This is why a MASLD diagnosis should trigger cardiovascular risk evaluation, not just liver monitoring — and it's also why GLP-1 drugs that were developed for diabetes and obesity have turned out to be such a natural fit for this disease.
MASLD is also independently linked to a higher risk of chronic kidney disease (45–53% increased risk) and several cancers — colorectal cancer most consistently (28% increased risk in one large Japanese cohort of about 6 million people), with signals for gastric, esophageal, breast, pancreatic, and gynecologic cancers as well.
What's Actually Happening in Your Liver
Understanding the mechanism matters here for a very practical reason: the two FDA-approved drugs for this disease work through completely different pathways, and knowing why helps explain why your doctor might recommend one, the other, or eventually both together.
The "multiple hit" model
Older theories described MASLD progression as a "two-hit" process. Current research, including a comprehensive 2026 review in Molecular Biomedicine, has replaced this with a "multiple-hit" model — genetic predisposition, insulin resistance, gut microbiome changes, and diet all acting simultaneously rather than sequentially.
Here's the simplified chain of events:
Fat overload. Roughly 59% of the fat that accumulates in a MASLD liver comes from fatty acids released by insulin-resistant fat tissue elsewhere in the body; about 26% is newly manufactured by the liver itself (a process called de novo lipogenesis, driven by excess carbohydrate and insulin); the remaining 15% comes directly from dietary fat.
Lipotoxicity. Certain fat byproducts — not triglycerides themselves, but related toxic lipid species like ceramides and free cholesterol — damage the cell's mitochondria (its energy factories) and trigger oxidative stress.
Inflammation. Damaged liver cells release distress signals that activate the liver's resident immune cells, called Kupffer cells, and recruit additional immune cells from the bloodstream. This is the step that converts simple fatty liver into the more dangerous steatohepatitis (MASH).
Fibrosis. Chronic inflammation activates hepatic stellate cells, which begin laying down scar tissue (collagen). This fibrosis — not the amount of fat itself — is what actually predicts your long-term risk of cirrhosis, liver failure, and liver cancer.
This last point deserves emphasis because it's one of the most clinically important and most commonly misunderstood facts about this disease: the amount of fat in your liver does not reliably predict your outcome. The amount of scarring (fibrosis stage) does.
The immune system's role — why it matters for new drug development
A detailed 2025 review in Cellular & Molecular Immunology mapped out just how central immune cells are to this process, and the findings reshape how researchers think about future treatments.
Macrophages change character as disease progresses. A healthy liver is dominated (over 90%) by long-term resident immune cells called Kupffer cells. As MASLD develops, these original cells die off and get replaced by new immune cells recruited from the bone marrow. Some of these recruited cells — particularly a subtype marked by a protein called TREM2 — are actually protective: research shows that mice lacking TREM2 develop worse fibrosis, and TREM2-positive cells are essential for fibrosis to resolve once a person loses weight or otherwise improves their metabolic health. This matters clinically because it suggests fibrosis regression is an active, immune-cell-dependent repair process, not just the passive absence of injury — a concept with real implications for how long improvement might take and how it might be supported.
Specific immune subtypes correlate with worse fibrosis. A particular population of T-cells (CXCR6+ CD8+ T cells, and a Th17-polarized subset of CD4+ T cells) shows up disproportionately in people with MASH-related fibrosis, giving researchers specific molecular targets for next-generation drugs that current resmetirom and semaglutide therapy don't touch.
Why this matters practically: Both of the currently approved drugs act primarily on metabolism — they make the liver process fat more efficiently or reduce the amount of fat arriving at the liver in the first place. Neither directly targets the immune inflammatory cascade described above. That gap is exactly where the next wave of drugs in clinical trials (discussed in the pipeline section below) is aimed, and it's also a big part of why combination therapy is being actively studied: a metabolic drug plus an anti-inflammatory or antifibrotic drug, working on different parts of the same disease process.
Genetics: why some people get sicker on the same diet
Not everyone with obesity develops MASH, and some lean people do. Genetics explains a meaningful part of that — heritability estimates run 35–61%.
The most important gene by far is PNPLA3, specifically a variant called I148M. This single genetic change is associated with roughly double the risk of MASLD, a similar increase in MASH risk, and — in people who are homozygous for it (carry two copies) — up to a 10-fold increased risk of liver cancer in some European cohorts. In Japanese cohorts, the PNPLA3 GG genotype carried odds ratios of 13.2 to 22.3 for liver-related events including liver cancer, and the variant is more frequent and more clinically significant in lean MASLD patients specifically.
Other genes worth knowing about if you've had genetic testing or a family history discussion with your doctor:
TM6SF2 — increases liver disease risk but, interestingly, decreases cardiovascular risk, illustrating how this disease doesn't behave uniformly across organ systems
HSD17B13 — a protective variant; having it lowers your risk of progression
MBOAT7 and GCKR — both associated with increased risk, particularly for fibrosis
If you have a first-degree relative with MASLD, your own risk of advanced fibrosis can be up to 12-fold higher than the general population — a fact worth raising with your doctor if you haven't already.
How MASLD Is Diagnosed Today
This is an area that has changed substantially even in the last two years, and it's worth understanding because it affects whether you'll need an invasive liver biopsy at all.
The biopsy problem
Liver biopsy has long been the diagnostic "gold standard," but recent research has been notably candid about its real-world limitations. A 2025 review in npj Gut and Liver points out that a typical biopsy samples only about 1/50,000th of the total liver — meaning it can easily miss disease that's unevenly distributed, and two pathologists looking at the same sample can disagree on key findings like inflammation grade. Biopsy also carries real procedural risk (pain, bleeding, rarely worse) and cost.
Clinical interpretation: this doesn't mean biopsy is useless — it remains essential when the diagnosis is unclear or when a doctor needs to rule out other liver diseases — but it explains why guidelines worldwide, including Japan's newly updated 2026 evidence-based guidelines, now reserve biopsy for specific situations rather than using it as the default first step.
The stepwise, non-invasive approach most doctors now use
Step 1 — FIB-4 index. This is a simple calculation using your age, AST, ALT, and platelet count — values from blood tests you likely already have. No biopsy, no imaging, no extra cost. It's now the recommended first-line tool in essentially every major guideline worldwide.
FIB-4 below 1.3 (or below 2.0 if you're over 65): low risk, can typically be followed by your primary care doctor
FIB-4 between 1.3 and 2.67: intermediate risk, warrants further testing
FIB-4 above 2.67: high risk, referral to a liver specialist is recommended
A 2026 Japanese health-economic analysis found that routing patients through FIB-4 first, before deciding whether further specialist tests are needed, reduced unnecessary specialist referrals by 33.7–40.6% while actually lowering total cost per diagnosed patient compared with standard care.
Step 2 — Second-line non-invasive tests for people who land in the intermediate-or-higher risk zone. Options now include:
Elastography (FibroScan/VCTE, or shear-wave ultrasound) — measures liver stiffness directly. A liver stiffness reading below 8 kPa makes significant fibrosis unlikely; above 12 kPa makes it likely. In 2025, the FDA accepted FibroScan liver stiffness measurement as a reasonable alternative to biopsy in clinical trials for non-cirrhotic MASH — a meaningful regulatory shift.
MRI-PDFF (magnetic resonance imaging-proton density fat fraction) — the most accurate non-invasive measure of liver fat, with one Japanese validation study reporting 90% accuracy for detecting at least moderate steatosis. It's expensive and not universally available, but it's increasingly used as the reference standard in clinical trials, replacing biopsy.
Blood-based fibrosis markers — Enhanced Liver Fibrosis (ELF) test, type IV collagen 7S, Mac-2 binding protein glycosylation isomer (M2BPGi, widely used in Japan), and cytokeratin-18 fragments (a marker of cell death that helps flag active inflammation, not just scarring).
Composite scores combining imaging and blood markers — FAST score (FibroScan + AST), MAST score (MRI + AST), and MEFIB index (MRI elastography + FIB-4) all outperform any single test alone, with the FAST score achieving an AUROC (a measure of diagnostic accuracy, where 1.0 is perfect and 0.5 is no better than chance) of 0.90 in validation studies.
Step 3 — Biopsy, reserved for cases where non-invasive tests disagree with each other, where the diagnosis remains unclear, or where a definitive answer is needed before starting a specific drug therapy.
Why fibrosis stage, not fat percentage, is what actually matters
This is worth restating because it changes how you should read your own results. A study of nearly 1,400 Japanese patients with biopsy-confirmed disease found liver-related event rates of:
2.8 per 1,000 person-years at fibrosis stage F0–1 (none to minimal scarring)
5.4 per 1,000 person-years at F2
21.5 per 1,000 person-years at F3
90.1 per 1,000 person-years at F4 (cirrhosis)
That's roughly a 32-fold jump in event rate between minimal fibrosis and cirrhosis. Liver cancer incidence followed a similar but less steep pattern (1.7 → 4.5 → 14.2 → 16.9 per 1,000 person-years across the same stages). This is precisely why your doctor cares far more about your fibrosis stage than about how much fat showed up on your ultrasound.
One more nuance worth knowing: a phenomenon called "burned-out MASLD" describes patients whose liver fat has actually decreased — sometimes because the disease has progressed to the point that scarred tissue simply can't store as much fat anymore — while their fibrosis and cirrhosis risk remain high or even worsen. A 2025 study using FibroScan found patients with low-grade steatosis (counterintuitively) had higher rates of liver failure than those with moderate-to-severe steatosis. The clinical takeaway: a drop in liver fat on a follow-up scan is reassuring only in the context of fibrosis markers — it is not, by itself, proof your liver is getting healthier.
Treatment: What Actually Works, by the Numbers
For decades, MASLD/MASH had zero FDA-approved drug treatments. That changed twice in close succession — resmetirom in March 2024, and semaglutide (under the brand name Wegovy, already familiar to many as a weight-loss drug) in August 2025. Both target different parts of the disease process described above, and understanding how they differ is the key to understanding which patients each one suits.
Before either drug, lifestyle intervention was — and remains — the foundation of treatment. It's worth saying plainly: no drug replaces this. A frequently cited finding in MASH research is that people who achieve at least 10% body weight loss through diet and exercise alone see roughly 90% resolution of steatohepatitis and nearly 50% fibrosis regression on biopsy — numbers that meet or exceed what either approved drug achieves on its own. The drugs matter most for patients who cannot reach or sustain that level of weight loss, which, realistically, is most people — multiple reviews note that lifestyle changes, while effective when achieved, are notoriously difficult to sustain long-term.
Resmetirom (Rezdiffra) — Interpreting the Trial Data
What it is and how it works
Resmetirom is an oral, liver-targeted, selective thyroid hormone receptor-beta (THR-β) agonist. Here's the clinical logic: thyroid hormone signaling through the THR-β receptor in liver cells normally promotes fat-burning, bile acid production, and reduces fat and cholesterol storage. Research suggests MASLD is partly a state of localized liver hypothyroidism — even when a person's overall thyroid blood tests are completely normal — caused by the liver shifting away from producing the active form of thyroid hormone (T3) and toward an inactive form (reverse T3). Resmetirom restores that local signaling specifically inside liver cells.
Two design features matter clinically:
28-fold greater selectivity for THR-β over THR-α compared with the body's natural thyroid hormone, which is what protects the heart and bones from the harmful effects of excess thyroid stimulation (THR-α is the receptor subtype responsible for those side effects).
Liver-directed uptake via specific transport proteins that concentrate the drug in liver cells rather than letting it circulate systemically — another layer of selectivity that helps explain its relatively clean systemic side-effect profile.
The actual trial numbers
A 2024 systematic review and meta-analysis in Scientific Reports, registered with PROSPERO and pooling four randomized controlled trials (2,359 participants total; the formal meta-analysis included 2,234), found:
Liver fat reduction (MRI-PDFF), the primary efficacy measure:
Dose Timepoint Effect vs. placebo 80 mg 36–52 weeks −27.7 percentage points (p<0.00001) 80 mg 12–16 weeks −30.9 percentage points (p<0.00001) 100 mg 36–52 weeks −36.1 percentage points (p<0.00001) 100 mg 12–16 weeks −36.9 percentage points (p<0.00001)
Clinical interpretation: these are large, statistically unambiguous effects, and they appear quickly (most of the benefit is already present by 12–16 weeks). Critically, prior research (cited within this meta-analysis) established that a ≥30% relative reduction in liver fat by MRI-PDFF predicts a meaningfully higher chance of actual histologic improvement on biopsy — meaning these imaging changes aren't just a number moving on a scan, they track with real tissue-level improvement.
The histologic endpoints that matter most — from the pivotal MAESTRO-NASH phase 3 trial (cited within the broader literature on resmetirom): MASH resolution without worsening fibrosis was achieved in 25.9% of patients on 80 mg and 29.9% on 100 mg, compared with 9.7% on placebo. That's roughly a 2.7- to 3-fold improvement over placebo — a clinically meaningful difference, though it also means roughly 70–75% of treated patients did not achieve full resolution within the trial period. This is the number worth discussing directly with a doctor: resmetirom moves the needle substantially, but it is not a cure for most patients in the timeframe studied.
Beyond liver fat — the secondary findings:
LDL cholesterol: reduced by roughly 12.4–15.6 mg/dL versus placebo, both doses, both early and late timepoints
Triglycerides: reduced by roughly 18–24 mg/dL versus placebo
Liver enzymes (ALT, AST, GGT): significantly reduced at the 80 mg dose; AST and GGT reductions did not reach statistical significance at 100 mg in this pooled analysis, an inconsistency the original authors flag as worth confirming in larger trials
CK-18 (a marker of liver cell death): reduced by roughly 121–124 U/L versus placebo — meaningful because this tracks active cell injury, not just fat content
Blood sugar control (HbA1c, fasting insulin): no significant improvement at either dose. This is clinically important: resmetirom is not a metabolic/diabetes drug in the way semaglutide is, and shouldn't be expected to improve glycemic control.
The hormonal side effects worth knowing about:
Free T4 dropped significantly at both doses — believed to reflect less conversion to the inactive reverse-T3 form and more conversion to active T3, which the trial authors interpret as a sign the drug is working as intended rather than as a sign of drug-induced hypothyroidism. Still, this is something your doctor needs to interpret carefully if they're also checking your thyroid function for unrelated reasons — a falling FT4 on resmetirom is expected, not necessarily alarming.
Sex hormone binding globulin (SHBG) rose significantly in both sexes — a direct, expected marker of THR-β activation in the liver, and actually used by researchers as a biomarker confirming the drug reached its target.
Testosterone and estradiol increased in men; modest increases in some female hormone measures.
The original researchers explicitly note: "It is important to be aware of these alterations while interpreting sex steroids in patients on resmetirom" — meaning if you're on this drug and get separate hormone testing for any other reason, share that information with whoever is interpreting the results.
Safety profile:
No statistically significant difference in overall treatment-emergent adverse events between resmetirom and placebo at either dose
No significant difference in serious drug-related adverse events
Diarrhea was significantly more common with resmetirom in the first 12 weeks (occurring in ≥10% of patients; odds ratio 3.25 versus placebo) but the difference faded after 12 weeks
Nausea was elevated at both early and later timepoints (odds ratios 1.98 and 1.85, respectively)
Notably, ALT elevations were actually less common in the resmetirom group than in placebo in this pooled analysis for the moderate (Grade 2) category — a reassuring finding for a drug targeting the liver
Clinical bottom line on resmetirom: this is a real, statistically robust, liver-fat-and-lipid-lowering drug with a manageable GI side-effect profile and no major safety signal in trials to date. It does not meaningfully affect blood sugar. Roughly 1 in 4 to 1 in 3 patients achieve full MASH resolution within a year, which means most patients should expect improvement, not necessarily resolution, and that the drug is best understood as one component of a broader management plan rather than a standalone fix. As the original study authors put it, larger and longer-term trials are still needed to confirm whether these biomarker and imaging improvements ultimately translate into fewer cases of cirrhosis, liver failure, and death — the trial duration to date (up to ~52 weeks for most measures) cannot yet answer that question directly.
Semaglutide (Wegovy) — The Second Approved Option
What it is and how it works
Semaglutide is a GLP-1 receptor agonist — the same class of drug widely known for weight loss and type 2 diabetes treatment, here repurposed (and separately, formally approved) for MASH. Unlike resmetirom's direct liver-targeted mechanism, semaglutide works mostly indirectly: it acts on appetite centers in the brain and improves insulin sensitivity throughout the body, producing substantial weight loss that, in turn, relieves the metabolic burden on the liver. Recent secondary analyses of trial data also suggest some weight-independent benefit, meaning part of its liver effect may not be fully explained by weight loss alone — though weight loss remains the dominant driver.
The actual trial numbers — the ESSENCE trial
The phase 3 ESSENCE trial, published in the New England Journal of Medicine in 2025, randomized 800 patients with biopsy-confirmed MASH and significant (F2–F3) fibrosis to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 72 weeks. This is the trial that supported the August 2025 FDA approval.
Co-primary histologic endpoints at week 72:
Endpoint Semaglutide Placebo Difference MASH resolution without worsening fibrosis 62.9% 34.3% +28.7 points (p<0.001) ≥1-stage fibrosis improvement without worsening MASH 36.8% 22.4% +14.4 points (p<0.001) Both endpoints achieved simultaneously 32.7% 16.1% +16.5 points (p<0.001)
Clinical interpretation: these are larger absolute effect sizes than resmetirom's histologic resolution numbers (62.9% vs. resmetirom's 25.9–29.9%), but the two trials measured somewhat different populations and used different protocols, so a direct head-to-head comparison isn't strictly valid — no trial has pitted the two drugs against each other directly. What is directly comparable is the magnitude of benefit over each drug's own placebo arm, and on that basis semaglutide's improvement over placebo (28.7 points) is larger than resmetirom's reported improvement over placebo in the MAESTRO-NASH data (roughly 16–20 points, depending on dose).
Weight loss, the key driver: mean body weight change was −10.5% with semaglutide versus −2.0% with placebo (p<0.001) by week 72. Critically, the trial's secondary analyses showed a clear dose-response-like relationship between degree of weight loss and degree of liver benefit:
Patients with 2–5% weight loss: 57.1% achieved MASH resolution (vs. 43.1% on placebo)
Patients with >7% weight loss: 71.5% achieved MASH resolution (vs. 56.1% on placebo)
This is the single most clinically useful number in the entire semaglutide data set. It tells a doctor and a patient that the benefit scales with weight loss achieved — and that even modest weight loss (2–5%) produces meaningfully better outcomes than placebo, while substantial weight loss (>7%) pushes resolution rates above 70%. It also reframes a worthwhile conversation: this is not strictly a "liver drug" separate from weight management, but a tool that makes weight loss more achievable and that appears to deliver some liver benefit beyond what weight loss alone would predict.
An important scientific counterpoint, published as a letter to the editor in NEJM following the trial's release: other researchers pointed out that patients who achieve ≥10% weight loss through lifestyle intervention alone (no drug) have historically shown roughly 90% steatohepatitis resolution and nearly 50% fibrosis regression — numbers that, on the surface, look at least as good as semaglutide's. The honest clinical interpretation here is nuanced: it's not that semaglutide underperforms diet and exercise, but that the central practical problem driving semaglutide's value isn't its biological mechanism so much as its ability to help people actually sustain significant weight loss — something diet and exercise alone notoriously fail to sustain for most people over time, trial settings notwithstanding.
Cardiometabolic benefits beyond the liver: semaglutide improved blood pressure, HbA1c, and triglycerides — benefits resmetirom did not show in available data. This matters because, as established earlier, cardiovascular disease is the leading cause of death in MASLD, arguably making semaglutide's broader cardiometabolic profile clinically significant beyond the liver findings alone.
Safety: the trial reported no new safety signals; the profile was consistent with semaglutide's extensive prior safety record from diabetes and obesity trials (most commonly gastrointestinal side effects — nausea, vomiting, diarrhoea — typically most prominent during dose escalation). Nine deaths occurred during the trial (3 semaglutide, 6 placebo) — not concerning given the trial size and patient population, but worth knowing if you encounter the raw numbers elsewhere.
Clinical bottom line on semaglutide: strong histologic results, a clear and reassuring dose-response relationship with weight loss, and meaningful added cardiometabolic benefit make this a compelling option — particularly for patients who are overweight, have type 2 diabetes, or have significant cardiovascular risk factors alongside their liver disease. The tradeoff is a weekly injection rather than a daily pill, and the GI side effects are common to this drug class.
Comparing Your Options: A Clinical Decision Framework
Neither drug is "better" in an absolute sense — they suit different patient profiles, and current expert guidance increasingly discusses combining them rather than choosing one. Here is how the two compare directly:
Resmetirom
Drug Class: THR-β agonist (Thyroid Hormone Receptor-beta agonist).
Administration: Taken orally, once daily.
FDA Approval: Approved in March 2024.
Mechanism of Action: Works via direct liver fat metabolism.
Effect on Body Weight: Minimal effect on weight.
Effect on Blood Sugar: No demonstrated effect on blood glucose levels.
Effect on Blood Pressure: Not a primary effect of the drug.
MASH Resolution vs. Placebo: Shows a +16 to +20 point improvement over placebo.
Approved Indication: Approved for non-cirrhotic MASH with F2–F3 fibrosis.
Best-Suited Patient Profile: Ideal for normal weight or lean MASH patients, or those who prefer to avoid injections.
Common Side Effects: Diarrhea and nausea, particularly early in treatment.
Semaglutide
Drug Class: GLP-1 receptor agonist.
Administration: Subcutaneous injection, given once weekly.
FDA Approval: Approved in August 2025.
Mechanism of Action: Promotes weight loss and improves systemic insulin sensitivity.
Effect on Body Weight: Substantial weight loss, averaging around 10%.
Effect on Blood Sugar: Provides a significant improvement in blood glucose levels.
Effect on Blood Pressure: Demonstrates improved blood pressure levels.
MASH Resolution vs. Placebo: Shows a +28.7 point improvement over placebo.
Approved Indication: Approved for MASH with moderate-to-advanced fibrosis (F2–F3).
Best-Suited Patient Profile: Ideal for patients who are overweight/obese, have type 2 diabetes, or present a higher cardiovascular risk.
Common Side Effects: Nausea and general gastrointestinal (GI) symptoms.
A note on combination therapy: Several 2025–2026 reviews, including the Nature Reviews Drug Discovery therapeutic landscape review, specifically discuss the physiological rationale for combining a GLP-1 receptor agonist with a THR-β agonist — the idea being that a GLP-1 drug provides the metabolic and weight-loss benefit while resmetirom addresses liver fat metabolism directly, potentially compounding the antifibrotic effect through two independent mechanisms. This isn't yet an FDA-approved combination protocol, but it's an active area of clinical interest and ongoing study, and worth asking your doctor about if you have risk factors that overlap both drug profiles.
What's Coming Next: The Drug Pipeline
The two approved drugs are not the end of the story — current research describes a notably crowded late-stage pipeline, organized around several distinct mechanisms:
FGF21 analogs (efruxifermin, pegozafermin, efimosfermin) — these mimic a natural liver hormone with direct antifibrotic effects, and are in large phase 3 trials (SYNCHRONY, ENLIGHTEN-Fibrosis) for both non-cirrhotic and cirrhotic MASH.
Pan-PPAR agonists (lanifibranor) — improved liver histology and cardiometabolic markers (triglycerides, systemic inflammation) in the phase 2b NATIVE trial; common side effects included diarrhea, nausea, peripheral edema, mild anemia, and weight gain.
Dual and triple incretin agonists — survodutide (GLP-1/glucagon dual agonist) showed 34–36% of patients achieving ≥1-stage fibrosis improvement versus 22% on placebo in phase 2 data, though with higher discontinuation rates related to gastrointestinal side effects during dose escalation. Retatrutide, a triple GLP-1/GIP/glucagon agonist, showed strikingly large liver-fat reductions in phase 2a — up to 100% of participants at higher doses achieving ≥30% relative liver fat reduction by 24 weeks, versus roughly 4% on placebo — with a large outcomes trial (SYNERGY-Outcomes) now comparing it against tirzepatide in patients at high risk of liver-related complications.
Fatty acid synthase (FASN) inhibitors (denifanstat) — directly block the liver's own fat-manufacturing machinery (the de novo lipogenesis pathway discussed earlier), an approach distinct from both currently approved drugs.
An important caveat current research is candid about: several previously promising drug candidates — including selonsertib (an ASK1 inhibitor), elafibranor (a PPAR agonist), and cenicriviroc (a CCR antagonist) — were halted in late-stage trials due to insufficient efficacy, despite reasonable biological rationale and encouraging early data. This history is a useful reminder that mechanistic plausibility alone doesn't guarantee clinical success, and it's part of why current guidelines emphasize evidence from completed phase 3 trials rather than mechanism-based optimism.
Lifestyle Management: Still the Foundation
Regardless of where you land on drug therapy, the evidence is unambiguous that lifestyle change remains central, not supplementary.
What the data actually shows about weight loss thresholds:
5% weight loss: improves steatosis (fat content)
7–10% weight loss: the threshold most consistently associated with steatohepatitis resolution
≥10% weight loss: associated with fibrosis regression as well, not just inflammation improvement
Practical, doctor-aligned guidance (general principles; not a substitute for individualized medical or dietary advice):
A gradual approach (0.5–1 kg/week) is generally favored over rapid weight loss, which itself can occasionally worsen liver inflammation in the short term
Reducing dietary fructose and ultra-processed carbohydrate intake specifically targets the de novo lipogenesis pathway discussed earlier — this is a mechanistically targeted recommendation, not a generic "eat less sugar" suggestion
Both aerobic exercise and resistance training have evidence for reducing liver fat independent of weight loss, meaning exercise has value even for someone who isn't losing significant weight
Alcohol: given the MetALD data discussed earlier, even moderate alcohol intake is now understood to meaningfully worsen fibrosis risk in this disease — there is no firmly established "safe" amount once MASLD is present, and this is a conversation worth having directly and specifically with your doctor rather than assuming typical guidelines for the general population apply.
A safety note: if you have, or suspect you might have, disordered eating patterns, rapid or extreme dietary restriction is not the right path to pursue on your own — talk with your doctor about a sustainable, medically supervised approach instead.
Evidence Summary Tables
Resmetirom (THR-β Agonist)
MAESTRO-NAFLD-1 / MAESTRO-NASH (Pooled Meta-Analysis)
Phase: 2 & 3
Cohort Size : 2,234 patients
Key Result: Achieved a liver fat (MRI-PDFF) reduction of up to 36.9 points compared to the placebo group.
MAESTRO-NASH (Individual Trial)
Phase: 3
Cohort Size : 966 patients
Key Result: MASH resolution was achieved in 25.9\% to 29.9\% of patients, significantly outperforming the 9.7\% resolution rate in the placebo group.
Semaglutide (GLP-1 Receptor Agonist)
ESSENCE Trial
Phase: 3 (Interim results)
Cohort Size : 800 patients
Key Result: Achieved a high MASH resolution rate of 62.9%, compared to 34.3%for the placebo group.
Lanifibranor (Pan-PPAR Agonist)
NATIVE Trial
Phase: 2b
Key Result: Demonstrated significant improvements in liver histology (tissue structure) alongside beneficial cardiometabolic markers.
Retatrutide (Triple Hormone Receptor Agonist)
Retatrutide Phase 2a Trial
Phase: 2a
Key Result: Up to 100\% of trial participants achieved a 30\% reduction in liver fat content.
Here is the diagnostic test performance data
FAST Score
What it measures: Combined liver fibrosis (scarring) and disease activity.
Accuracy (AUROC): 0.90
Notes: Highly accurate assessment tool that calculates risk by combining physical elastography data, CAP (controlled attenuation parameter), and AST liver enzyme blood levels.
MRI-PDFF (Magnetic Resonance Imaging Proton Density Fat Fraction)
What it measures: Precise liver fat content.
Accuracy (AUROC): ~0.90 (specifically for moderate-to-severe, or Grade 2, steatosis).
Notes: Widely considered the non-invasive gold standard for quantifying liver fat, though its widespread clinical use is limited by high equipment costs and machine availability.
VCTE / FibroScan (Vibration-Controlled Transient Elastography)
What it measures: Liver stiffness to determine the severity of fibrosis.
Accuracy (AUROC): Ranging from 0.83 (for moderate, or F2 fibrosis) up to 0.89 (for advanced cirrhosis, or F4).
Notes: A highly popular, FDA-accepted alternative to invasive physical liver biopsies frequently utilized in modern clinical trials.
M2BPGi (Mac-2 Binding Protein Glycan Isomer)
What it measures: Fibrosis severity.
Accuracy (AUROC): Up to 0.87 (specifically for diagnosing advanced cirrhosis).
Notes: A specialized serum biomarker that is heavily utilized and clinically validated across Japanese medical networks.
FIB-4 Index (Fibrosis-4)
What it measures: Initial estimation of fibrosis risk.
Accuracy (AUROC): 0.65 – 0.76
Notes: Standard, frontline screening tool used to rule out advanced disease. It costs nothing extra to calculate because it relies entirely on routine, standard blood panels (age, AST, ALT, and platelets).
Common Myths and Mistakes
Myth: "If my ultrasound shows less fat than last time, my liver is improving." Not necessarily. As discussed above, fibrosis stage — not fat percentage — drives long-term risk, and "burned-out" MASLD can show reduced fat alongside worsening scarring. Ask specifically about your fibrosis markers, not just your steatosis grade.
Myth: "I'm not overweight, so I don't need to worry about this." Lean MASLD is real and, in some studies, carries a worse histologic profile and higher mortality risk than non-lean MASLD, partly because it's diagnosed later — clinicians and patients alike are less likely to suspect it. If you have any cardiometabolic risk factor (even just mildly elevated triglycerides or blood pressure) regardless of body weight, ask about screening.
Myth: "A little wine or beer is fine since I don't drink heavily." The MetALD data above directly contradicts this for anyone who already has MASLD risk factors — even alcohol intake below traditional "heavy drinking" thresholds is independently associated with increased fibrosis progression in this specific population.
Myth: "Resmetirom or semaglutide will fix the problem on their own." Both drugs were tested and approved as adjuncts to lifestyle management, not replacements for it, and neither achieves resolution in the majority of patients within a year. Drug therapy improves your odds; it does not guarantee an outcome.
Mistake: assuming a liver biopsy is always required for diagnosis. Current Japanese and international guidelines explicitly state biopsy is not routinely required — the non-invasive stepwise pathway described above is now standard first-line practice in most cases.
Mistake: ignoring cardiovascular risk because "it's a liver problem." As covered extensively above, cardiovascular disease — not liver failure — is the leading cause of death for most people with this diagnosis who haven't progressed to cirrhosis. A MASLD diagnosis should prompt a cardiovascular risk conversation, not just liver monitoring.
Frequently Asked Questions
Is MASLD the same thing as NAFLD? Functionally, yes, for the vast majority of patients — the diagnostic criteria were designed to capture essentially the same population, and clinical evidence built up under the NAFLD/NASH names remains directly applicable. The name changed in 2023 to better reflect the disease's metabolic origins and reduce stigma; your underlying disease did not change.
Can MASLD be reversed? Early-stage disease (minimal fibrosis) is often reversible through sustained weight loss and metabolic improvement. Advanced fibrosis and cirrhosis are much harder to reverse, though even cirrhosis can sometimes show improvement with sufficiently aggressive metabolic treatment — this is an area of active research, and individual outcomes vary substantially.
Do I need a liver biopsy to be diagnosed? Usually not. Current guidelines recommend a stepwise non-invasive approach (FIB-4, then elastography or blood-based markers) and reserve biopsy for cases where results are unclear or a specific treatment decision requires histologic confirmation.
What's the difference between MASLD and MASH? MASLD is the umbrella term for fatty liver with metabolic risk factors. MASH is the more severe subtype involving active inflammation and a specific type of cell damage (hepatocyte ballooning), and it's the stage most likely to progress to scarring.
Is resmetirom or semaglutide "better"? Neither is universally better — they suit different patient profiles. Resmetirom may suit people closer to normal weight who prefer an oral medication and don't have major glycemic or cardiovascular concerns. Semaglutide may suit people who are overweight, have type 2 diabetes, or have elevated cardiovascular risk, given its added metabolic and cardiometabolic benefits. This decision should be made with your doctor based on your specific risk profile, fibrosis stage, and other health conditions.
Will losing weight on my own work as well as the drugs? The data suggests sustained weight loss of ≥10% through lifestyle change alone can produce results comparable to or exceeding either drug's average effect. The practical challenge, well documented in the research, is that sustaining that level of weight loss long-term is difficult for most people without ongoing support — which is part of why drug therapy has a role even though lifestyle change theoretically "works as well."
Does MASLD cause symptoms? Often none, especially in earlier stages — which is exactly why screening based on risk factors (rather than waiting for symptoms) is now the recommended approach. By the time symptoms like fatigue or abdominal discomfort appear, disease may already be more advanced.
Can children get MASLD? Yes. Global pediatric prevalence is estimated at around 13%, and rates have been rising alongside childhood obesity trends.
Is fasting insulin or HbA1c testing part of MASLD screening? These aren't part of the core MASLD diagnostic criteria, but since type 2 diabetes and insulin resistance are closely linked to MASLD risk and progression, many doctors check them as part of a broader cardiometabolic risk assessment.
Should I be tested for the PNPLA3 gene variant? This isn't yet part of routine standard-of-care screening for most patients, though it's increasingly discussed in research as a way to identify people at meaningfully higher risk, particularly those with a strong family history or lean MASLD. Ask your doctor whether it's relevant given your specific situation.
If my liver enzymes (ALT/AST) are normal, can I still have MASLD or even MASH? Yes — this is an important and underappreciated point. Liver enzymes can be normal even with significant fibrosis present, which is part of why doctors increasingly rely on FIB-4 and other composite scores rather than liver enzymes alone.
Conclusion and Action Steps
MASLD has moved, in a very short window, from a condition with no approved drug treatment to one with two distinct, evidence-backed pharmacological options, a far more sophisticated and less invasive diagnostic pathway, and a genuinely crowded pipeline of additional therapies in late-stage trials. That's a meaningfully different landscape than existed even three years ago, and it's worth your doctor — and you — being current on it.
If you're working through this with a doctor, useful next steps include:
Ask for your FIB-4 score, calculated from bloodwork you may already have. This single number is the recommended starting point in essentially every current guideline.
Ask specifically about your fibrosis stage, not just whether you have "fatty liver" — fibrosis stage, not fat percentage, is what drives your actual long-term risk.
Bring up cardiovascular risk explicitly — it's the leading cause of death in this disease until cirrhosis develops, and it's easy for liver-focused visits to overlook it.
If lifestyle change hasn't achieved sustained results, ask whether resmetirom or semaglutide fits your specific risk profile — weight, diabetes status, and cardiovascular risk factors should all inform that conversation.
If you have a first-degree relative with MASLD or cirrhosis, mention it — family history materially changes your own risk calculation.
Reassess alcohol intake honestly, even if it's modest — the data on MetALD suggests there may be no fully "safe" threshold once metabolic risk factors are present.
This article is for educational purposes and reflects the published research available as of mid-2026. It is not a substitute for personalized medical advice. If you have concerns about your liver health, talk with your doctor or a gastroenterologist/hepatologist about testing and treatment options specific to your situation.
Related Articles
Why Your Scale Isn’t Moving: The Science of Fat Burning Beyond Weight Loss | DR T S DIDWAL
How Glycemic Index and Glycemic Load Influence Type 2 Diabetes | DR T S DIDWAL
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
Sources and References
He Y, Chen Y, Qian S, et al. Immunopathogenic mechanisms and immunoregulatory therapies in MASLD. Cell Mol Immunol. 2025;22:1159-1177. doi:10.1038/s41423-025-01307-5
Suvarna R, Shetty S, Pappachan JM. Efficacy and safety of Resmetirom, a selective thyroid hormone receptor-β agonist, in the treatment of metabolic dysfunction-associated steatotic liver disease (MASLD): a systematic review and meta-analysis. Sci Rep. 2024;14:19790. doi:10.1038/s41598-024-70242-8
Tantu MT, Farhana FZ, Haque F, et al. Pathophysiology, noninvasive diagnostics and emerging personalized treatments for metabolic associated liver diseases. npj Gut Liver. 2025;2:18. doi:10.1038/s44355-025-00030-2
Do A, Zahrawi F, Mehal WZ. Therapeutic landscape of metabolic dysfunction-associated steatohepatitis (MASH). Nat Rev Drug Discov. 2025;24:171-189. doi:10.1038/s41573-024-01084-2
Ren R, Liang X, Wei X. Metabolic dysfunction-associated steatotic liver disease: pathogenesis and novel treatment options. Mol Biomed. 2026;7:80. doi:10.1186/s43556-026-00486-5
Seko Y, Yamaguchi K. Management of MASLD/MASH: challenges, innovations, and the future of patient-centered care in Japan. J Gastroenterol. 2026;61:880-908. doi:10.1007/s00535-026-02401-9
Akuta N, Kogiso T, Ikejima K, et al. Evidence-based clinical practice guidelines for metabolic dysfunction-associated steatotic liver disease (MASLD) 2026. J Gastroenterol. 2026;61:693-710. doi:10.1007/s00535-026-02408-2
Sanyal AJ, Newsome PN, Kliers I, et al.; ESSENCE Study Group. Phase 3 trial of semaglutide in metabolic dysfunction-associated steatohepatitis. N Engl J Med. 2025;392:2089-2099. doi:10.1056/NEJMoa2413258
Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77:1335-1347.
Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79:1542-1556.
Harrison SA, Bedossa P, Guy CD, et al. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390:497-509. doi:10.1056/NEJMoa2309000
Le P, Payne JY, Zhang L, et al. Disease state transition probabilities across the spectrum of NAFLD: a systematic review and meta-analysis of paired biopsy or imaging studies. Clin Gastroenterol Hepatol. 2023;21:1154-1168.
Mantovani A, Csermely A, Petracca G, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6:903-913.
Quek J, Chan KE, Wong ZY, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8:20-30.
Younossi ZM, Kalligeros M, Henry L. Epidemiology of metabolic dysfunction-associated steatotic liver disease. Clin Mol Hepatol. 2025;31:S32-50.
Fujii H, Iwaki M, Hayashi H, et al. Clinical outcomes in biopsy-proven nonalcoholic fatty liver disease patients: a multicenter registry-based cohort study. Clin Gastroenterol Hepatol. 2023;21:370-379.
Tamaki N, Kimura T, Wakabayashi SI, et al. Long-term clinical outcomes in steatotic liver disease and incidence of liver-related events, cardiovascular events and all-cause mortality. Aliment Pharmacol Ther. 2024;60:61-69.
Stine JG, et al. Change in MRI-PDFF and histologic response in patients with non-alcoholic steatohepatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2021;19:2274-2283.
Ito T, Ishigami M, Zou B, et al. The epidemiology of NAFLD and lean NAFLD in Japan: a meta-analysis with individual and forecasting analysis, 1995-2040. Hepatol Int. 2021;15:366-379.
EASL-EASD-EASO. Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. 2024;81:492-542.
Vilar-Gomez E, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology. 2015;149:367-378.
Newsome PN, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med. 2021;384:1113-1124.
Gawrieh S, et al. Saroglitazar, a PPAR-α/γ agonist, for treatment of NAFLD: a randomized controlled double-blind phase 2 trial. Hepatology. 2021;74:1809-1824.
Sookoian S, Rotman Y, Valenti L. Genetics of metabolic dysfunction-associated steatotic liver disease: the state of the art update. Clin Gastroenterol Hepatol. 2024;22:2177-2187.
A note on sourcing: this article draws primarily on seven peer-reviewed sources listed at the top of the reference list (1–7), supplemented with directly cited primary trial data (the ESSENCE and MAESTRO-NASH trials) and supporting epidemiological literature referenced within those reviews. Specific statistics are attributed inline; readers seeking primary source verification should consult the DOIs above.