The Cardiometabolic Connection: Why Metabolism Is Now Central to Heart Disease and Diabetes
Latest cardiometabolic research reveals how heart disease, diabetes, obesity, and metabolism are linked. Understand risk factors, insulin resistance, inflammation, and new treatment strategies.
METABOLISMHEART
Dr. T.S. Didwal, M.D.(Internal Medicine)
5/25/202625 min read
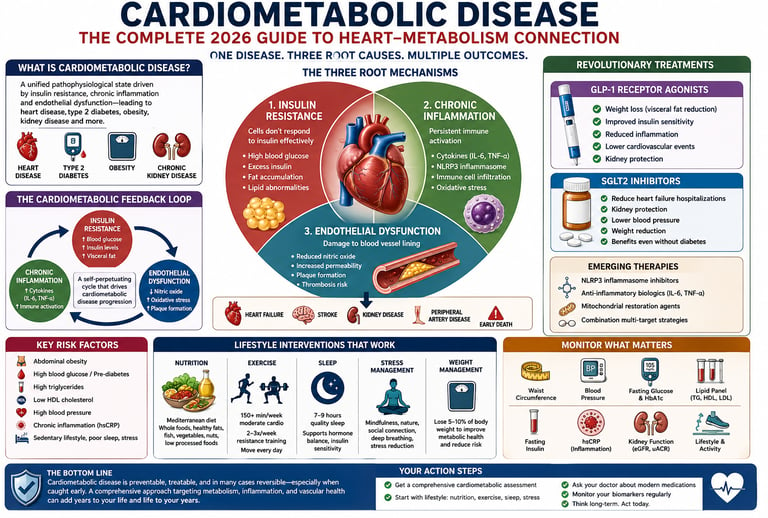
Cardiometabolic disease is a unified disorder linking heart disease, insulin resistance, obesity, type 2 diabetes, and chronic inflammation. It develops when metabolic dysfunction damages blood vessels, mitochondria, and cardiovascular health simultaneously. Modern treatment combines lifestyle medicine, GLP-1 therapies, SGLT2 inhibitors, and early risk detection to prevent heart attacks, stroke, and metabolic decline.
Your heart and your metabolism are not two separate systems — they are one deeply connected network, and when that network breaks down, the consequences are severe.
Cardiometabolic disease — the convergence of cardiovascular disease, type 2 diabetes, obesity, and metabolic dysfunction — has become the defining health crisis of the 21st century. Researchers now warn that this is no longer a matter of individual conditions coincidentally overlapping. It is a unified, self-amplifying biological process driven by three core mechanisms: insulin resistance, chronic inflammation, and endothelial dysfunction.
What makes this especially urgent is the scale. As of 2025–2026, cardiometabolic diseases collectively represent the leading cause of mortality worldwide, surpassing all other causes of death (American College of Cardiology, 2025). And the risk begins long before a formal diagnosis — even mild insulin resistance or excess visceral fat substantially raises your chances of heart failure, stroke, and kidney disease (Kim, 2025).
The good news? The science of cardiometabolic medicine has never advanced faster. Breakthrough drug classes, AI-powered risk tools, and precision lifestyle interventions are giving clinicians and patients more power than ever to change course — especially when acting early.
In this guide, you will learn:
What cardiometabolic disease really is, and how it differs from simply having two conditions at once
The three root mechanisms driving disease progression
What the latest 2025–2026 research reveals about risk, treatment, and prevention
Which medications (GLP-1s, SGLT2 inhibitors) are reshaping outcomes
Practical, evidence-based steps you can take today
Clinical Pearls for Cardiometabolic Disease :
1. Think "Cardiometabolic Continuum," Not Separate Diseases
Cardiovascular disease and type 2 diabetes are not coincidental — they share the same core drivers (insulin resistance, chronic inflammation, and endothelial dysfunction). Treat them as one interconnected syndrome. Patients with pre-diabetes or visceral obesity already have elevated heart failure and CKD risk even before a formal diabetes diagnosis.
2. Look Beyond HbA1c — Measure Fasting Insulin and hsCRP Early
Normal fasting glucose or HbA1c does not rule out significant risk. Check fasting insulin (to detect insulin resistance) and high-sensitivity CRP (hsCRP >2 mg/L) in at-risk patients. These often reveal hidden cardiometabolic risk years before classic markers become abnormal.
3. Prioritize Visceral Fat Over Total Body Weight
Waist circumference (>40 inches men, >35 inches for women) is more clinically useful than BMI. "TOFI" patients (Thin Outside, Fat Inside) can have high cardiometabolic risk despite being of normal weight. Focus on reducing visceral adiposity through Zone 2 exercise, time-restricted eating, and the Mediterranean diet.
4. Use Multi-Target Therapies Aggressively (GLP-1s & SGLT2i)
GLP-1 receptor agonists (especially tirzepatide) and SGLT2 inhibitors are true cardiometabolic drugs. Their benefits on MACE, heart failure, and kidney outcomes are often independent of glucose-lowering. Consider them early in patients with obesity, diabetes, heart failure, or CKD — they hit multiple mechanisms simultaneously.
5. Zone 2 Exercise is the MVP of Lifestyle Interventions
Prescribe 150–200+ minutes/week of Zone 2 cardio (can speak in full sentences, ~60-70% max HR). It improves mitochondrial function, insulin sensitivity, fatty acid oxidation, and reduces inflammation more effectively than high-intensity training alone for most patients. Combine with resistance training 2–3x/week.
6. Sleep and Inflammation Are Non-Negotiable Therapeutic Targets
Chronic short sleep (<7 hours) or untreated OSA rapidly worsens insulin resistance and inflammation. Treat sleep as a core cardiometabolic intervention, equivalent in importance to diet and exercise. Also address chronic stress — both drive visceral fat and endothelial dysfunction via cortisol and sympathetic overdrive.
Bonus Pearl: The best outcomes occur with early, integrated care — addressing all three root mechanisms (insulin resistance, inflammation, endothelial dysfunction) together rather than treating individual risk factors in silos.
What Is Cardiometabolic Disease?
Cardiometabolic disease is not simply a matter of having heart disease and diabetes at the same time. It describes a unified pathophysiological state in which cardiovascular dysfunction and metabolic disorders emerge from, and reinforce, the same underlying biological processes.
Think of it this way: if you have two separate house fires in two separate rooms, you can fight each one independently. But if both fires share the same wall and the same fuel source, fighting them separately is far less effective — and much more dangerous.
That shared "fuel source" in cardiometabolic disease includes:
Insulin resistance — cells stop responding to insulin properly, causing elevated blood glucose, compensatory hyperinsulinemia, and fat accumulation in organs
Chronic low-grade inflammation — a persistent immune activation that damages blood vessel walls and promotes plaque formation
Endothelial dysfunction — the lining of blood vessels loses its protective properties, allowing fatty deposits to accumulate and increasing clotting risk
These three mechanisms form a reinforcing feedback loop: insulin resistance promotes inflammation, inflammation worsens endothelial function, and endothelial dysfunction accelerates insulin resistance further (Eroglu, Capone, & Schiattarella, 2024).
Cardiometabolic Syndrome vs. Metabolic Syndrome: What's the Difference?
Metabolic syndrome is a specific clinical diagnosis requiring the presence of three or more of five criteria: abdominal obesity, high triglycerides, low HDL cholesterol, elevated blood pressure, and elevated fasting glucose.
Cardiometabolic syndrome is a broader, more modern concept. It acknowledges that even individuals who don't meet the formal metabolic syndrome criteria may already be experiencing the biological cascade that leads to heart disease, kidney failure, and type 2 diabetes. The distinction matters because it shifts focus from a diagnostic checklist to a continuum of risk.
The Three Root Mechanisms
1. Insulin Resistance: The Starting Point
Insulin resistance is arguably the most upstream driver of cardiometabolic disease. When muscle, fat, and liver cells stop responding to insulin efficiently, the pancreas compensates by producing more — leading to chronically elevated insulin levels (hyperinsulinemia).
This has cascading consequences:
Elevated blood glucose damages blood vessel walls directly through a process called glycation
Excess insulin promotes sodium retention, raising blood pressure
Hyperinsulinemia drives fat storage — particularly visceral (abdominal) fat, which is metabolically active and pro-inflammatory
Lipid dysregulation follows, raising small dense LDL particles and triglycerides while dropping protective HDL
According to a 2025 analysis in the CardioMetabolic Syndrome Journal, patients with even pre-diabetic levels of insulin resistance face significantly elevated risks for heart failure and chronic kidney disease — well before diabetes is formally diagnosed (Kim, 2025).
2. Chronic Inflammation: The "Invisible Fire"
Once visceral fat accumulates and insulin resistance takes hold, the body's immune system enters a state of low-grade, chronic activation. This is not the acute inflammation you feel from a cut or infection — it's a sustained, smoldering immune response that silently damages tissues over years.
Key inflammatory players include:
Cytokines (IL-6, TNF-alpha) that circulate in the bloodstream and damage arterial walls
The NLRP3 inflammasome — a molecular switch that, when chronically activated, accelerates both arterial plaque formation and insulin resistance simultaneously
Immune cell infiltration in fat tissue and arterial walls, accelerating atherosclerosis
A landmark 2024 review in EBioMedicine demonstrated that these inflammatory pathways are not merely associated with cardiometabolic disease — they are mechanistically central to its progression (Eroglu et al., 2024). Crucially, a 2026 European Heart Journal scientific statement identified novel cardiovascular metabolic risk factor mechanisms, including inflammatory signaling pathways as key therapeutic targets (Evans et al., 2026).
3. Endothelial Dysfunction: Where the Damage Is Done
The endothelium — a single-cell-thick layer lining every blood vessel in your body — is far more than a passive barrier. It regulates blood flow, prevents clotting, controls inflammation, and responds dynamically to metabolic signals.
In cardiometabolic disease, chronic insulin resistance and inflammation impair endothelial function in ways that:
Reduce nitric oxide production (a key vasodilator), raising blood pressure
Increase adhesion molecule expression, helping inflammatory cells and lipids stick to vessel walls
Accelerate atherosclerotic plaque formation and increase plaque vulnerability to rupture
Endothelial dysfunction is now considered the critical intersection point where metabolic disturbance converts into structural cardiovascular disease (Eroglu et al., 2024).
How Heart Disease and Diabetes Are Biologically Linked
For decades, cardiology and endocrinology treated these as parallel problems. The new science is unambiguous: they are the same problem viewed from different angles.
Here is how the biology connects:
Insulin Resistance
Effect on Metabolism: Causes elevated blood glucose levels and dyslipidemia (unhealthy blood lipid and cholesterol profiles).
Effect on Heart & Vessels: Directly triggers endothelial damage (harm to the blood vessel lining) and accelerates structural plaque formation.
Visceral Adiposity (Excess Deep Belly Fat)
Effect on Metabolism: Drives severe adipokine dysregulation and systemic, low-grade metabolic inflammation.
Effect on Heart & Vessels: Increases structural arterial stiffness, reducing the elasticity of the blood vessels.
Hyperinsulinemia (Chronically High Insulin Levels)
Effect on Metabolism: Constantly signals the body to store fat and down-regulates fat oxidation (burning).
Effect on Heart & Vessels: Forces sodium retention in the kidneys, directly contributing to chronic hypertension (high blood pressure).
Chronic Inflammation
Effect on Metabolism: Weakens and damages pancreatic beta-cells, progressively destroying your ability to produce insulin.
Effect on Heart & Vessels: Destabilizes arterial walls, leading directly to plaque rupture and localized thrombosis (blood clots).
Mitochondrial Dysfunction
Effect on Metabolism: Impairs your cells' ability to oxidize glucose efficiently, causing severe metabolic inflexibility.
Effect on Heart & Vessels: Significantly reduces cardiac energy efficiency, starving the heart muscle of the cellular fuel it needs to pump.
Oxidative Stress (Excess Cellular Free Radicals)
Effect on Metabolism: Floods cellular signaling pathways, which further promotes and reinforces systemic insulin resistance.
Effect on Heart & Vessels: Damages cellular walls and aggressively accelerates vascular aging.
A 2026 scoping review in the Journal of Diabetes & Metabolic Disorders confirmed that managing metabolic risks in coronary artery disease requires an integrated approach — treating these mechanisms simultaneously yields substantially better outcomes than sequential, organ-specific management (Gudla et al., 2026).
Who Is at Risk? Key Risk Factors Explained
Cardiometabolic risk is not binary — it exists on a spectrum. The following risk factors compound one another, and their combination is far more dangerous than any single factor alone.
Primary Metabolic Risk Factors
Abdominal obesity (waist circumference >40 inches in men, >35 inches in women)
Elevated fasting glucose (≥100 mg/dL) or pre-diabetes (HbA1c 5.7–6.4%)
Hypertriglyceridemia (≥150 mg/dL)
Low HDL cholesterol (<40 mg/dL in men, <50 mg/dL in women)
Elevated blood pressure (≥130/85 mmHg)
Emerging and Underappreciated Risk Factors
Elevated high-sensitivity CRP (hsCRP) — a marker of vascular inflammation; levels >2 mg/L indicate significantly elevated cardiovascular risk even with normal cholesterol
Sleep-disordered breathing (obstructive sleep apnea) directly promotes insulin resistance and sympathetic nervous system activation
Sedentary behavior, independent of exercise habits, prolonged sitting impairs insulin sensitivity and endothelial function
Chronic psychological stress — activates the HPA axis, elevating cortisol, promoting visceral fat deposition, and worsening inflammation
Gut microbiome dysbiosis — emerging evidence links reduced microbial diversity to both metabolic dysfunction and cardiovascular risk
Socioeconomic and environmental factors — food insecurity, air pollution, and neighborhood walkability independently affect cardiometabolic risk
The "Pre-Disease" Window: Why It Matters
One of the most important shifts in cardiometabolic medicine is the recognition that significant biological damage occurs long before diagnostic thresholds are crossed. According to research published in 2025, individuals with subclinical insulin resistance — no diabetes diagnosis, normal fasting glucose — already show measurable endothelial dysfunction and early atherosclerosis (Kim, 2025).
This means the best time to intervene is before symptoms appear.
2025–2026 Breakthrough Research
The past two years have produced a remarkable convergence of findings that are reshaping clinical practice.
The ACC's Transformative CV Trends Report (2025)
The American College of Cardiology's landmark 2025 analysis identified several paradigm shifts in cardiovascular medicine, including the emergence of real-time, AI-driven risk stratification that allows treatment to be adjusted continuously — not just at annual checkups. The ACC emphasized that precision medicine approaches and multidisciplinary care models combining cardiology with endocrinology consistently outperform traditional siloed care (American College of Cardiology, 2025).
Nature Metabolism: Shaping Cardiometabolic Innovation (2025)
A collaborative paper in Nature Metabolism outlined the research agenda for the next decade in cardiometabolic medicine. The authors identified three priority areas: mechanistic understanding of the molecular drivers of disease, personalized medicine using genetic and biomarker profiling, and technology-enabled care (including wearable sensors and AI risk tools) (Clemmensen et al., 2025).
ESC Scientific Statement on Cardiovascular Metabolic Risk (2026)
A major 2026 scientific statement from the European Society of Cardiology — co-authored by experts across the ESC Council on Basic Cardiovascular Science and four ESC Working Groups — identified novel cardiovascular metabolic risk factor mechanisms and highlighted new therapeutic opportunities at the intersection of metabolism and vascular biology (Evans et al., 2026). This authoritative statement reinforces the field's shift toward integrated cardiometabolic management.
Frontiers in Cardiovascular Medicine (2026)
New 2026 research published in Frontiers in Cardiovascular Medicine is further delineating how metabolic dysregulation drives structural cardiac remodeling — including changes in cardiac fibrosis, left ventricular function, and myocardial energetics — providing new targets for intervention before overt heart failure develops.
Biomedicines: Third Edition of Cardiovascular and Metabolic Disease Review (2025)
A comprehensive 2025 third-edition review in Biomedicines synthesized current evidence on treatment strategies and future directions in cardiovascular and metabolic disease management, highlighting the growing body of evidence supporting early, multi-targeted pharmacological intervention (Caturano, 2025).
Revolutionary Treatments: GLP-1s, SGLT2 Inhibitors & Beyond
Perhaps the most exciting development in cardiometabolic medicine is the emergence of drug classes that simultaneously address multiple pathological mechanisms — moving medicine firmly into the era of multi-target therapy.
GLP-1 Receptor Agonists (e.g., semaglutide, tirzepatide)
Primary Mechanism: Act as incretin mimetics to suppress appetite, delay gastric emptying, and enhance glucose-dependent insulin secretion.
Cardiovascular Benefit: ✅ High (Strongly protects against major adverse cardiovascular events like stroke and heart attack).
Metabolic Benefit: High✅ (Drives profound weight loss, lowers HbA1c, and reduces visceral adiposity).
Kidney Benefit: Moderate ✅(Provides notable secondary renal protection by decreasing inflammation and oxidative stress).
SGLT2 Inhibitors (e.g., empagliflozin, dapagliflozin)
Primary Mechanism: Block sodium-glucose cotransporter 2 in the proximal tubules of the kidneys to promote urinary glucose and sodium excretion.
Cardiovascular Benefit: ✅ High (Drastically reduces heart failure hospitalizations and cardiovascular mortality).
Metabolic Benefit: ✅ Moderate (Aids in blood sugar control, mild caloric loss, and modest blood pressure reductions).
Kidney Benefit: ✅ High (Provides powerful renal protection, slows the progression of chronic kidney disease, and reduces macroalbuminuria).
NLRP3 Inflammasome Inhibitors (Emerging Therapeutics)
Primary Mechanism: Selectively block the NLRP3 inflammasome assembly to stop the chronic, low-grade systemic inflammation that drives metabolic decay.
Cardiovascular Benefit: 🔬 Promising (Early human trials show intense potential for mitigating atherosclerotic plaque instability).
Metabolic Benefit: 🔬 Promising (Aims to reverse tissue-specific insulin resistance by quenching chronic baseline inflammation).
Kidney Benefit: 🔬 Early Data (Preclinical models indicate a significant reduction in inflammatory renal fibrosis).
Mitochondrial Targeting Agents (Emerging Therapeutics)
Primary Mechanism: Optimize cellular energy metabolism, reduce reactive oxygen species (ROS), and repair age-related mitochondrial decay.
Cardiovascular Benefit: 🔬 Promising (Shows potential for preserving myocardial tissue and improving cardiac pumping efficiency).
Metabolic Benefit: 🔬 Promising (Aims to directly restore metabolic flexibility and cellular energy expenditure).
Kidney Benefit: — Data currently limited or not yet established.
Statins (e.g., atorvastatin, rosuvastatin)
Primary Mechanism: Inhibit the HMG-CoA reductase enzyme to aggressively decrease LDL cholesterol synthesis, while providing pleiotropic (anti-inflammatory and plaque-stabilising) effects.
Cardiovascular Benefit: ✅ Established (The undisputed clinical gold standard for primary and secondary cardiovascular event prevention).
Metabolic Benefit: ✅ Some Benefit (Slightly neutral-to-complex blood sugar profile, but offers essential systemic vascular protection).
Kidney Benefit: ✅ Some Benefit (Provides secondary endothelial and vascular tracking benefits to the kidneys over time).
The Role of Inflammation in Cardiometabolic Disease
Inflammation is no longer considered a side effect of cardiometabolic disease — it is recognized as a primary driver of disease progression.
How Inflammation Links Metabolism to Atherosclerosis
When visceral fat accumulates, adipose tissue stops functioning normally. Instead of acting as a healthy energy reservoir, it becomes an active pro-inflammatory organ — secreting cytokines like TNF-alpha and IL-6 into the bloodstream, recruiting immune cells (particularly macrophages), and promoting a state of chronic systemic inflammation.
These circulating inflammatory signals:
Damage endothelial cells, increasing permeability and adhesion molecule expression
Oxidize LDL cholesterol, converting it into the far more dangerous oxidized LDL that initiates plaque formation
Activate smooth muscle cells within arterial walls, contributing to plaque buildup and arterial stiffening
Destabilize existing plaques, increasing the risk of rupture and acute myocardial infarction
The NLRP3 inflammasome deserves special mention. This intracellular molecular complex acts as a master switch for sterile inflammation. In cardiometabolic disease, it is chronically activated by metabolic signals including saturated fatty acids, uric acid crystals, and glucose — triggering the release of IL-1beta and IL-18, potent cytokines that accelerate atherosclerosis and worsen insulin resistance simultaneously.
Measuring Inflammation: Clinical Tools
High-sensitivity CRP (hsCRP): The most widely used clinical marker. Values >2 mg/L indicate elevated cardiovascular risk. The JUPITER trial showed that statin therapy reduced cardiovascular events even in people with normal LDL but elevated hsCRP.
IL-6: A more direct upstream marker, increasingly available in advanced metabolic testing
Fibrinogen and Lp-PLA2: Additional inflammatory biomarkers gaining clinical relevance
Lifestyle Anti-Inflammatory Strategies
Before reaching for medications, several lifestyle practices have powerful, evidence-based anti-inflammatory effects:
Mediterranean diet: Rich in polyphenols, omega-3 fatty acids, and fiber — consistently shown to reduce CRP, IL-6, and cardiovascular events
Regular aerobic exercise: Even 150 minutes per week of moderate exercise significantly reduces circulating inflammatory markers
Quality sleep (7–9 hours): Sleep deprivation activates the same inflammatory pathways as metabolic disease
Stress reduction: Chronic psychological stress maintains cortisol elevation, promoting visceral fat and inflammation
Mitochondrial Dysfunction: The Hidden Driver
Your heart beats approximately 100,000 times per day. This requires an extraordinary, continuous supply of ATP — the cellular energy currency. That energy comes almost entirely from mitochondria, the organelles that convert nutrients into usable fuel.
In cardiometabolic disease, mitochondria in both heart muscle cells (cardiomyocytes) and metabolic tissues become progressively dysfunctional. This has profound consequences:
Reduced ATP production: The heart literally runs low on fuel, impairing contractile function
Increased reactive oxygen species (ROS): Dysfunctional mitochondria produce excessive free radicals that damage cell membranes, proteins, and DNA
Impaired fatty acid oxidation: The heart normally derives 60–70% of its energy from fat; in cardiometabolic disease, this metabolic flexibility is lost
Promotion of insulin resistance: Accumulated lipid metabolites in muscle interfere with insulin signaling
Multiple 2025–2026 studies highlight mitochondrial dysfunction as both a consequence and an amplifier of cardiometabolic disease — creating another self-perpetuating feedback loop (Eroglu et al., 2024; Ren et al., 2025).
How to Support Mitochondrial Health
Zone 2 Exercise is currently the strongest evidence-based intervention for improving mitochondrial function. Zone 2 refers to moderate-intensity cardio where you can hold a conversation — roughly 60–70% of maximum heart rate. At this intensity:
Mitochondrial biogenesis is stimulated (you grow more and better mitochondria)
Fatty acid oxidation capacity improves
Insulin sensitivity in muscle increases dramatically
Aim for 3–5 hours of Zone 2 exercise per week for meaningful cardiometabolic benefit.
Other mitochondria-supportive strategies include:
Resistance training: Builds metabolically active muscle mass, improving glucose disposal
Adequate dietary protein: Supports mitochondrial enzyme synthesis
Avoiding prolonged caloric excess: Mitochondrial overload accelerates dysfunction
Emerging supplements (coenzyme Q10, NAD+ precursors like NR/NMN): Early evidence for modest benefit; consult your physician
Skeletal Muscle: The Missing Link in Cardiometabolic Health
Skeletal muscle is the body’s largest glucose-disposal organ, responsible for clearing nearly 70–80% of glucose after meals under insulin-stimulated conditions. This means that muscle health is not just about strength or mobility — it is central to metabolic health, insulin sensitivity, and cardiovascular protection.
Sarcopenia and Cardiometabolic Disease
With aging, physical inactivity, chronic inflammation, and poor nutrition, many individuals gradually lose skeletal muscle mass and function — a condition known as sarcopenia. This age-related decline in muscle reduces the body’s capacity to absorb and utilize glucose efficiently, worsening insulin resistance and increasing the risk of type 2 diabetes, obesity, and cardiovascular disease.
Importantly, sarcopenia and visceral obesity often coexist in a dangerous combination termed sarcopenic obesity, which is strongly associated with:
higher inflammatory burden
impaired mitochondrial function
frailty
endothelial dysfunction
elevated cardiovascular mortality risk
Muscle Insulin Sensitivity: Why Muscle Matters
Healthy skeletal muscle acts like a metabolic “glucose sink.” During and after exercise, muscle cells increase glucose uptake through insulin-dependent and insulin-independent pathways, particularly via GLUT4 transporter activation.
When muscle becomes insulin resistant:
glucose remains elevated in the bloodstream
The pancreas compensates with hyperinsulinemia
visceral fat accumulation accelerates
Inflammatory signalling increases
cardiometabolic risk rises substantially
This is one reason physically active individuals often maintain better metabolic health even at similar body weights.
Resistance Training Physiology
Resistance training is one of the most powerful non-pharmacological interventions for cardiometabolic disease because it directly targets skeletal muscle biology.
Regular resistance exercise:
increases lean muscle mass
improves GLUT4-mediated glucose uptake
enhances mitochondrial density and metabolic flexibility
lowers visceral fat
improves resting metabolic rate
reduces inflammatory cytokines
enhances insulin sensitivity independently of weight loss
Even 2–3 sessions per week can significantly improve glycemic control and reduce cardiometabolic risk markers.
Aging-Related Metabolic Decline
Beginning around age 30–40, adults gradually lose muscle mass and strength unless resistance training and adequate protein intake are maintained. This contributes to:
reduced metabolic rate
impaired glucose disposal
increased fat accumulation
declining mitochondrial efficiency
worsening insulin resistance
This age-associated metabolic decline helps explain why cardiometabolic disease risk rises sharply with aging.
Modern cardiometabolic medicine increasingly recognizes that preserving skeletal muscle is not merely a fitness goal — it is a critical strategy for preventing diabetes, frailty, cardiovascular disease, and loss of metabolic resilience with aging.
Lifestyle Interventions That Work
Medications are powerful tools — but lifestyle modification remains the most cost-effective, accessible, and side-effect-free intervention for cardiometabolic disease. The following strategies have the strongest evidence base.
Nutrition
Mediterranean Diet Pattern (Strongest Evidence)
Emphasizes vegetables, legumes, whole grains, nuts, olive oil, fish, and moderate red wine
The PREDIMED trial showed a 30% reduction in major cardiovascular events
Reduces insulin resistance, inflammation, blood pressure, and LDL simultaneously
DASH Diet (Strong Evidence for Blood Pressure)
Particularly effective for reducing hypertension — a key cardiometabolic risk factor
Rich in potassium, magnesium, calcium; low in sodium and saturated fat
Time-Restricted Eating (Growing Evidence)
Limiting eating to a 8–12 hour window may improve insulin sensitivity and reduce visceral fat
Particularly relevant for people with metabolic syndrome
Foods to Emphasize:
Fatty fish (salmon, mackerel, sardines) — omega-3 fatty acids reduce triglycerides and inflammation
Leafy green vegetables — rich in nitrates that improve endothelial function
Berries — polyphenols reduce oxidative stress and insulin resistance
Extra virgin olive oil — oleocanthal has NSAID-like anti-inflammatory properties
Legumes — improve glycemic control and reduce cardiovascular risk
Foods to Minimize:
Ultra-processed foods promote inflammation, weight gain, and insulin resistance
Sugar-sweetened beverages rapidly elevate blood glucose and promote visceral fat
Trans fats (partially hydrogenated oils) — directly damage endothelial cells
Excess sodium — raises blood pressure, particularly in salt-sensitive individuals
Physical Activity: A Structured Protocol
Here is the structured physical activity protocol rewritten in a highly scannable, point-by-point format:
Zone 2 Cardio (e.g., Brisk Walking, Cycling, Swimming)
Frequency: 4–5 times per week
Duration: 45–60 minutes per session
Cardiometabolic Benefits: Drastically improves baseline insulin sensitivity, accelerates mitochondrial biogenesis (building more cellular energy factories), and optimizes foundational heart function.
Resistance Training (e.g., Weightlifting, Bodyweight Circuits)
Frequency: 2–3 times per week
Duration: 30–45 minutes per session
Cardiometabolic Benefits: Stimulates muscle mass preservation (combating age-related muscle loss), optimizes glucose disposal by using muscle tissue as a metabolic sink for blood sugar, and elevates your baseline resting metabolic rate.
High-Intensity Interval Training (HIIT)
Frequency: 1–2 times per week
Duration: 20–30 minutes per session
Cardiometabolic Benefits: Aggressively increases your VO2max (the gold-standard marker for cardiovascular longevity) and enhances overall myocardial and respiratory efficiency under load.
Daily Movement Breaks (e.g., Stretching, Brief Stairs, Walking)
Frequency: Continuous throughout the day (every 30–60 minutes)
Duration: 5–10 minutes at a time
Cardiometabolic Benefits: Serves as a vital vascular circuit-breaker that immediately counters the negative metabolic, inflammatory, and circulatory consequences of prolonged daytime sitting.
Sleep Optimization
Targeting 7–9 hours of quality sleep per night is not optional — it is metabolically essential. Research consistently shows that sleep deprivation:
Raises cortisol and ghrelin (hunger hormone), promoting overeating
Reduces insulin sensitivity within days
Activates inflammatory pathways identical to those in metabolic syndrome
Increases blood pressure through sympathetic nervous system activation
Stress Management
Chronic psychological stress is increasingly recognized as an independent cardiometabolic risk factor. Evidence-based approaches include:
Mindfulness-based stress reduction (MBSR) — shown to reduce cortisol and inflammatory markers
Regular social connection — protective against cardiovascular disease in large epidemiological studies
Nature exposure — brief time outdoors reduces cortisol and blood pressure
Cardiometabolic Risk: Evidence Summary Table
Here is the clinical breakdown of each lifestyle, training, and pharmaceutical intervention rewritten in a highly scannable, point-by-point format:
Mediterranean Diet
Effect on Insulin Resistance: ✅ Significant improvement in glucose regulation.
Effect on Inflammation: ✅ Significant reduction in systemic inflammatory markers.
Effect on Cardiovascular Risk: ✅ -30% reduction in Major Adverse Cardiovascular Events (MACE).
Evidence Level: Gold Standard — Randomized Controlled Trial (The landmark PREDIMED Study).
Zone 2 Exercise (150 minutes/week)
Effect on Insulin Resistance: ✅ Significant increase in tissue-specific insulin sensitivity.
Effect on Inflammation: ✅ Moderate systemic anti-inflammatory adaptation.
Effect on Cardiovascular Risk: ✅ Significant reduction in long-term cardiovascular mortality.
Evidence Level: High — Proven across multiple large-scale Randomized Controlled Trials.
GLP-1 Receptor Agonists (e.g., Semaglutide)
Effect on Insulin Resistance: ✅ Significant metabolic improvement via appetite suppression and body fat reduction.
Effect on Inflammation: ✅ Moderate baseline reduction in vascular inflammatory cascades.
Effect on Cardiovascular Risk: ✅ Significant drop in major adverse events like stroke and heart attack.
Evidence Level: High — Documented extensively across multiple multi-center clinical trials.
SGLT2 Inhibitors (e.g., Empagliflozin)
Effect on Insulin Resistance: ✅ Moderate improvement due to urinary glucose elimination.
Effect on Inflammation: ✅ Moderate down-regulation of inflammatory markers.
Effect on Cardiovascular Risk: ✅ Significant prevention of heart failure hospitalizations and cardiac death.
Evidence Level: High — Backed firmly by multiple robust Randomized Controlled Trials.
Weight Loss (5% to 10% Body Weight Reduction)
Effect on Insulin Resistance: ✅ Significant reduction in visceral fat, restoring insulin pathway function.
Effect on Inflammation: ✅ Significant reduction in circulating inflammatory cytokines secreted by excess fat tissue.
Effect on Cardiovascular Risk: ✅ Significant drop in comprehensive vascular and plaque risks.
Evidence Level: High — Confirmed across various clinical metabolic trials.
Sleep Optimization (7 to 9 Hours/Night)
Effect on Insulin Resistance: ✅ Moderate metabolic balance by preventing sleep-deprivation-induced cortisol spikes.
Effect on Inflammation: ✅ Moderate baseline recovery and cellular cleanup.
Effect on Cardiovascular Risk: ✅ Moderate long-term vascular protection.
Evidence Level: Moderate — Proven through long-term prospective cohort studies.
Statins (Lipid-Lowering Therapy)
Effect on Insulin Resistance: ➖ Minimal effect (Slightly complex profile, but secondary to vast vascular benefits).
Effect on Inflammation: ✅ Moderate reduction specifically measured by high-sensitivity C-reactive protein ($hs\text{-}CRP$).
Effect on Cardiovascular Risk: ✅ Established clinical reduction in atherosclerotic event rates.
Evidence Level: High — Supported by decades of extensive, global Randomized Controlled Trials.
Stress Reduction (Mindfulness-Based Stress Reduction - MBSR)
Effect on Insulin Resistance: ✅ Modest benefit by gently suppressing chronic sympathetic (fight-or-flight) overactivity.
Effect on Inflammation: ✅ Modest overall structural reduction in chronic stress-induced markers.
Effect on Cardiovascular Risk: ✅ Modest protection via improved blood pressure regulation and heart rate variability.
Evidence Level: Moderate — Backed by targeted clinical Randomized Controlled Trials.
Common Myths & Mistakes
Myth 1: "My cholesterol is normal, so my heart is fine."
The truth: Normal LDL cholesterol does not rule out significant cardiovascular risk. Elevated hsCRP (inflammation), insulin resistance, high triglycerides, and low HDL can each independently elevate risk even with optimal LDL. The cardiometabolic risk picture requires a broader assessment.
Myth 2: "Diabetes is a blood sugar problem — it's separate from heart disease."
The truth: Type 2 diabetes and cardiovascular disease share the same pathophysiological roots. Most people with type 2 diabetes die of cardiovascular causes, not hyperglycemia. Treating blood sugar without addressing cardiovascular risk comprehensively is missing most of the problem.
Myth 3: "I just need to lose weight — then everything will improve."
The truth: While weight loss is valuable, cardiometabolic disease is driven by where fat is stored (visceral vs. subcutaneous), how you lose weight (muscle-preserving vs. muscle-depleting), and the underlying inflammatory and metabolic mechanisms. Two people with identical BMIs can have vastly different cardiometabolic risk profiles.
Myth 4: "These new GLP-1 medications are just diet pills."
The truth: GLP-1 receptor agonists are among the most cardiovascularly protective medications ever developed. In the SELECT trial (2023), semaglutide reduced major adverse cardiovascular events by 20% in people with obesity — regardless of diabetes status. These are serious cardiometabolic medicines with wide-ranging systemic effects.
Myth 5: "I should wait until I have a diagnosis to start worrying."
The truth: The most important interventions happen in the pre-disease window. Once structural heart disease or significant atherosclerosis develops, repair is far more difficult than prevention. Early metabolic warning signs — pre-diabetes, elevated hsCRP, abdominal obesity — are the time to act.
Myth 6: "Cardiometabolic disease only affects overweight people."
The truth: While excess adiposity is a major risk factor, "metabolically unhealthy normal weight" (sometimes called TOFI — "thin outside, fat inside") is real and increasingly recognized. People with normal BMI but significant visceral fat, sedentary lifestyles, and poor diet can have substantial cardiometabolic risk.
A New Medical Specialty for a New Era
One of the most forward-thinking proposals emerging from 2025 research is the call to establish Cardiovascular-Endocrine-Metabolic Medicine as a formal clinical sub-specialty.
A compelling 2025 paper in Biomolecules argues that the current model — in which cardiologists, endocrinologists, and nephrologists each manage their "piece" of the cardiometabolic patient in separate clinic appointments — is fundamentally insufficient (Theodorakis, Nikolaou, & Krentz, 2025). This fragmentation leads to:
Conflicting medication decisions between specialists
Missed opportunities to use single medications that benefit multiple systems simultaneously
Inefficient, expensive care with poor coordination
The proposed sub-specialty would train clinicians with deep expertise across cardiovascular disease, metabolic dysfunction, diabetes, obesity, and chronic kidney disease — enabling genuinely integrated patient care.
What this means for you now: While this formal specialty doesn't exist everywhere yet, you can seek out academic medical centers and progressive health systems that have already implemented integrated cardiometabolic care clinics. Alternatively, work with your primary care physician to ensure your cardiometabolic risk factors are being addressed comprehensively — not in separate silos.
Cardiometabolic Disease Prevention Checklist
Use this checklist to assess and guide your cardiometabolic health:
Lifestyle Foundations
Achieving 150+ minutes of moderate aerobic activity per week
Including 2–3 sessions of resistance training per week
Following a predominantly whole-food, Mediterranean-style diet
Sleeping 7–9 hours per night consistently
Limiting ultra-processed foods and sugar-sweetened beverages
Practicing regular stress management (mindfulness, social connection, nature)
Taking regular movement breaks during prolonged sitting
Key Biomarkers to Monitor (discuss with your doctor)
Fasting glucose and HbA1c (to detect pre-diabetes early)
Fasting insulin (sensitive marker of insulin resistance, often overlooked)
Lipid panel including triglycerides and HDL
High-sensitivity CRP (hsCRP) for inflammation
Blood pressure (home monitoring as well as clinic readings)
Waist circumference (measure, not just BMI)
Kidney function (eGFR and urine albumin-to-creatinine ratio)
Medical Conversation Points
Ask about SGLT2 inhibitors or GLP-1 agonists if you have diabetes, heart failure, or obesity
Request comprehensive cardiometabolic risk assessment, not just cholesterol
Discuss integrated care if you are seeing multiple specialists
Consider wearable technology for continuous health monitoring
FAQs
What is the difference between cardiometabolic disease and metabolic syndrome?
Metabolic syndrome is a clinical diagnosis requiring three or more of five specific criteria (abdominal obesity, high triglycerides, low HDL, elevated blood pressure, elevated fasting glucose). Cardiometabolic disease is a broader concept describing the unified biological processes — primarily insulin resistance, chronic inflammation, and endothelial dysfunction — that drive both cardiovascular and metabolic disorders. You can have significant cardiometabolic disease risk without formally meeting metabolic syndrome criteria.
Can cardiometabolic disease be reversed?
Evidence strongly supports that early-stage cardiometabolic disease — particularly insulin resistance and pre-diabetes — can be substantially reversed or halted through lifestyle intervention. Weight loss of as little as 5–7% of body weight, combined with regular exercise and dietary improvement, has been shown to normalize blood glucose, reduce inflammation, and improve cardiovascular risk markers. More advanced disease (established atherosclerosis, type 2 diabetes with complications) is less fully reversible but can still be meaningfully improved and progression halted.
Are GLP-1 medications safe long-term?
GLP-1 receptor agonists have now been studied in large-scale cardiovascular outcomes trials with follow-up of 2–5+ years, consistently demonstrating both safety and significant cardiovascular benefit. The most common side effects are gastrointestinal (nausea, vomiting), which typically resolve over time. Rare but serious concerns include pancreatitis and, at very high doses in animal models, thyroid C-cell effects. Discuss the complete benefit-risk profile with your physician.
What blood tests should I ask for to assess cardiometabolic risk?
Beyond standard cholesterol panels, consider requesting: fasting insulin (to detect insulin resistance early), HbA1c, hsCRP (inflammation), a complete metabolic panel (kidney function), uric acid (elevated levels correlate with cardiometabolic risk), and a lipoprotein(a) — Lp(a) — level (a genetically determined independent cardiovascular risk factor). Your doctor can advise which are appropriate for your situation.
How does sleep affect cardiometabolic health?
Consistently poor sleep (less than 6 hours or fragmented sleep from obstructive sleep apnea) impairs insulin sensitivity within days, elevates inflammatory cytokines, raises cortisol and blood pressure, and disrupts appetite hormones — promoting overeating and weight gain. In large epidemiological studies, short sleep duration is associated with 20–48% increased risk of cardiovascular events. Sleep is not a passive recovery state — it is active cardiometabolic maintenance.
Is belly fat really more dangerous than fat elsewhere?
Yes, definitively. Visceral adipose tissue (fat surrounding abdominal organs) is metabolically active in ways that subcutaneous fat (under the skin) is not. Visceral fat secretes pro-inflammatory adipokines, releases free fatty acids directly into the portal circulation (reaching the liver first), and promotes insulin resistance at a systemic level. Waist circumference is a better predictor of cardiometabolic risk than BMI alone.
What role does the gut microbiome play in cardiometabolic disease?
An active area of research. Reduced gut microbial diversity — associated with poor diet, sedentary lifestyle, and antibiotic overuse — appears to promote metabolic endotoxemia (leakage of bacterial components into the bloodstream that drives systemic inflammation), impair glucose metabolism, and alter bile acid signaling (which regulates lipid absorption and insulin sensitivity). A high-fiber, plant-rich diet is the strongest evidence-based approach to supporting a cardiometabolically protective microbiome.
How does stress cause heart disease?
Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system, leading to persistently elevated cortisol and catecholamines. These hormones raise blood pressure and heart rate, promote visceral fat deposition, increase platelet aggregation (clotting risk), impair endothelial function, and drive systemic inflammation. People with high chronic stress have significantly elevated rates of myocardial infarction, even controlling for traditional risk factors.
What is Zone 2 exercise and why is it so important for metabolic health?
Zone 2 exercise is moderate-intensity cardio performed at approximately 60–70% of maximum heart rate — typically described as an effort level where you can speak in full sentences but are breathing more than at rest. At this intensity, your muscles primarily burn fat for fuel, training the mitochondria to become more efficient at fatty acid oxidation. Regular Zone 2 training improves insulin sensitivity, increases mitochondrial density, reduces inflammation, and provides significant cardiovascular protection. Aim for 3–5 hours per week across multiple sessions.
Should I use wearable technology to monitor cardiometabolic health?
Wearable devices — including continuous glucose monitors (CGMs), heart rate variability (HRV) trackers, and smartwatches — can provide valuable real-time cardiometabolic data. CGMs in particular have demonstrated clinical value beyond diabetes: seeing how specific meals spike your glucose enables personalized dietary optimization. The 2025 ACC trends report and Nature Metabolism analysis both highlight technology-enabled monitoring as a key enabler of precision cardiometabolic medicine. That said, data from wearables should be interpreted in the context of professional medical guidance.
At what age should I start thinking about cardiometabolic risk?
Earlier than most people realize. Atherosclerosis begins in adolescence or early adulthood. Insulin resistance can develop in the 20s and 30s in individuals with poor lifestyle habits. The risk factors that matter most — diet, exercise, sleep, stress, weight — are established in early adulthood. However, meaningful intervention has clear benefits at any age, including in older adults. The key principle: the earlier you act, the more biological capital you have to work with.QV
Conclusion & Action Steps
Cardiometabolic disease is not a future threat — for hundreds of millions of people worldwide, it is an active biological process quietly unfolding right now. But the science of 2025–2026 offers an extraordinarily clear message: this process can be interrupted, slowed, and in many cases reversed, especially when you act early.
The unifying insight that drives modern cardiometabolic medicine is this — your heart and your metabolism are one system. Winning for one means winning for the other. The medications (GLP-1s, SGLT2 inhibitors), the lifestyle strategies (Mediterranean diet, Zone 2 exercise, quality sleep), and the emerging therapies (anti-inflammatories, mitochondrial agents) all work best when applied as part of a coherent, integrated approach that targets the shared root causes.
Your Action Steps
Schedule a comprehensive cardiometabolic assessment — not just cholesterol, but fasting insulin, hsCRP, HbA1c, waist circumference, and blood pressure
Start with lifestyle — even modest improvements in diet, exercise, and sleep produce measurable cardiometabolic benefits within weeks
Ask about modern medications — if you have any combination of diabetes, obesity, heart failure, or chronic kidney disease, ask your physician specifically about SGLT2 inhibitors and GLP-1 agonists
Monitor more than annually — consider wearable technology, home blood pressure monitoring, and periodic biomarker tracking to catch changes early
Seek integrated care — if you are seeing multiple specialists, ensure they are communicating and viewing your health as a single system
Prioritize sleep and stress — these are not lifestyle luxuries; they are cardiometabolic medicines
Think long-term — cardiometabolic health is not a sprint. It is the cumulative effect of daily choices compounding over years.
The most powerful intervention is the one you begin today. Your biology is remarkably responsive when given the right inputs. Start now, and let the science guide the way.
References
American College of Cardiology. (2025, January 1). Cover story: Transformative trends in CV medicine for 2025. American College of Cardiology. https://www.acc.org/latest-in-cardiology/articles/2025/01/01/42/cover-story-transformative-trends-in-cv-medicine-for-2025
Caturano, A. (2025). Cardiovascular and metabolic disease: New treatment and future directions—The 3rd edition. Biomedicines, 13(8), Article 1914. https://doi.org/10.3390/biomedicines13081914
Clemmensen, C., Gerhart-Hines, Z., Schwartz, T. W., et al. (2025). Shaping the future of cardiometabolic innovation: Advances and opportunities. Nature Metabolism, 7, 1495–1497. https://doi.org/10.1038/s42255-025-01343-5
Eroglu, T., Capone, F., & Schiattarella, G. G. (2024). The evolving landscape of cardiometabolic diseases. EBioMedicine, 109, Article 105447. https://doi.org/10.1016/j.ebiom.2024.105447
Estruch, R., Ros, E., Salas-Salvadó, J., et al. (2018). Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts (PREDIMED). New England Journal of Medicine, 378(25), Article e34. https://doi.org/10.1056/NEJMoa1800389
Evans, P. C., Vilahur, G., Kleinbongard, P., Osto, E., Remme, C. A., Madonna, R., Aksentijevic, D., Sourij, H., Davidson, S. M., Santovito, D., Gindlhuber, J., Weber, C., Linke, W. A., Lutgens, E., Bertrand, L., Dawson, D., Bäck, M., Norata, G. D., Wojta, J., & Perrino, C. (2026). Novel cardiovascular metabolic risk factor mechanisms and therapeutic opportunities: A scientific statement of the ESC Council on Basic Cardiovascular Science. European Heart Journal, Article ehag116. Advance online publication. https://doi.org/10.1093/eurheartj/ehag116
Frontiers in Cardiovascular Medicine. (2026). Metabolic remodeling in structural cardiac disease [Abstract]. Frontiers in Cardiovascular Medicine. https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2026.1824863/abstract
Gudla, S. S., Bhumireddy, S. K. A., Vadaga, A. K., et al. (2026). Managing metabolic risks in coronary artery disease: A scoping review of recent clinical and therapeutic evidence. Journal of Diabetes & Metabolic Disorders, 25, Article 118. https://doi.org/10.1007/s40200-026-01916-5
Hawley, J. A., & Hoffman, N. J. (2025). Twenty years of progress in human exercise metabolism research. Nature Reviews Endocrinology, 21(10), 658–659. https://doi.org/10.1038/s41574-025-01181-1
Kim, H. (2025). Expanding the role of novel therapeutics in cardiometabolic syndrome: Beyond heart failure and diabetes. CardioMetabolic Syndrome Journal, 5(1), Article 9. https://doi.org/10.51789/cmsj.2025.5.e4
Laha, A., Bhatt, D. L., & Nissen, S. E. (2024). Obesity, metabolic syndrome, and cardiovascular disease. JACC: Basic to Translational Science, 9(4), 543–557. https://doi.org/10.1016/j.jacbts.2023.11.011
Luyster, F. S., Strollo, P. J., Zee, P. C., & Walsh, J. K. (2012). Sleep: A health imperative. Sleep, 35(6), 727–734. https://doi.org/10.5665/sleep.1846
Marso, S. P., Daniels, G. H., Brown-Frandsen, K., et al. (2016). Liraglutide and cardiovascular outcomes in type 2 diabetes (LEADER trial). New England Journal of Medicine, 375(4), 311–322. https://doi.org/10.1056/NEJMoa1603827
McMurray, J. J. V., Solomon, S. D., Inzucchi, S. E., et al. (2019). Dapagliflozin in patients with heart failure and reduced ejection fraction (DAPA-HF). New England Journal of Medicine, 381(21), 1995–2008. https://doi.org/10.1056/NEJMoa1911303
Packer, M., Anker, S. D., Butler, J., et al. (2021). Cardiovascular and renal outcomes with empagliflozin in heart failure (EMPEROR-Reduced). New England Journal of Medicine, 385(16), 1451–1461. https://doi.org/10.1056/NEJMoa2103765
Ren, J., Chen, X., & Wang, X. (2025). Emerging therapeutic frontiers in cardiometabolic and inflammatory diseases. British Journal of Pharmacology, 182(20), 4737–4740. https://doi.org/10.1111/bph.70159
Ridker, P. M., Danielson, E., Fonseca, F. A. H., et al. (2008). Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein (JUPITER). New England Journal of Medicine, 359(21), 2195–2207. https://doi.org/10.1056/NEJMoa0807646
Ridker, P. M., Everett, B. M., Thuren, T., et al. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease (CANTOS trial). New England Journal of Medicine, 377(12), 1119–1131. https://doi.org/10.1056/NEJMoa1707914
Schiattarella, G. G., & Hill, J. A. (2021). Inhibition of hypertrophy is a good therapeutic strategy in ventricular pressure overload. Circulation, 143(9), 929–933. https://doi.org/10.1161/CIRCULATIONAHA.120.051670
ScienceDirect. (2025). Emerging pathophysiology of cardiometabolic disorders [Review]. Metabolism — Clinical and Experimental. https://www.sciencedirect.com/science/article/pii/S0939475325004399
Theodorakis, N., Nikolaou, M., & Krentz, A. (2025). Cardiovascular-endocrine-metabolic medicine: Proposing a new clinical sub-specialty amid the cardiometabolic pandemic. Biomolecules, 15(3), Article 373. https://doi.org/10.3390/biom15030373
Last updated: May 2026