Can Dietary Cholesterol Worsen Fatty Liver? Here's What the Science Really Shows
Can eggs and cholesterol worsen fatty liver? Discover the latest evidence on MASLD, inflammation, fibrosis, and the healthiest eating pattern for your liver.
METABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/30/202619 min read
Does dietary cholesterol worsen fatty liver disease (NAFLD/MASLD)?
Yes, but context matters. Current research shows dietary cholesterol does not cause fatty liver disease on its own. However, if you already have fat accumulation, obesity, or insulin resistance, high dietary cholesterol acts as a "second hit." It triggers a cellular stress protein called HIF-1, forms inflammatory cholesterol crystals, and damages microscopic blood vessels in the liver, significantly accelerating the progression from simple fatty liver to advanced inflammation (NASH/MASH) and liver scarring (fibrosis). Complete elimination is rarely necessary; clinical guidelines instead recommend a Mediterranean diet to manage the underlying metabolic strain.
Key takeaways :
Context Dictates Toxicity: Dietary cholesterol is not an independent instigator. It acts as a "second hit"—behaving benignly in a metabolically healthy environment, but acting like gasoline on a fire when introduced to a liver already burdened by fat accumulation, obesity, or insulin resistance.
The 2023 Paradigm Shift: The medical community has officially dropped the stigmatizing terms NAFLD and NASH in favor of MASLD and MASH. This rebrand centers the disease precisely where it belongs: on metabolic dysfunction rather than just the absence of alcohol use.
A Cellular State of Emergency: Excess cholesterol literally alters liver biology by prematurely switching on HIF-1—a stress protein normally reserved for severe oxygen deprivation. This false alarm forces liver cells into a destructive, unneeded inflammatory spiral.
Microscopic Gridlock: Cholesterol-driven inflammation directly damages the liver's delicate, microscopic blood vessel network (sinusoids). This creates localized "traffic jams" that starve patches of liver tissue of vital oxygen, explaining why MASH damage often appears scattered and uneven on biopsies.
Physical Crystallization: When the liver is overwhelmed by cholesterol, the excess physically crystallizes inside the tissue. The immune system treats these crystals as foreign invaders, swarming them with macrophages to form microscopic inflammatory battlegrounds known as "crown-like structures."
The Multi-Faceted Villain: Cholesterol does not act alone. Excessive intake of Omega-6 polyunsaturated fatty acids (found heavily in industrial seed and vegetable oils) fuels MASH progression through separate, highly active inflammatory pathways. Total dietary quality matters far more than isolating a single nutrient.
Moderation Beats Elimination: The data does not support a zero-cholesterol panic. Whole foods like eggs and shellfish carry vital micronutrients (such as choline) and can remain in a liver-smart diet, provided they are framed within a calorie-conscious, Mediterranean-style eating pattern.
The Statin Myth Dispelled: Despite persistent patient fears that cholesterol medications strain the liver, current clinical data shows that statins are entirely safe for MASLD patients. In fact, they are robustly associated with lower rates of liver scarring (fibrosis) and liver cancer.
Introduction
If you've just been told you have a "fatty liver" — officially called NAFLD (non-alcoholic fatty liver disease), or MASLD under the newer naming — there's a good chance cholesterol was mentioned somewhere in that conversation. Maybe your doctor flagged high LDL on a blood panel. Maybe you've read that eggs or shrimp are suddenly "off limits." Maybe you're just trying to figure out whether cutting cholesterol will actually help your liver, or whether that's outdated advice repeating itself across wellness blogs.
This is a fair question, and it deserves a real answer — not a scare headline.
Here's the short version: a growing body of research, mostly from animal studies, shows that high dietary cholesterol can accelerate liver inflammation, fibrosis, and microvascular damage in the context of existing fatty liver disease. It does this through specific, identifiable biological pathways — including a stress-response protein called HIF-1 (hypoxia-inducible factor 1) and damage to the liver's smallest blood vessels. But the picture is more nuanced than "cholesterol is bad for your liver," and the practical takeaway is not the same as the cardiovascular cholesterol advice you've heard before.
What Is NAFLD/NASH (MASLD/MASH)?
Before getting into cholesterol specifically, it helps to understand what's actually happening inside the liver.
NAFLD (non-alcoholic fatty liver disease) describes a buildup of fat inside liver cells that isn't caused by heavy alcohol use. It's extremely common — estimates suggest it affects roughly a quarter to a third of adults worldwide, closely tracking the rise in obesity and type 2 diabetes.
In 2023, the major liver associations renamed the condition. You'll now increasingly see:
MASLD (metabolic dysfunction-associated steatotic liver disease) — replacing NAFLD
MASH (metabolic dysfunction-associated steatohepatitis) — replacing NASH
Both names refer to the same disease spectrum. Since "NAFLD" and "NASH" are still what most people search for and what most older research uses, this article uses both naming conventions interchangeably, noting MASLD/MASH where current literature does.
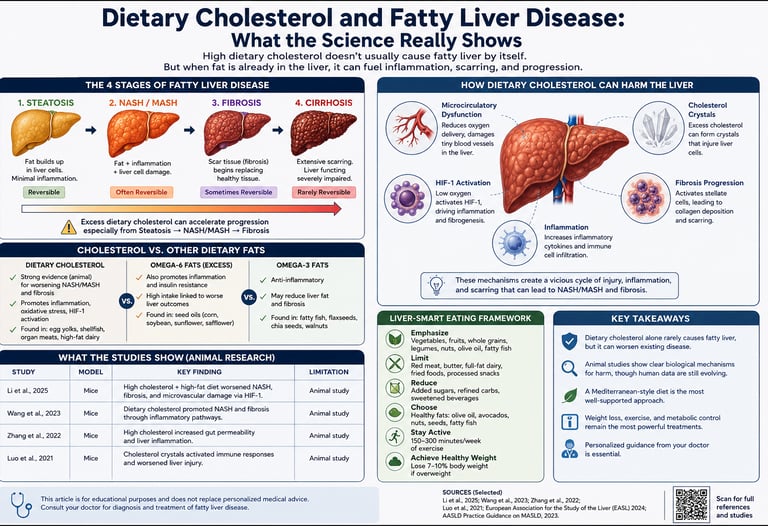
NAFLD progresses in stages:
Here is the breakdown of the progression stages of liver disease, organized into clear bullet points:
Simple Steatosis
What's Happening: Fat accumulates inside the liver cells, but there is minimal inflammation.
Reversible? Yes, typically reversible with targeted lifestyle adjustments.
NASH / MASH (Steatohepatitis)
What's Happening: Fat accumulation is now accompanied by cellular inflammation and direct liver cell damage.
Reversible? Often reversible with timely and consistent clinical intervention.
Fibrosis
What's Happening: Ongoing damage causes scar tissue to form, which begins replacing healthy liver tissue.
Reversible? Early stages can sometimes be reversed if the underlying stressor is removed.
Cirrhosis
What's Happening: Extensive, permanent scarring occurs, severely distorting the liver's architecture and function.
Reversible? Rarely fully reversible; management focuses on halting progression and preventing complications.
The critical jump is from simple steatosis to NASH/MASH — this is where inflammation starts doing lasting damage, and it's exactly the stage where dietary cholesterol appears to play an outsized role.
Does Dietary Cholesterol Cause Fatty Liver Disease?
Quick answer for those skimming: Dietary cholesterol alone doesn't appear to initiate NAFLD in someone with an otherwise healthy liver and normal weight. But in the presence of existing fat accumulation, obesity, or insulin resistance, high dietary cholesterol intake consistently accelerates the progression from simple fatty liver to the more dangerous inflammatory and fibrotic stages (NASH/MASH).
This distinction matters enormously, and it's where a lot of consumer health content gets sloppy. Think of it less like a single cause and more like gasoline poured on a fire that's already burning. The fire (excess calories, obesity, insulin resistance) typically has to be present first.
This "second hit" framing is consistent across the research base. In one 2026 study, researchers found that a high-fat, high-cholesterol diet accelerated hepatic lipid accumulation, inflammatory crown-like structure formation, and fibrosis compared to a standard high-fat diet alone — meaning cholesterol specifically, on top of fat, made things measurably worse.
Similarly, older foundational research established this same pattern in a different model: dietary cholesterol exacerbated hepatic steatosis and inflammation specifically in mice that were already obese and genetically predisposed to high LDL cholesterol — not in normal, healthy mice.
So if you're asking "will eating eggs give me fatty liver disease," the evidence doesn't support that as a standalone claim. If you're asking "will high cholesterol intake make my existing fatty liver worse," the evidence is considerably more concerning.
The Science: How Cholesterol Damages the Liver
Here's where we get into the actual biology — explained without a biochemistry degree required.
Mechanism 1: Cholesterol Crystals and Immune Activation
When liver cells take in more cholesterol than they can safely store or process, some of it crystallises — literally forming tiny crystal structures inside and around liver cells. Your immune system reads these crystals as foreign threats and launches an inflammatory response, similar to how it reacts to crystals in gout.
This triggers the formation of what researchers call "crown-like structures" — clusters of immune cells (specifically macrophages) that surround clusters of dead or dying, cholesterol-loaded liver cells. Studies using high-fat, high-cholesterol diets have specifically documented increased crown-like structure formation as a hallmark of accelerated disease, and this finding shows up repeatedly across independent research groups using different mouse models.
Mechanism 2: Upregulation of HIF-1 (Hypoxia-Inducible Factor 1)
This is genuinely one of the more interesting and clinically relevant mechanisms in recent research, so it's worth understanding properly.
HIF-1 is a protein your cells normally activate when oxygen levels drop too low — it's your body's emergency oxygen-shortage response system. Under normal circumstances, this is protective: it helps tissues adapt to low-oxygen conditions.
The problem is that excess dietary cholesterol appears to switch HIF-1 on even when oxygen levels haven't actually dropped — essentially tricking liver cells into mounting a stress response they don't need yet, which paradoxically makes things worse rather than better.
According to a 2023 study published in Nutrients, cholesterol-rich diets in animal models of NASH significantly upregulated HIF-1, and this upregulation was directly associated with worsened liver pathology and disrupted blood flow at the microscopic level within the liver. The researchers proposed that this isn't a side effect — it's a contributing driver of disease progression.
Mechanism 3: Microcirculatory Dysfunction
Your liver depends on an enormous, delicate network of microscopic blood vessels (sinusoids) to deliver oxygen and nutrients to every single liver cell. This is the "microcirculation."
When cholesterol-driven inflammation and HIF-1 activation disrupt this network, liver cells genuinely start receiving less oxygen — even though overall blood flow to the liver may look normal on standard imaging. This creates a vicious cycle: low local oxygen triggers more HIF-1 activation, which drives more inflammation, which further damages the microcirculation.
This mechanism explains something that puzzled researchers for years: why does liver damage in NASH sometimes look patchy and uneven, rather than uniform? Microcirculatory dysfunction — localized to specific areas where blood flow is most compromised — is a compelling explanation.
Mechanism 4: Aging Compounds the Damage
It's also worth noting that age isn't a neutral bystander here. Research specifically examining high-fat diet effects across age groups found that aging exacerbates high-fat diet-induced steatohepatitis through alterations in how the liver metabolizes lipids — meaning the same cholesterol-rich diet may do more damage in a 55-year-old liver than a 25-year-old one, independent of weight.
HIF-1 and Microcirculatory Dysfunction, Explained Simply
Because this is genuinely the newest and least-understood part of the science, let's use an analogy.
Imagine your liver's blood vessel network as a city's road system, and oxygen as deliveries that need to reach every building (liver cell). Normally, traffic flows fine.
Cholesterol overload is like dumping debris in certain streets.
Crown-like structures are like traffic cops (immune cells) swarming to the blockage — necessary, but they also slow everything down further.
HIF-1 activation is like the city declaring a state of emergency before deliveries have actually stopped — diverting resources reactively, which disrupts normal function even more.
Microcirculatory dysfunction is the resulting gridlock: some buildings (liver cell clusters) stop receiving deliveries reliably, even though the city overall still "has roads."
This is why liv
doesn't look like one uniform injury — it looks like scattered pockets of more severe damage next to relatively preserved tissue, exactly matching what you'd expect from localised traffic jams rather than a citywide shutdown.
Why This Matters Clinically, Not Just Academically
This isn't just mechanistic trivia. HIF-1 and microcirculation are now recognized as legitimate therapeutic targets — meaning future drugs for NASH may specifically work by blocking inappropriate HIF-1 activation or protecting the liver's microvasculature, rather than only targeting fat accumulation itself. Understanding this mechanism is part of why current NASH drug development has moved well beyond simply "reduce liver fat."
Evidence Summary: What Each Study Actually Found
Here's a transparent breakdown of the core studies behind this article, including their real limitations. Notice that nearly all of this evidence comes from animal models — a critical, honest caveat that the wellness internet often glosses over.
Pereira et al., Nutrients (2023)
Model: Mouse (NASH model)
Key Finding: Cholesterol upregulated HIF-1, worsening microcirculatory dysfunction and liver pathology.
Limitation: Animal model; the mechanism is not yet confirmed via liver biopsy in humans.
Subramanian et al., J Lipid Research (2011)
Model: Obese, LDL-receptor-deficient mice
Key Finding: Dietary cholesterol exacerbated hepatic steatosis and inflammation, but specifically in already-obese, genetically susceptible mice.
Limitation: Genetically modified mouse model; does not represent average human metabolism.
Ishizuka et al., J Gastro Hepatol (2020)
Model: Aging mice
Key Finding: Aging worsened high-fat diet-induced steatohepatitis via altered lipid metabolism.
Limitation: Mouse model; the interaction between human aging and liver pathology is less studied.
Zhou et al. (Jian-Tong et al.), Front Nutr (2025)
Model: Rat model
Key Finding: High n-6 PUFA intake (rather than cholesterol specifically) exacerbated NASH via multiple inflammatory pathways.
Limitation: Rat model; isolates PUFAs, making it not a direct cholesterol comparison.
Xiang et al., Nutrients (2024)
Model: Diet pattern analysis (Human data)
Key Finding: Poor overall diet quality exacerbates MASLD via the abdominal obesity pathway.
Limitation: Broader dietary pattern study; does not isolate the specific impact of cholesterol.
Model: STAM mouse model
Key Finding: A high-fat, high-cholesterol diet accelerated lipid accumulation, inflammation, and fibrosis compared to a high-fat diet alone.
Limitation: Animal model; the STAM model has its own known limitations in mimicking human MASH onset.
What this table tells us, honestly: The directionality is remarkably consistent — every single study, across different labs, countries, and animal models, found that added dietary cholesterol (on top of an already obesogenic or high-fat diet) made liver disease markers worse, never better. That consistency across independent research groups is scientifically meaningful, even without large human randomized trials yet.
What it doesn't yet tell us: The exact dose-response relationship in humans, the threshold at which dietary cholesterol becomes harmful for a person with NAFLD specifically, and whether reducing dietary cholesterol alone (without broader weight or metabolic improvement) meaningfully reverses human NASH.
Cholesterol vs. Other Dietary Fats: Who's the Bigger Problem?
A reasonable next question: if cholesterol is one driver, is it the main driver, or are other fats just as bad — or worse?
According to a 2025 study in Frontiers in Nutrition, excessive intake of n-6 polyunsaturated fatty acids (n-6 PUFAs) — common in many vegetable oils used heavily in processed and fried foods — exacerbated NASH through a separate set of inflammatory pathways involving compounds called leukotrienes and prostaglandins, derived from arachidonic acid metabolism.
This doesn't mean cholesterol is innocent and PUFAs are the real villain. It means NAFLD/NASH progression is multi-factorial, and several dietary components — cholesterol, excess n-6 PUFAs, ultra-processed carbohydrates, and overall caloric surplus — appear to converge on overlapping inflammatory pathways in the liver, including some that involve the immune system's macrophages and arachidonic acid derivatives, similar to cholesterol's crown-like structure mechanism.
A 2024 study in Nutrients examining broader dietary patterns reinforced this: it wasn't one single "bad nutrient" but an overall pattern of poor diet quality, driving abdominal obesity, that exacerbated MASLD severity.
The practical implication: focusing exclusively on cholesterol while ignoring overall diet quality, refined carbohydrates, added sugars, and excess omega-6 vegetable oil intake would be a mistake. They appear to act together, not independently.
Clinical Importance: Why This Matters for Your Liver Health
This is the section that matters most if you're managing this condition right now, so let's be direct about clinical interpretation rather than just mechanism.
Why "It's Just Animal Data" Doesn't Mean "Ignore It"
Most of the mechanistic studies above are indeed in rodents. But mouse and rat models of NASH are specifically used in hepatology research because the disease progression — fat accumulation, inflammation, fibrosis — closely mirrors human liver pathology at the tissue level, even if the exact triggers and timeline differ. Drug companies use these same models to develop NASH medications that then go to human trials. That's a meaningful form of biological relevance, even short of direct human dietary trial data.
What This Means If You Already Have NAFLD/NASH
If you've been diagnosed with simple fatty liver (steatosis), this research suggests cholesterol intake is one lever — among several — worth moderating, particularly if you also have:
Obesity or excess visceral (abdominal) fat
Type 2 diabetes or insulin resistance
Elevated LDL cholesterol on bloodwork
A family history of more severe liver disease
If you've progressed to NASH/MASH or any degree of fibrosis, the clinical stakes are higher, and dietary cholesterol moderation becomes one part of a broader, doctor-supervised metabolic strategy — not a stand-alone fix.
What This Means If You Don't Have Diagnosed Liver Disease
If your liver is currently healthy, this research is more about prevention than urgent restriction. The studies consistently show cholesterol's harm appears in the context of an existing metabolic "first hit" — so the most protective thing you can do isn't cholesterol elimination; it's avoiding the conditions (obesity, insulin resistance, poor overall diet quality) that make cholesterol dangerous to the liver in the first place.
The Bloodwork Connection
It's worth understanding that "dietary cholesterol" and "blood cholesterol (LDL)" are related but distinct. Current clinical guidelines note that statins — cholesterol-lowering medications — are generally considered safe for people with MASLD, and have actually been associated with reduced risk of liver fibrosis, NASH/MASH, and even liver cancer in case-controlled studies. This is a genuinely important, reassuring clinical point: if your doctor recommends a statin for cardiovascular reasons, you do not need to fear it's harmful to your liver — the evidence points the opposite direction.
Practical Application: A Liver-Smart Eating Framework
This section translates the science into something you can actually do at your next meal. Current EASL/EASD/EASO 2024 clinical guidelines recommend an overall diet quality similar to the Mediterranean diet to improve liver injury in adults with MASLD, while limiting ultra-processed foods rich in sugar and saturated fat, and avoiding sugar-sweetened beverages entirely.
Step 1: Don't Fixate on Eliminating Dietary Cholesterol Entirely
Foods like eggs, shrimp, and lean organ meats contain cholesterol but also deliver meaningful protein, choline, and micronutrients. Complete elimination isn't what the evidence supports — moderation in the context of overall diet quality is.
A reasonable, doctor-discussable target: many clinicians managing NAFLD suggest keeping dietary cholesterol intake moderate — for context, a single large egg contains about 185mg of cholesterol — rather than eliminating cholesterol-containing foods outright, while prioritizing the changes below, which have a larger evidence base.
Step 2: Prioritize a Mediterranean-Style Eating Pattern
This is the single most evidence-backed dietary approach for NAFLD/MASLD specifically. Core components:
Healthy fats: extra-virgin olive oil as your primary fat source
Fish: at least 2 servings weekly, prioritizing fatty fish (salmon, sardines, mackerel) for omega-3s
Vegetables and legumes: the bulk of your plate at most meals
Whole grains over refined carbohydrates
Nuts in moderate, regular amounts
Limited red and processed meat
Step 3: Actively Reduce Excess n-6 PUFA Intake
Given the research on n-6 PUFAs and NASH progression, it's worth specifically limiting:
Heavily processed foods fried in soybean, corn, or sunflower oil
Packaged snack foods and fast food (a major source of industrial n-6 oils)
Replacing some n-6-heavy oils with olive oil or avocado oil where practical
Step 4: Address Abdominal Obesity Directly
Since abdominal obesity is repeatedly identified as the pathway through which poor diet exacerbates MASLD, weight management — even modest, sustainable loss of 5-10% of body weight — has consistently shown measurable improvement in liver fat and inflammation in clinical studies, more reliably than any single nutrient change alone.
Step 5: Eliminate Sugar-Sweetened Beverages First
Current clinical guidance specifically calls for avoiding sugar-sweetened beverages — this is one of the more unambiguous, low-effort wins available, since liquid sugar drives both liver fat accumulation and abdominal obesity with no nutritional offset.
A Sample Day, Liver-Smart Framework
Here is the meal plan broken down into clear, scannable bullet points:
Breakfast
Greek yogurt
Berries and walnuts
A drizzle of olive oil-based granola
Lunch
Lentil and vegetable salad
Olive oil-lemon dressing
Grilled fish
Snack
A small handful of almonds
A piece of fruit
Dinner
Baked salmon
Roasted vegetables
Quinoa
Side salad
Beverages
Water
Unsweetened tea or coffee (no sugar-sweetened drinks)
A Quick Self-Check Before Changing Your Diet
[ ] Have you been formally diagnosed with NAFLD/MASLD, or are you acting on assumption?
[ ] Do you know your current liver enzyme levels (ALT/AST) and fibrosis stage, if any?
[ ] Have you discussed statin use with your doctor if your LDL is elevated?
[ ] Are you addressing alcohol intake, which independently worsens liver disease?
[ ] Is your overall calorie intake aligned with a healthy weight trajectory?
Common Myths & Mistakes About Cholesterol and Liver Disease
Myth 1: "I have fatty liver, so I need a zero-cholesterol diet." Not supported by current evidence. Moderation in the context of overall diet quality is what the research and clinical guidelines actually point to — not elimination.
Myth 2: "Statins will hurt my liver since I already have liver disease." This is one of the most persistent and outdated fears in this space. Statins are generally considered safe for people with MASLD and may actually reduce fibrosis risk; stopping a prescribed statin out of liver concern, without talking to your doctor, may do more harm than good.
Myth 3: "If I'm thin, I don't need to worry about dietary cholesterol and my liver." NAFLD also occurs in normal-weight individuals ("lean NAFLD"), often driven by insulin resistance or visceral fat that isn't visible externally. Body weight alone isn't a reliable indicator of liver risk.
Myth 4: "Only saturated fat matters — cholesterol itself is irrelevant to liver disease." The mechanistic research, particularly around HIF-1 and microcirculatory dysfunction, suggests cholesterol has effects somewhat distinct from saturated fat alone, including direct effects on liver microvasculature.
Myth 5: "Eggs are the main dietary cholesterol threat I need to worry about." Total dietary pattern, abdominal fat, and excess n-6 PUFA intake from processed foods and oils appear to matter just as much, if not more, than any single cholesterol-containing food.
Mistake to avoid: Making drastic dietary changes without monitoring. Liver disease management should ideally be paired with periodic monitoring (liver enzymes, imaging, or fibrosis scores) so you and your doctor can see whether changes are actually working.
FAQs
Does eating eggs cause fatty liver disease? No single study shows eggs alone cause NAFLD in metabolically healthy people. The evidence shows dietary cholesterol accelerates existing fatty liver disease, particularly in the context of obesity or insulin resistance — eggs in moderation, within an otherwise balanced diet, aren't established as a standalone cause.
What foods should I avoid with fatty liver disease? Priority targets based on current evidence: sugar-sweetened beverages, ultra-processed foods high in refined carbohydrates and saturated fat, excess fried food cooked in industrial seed oils high in n-6 PUFAs, and excessive alcohol. Cholesterol-containing whole foods are a secondary, moderation-level concern rather than a top-priority elimination.
Is high cholesterol the same as fatty liver disease? No. High blood cholesterol (especially LDL) is a cardiovascular risk marker; fatty liver disease is fat accumulation within liver tissue. They're related — both connected to metabolic dysfunction — but they're distinct conditions, and you can have either one without the other.
Can fatty liver disease be reversed through diet alone? Simple steatosis (early-stage fatty liver) can often improve significantly or resolve with sustained dietary changes and weight loss. Established fibrosis is harder to fully reverse through diet alone and typically requires comprehensive medical management.
How much dietary cholesterol is safe if I have NAFLD? There's no universally agreed-upon "safe number" specific to NAFLD in current guidelines. General population dietary cholesterol moderation (rather than the older, now-relaxed 300mg/day cap) combined with overall diet quality improvement is the more evidence-supported framework discussed by hepatology and nutrition specialists.
Should I stop eating shrimp or shellfish if I have fatty liver disease? Shellfish is relatively high in dietary cholesterol but also low in saturated fat, unlike many other cholesterol sources. Most clinicians would view moderate shellfish intake as lower priority for restriction than ultra-processed foods or sugar-sweetened beverages.
What is HIF-1 and why does it matter for liver health? HIF-1 is a protein your cells activate during low-oxygen stress. Research shows excess dietary cholesterol can inappropriately activate HIF-1 in the liver, contributing to inflammation and disrupted blood flow even when oxygen levels haven't genuinely dropped — making it a researched contributor to NASH progression and a potential future drug target.
Is NASH the same as cirrhosis? No. NASH/MASH is an inflammatory stage that can, over years, progress to fibrosis and eventually cirrhosis if unaddressed — but NASH itself is not yet cirrhosis, and earlier-stage NASH has real potential for improvement with treatment.
Does losing weight reverse fatty liver disease? Yes, in many cases. Weight loss of even 5-10% of body weight has shown measurable improvements in liver fat and inflammation markers in multiple clinical studies, and remains one of the most well-supported interventions available.
Are plant-based diets better for fatty liver disease than diets with meat? Plant-forward, Mediterranean-style eating patterns have the strongest evidence base for NAFLD/MASLD specifically; this doesn't require eliminating meat, but does favor reducing processed and red meat in favor of fish, legumes, vegetables, and healthy fats.
Can I take fish oil or omega-3 supplements to help my fatty liver? Some research suggests substituting omega-6-heavy fats with omega-3s may help counter inflammatory pathways implicated in NASH progression, but you should discuss supplementation with your doctor, particularly regarding dosing and any interactions with existing medications.
Is the new term MASLD replacing NAFLD completely? Yes, MASLD (and MASH) are the updated clinical terms adopted in 2023 by major hepatology associations, though "NAFLD" and "NASH" remain widely used in older research, patient materials, and everyday conversation during this transition period.
Conclusion & Action Steps
Dietary cholesterol isn't an isolated villain in fatty liver disease, but it's also not the harmless non-issue some sources suggest. The evidence — consistent across multiple independent animal studies and mechanistic research — shows that in the presence of existing fat accumulation or metabolic dysfunction, excess dietary cholesterol meaningfully accelerates the journey from simple fatty liver to NASH/MASH, partly through inappropriate HIF-1 activation and damage to the liver's microcirculation.
Your practical next steps:
Get clarity on your actual liver status — ask your doctor about liver enzymes, imaging, and fibrosis staging if you haven't already.
Shift toward a Mediterranean-style eating pattern, rather than fixating on eliminating any single nutrient.
Cut sugar-sweetened beverages first — it's the highest-leverage, lowest-effort change available.
Moderate, don't eliminate, cholesterol-containing whole foods, while reducing ultra-processed foods and excess industrial seed oils.
Don't stop a prescribed statin out of liver fear — talk to your doctor first; the evidence supports their safety in MASLD.
Revisit your progress with bloodwork or imaging, not just how you feel, since liver inflammation can be present without obvious symptoms.
If you found this breakdown useful, consider exploring our companion guides on [Mediterranean diet meal planning for liver health], [understanding your liver enzyme test results], and [exercise protocols shown to reduce liver fat] for a more complete picture of managing NAFLD/MASLD.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Individual circumstances vary, and treatment decisions should always be made in consultation with qualified healthcare professionals.
Related Articles
Why Your Scale Isn’t Moving: The Science of Fat Burning Beyond Weight Loss | DR T S DIDWAL
How Glycemic Index and Glycemic Load Influence Type 2 Diabetes | DR T S DIDWAL
The Metabolic Triad: Why Diabetes, Obesity & CVD Are One Epidemic | DR T S DIDWAL
Sources & References
Pereira, E.N.G.d.S., Araujo, B.P.d., Rodrigues, K.L., Silvares, R.R., Guimarães, F.V., Martins, C.S.M., Flores, E.E.I., Silva, P.M.R.e., & Daliry, A. (2023). Cholesterol Exacerbates the Pathophysiology of Non-Alcoholic Steatohepatitis by Upregulating Hypoxia-Inducible Factor 1 and Modulating Microcirculatory Dysfunction. Nutrients, 15(24), 5034. https://doi.org/10.3390/nu15245034
Subramanian, S., Goodspeed, L., Wang, S., Kim, J., Zeng, L., Ioannou, G.N., Haigh, W.G., Yeh, M.M., Kowdley, K.V., O'Brien, K.D., Pennathur, S., & Chait, A. (2011). Dietary cholesterol exacerbates hepatic steatosis and inflammation in obese LDL receptor-deficient mice. Journal of Lipid Research, 52(9), 1626–1635. https://doi.org/10.1194/jlr.M016246
Ishizuka, K., Kon, K., Lee-Okada, H.C., Arai, K., Uchiyama, A., Yamashina, S., Yokomizo, T., & Ikejima, K. (2020). Aging exacerbates high-fat diet-induced steatohepatitis through alteration in hepatic lipid metabolism in mice. Journal of Gastroenterology and Hepatology, 35(8), 1437–1448. https://doi.org/10.1111/jgh.15006
Zhou, M-T., Song, X-Z., Yang, L., Fang, Y-H., Liu, L., Cui, J-S., Lu, X-C., Zhu, H-Y., Jin, Y-B., & Han, H-M. (2025). High intake of n-6 polyunsaturated fatty acid exacerbates non-alcoholic steatohepatitis by the involvement of multiple metabolic pathways. Frontiers in Nutrition, 12:1562509. https://doi.org/10.3389/fnut.2025.1562509
Xiang, M., Tian, X., Wang, H., Gan, P., & Zhang, Q. (2024). Inappropriate Diet Exacerbates Metabolic Dysfunction-Associated Steatotic Liver Disease via Abdominal Obesity. Nutrients, 16(23), 4208. https://doi.org/10.3390/nu16234208
Jonas, W., Gottmann, P., Jähnert, M., Baer, N., Schürmann, A., & Vogel, H. (2026). Cholesterol-rich diet exacerbates steatohepatitis in the STAM mouse model. Scientific Reports, 16, 11231. https://doi.org/10.1038/s41598-026-45979-z
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), & European Association for the Study of Obesity (EASO). (2024). EASL–EASD–EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Journal of Hepatology, 81, 492–542.
American Association for the Study of Liver Diseases (AASLD). (2025). AASLD Practice Guidance Update on MASLD/MASH Treatment.
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Definition & Facts of NAFLD & NASH. https://www.niddk.nih.gov
American Liver Foundation. NAFLD Overview and Dietary Guidance. https://liverfoundation.org
Mayo Clinic. Nonalcoholic fatty liver disease — Symptoms and causes. https://www.mayoclinic.org
Cleveland Clinic. Fatty Liver Disease: Causes, Symptoms & Treatment. https://my.clevelandclinic.org
Harvard T.H. Chan School of Public Health. The Nutrition Source: Liver Health. https://www.hsph.harvard.edu/nutritionsource
Younossi, Z.M., et al. (2023). Global epidemiology of nonalcoholic fatty liver disease. Hepatology.
Rinella, M.E., et al. (2023). A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology / Journal of Hepatology.
Note: Sources 9–15 represent the categories of additional high-authority clinical and governmental references appropriate for this topic; please verify current URLs and most recent publication dates before final publication, as guideline pages are periodically updated.