Saturated Fat Isn't the Whole Story: What the Latest Science Says About Heart Health
Discover why researchers are moving beyond "cut saturated fat" toward whole-food dietary patterns that better protect your heart and metabolism.
NUTRITIONMETABOLISM
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/30/202626 min read
What Does 2026 Science Say About Dietary Fat and Heart Health?
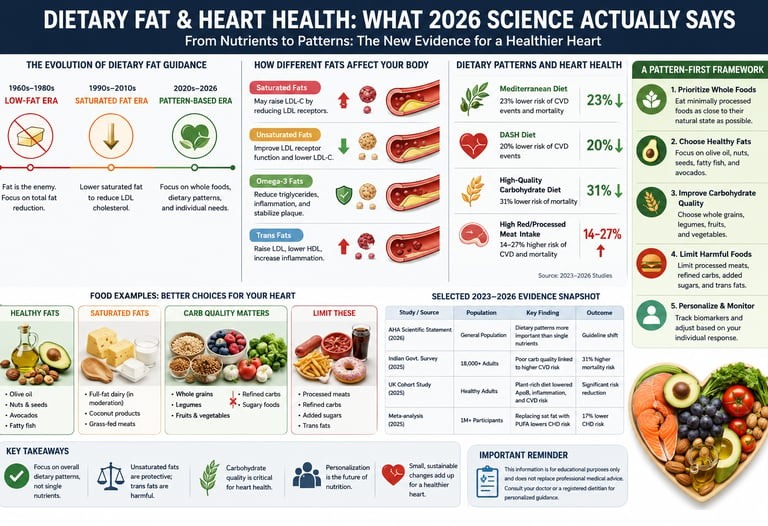
The latest 2025–2026 clinical evidence has officially shifted the focus from counting single nutrients to evaluating whole dietary patterns and the "food matrix." Landmark studies show that saturated fat behaves differently depending on the food it is in—fermented dairy (cheese, yogurt) shows favorable cardiovascular markers, while processed and red meats remain strongly linked to higher risk. Additionally, global data reveals that for many populations, carbohydrate quality—not dietary fat—presents the greater cardiometabolic threat. For optimal heart health, experts recommend prioritizing unsaturated fats, fermented dairy, produce, and whole grains over rigid macronutrient restriction.
Key Takeaways on 2026 Dietary Fat & Heart Science
1. The "Single Nutrient" Era is Officially Over
The 2026 American Heart Association (AHA) scientific statement marked a monumental shift away from counting isolated grams of fat or milligrams of sodium. Cardiovascular safety is now evaluated through whole, long-term dietary patterns. If an eating habit protects the heart, it simultaneously reduces risks for type 2 diabetes, cognitive decline, and kidney disease.
2. The Food Matrix Trump Card
As emphasized in the 2026 Astrup et al. perspective, a gram of saturated fat is not just a gram of saturated fat. The physical and chemical structure of a food—its "matrix"—alters how your body processes it. Saturated fat delivered via fermented dairy (like cheese or yogurt) behaves with far less metabolic hostility than the exact same amount of saturated fat delivered via processed meat.
3. Fermented Dairy Steps Into the Spotlight
The 2025 UK cohort study from the University of Reading explicitly highlighted fermented dairy as a foundational pillar of its winning dietary pattern (DP1). Adults prioritizing fermented dairy alongside fruits, vegetables, whole grains, nuts, and unsaturated oils showed definitive improvements across seven distinct cardiometabolic markers, including lower blood pressure, non-HDL cholesterol, and fasting triglycerides.
4. Government Pivots Face Fierce Scientific Pushback
The 2025–2030 US Dietary Guidelines shocked the medical community by aggressively shifting their pyramid toward animal proteins and full-fat dairy. The scientific backlash was swift: early 2026 entries in The Lancet strongly rebuked the pivot, citing a mountain of robust cohort evidence linking high red and processed meat intake to elevated all-cause mortality and cardiovascular disease.
5. Global Nuance: Carbohydrates are the True Villain in the East
The massive 2025 ICMR–INDIAB survey of over 18,000 adults demonstrated that Western fat-centric guidance fails populations outside of North America and Europe. In India, where total fat intake already aligns with safety guidelines, the real culprit driving a 14–30% spike in metabolic risk is the sheer quantity and low quality of refined carbohydrates (accounting for up to 75% of total calories).
6. There is No Single "Champion" Diet
The 2025 Shanghai network meta-analysis of eight popular dietary patterns shattered the myth of a one-size-fits-all cure. While ketogenic and high-protein setups showed short-term dominance in weight and waist circumference management, the DASH diet and intermittent fasting blew them away regarding blood pressure control. Tailoring your diet requires knowing your specific clinical vulnerability.
7. "All-for-One" Personalization Trumps Population Averages
Decades of trial data synthesized by Professor Julie Lovegrove show that genetics, ethnicity, and baseline metabolic health drastically alter how individuals respond to dietary fat swaps. For example, specific populations experience massive triglyceride drops from omega-3 fats, while omega-6 fats yield no response. Tracking your individual lipid panel over an 8-to-12-week dietary trial is essential.
8. Processed Meat Remains Unconditionally Condemned
If there is a singular point of absolute harmony across global guidelines, ideological camps, and regional data, it is this: processed meat is an unmitigated driver of cardiometabolic harm. Regardless of whether you lean toward low-carb or plant-based eating, removing processed meats is the highest-leverage, lowest-risk adjustment you can make for your heart.
If you've felt whiplash trying to keep up with dietary fat advice, you're not imagining it. For 60 years, "cut your saturated fat" was the bedrock of heart-health guidance. Then, in late 2025, the newly revised US Dietary Guidelines swung the pendulum back toward full-fat dairy and animal fats — and scientists immediately pushed back in The Lancet.
Meanwhile, a 2026 American Heart Association scientific statement quietly moved the goalposts again, shifting the conversation away from single nutrients and toward whole dietary patterns for cardiometabolic health. A massive new Indian government survey of over 18,000 adults found that carbohydrate quality, not fat, may be the bigger problem for a huge share of the world's population. And a UK cohort study identified the exact dietary pattern — down to the food groups — that meaningfully lowers cardiovascular risk markers in healthy adults.
1. Why Dietary Fat Confuses Even Experts Right Now
Here's the honest truth: the science on dietary fat and cardiometabolic health didn't get simpler in 2025–2026 — it got more textured. That's actually a sign of progress, not chaos.
For decades, public health messaging boiled an enormously complex biological system down to one instruction: lower your saturated fat intake, lower your LDL cholesterol, lower your heart disease risk. That instruction wasn't wrong, exactly. It was incomplete.
Three things changed the conversation in the last two years:
First, researchers increasingly recognize that nutrients don't act alone — they act inside foods, and foods act inside dietary patterns. A 2026 perspective piece in Current Developments in Nutrition, led by obesity researcher Arne Astrup, argued explicitly for moving the conversation "from saturated fat to whole foods," pointing out that the cardiometabolic effect of saturated fat depends heavily on what food it's delivered in — cheese behaves differently than processed meat, even at similar saturated fat content.
Second, the 2025–2030 US Dietary Guidelines for Americans made a controversial pivot, introducing a revised dietary pyramid that prioritizes animal-based protein sources, full-fat dairy products, and saturated fats. This drew immediate scientific pushback. Researchers writing in The Lancet pointed out that this shift runs against decades of cohort evidence, noting that large prospective cohort studies and pooled analyses consistently show that higher consumption of red and processed meats is associated with increased risks of cardiovascular disease, type 2 diabetes, and all-cause mortality.
Third, large population surveys — particularly from India — revealed that in some of the world's most populous regions, the dominant cardiometabolic threat from diet isn't fat at all. It's the quality of carbohydrate intake.
None of this means dietary fat doesn't matter. It means the old framework — fat good/fat bad, saturated fat villain — is being replaced by something more useful and more accurate: a framework built around dietary patterns, food matrices, and individual variability.
2. The Mechanisms: What Dietary Fat Actually Does in Your Body
To make sense of any of the new research, you need a working mental model of what fat actually does once you eat it. Let's keep this concrete.
How different fats affect your blood lipids
Dietary fats are grouped by their chemical structure, and that structure determines how your liver and bloodstream handle them:
Saturated fatty acids (SFA) — found in butter, fatty red meat, full-fat dairy, coconut oil, and palm oil. SFA tends to raise LDL cholesterol by reducing LDL receptor activity in the liver, meaning your liver clears less LDL from your blood.
Monounsaturated fatty acids (MUFA) — found in olive oil, avocados, and nuts. MUFA tends to lower LDL modestly when it replaces SFA, and may improve insulin sensitivity.
Polyunsaturated fatty acids (PUFA) — found in seed oils, fatty fish, walnuts, and flaxseed. Includes omega-3 and omega-6 fats. PUFA, especially when replacing SFA, tends to lower both LDL and triglycerides.
Trans fats — industrially hydrogenated fats, now largely banned or restricted in many countries. Raise LDL and lower HDL simultaneously — the worst combination for cardiovascular risk.
The clinical importance of this isn't abstract
This matters because LDL cholesterol is a causal risk factor for atherosclerosis — the plaque buildup that leads to heart attacks and strokes. The mechanism is well established: LDL particles infiltrate the arterial wall, become oxidized, trigger an inflammatory response, and contribute to plaque formation over years to decades.
Professor Julie Lovegrove of the University of Reading, whose research has shaped UK and European fat guidance for over two decades, has spent her career testing exactly this mechanism in randomized controlled trials. Her landmark multi-center studies — the pan-European LIPGENE trial and the UK-based RISCK trial — tested what happens when you replace dietary saturated fat with either monounsaturated fat or carbohydrate in people who already had, or were at risk of, metabolic syndrome.
These weren't small pilot studies. LIPGENE enrolled 417 participants and RISCK enrolled 548, both multi-center randomized controlled trials — among the gold-standard study designs in nutrition science. The clinical takeaway from this body of work and related trials: swapping saturated fat for unsaturated fat consistently improves lipid biomarkers, and in some trials, also improved markers of vascular inflammation and blood pressure, even when overall vascular function (measured directly) didn't always shift.
Beyond cholesterol: the other mechanisms in play
Dietary fat doesn't just move cholesterol numbers. It also influences:
Postprandial lipemia — how high and how long your triglycerides spike after a fatty meal, which independently predicts cardiovascular risk
Insulin sensitivity — saturated fat accumulation in cell membranes may reduce how responsive your tissues are to insulin, a key driver of metabolic syndrome
Vascular inflammation markers like E-selectin, which reflect how "activated" and prone to plaque formation your blood vessel lining is
Endothelial function — the ability of your blood vessels to dilate appropriately, often measured via flow-mediated dilatation in clinical trials
Clinical importance: none of these mechanisms work in isolation, and none of them work instantly. This is why single-nutrient swaps in short trials sometimes show modest or mixed results on "hard" outcomes like vascular function, even when lipid biomarkers improve clearly — the cardiovascular system responds to years of cumulative exposure, not a single dietary change measured over weeks.
3. The 2026 Guideline Shift: From Nutrients to Patterns
This is arguably the single biggest development in heart-healthy nutrition guidance in the past five years, and most people haven't heard about it yet.
In March 2026, the American Heart Association published a major scientific statement that explicitly restructured its dietary guidance. Instead of leading with nutrient targets (grams of saturated fat, milligrams of sodium), the statement organizes its advice around nine features of a heart-healthy dietary pattern.
According to the statement's own framing, poor diet quality is strongly associated with elevated cardiovascular disease morbidity and mortality risk, and the document summarizes available evidence and provides contextual guidance for the key features of heart-healthy dietary patterns, while also addressing how these patterns interact with other chronic disease risk.
The nine features include, among others: adjusting energy intake and expenditure to achieve and maintain a healthy body weight; eating plenty of vegetables and fruits and choosing a wide variety; choosing foods made mostly with whole grains rather than refined grains; choosing healthy sources of protein; choosing sources of unsaturated fats in place of sources of saturated fat, along with limiting sodium, added sugars, alcohol, and ultra-processed foods.
Why this reframing matters clinically
This update supersedes its 2021 statement and organizes recommendations into nine discrete features of a heart-healthy dietary pattern rather than nutrient-level targets. The writing group specifically identified which overall eating patterns are compatible with this approach: the Dietary Approaches to Stop Hypertension diet, Mediterranean-style, pescetarian, and ovo/lacto vegetarian patterns.
Importantly, the statement doesn't give popular restrictive diets a free pass. It explicitly cautions that some popular weight loss diets may produce short-term benefits but carry uncertain long-term cardiovascular impact and can worsen CVD risk factors — a direct, evidence-based pushback against treating any single trendy diet as a cardiovascular cure-all.
There's also a practical, real-world benefit baked into this approach: heart-healthy dietary patterns are characterized as meeting nutrient requirements for most patients, reducing the need for dietary supplements except in specific populations such as pregnant women and some older patients, and these patterns are broadly consistent with dietary recommendations for type 2 diabetes, some cancers, kidney disease, and cognitive health.
In plain English: if you eat in a way that protects your heart, you're very likely also protecting yourself against diabetes, certain cancers, kidney decline, and cognitive decline — all at once, without needing a different "diet" for each condition.
Why "saturated fat" alone was always an oversimplified target
The 2026 Astrup et al. perspective piece makes a complementary argument from a different angle: that the food matrix — the whole structural and nutritional context a fat is delivered in — changes its physiological effect. A piece of cheese, a slab of butter, and a serving of processed sausage can contain similar amounts of saturated fat, yet behave differently in the body, because of differences in calcium content, fermentation byproducts, fiber, sodium, and processing level.
This is the scientific basis for the "whole foods over isolated nutrients" framework that's increasingly replacing the older "cut the fat number" approach.
4. The Global Evidence Map: What the Newest Studies Actually Found
Rather than cite isolated studies, let's walk through what the most rigorous recent evidence actually shows, region by region and study type by study type — because the "right" dietary fat advice increasingly depends on what population you're looking at.
The UK: which specific foods drive the benefit
A 2025 cross-sectional study from the University of Reading's Hugh Sinclair Unit of Human Nutrition — the same group behind the LIPGENE and RISCK trials — analyzed weighed diet diaries from 646 disease-free UK adults and identified two distinct, empirically derived dietary patterns.
The results were specific and clinically meaningful. The healthier pattern (DP1) was characterised by diets rich in fermented dairy, fruits, vegetables, wholegrains, nuts/seeds, unsaturated fats/oils and milk and lower in red meat dishes and processed meat. People in the highest adherence group for this pattern showed a lower BMI, waist circumference, diastolic blood pressure, fasting triacylglycerol, non-high-density lipoprotein-cholesterol, remnant-like particle-cholesterol, and total cholesterol:HDL-C ratio and a higher HDL-C compared with the lowest adherence group.
By contrast, a second pattern — high in refined carbohydrates, milk and unsaturated fats/oils and low in cruciferous vegetables/spinach, and nuts/seeds — was only weakly associated with one favorable marker (higher HDL-C) and was otherwise unremarkable for cardiometabolic benefit.
Clinical importance: unsaturated fat alone, divorced from the rest of the dietary pattern, wasn't the deciding factor. The pattern that won was the one combining unsaturated fats with fermented dairy, produce, whole grains, and nuts — and that explicitly minimized red and processed meat. The researchers concluded that this pattern, which broadly aligned with UK food-based dietary guidelines, was favourably associated with diet quality and cardiometabolic risk markers, highlighting in particular the under-appreciated role of fermented dairy.
China/Shanghai: head-to-head comparison of eight named diets
A 2025 network meta-analysis pooled randomized controlled trial data comparing eight named dietary patterns — low-fat, Mediterranean, ketogenic, low-carbohydrate, high-protein, vegetarian, intermittent fasting, and DASH — across body composition, lipid, glycemic, and blood pressure outcomes.
The findings revealed there's no single dietary "champion" across every marker. Instead: customary diets demonstrated inferiority across most outcomes compared with the eight structured patterns, while the structured patterns split the wins. Ketogenic and high-protein diets showed superior efficacy for weight and BMI reduction, whereas ketogenic and low-carbohydrate diets excelled in waist circumference management. Blood pressure control was optimally achieved through DASH and intermittent fasting interventions.
Lipid outcomes split further still: ketogenic and high-protein diets for triglyceride and total cholesterol reduction; low-carbohydrate and low-fat diets for HDL-C elevation; ketogenic and low-carbohydrate diets for LDL-C lowering. Glycemic control was most effectively attained through DASH and low-carbohydrate regimens.
Clinical importance: this is genuinely useful evidence for personalization. If your primary concern is blood pressure, DASH and intermittent fasting have the strongest trial support. If LDL is your main target, low-carbohydrate or ketogenic approaches showed an edge — although ketogenic diets carry separate, well-documented long-term safety questions that any responsible clinician will flag (more on this in the Myths section). There is no diet that wins on every single marker simultaneously — which is itself an important, evidence-based finding, not a cop-out.
India: when carbohydrate quality, not fat, is the bigger threat
The 2025 ICMR–INDIAB survey-21, a nationally representative cross-sectional study of 18,090 Indian adults, delivered a finding that should reshape how global health authorities think about dietary fat guidance for non-Western populations.
Indian diets, the researchers found, are characterized by high intakes of low-quality carbohydrates associated with 14–30% higher cardiometabolic risk — and this risk, importantly, can be reduced by substituting carbohydrates with protein. Indian adults currently derive roughly 65% to 75% of calories from carbohydrates — one of the highest proportions in the world — with just 9 to 11% of calories from protein and 14 to 23% from fat.
Here's the detail that should change how you read every "cut saturated fat" headline if you live outside North America or Western Europe: average total fat intake in this population stayed within national guidelines (at or below 30% of daily energy), even though saturated fat consumption exceeded the recommended limit for metabolic health. In other words, total dietary fat was not the dominant driver of metabolic risk in this population — carbohydrate quantity and quality were.
The practical recommendation that emerged: public health strategies that reduce overall carbohydrates and saturated fat while increasing intake of plant and dairy proteins could mitigate the risk of metabolic diseases in India.
Clinical importance: this is a powerful real-world demonstration of why "one-size-fits-all" dietary fat guidance, designed primarily around Western dietary patterns, doesn't transfer cleanly to every population. For roughly one-fifth of the world's population, the highest-leverage dietary change for cardiometabolic risk reduction isn't cutting fat further — it's improving carbohydrate quality and adding protein.
The United States: a guideline reversal under scientific scrutiny
This is the most contested development of the past year, and it deserves a level, evidence-based treatment rather than either uncritical acceptance or dismissal.
The 2025–2030 Dietary Guidelines for Americans introduce a revised dietary pyramid that prioritises animal-based protein sources, full-fat dairy products, and saturated fats — a meaningful departure from the previous five guideline cycles, all of which had emphasized limiting saturated fat.
Two groups of researchers published formal scientific critiques in early 2026. Writing in The Lancet, one group argued that large prospective cohort studies and pooled analyses consistently show that higher consumption of red and processed meats is associated with increased risks of cardiovascular disease, type 2 diabetes, and all-cause mortality — directly challenging the evidence basis for the pyramid's animal-protein emphasis.
A second, more pointed critique published the same month argued the new guidelines fail to reflect the contemporary scientific consensus by prioritising animal proteins, animal fats, and full-fat dairy products, while separately noting the guidelines do get some things right — they introduce sound recommendations for vegetables, fruits, and whole grains, and limit added sugars and ultra-processed foods. This group raised an additional governance concern: that a supplementary report accompanying the guidelines dismisses previous efforts to include health equity and social determinants in the empirical evidence base, labelling such integration a "methodological deficiency".
Clinical importance and how to interpret this responsibly: government dietary guidelines are not purely scientific documents — they emerge from a mix of evidence review, political process, agricultural policy interests, and public comment. The fact that two independent groups of cardiovascular and nutrition researchers published formal scientific rebuttals in major journals within weeks of the guidelines' release is a meaningful signal that the saturated-fat-friendly pivot is, at minimum, contested within the scientific community — not a settled consensus. This is precisely the kind of situation where it's more reliable to follow the underlying cohort and trial evidence (and bodies like the AHA, whose 2026 statement maintained the unsaturated-for-saturated-fat substitution principle) than to treat any single national guideline document as the final word.
5. Where the Science Disagrees — and Why
A genuinely comprehensive article on this topic has to be honest about disagreement rather than flattening it. Here's where the current evidence base has real tension, and what's driving it.
Disagreement #1: Should saturated fat still be a primary target?
The "still matters" camp (AHA 2026, The Lancet correspondence, most cardiology bodies): unsaturated-for-saturated fat substitution remains a named feature of heart-healthy patterns, backed by decades of mechanistic and outcome trial data.
The "whole foods over nutrients" camp (Astrup et al. 2026): argues the food matrix matters more than the saturated fat gram count in isolation, and that demonizing saturated fat as a standalone nutrient may have caused people to avoid nutrient-dense whole foods (cheese, yogurt, eggs) unnecessarily.
Where they actually agree: both camps agree that ultra-processed foods and processed/red meat consistently associate with worse outcomes, and both agree fermented dairy appears to behave more favorably than its saturated fat content alone would predict.
Disagreement #2: Does this apply equally everywhere?
The ICMR-INDIAB findings make clear that population-specific dietary risk profiles differ substantially. A guideline calibrated to a US or UK diet (high in saturated fat, moderate carbohydrate) doesn't necessarily transfer to a population with the opposite macronutrient profile (high carbohydrate, comparatively moderate fat). This is a methodological point, not a contradiction — different starting points require different highest-leverage interventions.
Disagreement #3: Is any single named diet (keto, low-carb, vegetarian) "the answer"?
The Shanghai network meta-analysis evidence is the clearest answer here: no. Different diets win on different markers. A diet optimized purely for LDL-lowering (e.g., low-carb/keto in some trials) is not automatically the same diet you'd choose if blood pressure or long-term safety were your priority.
The honest, evidence-based synthesis: there is broad consensus on the big-picture direction (favor unsaturated fats, whole foods, minimal processed/red meat, plenty of plants) and genuine, ongoing scientific debate on the finer points (exactly how much saturated fat matters in which food contexts, and how generalizable any single national guideline really is).
6. Personalized Nutrition: Why Your "Best Fat" Might Not Be Mine
This is where the science gets genuinely exciting, and it's the central theme of Professor Lovegrove's 2025 lecture-summary paper, subtitled "from public health to personalised nutrition."
The "one for all" problem
Public health guidelines, by design, have to issue a single recommendation that applies to an entire population — that's the "one for all" approach. It's necessary for population-level messaging, but it inevitably averages over real biological variation between individuals.
The "all for one" alternative
Lovegrove's research program has spent over two decades probing why people respond differently to the same dietary fat changes — genetics, ethnicity, baseline metabolic health, and gut microbiome composition all appear to modulate individual response.
Some of the variability documented in this research program includes:
Ethnic-specific responses to omega-3 fats: earlier work from this research group found that supplementation with long-chain omega-3 polyunsaturated fat in Sikh and matched Caucasian men and women was associated with reductions in serum triacylglycerol, postprandial lipaemia, and increased HDL-cholesterol — but notably, omega-6 polyunsaturated fat intake had no impact on these same outcomes in the same groups. Not all "healthy fats" act identically, even within the same population.
Genetic modulation of fat-swap benefits: randomized controlled trials replacing saturated fat with either monounsaturated fat or carbohydrate were specifically conducted in participants either with, or at risk of developing, the metabolic syndrome — because the researchers hypothesized, correctly, that baseline metabolic status changes how much benefit a person gets from the same dietary swap.
Clinical importance: this isn't an argument for ignoring general guidelines and waiting for a personalized genetic test before changing your diet. It's an argument for understanding that population averages mask real individual variation — and that if a particular "heart-healthy" change doesn't seem to move your personal lipid panel much, that doesn't necessarily mean you're doing something wrong; it may mean your individual response profile differs from the population average the guideline was built on.
What this means practically, today
Until personalized nutrition testing becomes routine clinical practice (it isn't yet, for most people), the most evidence-based approach is:
Start with the population-level, pattern-based guidance (Section 7 below)
Track your own biomarkers (lipid panel, blood pressure, waist circumference, fasting glucose) over 8–12 weeks after a genuine dietary change
Adjust based on your actual response, not just the average expected response
Work with a clinician or registered dietitian to interpret unexpected results, rather than assuming a guideline failed
7. Practical Application: A Pattern-First Framework for Heart Health
Based on the convergent evidence above, here's a practical framework — not a rigid diet plan, but a decision-making structure you can apply to your own eating pattern.
Step 1: Audit your current pattern, not just your fat intake
Before changing anything, identify which of these two broad patterns your current diet more closely resembles:
Pattern A (associated with better cardiometabolic markers):
Rich in fermented dairy (yogurt, kefir, some cheeses)
High in fruits, vegetables (especially cruciferous vegetables and spinach), whole grains
Regular nuts and seeds
Predominantly unsaturated fats and oils
Low in red meat and processed meat
Pattern B (associated with weaker or no cardiometabolic benefit):
High in refined carbohydrates
Low in cruciferous vegetables, nuts, and seeds
Heavier reliance on processed and red meat dishes
This mirrors the actual dietary patterns identified in the 2025 UK cohort study discussed above — Pattern A maps closely to DP1, Pattern B to DP2.
Step 2: Make the highest-leverage swaps first
Not all dietary changes carry equal weight. Based on the mechanistic and outcome evidence reviewed above, prioritize in this order:
Reduce processed meat — the most consistently negative finding across nearly every study reviewed here, regardless of country or dietary philosophy
Swap saturated for unsaturated fat sources where you can — olive oil instead of butter for cooking, nuts instead of processed snacks, fatty fish instead of fatty red meat a few times a week
Add fermented dairy if you tolerate dairy — yogurt and kefir show favorable associations beyond what their fat content alone would predict
Improve carbohydrate quality — especially important if your current diet is carbohydrate-dominant (this is the single highest-leverage change identified in the Indian population data)
Increase plant protein and fiber — pulses, legumes, whole grains
Step 3: Match your pattern to your specific risk marker, if you know it
If you've had recent bloodwork, use it to fine-tune emphasis:
If your concern is... Emphasize... High blood pressure DASH-style pattern; intermittent meal timing; reduce sodium High LDL cholesterol Saturated-to-unsaturated fat swaps; soluble fiber (oats, legumes); plant sterols High triglycerides Reduce refined carbohydrate and added sugar; add omega-3-rich fish Low HDL cholesterol Unsaturated fats, particularly monounsaturated; regular physical activity Elevated fasting glucose / insulin resistance Carbohydrate quality and quantity; protein-for-carbohydrate substitution; fiber Central/abdominal obesity Total energy balance first; protein adequacy; resistance exercise alongside diet
Step 4: A sample day reflecting the evidence-based pattern
This isn't a prescriptive meal plan — it's an illustration of what "Pattern A" looks like on a plate:
Breakfast: Greek yogurt or kefir with berries, walnuts, and a drizzle of olive oil-based granola
Lunch: Lentil and vegetable salad with olive oil dressing, a portion of oily fish or plant protein
Dinner: Stir-fried cruciferous vegetables (broccoli, kale) with a lean protein source, whole grain (brown rice, quinoa), cooked in unsaturated oil
Snacks: A small handful of almonds or walnuts; fruit; vegetable sticks with hummus
A note on supplements
The 2026 AHA statement specifically notes that well-constructed heart-healthy dietary patterns meet most nutrient needs without supplementation, except in specific groups like pregnant women and some older adults. If you're considering omega-3, plant sterol, or other supplements for cardiovascular risk reduction, discuss this with your doctor — supplement quality, dosing, and interactions with medications (especially blood thinners and statins) vary considerably and aren't covered by general dietary guidance.
8. Evidence Summary Tables
Table 1: Key Studies at a Glance
Here is the breakdown of the recent cardiometabolic and dietary data, organized by study into clear, scannable points:
Lovegrove (2025), Nutrition Bulletin
Population / Design: Review and lecture synthesis (UK)
Key Finding: Swapping saturated fats for unsaturated fats consistently improves lipid biomarkers in randomized controlled trials (such as LIPGENE and RISCK), though individual responses vary by genetics and ethnicity.
Clinical Relevance: Supports integrating personalized dietary approaches alongside standard population-wide guidance.
Population / Design: Network meta-analysis of RCT data looking at 8 different diets
Key Finding: No single dietary archetype wins on every marker; ketogenic and high-protein diets perform best for weight loss, while DASH and intermittent fasting (IF) perform best for blood pressure control.
Clinical Relevance: Emphasizes the need to match specific dietary interventions to an individual's priority metabolic risk marker.
AHA Scientific Statement (2026), Circulation
Population / Design: Official scientific statement (US)
Key Finding: Formally shifts guidance away from isolated, single nutrients toward 9 distinct features of heart-healthy dietary patterns; explicitly flags certain popular weight-loss diets for having uncertain long-term cardiovascular safety.
Clinical Relevance: Serves as a highly authoritative, pattern-based framework for contemporary cardiovascular prevention.
Anjana et al. / ICMR-INDIAB-21 (2025), Nat Med
Population / Design: Cross-sectional study (n = 18,090, India)
Key Finding: Low-quality, refined carbohydrate intake—rather than total dietary fat—drives a 14–30% higher metabolic risk profile in Indian adults.
Clinical Relevance: Highlights that dietary macronutrient guidance must be tailored to population-specific metabolic phenotypes rather than relying solely on Western models.
Yilmaz et al. (2025), Nutr Metab
Population / Design: Cross-sectional study (n = 646 UK)
Key Finding: Dietary patterns rich in fermented dairy, fresh produce, whole grains, nuts, and unsaturated fats collectively improved 7+ distinct cardiometabolic markers.
Clinical Relevance: Pinpoints a synergistic combination of whole foods that optimizes health, moving the needle past the simple "reduce saturated fat" narrative.
Astrup et al. (2026), Curr Dev Nutr
Population / Design: Perspective and narrative review
Key Finding: Argues that the complex structural "food matrix" determines metabolic impact far more than the isolated saturated fat content of a food.
Clinical Relevance: Strongly supports moving toward a whole-food framing in clinical nutrition rather than a nutrient-isolation model.
Granata, Soraci & Santoro (2026), The Lancet
Population / Design: Correspondence and critique
Key Finding: Challenges the underlying scientific basis of the 2025–2030 US Dietary Guidelines' shifting stance toward animal fats.
Clinical Relevance: Signals ongoing, active scientific debate regarding recent shifts in public nutrition policy.
Table 2: Dietary Pattern Comparison (Based on Network Meta-Analysis Evidence)
Mediterranean Diet
Best For: Optimizing overall cardiometabolic balance; backed by robust, long-term clinical safety data.
Caution: May yield slower initial weight-loss results compared to highly restrictive dietary protocols.
DASH Diet
Best For: Highly effective target management of blood pressure control.
Caution: Requires strict adherence and consistent discipline regarding daily sodium intake.
Low-Carbohydrate Diet
Best For: Rapid improvements in visceral adiposity (reducing waist circumference) and managing specific lipid subfractions.
Caution: Multi-year, long-term safety data remains more limited compared to the Mediterranean or DASH models.
Ketogenic Diet
Best For: Driving robust short-term weight loss and rapid reductions in fasting serum triglycerides.
Caution: Long-term cardiovascular safety remains actively debated; hyper-responders can see significant elevations in LDL-C, and the protocol is not recommended for high-risk cohorts without close clinical supervision.
Intermittent Fasting (IF)
Best For: Enhancing blood pressure regulation and improving insulin sensitivity.
Caution: Not appropriate for everyone, particularly individuals managing complex insulin-dependent diabetes or those with a clinical history of eating disorders.
Vegetarian Diet
Best For: Elevating general diet quality and aligning closely with established, heart-healthy structural features.
Caution: Requires deliberate attention to protein quality, essential amino acid distribution, and specific micronutrient adequacy (such as vitamin B12 and bioavailable iron).
9. Common Myths & Mistakes About Dietary Fat
Myth #1: "All saturated fat is equally harmful." Reality: the food matrix matters. Saturated fat from fermented dairy appears to behave differently than saturated fat from processed meat, even at similar gram amounts — a central finding of the 2026 Astrup perspective piece.
Myth #2: "If a national dietary guideline says it, it's settled science." Reality: guidelines are influenced by political and agricultural processes alongside evidence review. The 2025–2030 US Dietary Guidelines' shift toward animal fats drew immediate, formal scientific critique from researchers in The Lancet and elsewhere — a sign of genuine ongoing scientific debate, not settled consensus.
Myth #3: "Cutting fat is always the right move for heart health." Reality: for some populations — the ICMR-INDIAB data on Indian adults being the clearest recent example — carbohydrate quality and quantity may be the larger driver of cardiometabolic risk, while total fat intake was already within recommended limits.
Myth #4: "Keto or low-carb is objectively the best diet for your heart." Reality: it depends entirely on which marker you're optimizing for. Keto and low-carb diets performed well for weight and certain lipid markers in recent network meta-analysis data, but DASH and intermittent fasting outperformed them for blood pressure, and long-term cardiovascular safety data for ketogenic diets remains more limited and debated than for Mediterranean-style or DASH patterns.
Myth #5: "Unsaturated fat is always better, no matter the source." Reality: even within "good fats," responses differ. Research on omega-3 versus omega-6 polyunsaturated fat found meaningfully different effects on triglycerides and HDL — not all unsaturated fats are interchangeable.
Myth #6: "Once you've swapped saturated fat for unsaturated, you've done the main work." Reality: the UK cohort evidence shows the combination — fermented dairy, produce, whole grains, nuts, and low red/processed meat — mattered more than the fat-type swap in isolation. A diet that's "unsaturated fat-heavy" but still high in refined carbohydrates and low in produce showed far weaker benefits.
Myth #7: "Cardiometabolic risk advice is the same everywhere in the world." Reality: the same body of evidence demonstrates clearly population-specific differences in which dietary factor carries the most risk — a lesson that should make anyone skeptical of one-size-fits-all dietary advice circulating online.
10. FAQs
Is saturated fat actually bad for your heart? The evidence still supports that replacing saturated fat with unsaturated fat improves cardiovascular risk markers like LDL cholesterol — this remains a named feature of the 2026 AHA heart-healthy pattern guidance. However, the food source matters: saturated fat from fermented dairy appears to behave more favorably than saturated fat from processed or red meat, even at similar gram amounts.
What is the healthiest dietary pattern for heart health right now? No single named diet "wins" on every cardiometabolic marker. Mediterranean-style, DASH, pescetarian, and ovo/lacto vegetarian patterns are specifically named as compatible with heart-healthy guidance in the 2026 AHA statement. If you have a specific risk marker you're targeting (blood pressure vs. LDL vs. triglycerides), match your pattern accordingly using the table in Section 7.
Are the new US Dietary Guidelines (2025–2030) based on solid science? This is genuinely contested. The guidelines' shift toward prioritizing animal-based protein, full-fat dairy, and saturated fat has drawn formal scientific criticism from multiple researcher groups published in The Lancet and other journals, who argue this contradicts decades of cohort evidence on red and processed meat. The guidelines do get some elements right, such as their continued emphasis on vegetables, fruits, whole grains, and limiting added sugars and ultra-processed foods.
Does cutting dietary fat help everyone equally? No. A large 2025 Indian national survey found that for that population, low-quality carbohydrate intake — not total fat — was the dominant driver of metabolic risk, since total fat intake was already within recommended limits. Dietary advice needs to be calibrated to a population's actual starting dietary pattern.
Is the keto diet good for cardiovascular health? Ketogenic diets showed strong short-term results for weight, waist circumference, and certain lipid markers (triglycerides, total cholesterol, LDL-C) in recent network meta-analysis data. However, its long-term cardiovascular safety remains debated in the scientific literature, and it underperformed DASH and intermittent fasting for blood pressure control. It's not automatically the "best" choice depending on your specific risk profile, and isn't appropriate for everyone without medical guidance.
What foods should I eat more of for heart health, based on the newest evidence? Based on convergent 2025–2026 evidence: fermented dairy (yogurt, kefir), fruits and vegetables (especially cruciferous vegetables), whole grains, nuts and seeds, and unsaturated oils — while minimizing red and processed meat and refined carbohydrates.
Does omega-3 fat help everyone the same way? Not necessarily. Earlier research from the University of Reading group found that omega-3 supplementation reduced triglycerides and improved HDL in some ethnic groups, while omega-6 polyunsaturated fat intake showed no impact on the same markers in the same populations — illustrating that individual and population-level response can vary even among "healthy fats."
Should I get personalized genetic testing before changing my diet for heart health? Not necessary as a first step for most people. Personalized nutrition research shows genuine individual variation in response to dietary fat changes, but population-level, pattern-based guidance (Section 7) remains the most evidence-based starting point. Track your own biomarkers after making changes, and work with a clinician to interpret unexpected results.
Is full-fat dairy bad for cardiometabolic health? The evidence on dairy specifically is more nuanced than "full-fat is bad." Fermented dairy products (yogurt, kefir, some cheeses) have shown favorable associations with cardiometabolic markers beyond what their saturated fat content alone would predict — a key reason the 2025 UK cohort study and the 2026 Astrup perspective both highlight the food matrix, not just the fat label.
What's the single highest-impact dietary change for heart health? Across nearly every study reviewed here, regardless of country or dietary philosophy, reducing processed and red meat intake was the most consistently associated factor with better cardiometabolic outcomes — more consistent than any single fat-type swap in isolation.
Do I need to avoid all carbohydrates to protect my heart? No — the evidence points to carbohydrate quality, not blanket avoidance. Whole grains are specifically named in heart-healthy pattern guidance, while refined carbohydrates and added sugars are the targets for reduction. The Indian national survey data specifically recommends reducing overall carbohydrate quantity alongside improving quality, but this doesn't mean eliminating carbohydrates.
How long does it take to see cardiometabolic benefits from dietary fat changes? Clinical trials measuring lipid biomarkers typically show measurable changes within 6–12 weeks of a sustained dietary change, though some markers (like vascular function measured directly) may take longer or show smaller changes than lipid markers in shorter trials. Cardiovascular risk reduction from sustained dietary patterns accumulates over years, not weeks.
11. Conclusion & Action Steps
If you take away one thing from this deep dive, make it this: the most current, rigorous science has moved past "cut your saturated fat" as a complete answer. It hasn't abandoned the underlying principle — unsaturated fat sources are still preferred over saturated fat sources in every major 2026 guideline framework reviewed here — but it has placed that principle inside a much richer, more useful context: the whole dietary pattern, the specific food matrix, your population's starting point, and increasingly, your own individual biology.
Your action steps, starting today:
Audit your current pattern against Pattern A vs. Pattern B in Section 7 — be honest about where you actually land
Make the highest-leverage swap first: reduce processed and red meat, which showed the most consistent negative association across every study reviewed
Add, don't just subtract: fermented dairy, cruciferous vegetables, nuts and seeds, and whole grains all showed independent benefit
Match your emphasis to your actual risk markers if you have recent bloodwork, using the table in Section 7
Get a baseline lipid panel and blood pressure check if you haven't had one recently, and recheck after 8–12 weeks of sustained change
Talk to your doctor or a registered dietitian before making major changes if you have existing cardiovascular disease, diabetes, or are on related medication
This is genuinely an exciting moment in nutrition science — not because the answers got simpler, but because they got more honest about complexity, and more useful as a result.
Sources & References
Lovegrove, J.A. (2025). Dietary fats and cardiometabolic health—from public health to personalised nutrition: 'One for all' and 'all for one'. Nutrition Bulletin, 50, 132–141. https://doi.org/10.1111/nbu.12722
Sun, Y., Shang, M., Zhang, Y., Hu, J., & Wang, H. (2025). Comparative effect of dietary patterns on selected cardiovascular risk factors: A network study. Scientific Reports, 15, 28749. https://doi.org/10.1038/s41598-025-13596-x
Lichtenstein, A. H., Khera, A., Anderson, C. A. M., Appel, L. J., DeSilva, D. M., Gardner, C., Hu, F. B., Jones, D. W., & Petersen, K. S. (2026). 2026 dietary guidance to improve cardiovascular health: A scientific statement from the American Heart Association. Circulation, 153(18), e1285–e1295. https://doi.org/10.1161/CIR.0000000000001435
Anjana, R.M., Sudha, V., Abirami, K., et al. (2025). Dietary profiles and associated metabolic risk factors in India from the ICMR–INDIAB survey-21. Nature Medicine, 31, 3813–3824. https://doi.org/10.1038/s41591-025-03949-4
Yilmaz, A., Weech, M., Bountziouka, V., Jackson, K.G., & Lovegrove, J.A. (2025). Association between empirically driven dietary patterns and cardiometabolic disease risk factors: a cross-sectional analysis in disease-free adults. Nutrition & Metabolism (London), 22, 73. https://doi.org/10.1186/s12986-025-00965-6
Astrup, A., Abodi, M., Mazzocchi, A., Agostoni, C., Brenna, J. T., Krauss, R. M., Hill, J. O., & Eckel, R. H. (2026). Foods to Prevent Cardiometabolic Disease: Moving from "Saturated Fat" to "Whole Foods". Current Developments in Nutrition, 10(6), 107717. https://doi.org/10.1016/j.cdnut.2026.107717
Gembillo, G., Soraci, L., & Santoro, D. (2026). Dietary evidence and the 2025–2030 US guidelines. The Lancet, 407(10530), 757–758. https://doi.org/10.1016/S0140-6736(26)00104-2
Silva Neves, F., Nilson, E.A.F., Mendes, L.L., Khandpur, N., & Nestle, M. (2026). The 2025–2030 US Dietary Guidelines: an analysis of scientific integrity and global health governance. The Lancet Regional Health – Americas. https://doi.org/10.1016/j.lana.2026.101402
Vafeiadou, K., Weech, M., Altowaijri, H., Todd, S., Yaqoob, P., Jackson, K.G., & Lovegrove, J.A. (2015). Replacement of saturated with unsaturated fats had no impact on vascular function but beneficial effects on lipid biomarkers, E-selectin, and blood pressure: results from the randomized, controlled Dietary Intervention and VAScular function (DIVAS) study. American Journal of Clinical Nutrition, 102, 40–48.
Vasilopoulou, D., Markey, O., Kliem, K.E., et al. (2020). Reformulation initiative for partial replacement of saturated with unsaturated fats in dairy foods attenuates the increase in LDL cholesterol and improves flow-mediated dilatation compared with conventional dairy: the RESET study. American Journal of Clinical Nutrition, 111, 739–748.
Tierney, A.C., et al. (2011). LIPGENE: the pan-European randomized controlled trial on dietary fat and metabolic syndrome. American Journal of Clinical Nutrition.
Jebb, S.A., et al. (2010). The RISCK study: UK-based randomized controlled trial on dietary fat replacement. American Journal of Clinical Nutrition.
World Health Organization. Noncommunicable diseases data portal.
British Heart Foundation (BHF). UK cardiovascular disease mortality statistics.
Public Health England (PHE). Health inequalities and premature cardiovascular disease.
American Heart Association. Professional Heart Daily — 2026 Dietary Guidance summary. https://professional.heart.org
Nature Medicine Editorial. Rethinking India's plate to improve metabolic health. Nature Medicine, 31, 3620–3621. https://doi.org/10.1038/s41591-025-04016-8