Obesity and Biological Aging: The Hidden Cellular Damage Shortening Your Healthspan
Can weight loss slow biological aging? Discover how obesity accelerates cellular aging and how evidence-based weight loss strategies can improve longevity, healthspan, and metabolic health. (158 characters)
OBESITYAGING
Dr. T.S. Didwal, M.D.(Internal Medicine)
6/16/202619 min read
Research shows obesity accelerates biological aging through chronic inflammation, oxidative stress, cellular senescence, and epigenetic changes. Studies suggest even modest weight loss (5–10%) combined with resistance training and adequate protein intake can improve biological aging markers and extend healthspan.
Key Takeaway
1. Obesity is an Aging Accelerator: Excess body weight doesn’t just increase disease risk; it actively speeds up biological aging at the cellular and molecular level.
2. The Danger of "Zombie Cells": Visceral fat drives chronic systemic inflammation ("inflammaging") and multiplies senescent cells—damaged cells that refuse to die and instead corrupt neighboring healthy tissue.
3. Track "Obesity-Years," Not Just BMI: Much like "pack-years" in smoking, the length of time you carry excess weight dictates the depth of cellular damage and creates a lasting "metabolic memory."
4. BMI is an Incomplete Metric: Standard weight scales hide sarcopenia (muscle loss). True biological age is better tracked through waist circumference, DEXA scans, and functional metrics like grip strength.
5. Modest Loss Yields Major Gains: You do not need a radical transformation to see results. Reversing biological age indicators and reducing inflammation can begin with a sustainable 5% to 10% reduction in total body weight.
6. A "Muscle-First" Approach is Mandatory: Aggressive caloric restriction without muscle protection backfires. The goal must be losing visceral fat while fiercely preserving lean muscle tissue to maintain metabolic youth.
7. Overcoming Anabolic Resistance: To protect aging muscle, individuals pursuing weight loss should prioritize a high-protein diet—targeting 1.2 to 1.6 grams of protein per kilogram of body weight daily.
8. Youthful Regeneration Holds at Any Age: While early intervention in your 20s and 30s offers the highest compounding returns, the body retains remarkable regenerative capacity. Strategic weight management can slow the biological clock at any life stage.
Introduction
Imagine two people born on the same day. At 35, one has maintained a healthy weight and active lifestyle. The other has lived with obesity since their mid-twenties. Their birth certificates say they are the same age—but their cells may tell a very different story.
A rapidly growing body of research now confirms what scientists have long suspected: biological aging is not simply a function of time. It is shaped, profoundly and measurably, by the metabolic environment in which our cells exist. And among the most powerful—yet modifiable—drivers of accelerated biological aging is excess body weight.
This article breaks down the real science linking weight and longevity, interprets what the clinical evidence actually means for real patients, and offers actionable strategies grounded in the best available data. Whether you are 30 or 70, carry 15 extra pounds or 80, the evidence holds a clear and empowering message: what you do with your body composition matters for how long—and how well—you live.
You will learn:
How obesity accelerates aging at the molecular and cellular level
Why how long you carry excess weight matters as much as how much you carry
The emerging science of "obesity-years" and metabolic memory
What modest, sustained weight loss can actually achieve for your biological age
Evidence-based strategies tailored for different life stages
1. Rethinking Obesity: It's Not Just a Disease Risk Factor—It's an Aging Accelerator
For decades, the clinical conversation around obesity has focused primarily on downstream disease: type 2 diabetes, cardiovascular disease, certain cancers, sleep apnea. These associations are real, well-established, and clinically important. But this framing misses something more fundamental.
Obesity does not merely increase the risk of age-related disease—it appears to accelerate the biological aging process itself.
A comprehensive 2023 review published in Endocrinology and Metabolism Clinics of North America (Malandrino et al.) mapped out the endocrine and metabolic pathways through which excess adiposity reshapes inflammation, hormone signaling, cellular repair mechanisms, and gene expression. The conclusion: obesity is not just a comorbidity. It is a driver of the aging biology that underlies almost all chronic disease.
This reframing has important clinical implications. It positions metabolic health as a cornerstone of longevity medicine, not merely a disease prevention strategy.
Clinical Takeaway: Framing obesity as an aging accelerator—rather than just a risk factor—motivates earlier intervention and shifts treatment goals from disease prevention to healthspan optimization.
2. Why BMI Alone Is No Longer Enough
Body Mass Index has been the dominant metric in obesity research and clinical practice for over 50 years. Its appeal is obvious: it is simple, cheap, and correlates reasonably well with population-level health outcomes. But for individual patients—especially older adults—BMI is an increasingly blunt instrument.
A 2025 editorial in The Lancet Healthy Longevity called explicitly for redefining obesity in the context of aging, arguing that traditional BMI cutoffs fail to account for:
Age-related muscle loss (sarcopenia): As lean mass declines with age, total body weight may appear "normal" while body fat percentage is dangerously elevated.
Fat redistribution: Aging shifts fat deposition toward visceral compartments, even at stable body weight—dramatically increasing metabolic and cardiovascular risk.
Functional capacity: A person's ability to walk, climb stairs, or rise from a chair is often more predictive of long-term health outcomes than their weight class.
The editorial called for renewed emphasis on body composition assessment, visceral adiposity measurement, and functional capacity evaluation—tools that better reflect the true burden of obesity in aging populations.
What this means in practice: A 68-year-old woman with a BMI of 27 and low muscle mass, high visceral fat, and poor grip strength may be at considerably higher metabolic risk than her BMI suggests. Conversely, a 55-year-old athlete with a BMI of 29 due to muscle mass may be biologically young and functionally excellent.
Clinical Takeaway: Clinicians and patients alike should look beyond the scale. Waist circumference, DEXA body composition, grip strength, and gait speed provide a far more accurate picture of obesity-related aging risk.
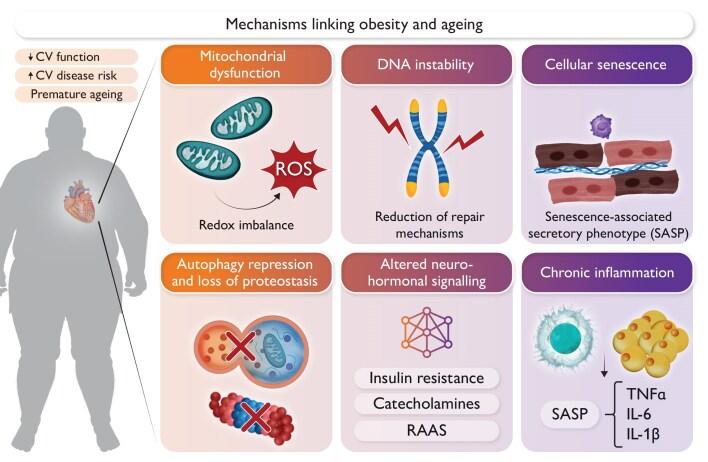
3. The Biological Mechanisms: How Excess Weight Ages Your Cells
Understanding how obesity accelerates aging helps explain why the effects are so pervasive—affecting not just the heart or liver, but cellular biology across the entire body.
3.1 Chronic Low-Grade Inflammation ("Inflammaging")
Visceral adipose tissue is metabolically active. It secretes pro-inflammatory cytokines—including interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α)—creating a state of chronic systemic inflammation that researchers have termed "inflammaging."
This is not acute inflammation (the kind that resolves after an infection). It is a persistent, low-level biological fire that damages tissues throughout the body over years and decades, contributing to endothelial dysfunction, insulin resistance, neurodegeneration, and accelerated cellular senescence.
3.2 Oxidative Stress
Fat cells—particularly those in visceral depots—generate reactive oxygen species (ROS) that damage cellular components including DNA, proteins, and lipid membranes. Over time, this oxidative damage accumulates. DNA repair mechanisms are overwhelmed. Mitochondrial function declines. Cells either die prematurely or shift into a dysfunctional senescent state.
3.3 Hormonal Dysregulation
Obesity disrupts the endocrine system at multiple levels:
Insulin resistance impairs glucose metabolism and promotes compensatory hyperinsulinemia, contributing to vascular aging and cancer risk
Elevated cortisol from chronic metabolic stress accelerates cellular aging
Reduced growth hormone impairs tissue repair and muscle maintenance
Altered sex hormone levels (including estrogen and testosterone) affect bone density, muscle mass, cognitive function, and cardiovascular risk
3.4 Cellular Senescence: The "Zombie Cell" Problem
Perhaps the most compelling mechanism is the accumulation of senescent cells—damaged cells that cease normal function but resist programmed cell death (apoptosis). These cells secrete a cocktail of inflammatory mediators known as the senescence-associated secretory phenotype (SASP), which spreads dysfunction to neighboring healthy cells.
Obesity dramatically increases the senescent cell burden across tissues. Research has demonstrated elevated markers of cellular senescence in adipose tissue, liver, and skeletal muscle of individuals with obesity—and these changes can be detected even in young adults.
Why this matters clinically: Senescent cells are now an active target for longevity medicine. Senolytics (drugs that clear senescent cells) are in clinical trials. But one of the most effective strategies for reducing senescent cell burden may also be one of the oldest: achieving and maintaining a healthy weight.
3.5 Epigenetic Aging
Epigenetic clocks—mathematical models based on DNA methylation patterns at specific genomic sites—can estimate biological age with remarkable precision. Studies using these tools have found that individuals with obesity exhibit accelerated epigenetic aging: their DNA methylation patterns resemble those of people significantly older than their chronological age.
This is not a theoretical construct. It is a measurable, reproducible biological signal that predicts mortality, disease onset, and functional decline independent of chronological age.
4. The Weight of Time: Why Duration of Obesity Matters
A crucial and often overlooked dimension of the obesity-aging relationship is temporal—not just how much excess weight someone carries, but how long they have carried it.
A 2025 study in Aging Clinical and Experimental Research (Ragusa et al.) explored this question directly, introducing the concept of "obesity-years": a cumulative measure of excess weight exposure over time, analogous to "pack-years" in tobacco research.
Key findings:
Duration predicts outcomes beyond current BMI. A person who has carried obesity for 20 years faces measurably different biological consequences than someone with the same current BMI who became obese five years ago—even after controlling for current body weight.
"Metabolic memory" is real. Even after weight loss, some of the cellular and epigenetic changes induced by long-term obesity can persist. This is consistent with findings from bariatric surgery research, where patients who lose significant weight still show residual cardiovascular and metabolic risk related to their prior obesity duration.
Mid-life obesity may be particularly damaging. Different life stages appear to show varying biological vulnerability to obesity's aging effects. Weight gained and carried during mid-life—roughly ages 35 to 55—appears especially detrimental to long-term healthy aging trajectories, potentially because it coincides with natural declines in metabolic resilience and repair capacity.
Clinical Interpretation
These findings carry several important messages:
Earlier intervention provides compounding benefits. Achieving metabolic health in your 30s or 40s yields greater long-term returns than achieving the same outcome in your 60s—though both are valuable.
Current BMI understates total risk. A patient who has maintained obesity for 25 years carries greater biological age acceleration than their current weight alone would suggest.
Post-weight-loss management still matters. Patients who successfully lose weight through lifestyle change, medication, or surgery should understand that some legacy effects of long-term obesity may persist, making ongoing metabolic monitoring important.
Clinical Takeaway: When assessing a patient's obesity-related risk, ask not only "how much?" but "how long?" Obesity duration is an independent predictor of biological aging that BMI alone cannot capture.
5. Young Bodies, Old Cells: Alarming Evidence from Young Adults
One of the most sobering developments in recent obesity-aging research is the evidence that biological aging acceleration occurs well before middle age—in people in their 20s and 30s who have lived with obesity since childhood or adolescence.
A 2025 study in JAMA Network Open (Correa-Burrows et al.) followed young adults and measured biological aging across multiple systems simultaneously:
Epigenetic age (DNA methylation-based biological age)
Telomere length (chromosomal protective caps that shorten with aging and cellular stress)
Inflammatory biomarkers (C-reactive protein, IL-6, and others)
Metabolic health indicators (fasting glucose, lipid profiles, liver enzymes)
What the data showed:
Young adults with sustained obesity showed biological aging acceleration across multiple measures simultaneously. In some cases, their cellular biology resembled that of someone 10–15 years older chronologically. A 28-year-old could have the inflammatory profile, telomere length, and epigenetic signature of a person in their early 40s.
Critically, multiple aging systems were affected at once—not just one marker or one organ. This suggests systemic biological aging, not localized tissue damage.
Interpreting the Clinical Significance
These findings challenge a common clinical and cultural assumption: that the health consequences of obesity are something people will "deal with later." The research demonstrates that later is already here for many young people.
However, there is an important countervailing message: young bodies retain significant regenerative capacity. The same biological resilience that makes young people appear healthier on average also means they may respond more completely to intervention. Early identification and treatment of obesity in young adults—before the cumulative burden of "obesity-years" escalates—offers the greatest potential for biological age reversal.
Clinical Takeaway: Adolescent and young-adult obesity is not a cosmetic or future concern. It produces measurable, real-time biological aging. Screening, early intervention, and sustained support in this age group represents a critical opportunity to compress morbidity and extend healthspan.
6. Clinical Validity: What the Research Actually Proves (and What It Doesn't)
Interpreting the obesity-aging literature requires appropriate scientific caution. The mechanisms are compelling and the data are consistent, but several important caveats apply.
Strengths of the Evidence Base
Multiple independent mechanisms have been identified and replicated across diverse study populations and methodologies
Biomarker convergence: Consistent findings across epigenetic clocks, telomere assays, inflammatory markers, and metabolic indicators strengthen causal inference
Dose-response relationships: Greater obesity severity and longer duration associate with greater biological aging—the expected pattern if the relationship is causal
Intervention data: Weight loss—whether through lifestyle modification, pharmacotherapy, or bariatric surgery—is associated with measurable improvements in biological aging markers, supporting reversibility
Important Limitations
Most biological aging studies are observational; causality is inferred, not proven in most cases
Epigenetic clocks, while powerful predictive tools, measure correlation with outcomes rather than the specific mechanisms of aging—they are informative but not definitive
The obesity paradox (discussed below in the FAQ) is real in older populations and complicates simplistic "less weight = better health" messaging for all age groups
Study populations often skew toward younger adults with severe obesity; generalizability to mild overweight or older populations requires caution
The Bottom Line on Clinical Validity
The evidence that obesity accelerates biological aging is strong, consistent, and mechanistically plausible. It does not require every study to be a randomized controlled trial to be actionable. The convergence of evidence across multiple biological systems, multiple study designs, and multiple populations is sufficient to inform clinical decision-making. The appropriate response is not "more research needed before acting" but "act now, while continuing to refine our understanding."
7. Treating Obesity in Older Adults: Unique Challenges and Solutions
The stakes of obesity-related aging are especially high in older populations—but so are the risks of poorly managed treatment. Clinicians working with older adults must navigate several complexities.
7.1 Sarcopenic Obesity: The Double Danger
Sarcopenic obesity—the coexistence of excess adiposity and insufficient skeletal muscle mass—is one of the most clinically dangerous body composition phenotypes in aging.
Muscle tissue is the body's primary site of glucose disposal and a central regulator of metabolic rate. As lean mass declines with age and adiposity increases, metabolic function deteriorates rapidly. Sarcopenic obese individuals face elevated risks of:
Frailty and falls
Functional disability and loss of independence
Metabolic complications (insulin resistance, dyslipidemia)
Cardiovascular events
Mortality
The danger of standard caloric-restriction approaches in this population is that they can accelerate muscle loss if protein intake and resistance exercise are not carefully integrated. This is not a theoretical risk—it has been demonstrated in intervention studies.
7.2 Anabolic Resistance
Older adults develop anabolic resistance—reduced muscle protein synthetic response to dietary protein and exercise stimuli. This means that the same protein intake and training load that maintain muscle mass in a 35-year-old may be insufficient in a 70-year-old.
Clinical implications:
Protein targets should be higher in older adults pursuing weight loss—often 1.2–1.6 g/kg/day rather than the standard 0.8 g/kg/day
Protein quality matters: leucine-rich sources (dairy, animal proteins) appear most effective at stimulating muscle protein synthesis
Resistance training frequency may need to be higher to overcome blunted anabolic signaling
7.3 Functional Goals Over Numerical Targets
In geriatric patients, the primary treatment goal should not be achieving a specific BMI but optimizing functional capacity and quality of life. Clinical success metrics should include:
Gait speed and walking endurance
Grip strength
Ability to perform activities of daily living independently
Falls frequency
Energy levels and sleep quality
A 5–10% reduction in body weight, achieved while preserving or increasing muscle mass, can produce clinically meaningful improvements in all of these domains—without requiring patients to achieve an "ideal" BMI.
Clinical Takeaway: In older adults, "better body composition" is a more clinically useful goal than "lower weight." Protect muscle, reduce visceral fat, and measure success by function—not the scale.
8. Evidence-Based Strategies to Slow Biological Aging Through Weight Management
What does the evidence actually support as effective interventions?
8.1 Resistance Training: Non-Negotiable
Across virtually every study of weight management in aging populations, resistance training emerges as the single most critical exercise modality. It preserves and builds lean mass, improves insulin sensitivity, reduces visceral fat, and attenuates inflammaging—all while weight loss is occurring.
Two to three sessions per week targeting major muscle groups, with progressive overload, represents a minimum effective dose for most adults. Older adults, beginners, and those with functional limitations should work with a physical therapist or exercise specialist to develop safe, individualized programs.
8.2 Protein-First Nutrition
Adequate protein intake is the nutritional cornerstone of weight management that preserves biological youth. Evidence-based recommendations:
Daily target: 1.2–1.6 g per kilogram of body weight for adults pursuing weight loss, particularly over age 50
Meal distribution: Distribute protein across meals (aiming for 25–40g per meal) to maximize muscle protein synthesis
Priority sources: Greek yogurt, eggs, lean meats, legumes, cottage cheese, and high-quality whey protein
Modest caloric deficit (250–500 kcal/day) combined with adequate protein is more effective than aggressive caloric restriction for preserving metabolic health and muscle mass.
8.3 Anti-Inflammatory Dietary Patterns
Beyond macronutrients, the inflammatory load of the overall dietary pattern matters. The Mediterranean dietary pattern—characterized by abundant vegetables, legumes, whole grains, olive oil, fish, and nuts—has the strongest evidence base for reducing systemic inflammation and supporting metabolic health. A 2025 study (Oshakbayev) also highlighted connections between dietary patterns, metabolic rate, and aging trajectories.
Practical anti-inflammatory dietary priorities:
Replace refined carbohydrates with whole grains and legumes
Increase omega-3 fatty acid intake (fatty fish, flaxseed, walnuts)
Prioritize leafy greens and cruciferous vegetables
Reduce ultra-processed food consumption
Limit added sugars and refined seed oils
8.4 Sleep and Stress Management
Sleep deprivation and chronic psychological stress independently drive visceral fat accumulation, elevate cortisol, and accelerate epigenetic aging. These are not lifestyle "extras"—they are biological imperatives for metabolic health.
Adults should target 7–9 hours of quality sleep per night
Chronic sleep restriction increases hunger hormones (ghrelin) and impairs glucose regulation
Stress reduction practices (mindfulness, structured relaxation, nature exposure) have measurable effects on cortisol and inflammatory biomarker levels
8.5 Pharmacotherapy and Metabolic Surgery
GLP-1 receptor agonists (such as semaglutide and tirzepatide) represent a genuine advance in obesity pharmacotherapy, producing sustained weight loss of 15–20% of body weight in clinical trials—outcomes previously achievable only through bariatric surgery. Emerging data suggest these agents may also directly reduce inflammatory markers and improve metabolic aging indicators beyond their weight loss effects.
Bariatric surgery remains the most effective intervention for severe obesity and produces durable improvements in metabolic health, inflammatory burden, and functional capacity. For appropriately selected patients, the benefits extend well beyond weight loss to include biological age reversal across multiple measured parameters.
9. Practical Protocol: A Starter Framework
The following is a simplified framework for clinicians and individuals ready to act. This is not a substitute for individualized medical guidance.
Step 1: Assess composition, not just weight
Measure waist circumference (risk threshold: >35 inches in women, >40 inches in men)
Consider DEXA or bioimpedance analysis for body composition
Assess grip strength and gait speed if over age 60
Step 2: Set functional goals
Identify 2–3 functional benchmarks: "walk 30 minutes without pain," "climb 2 flights of stairs easily," "carry groceries without difficulty"
Step 3: Build the protein habit
Calculate protein target (1.2 × body weight in kg = grams per day)
Plan three protein-anchored meals daily
Step 4: Start resistance training
Begin with 2 sessions per week, full-body, bodyweight or light resistance
Progress gradually; consult a physical therapist if managing joint issues
Step 5: Address sleep and stress
Identify your single biggest sleep disruptor and address it first
Build one daily stress-reduction practice into your routine
Step 6: Seek medical support
Discuss pharmacotherapy with your physician if lifestyle changes are insufficient
Ask about body composition assessment tools available at your clinic
10. Common Myths and Mistakes
Myth: "I need to lose a lot of weight to see health benefits." Reality: A 5–10% reduction in body weight produces measurable improvements in inflammation, metabolic markers, blood pressure, and functional capacity. Modest, sustained loss consistently outperforms dramatic, unsustainable approaches.
Myth: "It's too late to reverse obesity's effects." Reality: The body retains remarkable regenerative capacity at any age. While metabolic memory means some legacy effects of long-term obesity may persist, significant biological improvements follow weight loss at every age studied.
Myth: "Cardio is the best exercise for weight loss." Reality: For biological aging outcomes, resistance training has a stronger evidence base than cardio alone—particularly for preserving lean mass, improving insulin sensitivity, and reducing visceral fat.
Myth: "Any caloric restriction is fine as long as I lose weight." Reality: Aggressive restriction without adequate protein and resistance training can accelerate muscle loss, worsen sarcopenia, and paradoxically increase metabolic age. Quality of intake matters as much as quantity.
Myth: "BMI of 25 is the target for everyone." Reality: In older adults, the "obesity paradox" suggests that a BMI of 25–29.9 may actually be associated with better outcomes than being underweight. Functional capacity and body composition matter more than weight class.
11. Frequently Asked Questions
Q: Does obesity actually make you age faster, or just increase disease risk? Both, and they are connected. Obesity accelerates biological aging at the cellular level—through measurable changes in epigenetic clocks, telomere length, cellular senescence, and inflammatory markers—while also increasing risk for the age-related diseases that these biological changes drive. Accelerated cellular aging and elevated disease risk are two expressions of the same underlying pathology.
Q: I've been overweight for 20 years. Is it too late to benefit from weight loss? No. While metabolic memory means some biological changes from long-term obesity can persist after weight loss, every study examining this question has found substantial benefits from intervention regardless of obesity duration. Your body retains significant capacity for repair and functional recovery at any age.
Q: How much weight loss is needed to see biological aging improvements? As little as 5–10% of total body weight produces measurable reductions in inflammatory markers, improvements in metabolic function, and in some studies, improvements in epigenetic aging clocks. Dramatic transformation is not required to produce meaningful biological benefit.
Q: What is the "obesity paradox" and is it real? Yes, it is real—particularly in older adults. Research consistently shows that for people over approximately 65–70, a BMI in the "overweight" range (25–29.9) is associated with lower mortality than a BMI in the "normal" range. This likely reflects the protective role of muscle mass and nutritional reserve in aging. It underscores why functional capacity, not BMI, should be the primary clinical target in older populations.
Q: Is "metabolically healthy obesity" actually safe? Not fully. While some individuals with obesity lack typical metabolic complications (sometimes called metabolically healthy obese, or MHO), research suggests this is often a transient state. The biological aging processes driven by visceral adiposity and inflammation occur even in MHO individuals to some degree—and many will develop metabolic complications over time.
Q: Can you reverse epigenetic aging with weight loss? Early evidence suggests yes, partially. Studies examining epigenetic clocks in patients before and after significant weight loss—particularly bariatric surgery—have found measurable reductions in biological age estimates. This is among the most exciting findings in longevity medicine, though larger long-term studies are needed.
Q: What role do new weight loss medications play? GLP-1 receptor agonists (semaglutide, tirzepatide) have transformed obesity pharmacotherapy, producing sustained 15–20% body weight reductions in clinical trials—substantially greater than most lifestyle-only interventions. Beyond weight loss, these agents appear to reduce cardiovascular events, improve inflammatory markers, and may have direct beneficial effects on aging biology independent of weight change. They are an important clinical tool for appropriate patients.
Q: At what age is it most important to address obesity for longevity? Earlier is consistently better. Mid-life obesity (roughly ages 35–55) appears particularly detrimental to long-term aging trajectories, but the evidence also demonstrates that young adults already experience measurable biological aging from sustained obesity. There is no age at which intervention loses value—but compound benefits are greatest for those who achieve metabolic health earlier.
Q: What is the single most important thing I can do? Build and preserve muscle mass while achieving a healthy body composition through sustainable lifestyle changes. Resistance training combined with protein-first nutrition offers the most comprehensive protection against obesity-related aging—more than any single dietary intervention, supplement, or medication.
Q: Should I track my biological age? Monitoring can be motivating and clinically useful. Validated tools include epigenetic age tests (available commercially, though methodology varies), telomere length tests, and standard metabolic panels that reflect biological aging (fasting glucose, HbA1c, lipid panel, hsCRP, fasting insulin). Functional measures—grip strength, gait speed, VO2 max estimates—are also excellent biological age proxies and are accessible to any clinician.
12. Conclusion and Next Steps
The science is now unambiguous: obesity is not merely a risk factor for aging-related disease—it is an accelerant of biological aging itself. Through mechanisms including chronic inflammation, oxidative stress, hormonal dysregulation, cellular senescence, and epigenetic reprogramming, excess adiposity pushes the aging process into an accelerated state that is measurable, consequential, and partially reversible.
The emerging framework of "obesity-years" brings important nuance: it is not enough to know a patient's current weight. How long they have carried it matters. What their body is composed of matters. How they function matters.
And most powerfully: intervention matters at every age and every stage. The evidence consistently shows that modest, sustained weight loss—paired with resistance training and adequate protein—produces meaningful biological improvements, from reduced inflammation to improved epigenetic clocks to enhanced functional capacity.
Your next steps:
Ask your doctor to assess your body composition and functional capacity, not just your BMI
Calculate your daily protein target and start building protein-anchored meals
Begin a resistance training program—even two sessions per week produces meaningful benefits
Address your sleep quality; it is not optional for metabolic health
If lifestyle changes have been insufficient, ask about pharmacotherapy options
Track progress using functional markers: how you move, what you can do, how you feel
The goal is not a number on a scale. The goal is a longer health span—more years of living fully, moving freely, and thinking clearly. The biology is on your side. Act on it.
Author's Note: A Clinician's Perspective
As an internal medicine physician, I frequently meet patients who believe the consequences of excess weight are decades away. Many feel relatively healthy in their 30s and 40s and assume serious problems will not emerge until much later.
One patient in his early forties stands out. Despite having no diagnosed diabetes or heart disease, he had lived with obesity since his twenties. Laboratory testing revealed elevated inflammatory markers, insulin resistance, fatty liver disease, and declining exercise capacity. Chronologically, he was 42 years old. Metabolically, his body was showing signs typically associated with someone much older.
Over the next 18 months, he adopted a structured resistance-training program, increased protein intake, improved sleep habits, and achieved a sustained weight loss of approximately 12% of his body weight. His liver enzymes normalized, insulin sensitivity improved significantly, inflammatory markers decreased, and his physical performance improved dramatically.
Cases like this reinforce an important lesson: the goal is not simply weight loss. The goal is preserving muscle, reducing visceral fat, improving metabolic health, and extending healthspan. Biological aging is influenced by daily choices more than most people realize, and meaningful improvements can occur at virtually any age.
Related Articles
Beyond Fat Cells: The Hidden Lymphatic Link to Obesity, Insulin Resistance, and Inflammation
How Excess Weight May Be Aging Your Brain Faster Than You Think
The mTOR Switch: Why Your Cells Stopped Listening to Insulin | DR T S DIDWAL
Why Protein After 55 Isn’t Optional — The Science Behind Why the RDA Is Too Low | DR T S DIDWAL
Why Aerobic Exercise Is the Most Powerful ‘Drug’ for Heart, Fat Loss & Longevity | DR T S DIDWAL
Exercise Unlocks a Hidden Glucose Pathway in Muscle — Independent of Insulin | DR T S DIDWAL
References
Correa-Burrows P, Burrows R, Albala C, et al. Long-term obesity and biological aging in young adults. JAMA Network Open. 2025;8(7):e2520011. https://doi.org/10.1001/jamanetworkopen.2025.20011
Malandrino N, Bhat SZ, Alfaraidhy M, Grewal RS, Kalyani RR. Obesity and aging. Endocrinol Metab Clin North Am. 2023;52(2):317–339. https://doi.org/10.1016/j.ecl.2022.10.001
Ragusa FS, Tanaka T, Veronese N, et al. Weight of time: exploring the link between obesity and aging. Aging Clin Exp Res. 2025;37:236. https://doi.org/10.1007/s40520-025-03106-4
The Lancet Healthy Longevity. Defining obesity to improve ageing. Lancet Healthy Longev. 2025;6(2):100696. https://doi.org/10.1016/j.lanhl.2025.100696
Roderka MN, Puri S, Batsis JA. Addressing obesity to promote healthy aging. Clin Geriatr Med. 2020;36(4):631–643. https://doi.org/10.1016/j.cger.2020.06.006
Oshakbayev K. Overweight effects on metabolic rate, time perception, aging, and lifespan. Curr Res Physiol. 2025. Advance online publication. https://doi.org/10.1016/j.crphys.2024.100166
Correa-Burrows P, Burrows R, Kennedy BK, et al. Obesity and biological aging across the life course: A geroscience framework for metabolic health. Metabolism. 2026;181:156634. https://doi.org/10.1016/j.metabol.2026.156634
Prateek GV, Chen Z, Wright K, et al. Longitudinal analysis of body weight reveals homeostatic and adaptive traits linked to lifespan in diversity outbred mice. Nat Commun. 2026;17:1689. https://doi.org/10.1038/s41467-026-68392-6
Ukraintseva S, Duan H, Holmes R, Arbeev K, Yashin A. Age-related changes in body weight as determinants of extreme longevity. Innovation in Aging. 2024;8(Suppl 1):807. https://doi.org/10.1093/geroni/igae098.2618
Fontana L, Hu FB. Optimal body weight for health and longevity: bridging basic, clinical, and population research. Aging Cell. 2014;13(3):391–400.
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. Hallmarks of aging: An expanding universe. Cell. 2023;186(2):243–278.
Campisi J, et al. From discoveries in ageing research to therapeutics for healthy ageing. Nature. 2019;571(7764):183–192.
Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002.
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205–216.
Stenholm S, Harris TB, Rantanen T, Visser M, Kritchevsky SB, Ferrucci L. Sarcopenic obesity: definition, cause and consequences. Curr Opin Clin Nutr Metab Care. 2008;11(6):693–700.
This article is intended for educational and informational purposes and reflects current scientific evidence at the time of writing. It does not constitute medical advice. Individual circumstances vary significantly; all treatment decisions should be made in consultation with qualified healthcare professionals.